
Abstract
Introduction
G
Several animal studies have suggested that photobiomodulation (PBM) attenuates inflammation, stimulates viability and cell proliferation of healthy bone marrow mesenchymal stem cells (BMMSCs) in vivo 6 and promotes fracture healing, and increases new bone formation. 7,8 PBM could reduce pain and accelerate the fracture process in patients. 9 In another human investigation, Nesioonpour et al. reported that PBM (low-level laser therapy) could decrease pain after surgery, and PBM was easily tolerated by patients. 10 Some studies have demonstrated that PBM promotes bone formation in diabetic animals. Patrocinio-Silva et al. utilized PBM (808 nm laser, 100 mW, 120 J/cm2) on non-fractured long bones in streptozotocin (STZ)-induced TIDM rats. They started PBM just one week after STZ injection. PBM caused increase in the cortical area and Runt-related transcription factor 2 (RUNX2) expression. 11 Nascimento et al. reported that PBM [780 infrared gallium-aluminum-arsenide (IR GaAlAs) laser, 70 mW, 17.5 J/cm2] significantly improved bone healing in TIDM in animals. 12 Akyol and Güngörmüş found that PBM (GaAlAs laser, 808 nm, 2 × 5 J/cm2) stimulates trabecular bone formation of bone defect in femurs in STZ-induced TIDM rats. 13
However, other studies show that there are inconsistent results about positive effects of PBM on fracture healing in normal and diabetic animals. 14 –19
The process of fracture healing could be separated into two sets of anabolic (bone forming) and catabolic (bone remodeling) responses. Controlling catabolism can be as important as anabolic stimulation. 20
To the best of our knowledge, none of the published studies has investigated the effects of PBM with pulse wave laser on stereological parameters, and gene expression of RUNX2, osteocalcin, and receptor activator of nuclear factor kappa-B ligand (RANKL) in repairing tissue of tibial partial bone defect (partial osteotomy) in the STZ-induced TIDM in rats during catabolic response. In this study, we examined the effects of PBM on stereological parameters, and gene expression of RUNX2, osteocalcin and RANKL in repairing tissue of tibial partial osteotomy in the STZ-induced TIDM in rats during catabolic response of fracture healing. The results of this study could improve fracture healing in diabetic patients.
Materials and Methods
Animals and study design
Forty-eight 4-month-old female Wistar rats have been randomly divided into four groups of 12 each: group one (healthy control, no TIDM and no PBM), group two (healthy test, no TIDM and PBM), group three (diabetic control, TIDM and no PBM), and group four (diabetic test, no TIDM and PBM). TIDM was induced in the third and fourth groups. We made a partial bone defect in the right tibia of all the groups. The bone defects of second and fourth groups were irradiated by a low-level laser. Thirty days after the surgery, all rats were euthanized and all bone defects were extracted. Six bone defects of each group were submitted to histological and stereological examination, and remaining six underwent real-time polymerase chain reaction (RT-PCR). All techniques of current investigation were confirmed by the human and animal Ethics commission at Shahid Beheshti University of Medical Sciences.
Induction of TIDM
We induced TI DM in the third and fourth groups by dissolved STZ in distilled water (40 mg/kg, single dose, and intraperitoneal). 21 TIDM has been defined as blood glucose level greater than 250 mg/dL, which was measured in the blood samples made 7 days after STZ injection. The blood glucose levels and body weights were recorded throughout the experiment. We maintained entire animals for 1 month after administration of STZ to establish DM. 14
Surgery
The technique has been explained thoroughly in the previous article. 14 Under general anesthesia and sterile conditions, the skin of right leg of each rat was cut longitudinally, right below the knee joint on the medial side. Medial surface of tibia's shaft was exposed. A circular partial transversal standardized osteotomy with 1.5-mm diameter, deep to the central medullary canal, was made in the midpoint of the bone with a low speed drill (Delab Co., Dental Fabrik, Erfurt, Germany). Our previous study confirmed that a 1.5 mm bone defect fitted well with the dimensions of rats' tibia bone. It means the bone tolerated well the defect, and there was no complete fracture after partial osteotomy in the site of defect in tibia in diabetic animals. 14
The site was irrigated with saline solution to avoid burning. The muscles were sutured with a 03 catgut, and the skin was sutured with a 04 nylon reverse cutting needle. The rats received antibiotic therapy injections with ceftriaxone (50 mg/kg, intramuscular) immediately before the surgery and 24 and 48 h after the surgery. 14
Photobiomodulation
A laser unit (Mustang 2000; Technical Co., LO7 pen, Moscow, Russia) has been used. The specifications of laser are shown in Table 1. The laser protocol for this study was applied successfully on a complete osteotomy in an experimental rat model. 7 PBM was started on day 1 and was followed on the right tibia thrice per week for 30 days. In the test-irradiated rats, the total bone, including bone defect, was completely irradiated by three laser shots (Fig. 1). Thirty days after the beginning of treatments, all the rats have been euthanized. We extracted the right tibias of six rats for the histological examinations and the series of six samples have been frozen at −80°C for RT-PCR tests.

Laser radiation technique.
Stereological study
Measurement of bone volumes
All techniques were explained completely in our previous studies.
7,22
Live pictures of the callus in bone defect were evaluated using a projecting microscope. All volumes (V), including total volume of callus (mm3), bone marrow volume (mm3), trabecular bone volume (mm3), and cortical bone volume (mm3), were calculated using the Cavalieri method:
where Σp is the total of points hitting a callus section, a/p is the area associated with each point, and t is distance between the sampled sections. 7,22
Estimation of number of bone cells
The dissector method was used to estimate numerical density and total number of bone cells.
7,22
Numerical density of cells was obtained by
where ΣQ− is the number of cells, including osteocytes, osteoblasts, and osteoclasts counted (103) in all the dissectors, h is the height of the optical dissector, a/ƒ is the area of the counting frame, Σp is the total number of counted frames, BA is the microtome block advance to cut the block (25 μm), and t is the mean of the final section thickness (20 μm). The following formula was used to estimate the total number of bone cells: N (bone cell) = Nv × V (final). 7,22
RNA extraction and RT-PCR
RNA extraction and RT-PCR techniques were described completely in our previous study. 22 The total RNA was extracted using Trizol reagents (Invitrogen, Carlsbad, CA) using a tissue lyser instrument (Qiagen, GmbH, Germany). cDNA synthesis was performed using the Revert Aid First Strand cDNA synthesis kit (Fermentas, Vilnius, Lithuania). Gene expression of RUNX2, osteocalcin, and RANKL was monitored by quantitative RT-PCR using the SYBR Green PCR Master Mix (Takara Bio, Kusatsu, Shiga, Japan). The expression values were normalized by the genometric mean of 18s rRNA. The primers used to amplify cDNA are shown in Table 2. For each sample, three replicates were produced for each target gene. 22
RUNX2, Runt-related transcription factor 2; RANKL, receptor activator of nuclear factor kappa-B ligand.
Statistical analysis
We reported all data as mean ± standard deviation. One-way analysis of variance (ANOVA) and the least significant difference (LSD) were used to compare changes among groups of stereological and gene expression data (with normal distribution). A p-value of <0.05 was considered statistically significant.
Results
General observations
TIDM animals of group 4 showed decline in body weight at the final measurement (Table 3).
Stereological examination
Light micrographs of histological parameters are shown in Fig. 2. Findings of stereological examinations are presented in Figs. 3 –9.
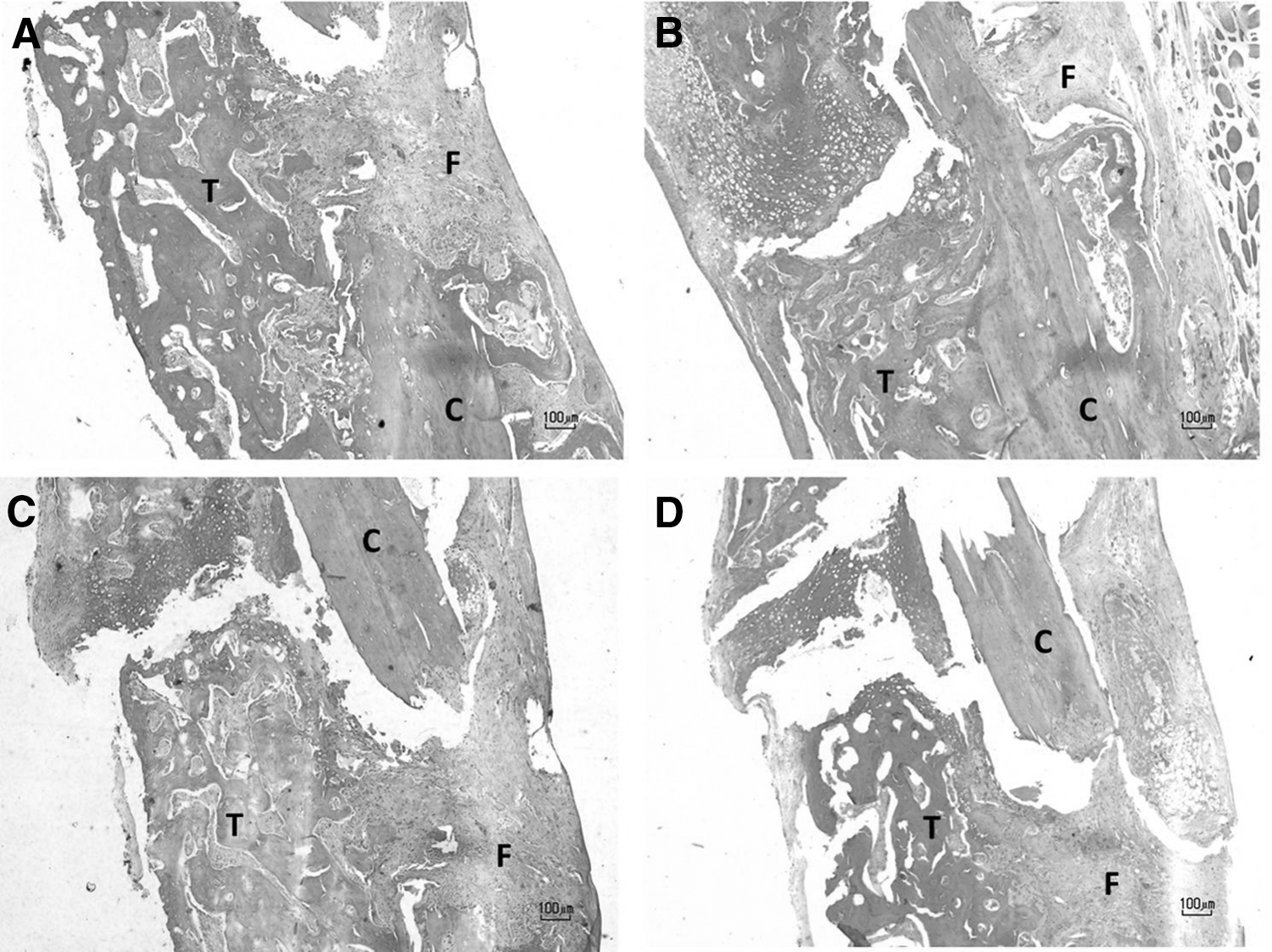
Light micrographs of studied groups (hematoxylin and eosin staining method).
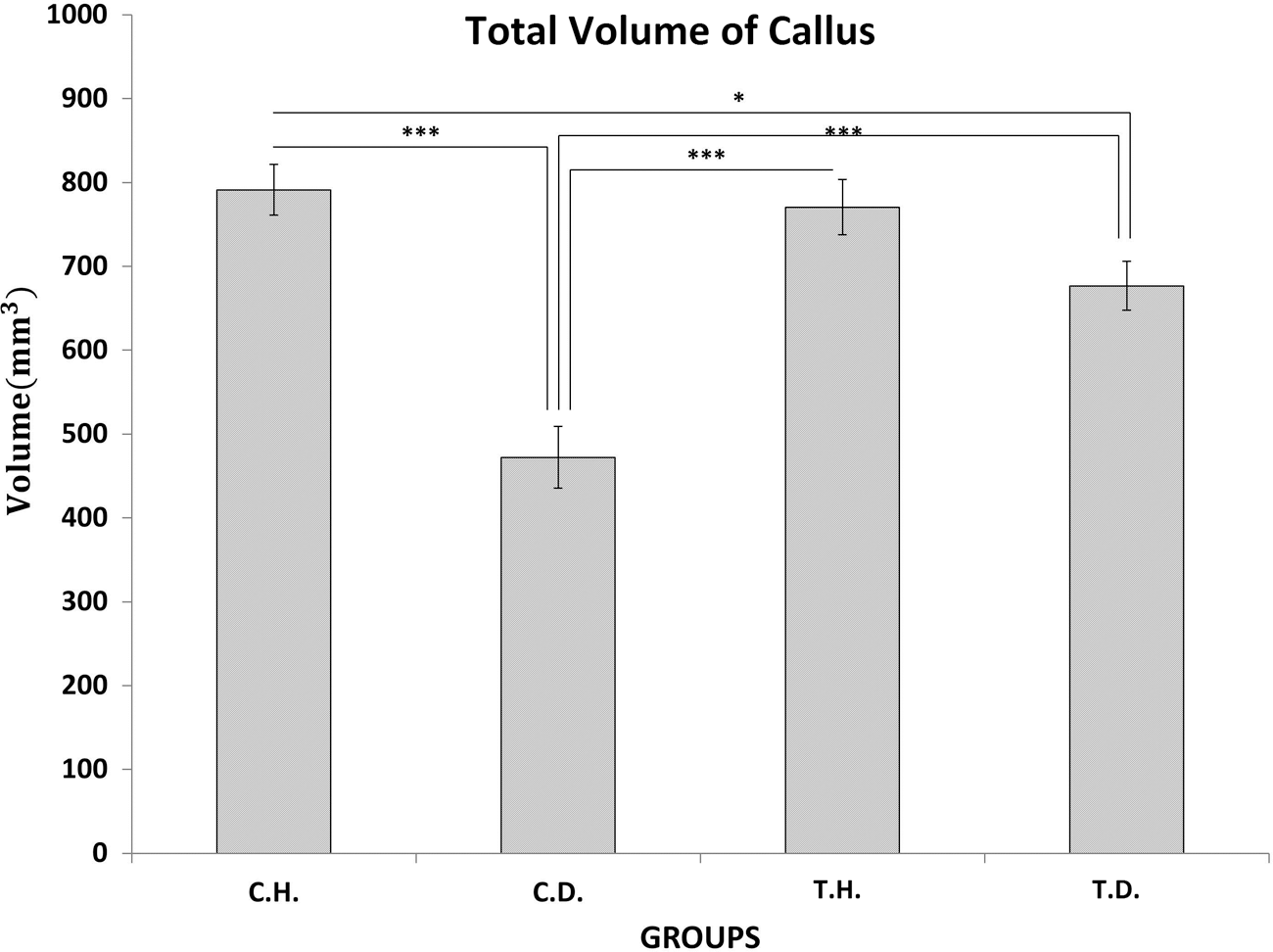
Mean ± SD of the total volume of callus (mm3) of the studied groups compared by ANOVA, and LSD tests, *p < 0.05, ***p < 0.001. SD, standard deviation; ANOVA, analysis of variance; LSD, least significant difference; C.H., control healthy; C.D., control diabetes; T.H., test healthy; T.D., test diabetes.

Mean ± SD of the bone marrow volume (mm3) of the studied groups compared by ANOVA, and LSD tests, ***p < 0.001.

Mean ± SD of the cortical bone volume (mm3) of the studied groups compared by ANOVA, and LSD tests, ***p < 0.001. Increased value of cortical bone volume in healthy test was close to significant difference compared to diabetic test (LSD test, p = 0.054).

Mean ± SD of the trabecular bone volume (mm3) of the studied groups compared by ANOVA, and LSD tests, **p < 0.01, ***p < 0.001.
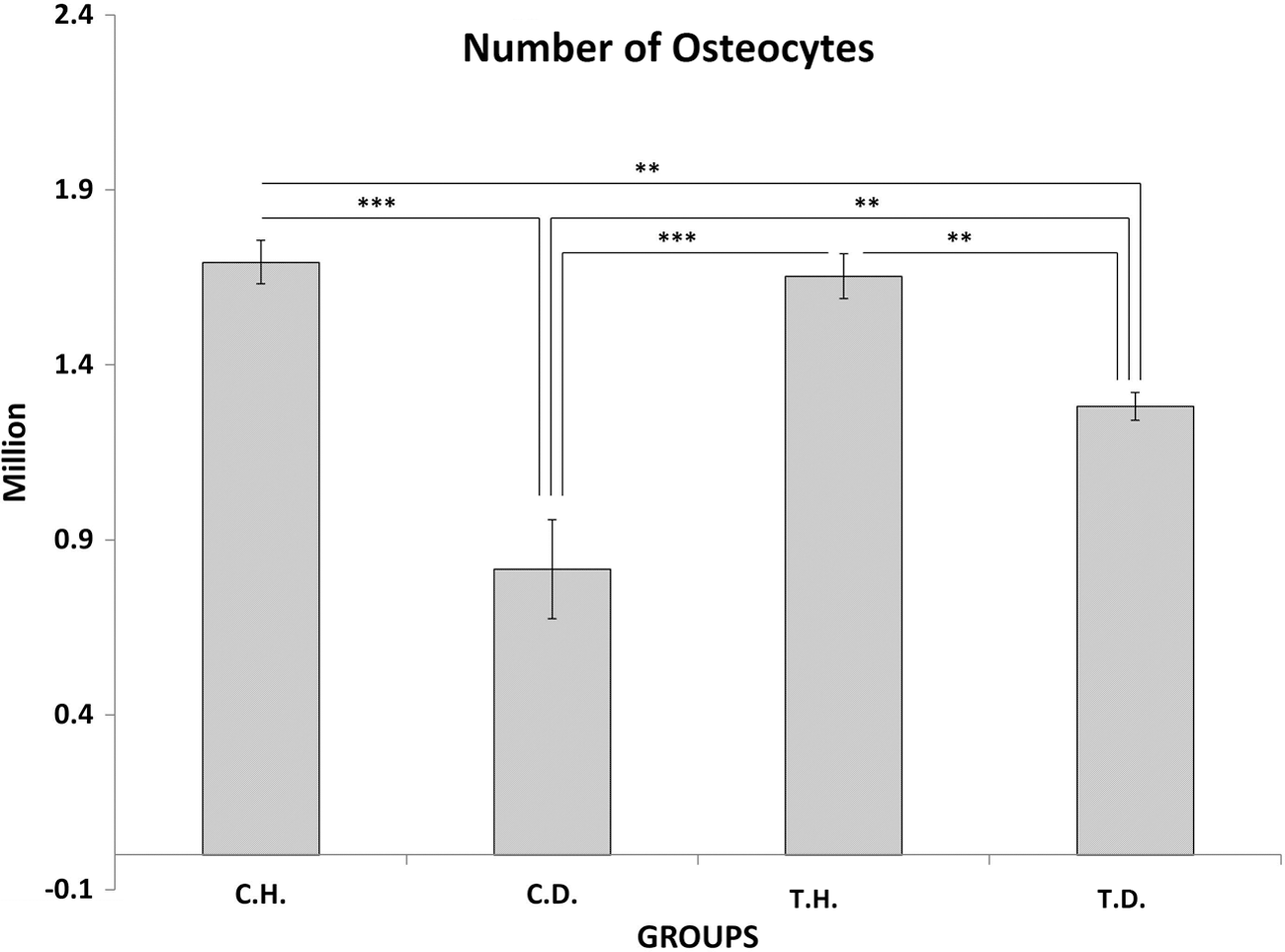
Mean ± SD of the osteocyte number (106) of the studied groups compared by ANOVA, and LSD tests **p < 0.01, ***p < 0.001.
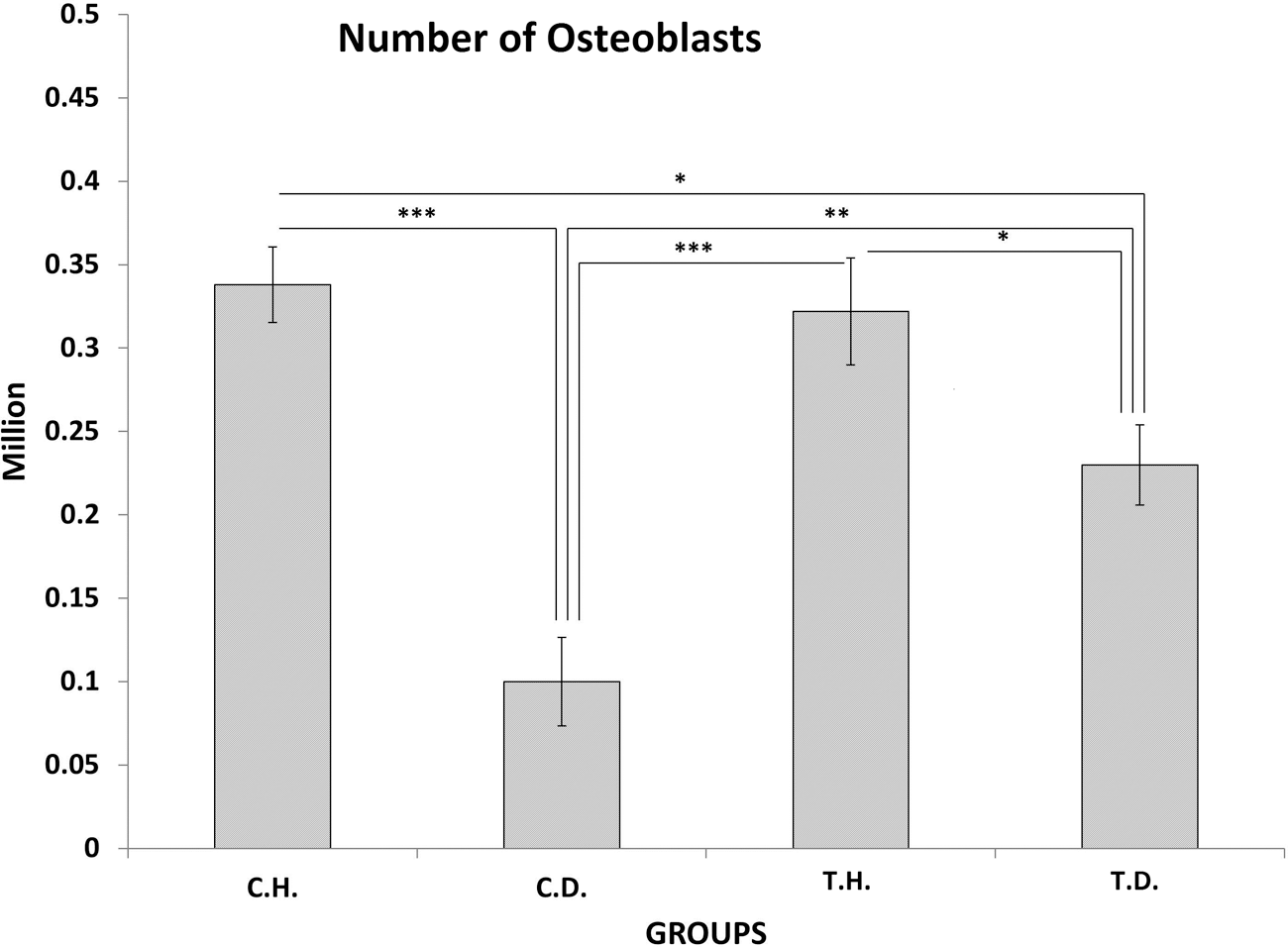
Mean ± SD of the osteoblast number (106) of the studied groups compared by ANOVA, and LSD tests *p < 0.05, **p < 0.01, ***p < 0.001.

Mean ± SD of the osteoclast number (103) of the studied groups compared by ANOVA, and LSD tests, ***p < 0.001.
In terms of total volumes (mm3) of callus, bone marrow, and cortical bone, findings of the statistical analysis revealed a significant reduction in control diabetic compared to other groups (LSD test, All p = 0.000). We found a significant reduction in total volume of callus of diabetic test compared to healthy control (LSD test, p = 0.024). The statistical difference in total volume of callus between healthy test and diabetic test was close to significant difference (LSD test, p = 0.059). Increased value of cortical bone volume in healthy test was close to significant difference compared to diabetic test (LSD test, p = 0.054).
LSD test revealed a significant decrease in trabecular bone volume (mm3) of diabetic control group compared to healthy control, healthy test, and diabetic test groups (p = 0.000, p = 0.000, and p = 0.001 respectively). Also, there was a significant difference in trabecular bone volume (mm3) of diabetic test group and other test groups (LSD test, all p = 0.001) (Figs. 3 –9).
LSD test demonstrated significant decreases in osteocyte number (106) of diabetic control rats compared to healthy rats, healthy test, and diabetic test rats (p = 0.000, p = 0.000, and p = 0.001 respectively). LSD test detected significant decreases in osteocyte numbers of diabetic test rats compared to healthy control and healthy test rats (p = 0.005, p = 0.009), and significant increase compared to diabetic control (p = 0.001) (Fig. 7).
We observed significant reduction of osteoblast number (106) of diabetic control rats compared to healthy control, healthy test, and diabetic test rats (LSD test, p = 0.000, p = 0.000, and p = 0.002 respectively). Based on the LSD test, significant decreases were found in osteoblast number of diabetic test group compared to healthy control and healthy test groups (p = 0.010, p = 0.025), and significant increase compared to diabetic control (p = 0.002) (Fig. 8).
We found a significant reduction in osteoclast number (103) of diabetic control rats compared to other groups (LSD test, all p = 0.000) (Fig. 9).
RT-PCR test
Based on the LSD test results, there was a significant increase in RUNX2 of diabetic control compared to healthy control and healthy test groups (p = 0.020 and p = 0.049, respectively). Our observation showed a significant increase in Osteocalcin of diabetic control group compared to those in healthy test, diabetic test, and healthy control groups (p = 0.002, p = 0.005, and p = 0.033 respectively). There were significant increases in RANKL of diabetic control group in comparison with the healthy test group (p = 0.041).
Discussion
We investigated the effects of PBM on stereological parameters, and gene expression using RT-PCR of RUNX2, osteocalcin, and RANKL levels in callus of tibial bone defect in the TIDM rats during catabolic response of fracture healing. TIDM has decreased entire stereological parameters of callus compared to those of healthy group. PBM (890 nm, 80 Hz, 1.5 J/cm2) increased the number of osteocytes and osteoblasts within the callus in TIDM rats compared to those in diabetic control. PBM has not increased bony cells number of the healthy rats.
Compared to healthy control group, fracture healing was delayed in diabetic rats during the catabolic response of fracture healing. Our findings are consistent with the findings of earlier studies, which reported that osteoblast number, new mineralized tissue area, blood vessel count, 23 and sum of histologic scores 24 of fracture healing in bone defects at the catabolic response were lesser in TIDM rats than those of control healthy animals.
The energy density of laser used in this work has been selected according to the previous reports of this laboratory, in which it was indicated that the 890-nm laser at 1.5 J/cm2 and 80 Hz frequency was able to increase bone strength in complete osteotomy 7 and partial osteotomy 14 bone defects.
The below hypothesis, which tries to describe the absence of biostimulatory effect of the PBM on stereological parameters of partial osteotomy in healthy rats during catabolic response, can be suggested as follows:
Clinical and paraclinical information, such as bone mineral density, histological and biochemical parameters, and gene expression findings can assist clinicians in determining the best treatment for patients with bone diseases. 24 Fundamental function of bone is to resist mechanical injury and absorb pressure. Bone strength depends on both quantity and quality of bone tissue. Quantity of bone is outlined by the geometry and shape of the bone and the microarchitecture of the trabecular and cortical bone morphology. Quality of bone is characterized by intrinsic properties of bony tissue such as turnover, mineral, and collagen. One of the major complications of diseases that can affect the bone diseases such as DM and osteoporosis, that is, fracture, is due to decrease in bone strength. Consequently, any management of bone diseases relies on improving bone power. 25 –31
Our results showed that PBM significantly increased the volume of total callus, total bone, bone marrow, trabecular bone, and cortical bone, and the number of osteocytes and osteoblasts of callus in TIDM rats compared to those of callus in diabetic control rats. These results (significant differences between test-irradiated group and control group in stereological parameters) may be in agreement with increase in trabecular bone on days 20 and 30 in bone defects of the diabetic rats in the test- irradiated group, as recently reported by Nascimento et al., 12 and Akyol and Güngörmüş. 13 Nascimento et al. 12 studied the effect of PBM (780 IR GaAlAs laser, 70 mW, 17.5 J/cm2) on fracture healing in TIDM animals on days 7, 18, and 30 after osteotomy. They found wide and thick trabecular bone formation in test and healthy normal groups. However, in diabetic control, the trabecular bone was thinner and more irregular on day 30. Nascimento et al. 12 also found that the new bone zone was significantly lower in diabetic group compared to ones in test-irradiated diabetic and healthy groups on day 30 after surgery. Akyol and Güngörmüş 13 studied the effects of PBM (GaAlAs laser, 808 nm, 2 × 5 J/cm2, five sessions) on repair of femoral partial osteotomy in STZ-induced TIDM in rats on days 10 and 20 after surgery. They found a significant increase in substantia spongiosa (cancellous bone) formation in diabetic test group compared to diabetic control group on day 20. Akyol and Güngörmüş 13 concluded that PBM revealed a positive result on cancellous bone in TIDM femoral partial osteotomy. 13
Besides, we observed that TIDM has increased RUNX-2 and osteocalcin in callus of tibial bone defect compared to healthy group, and RANKL gene expression compared to test-irradiated healthy rats. PBM significantly decreased osteocalcin gene expression in TIDM rats.
Recently, Park and Kang 32 evaluated the effect of PBM (980-nm GaAlAs diode laser, 0.01 W, 60 sec, and 13.95 J/cm2, every day) on the healing of extracted dental sockets in STZ-induced TIDM and normal rats on days 3, 5, 7, and 14 days after surgery. The samples were tested by hematoxylin and eosin method and reverse transcription-PCR. Compared to other groups, bone formation was inferior in diabetic rats on day 14. Bone formation in test-irradiated rats was more prominent than diabetic control. The density of RUNX-2 expression was considerably higher in test-irradiated diabetic rats than in diabetic control at 5, 7, and 14 days. Osteocalcin mRNA expression rate increased in all study groups, except for diabetic control. Osteocalcin mRNA expression rate was also higher in the test group than in nonirradiated diabetic rats on day 3. Similar expression of collagen type I mRNA was found in diabetic control and test-irradiated diabetic rats on days 3 and 14. 32 Magri et al. 33 studied the effects of PBM (808 nm, 100 mW, and 30, 60, and 120 J/cm2, thrice per week) on healing of tibial bone defect of STZ-induced TIDM in rats on days 15 and 30 after surgery. PBM started 15 days after STZ injection. 33 They observed a marked increase of RUNX2 on day 15 in test group compared to diabetic control. RUNX2 immunoexpression was the same among the study groups on day 30. Similar results for RANKL were reported by Magri et al. 33 for all study groups on day 15. More immunoexpression of RANKL was reported with energy densities of 30 and 120 J/cm2 compared to diabetic control on day 30. 33 Interestingly, Magri et al. 33 reported no statistically marked difference for the biomechanical test of studied groups on days 15 and 30.
Our RT-PCR test established that fracture repair was modulated in TIDM rats during catabolic response by significant enhances in RUNX2 and osteocalcin expressions compared to healthy control rats. Also, PBM decreased osteocalcin mRNA expression in diabetic rats during catabolic response of fracture healing. As bone calcification begins, osteocalcin is released by osteoblasts and increases only in the later stages of osteoblast differentiation. 34 Additional studies should be performed to offer more evidence regarding the stimulatory effects of PBM on bone repair in TIDM bone defect.
Conclusions
PBM was capable of biostimulating bone repair in STZ-induced TIDM during catabolic response of fracture healing, by significant increase of volumes of total callus, total bone, bone marrow, trabecular bone, and cortical bone, and the number of osteocytes and osteoblasts compared to control rats. Further, RT-PCR test established that bone repair was modulated in diabetic rats during catabolic response of fracture healing by significant increase in RUNX-2 and osteocalcin expressions compared to healthy control rats. PBM also decreased osteocalcin mRNA expression in diabetic rats.
Acknowledgments
We extend our appreciation for financial support (grant no. 11608) to the cellular and molecular biology research center, and the Vice Chancellor of Research at Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Footnotes
Author Disclosure Statement
No competing financial interests exist.