
Abstract
Objective:
The aim of this study was to evaluate the mineral content and morphology of primary tooth enamel prepared using an Er:YAG laser at different power settings.
Materials and methods:
The buccal surfaces of 45 noncarious primary molars were assessed in this study. The surfaces were cleaned and the teeth were randomly divided into nine groups (n = 5 each) to evaluate the effects of Er:YAG laser treatment at different energy levels: 200 mJ, 2 Hz; 200 mJ, 3 Hz; 200 mJ, 10 Hz; 250 mJ, 2 Hz; 250 mJ, 3 Hz; 250 mJ, 10 Hz; 300 mJ, 2 Hz; 300 mJ, 3 Hz; and 300 mJ, 10 Hz. The mean percentage weight (wt%) of calcium (Ca), phosphorous (P), fluoride (F), magnesium (Mg), potassium (K), and sodium (Na) in the primary tooth enamel was calculated for each group using scanning electron microscopy (SEM) with energy dispersive X-ray spectroscopy before and after laser application. The enamel morphology was also evaluated using SEM. The obtained data were statistically analyzed by one-way analysis of variance and Tukey's honest significant difference test.
Results:
The mean wt% of Ca, P, and F in the enamel exhibited a significant change after laser treatment (p < 0.05); the wt% of Mg, K, and Na remained unchanged (p > 0.05). There was no association between the power setting of the laser and changes in the wt% of minerals in the enamel (p > 0.05). SEM showed that enamel irradiated at different energy levels exhibited a characteristic lava flow appearance, and more surface irregularities were observed with the 250-mJ setting than with the 200-mJ setting.
Conclusions:
Our findings suggest that the mineral content and morphology of the enamel of primary teeth are affected by Er:YAG laser irradiation.
Introduction
L
Contemporary dental principles recommend, as often as possible, noninvasive rather than invasive strategies. In this context, cavity preparation with high-level lasers such as the Er:YAG laser has gained popularity in recent years. 2 This technology is considered to offer greater patient comfort by reducing the vibrations, noise, and pressure associated with rotary dental instruments and has consequently been presented as a viable alternative for conventional high-speed air turbines and low-speed burs. 2 These characteristics are valuable in the field of pediatric dentistry.
The physical interaction of the Er:YAG laser with dental tissue has been shown to be an effective mechanism for the selective ablation of carious and healthy dentin and enamel in both primary and permanent teeth, despite the different water and mineral contents of these different substrates and the different ablation thresholds for different hard tissues. 3
The crowns of teeth are covered by dental enamel, which is the hardest tissue in the human body. It is composed of 4% organic material and plasma and 92–96% inorganic matter or mineral content by weight. The mineral phase primarily consists of calcium phosphate in the form of hydroxyapatite crystals, which are carbonated or fluoridated. 4,5 The average growth period for the crowns of primary teeth is 6–14 months, whereas that for permanent teeth is 3–4 years. Therefore, primary teeth present thinner enamel than do their permanent succesors. 6 The degree of mineralization of primary tooth enamel is lower than that of permanent tooth enamel; therefore, the water content and, consequently, energy absorption of the former are higher. This necessitates the use of different parameters for primary tooth ablation and permanent tooth ablation. 3,7
Recent studies have reported the mineral content of hard tissues in dental crowns and roots prepared by different laser treatments. Ari and Erdemir reported that the adhesion of dental restorative materials to hard tissue was affected by changes in the mineral content of dentin. While Topçuoğlu and Köseoğlu determined that the laser systems used in their study did not affect the mineral content of root canal dentin. 8,9 Dilber et al. demonstrated that laser irradiation did not affect the composition of the dentin surface; the mean percentage weight (wt%) of calcium (Ca), potassium (K), magnesium (Mg), sodium (Na), and phosphorous (P) and the Ca/P ratio in the dentin assessed in different groups stratified by the type of laser treatment were not affected. 10
Very few studies have assessed the mineral content of hard tissues in primary teeth treated by lasers. 11,12 However, the effects of Er:YAG laser treatment on the mineral content of primary tooth enamel have not been adequately studied.
The aim of this study was to evaluate the mineral content and morphology of primary tooth enamel prepared using an Er:YAG laser at different power settings. The null hypothesis tested was that the levels of Ca, K, Mg, Na, F, and P and the Ca/P ratio in primary tooth enamel would not differ after Er:YAG laser treatment at different power settings.
Materials and Methods
In this study, we evaluated the mineral content and morphology of primary tooth enamel prepared using an Er:YAG laser at different power settings (Table 1).
Laser Parameters
When the average values of the parameters of minerals were considered at 95% confidence, the power analysis of the study was calculated as 99.9% (the highest) and 89.1% (the lowest). The maximum effect size of the study is 12.07 and the minimum effect size of 0.941. Thus, minimum of five samples per group was required.
Sample preparation
The buccal surfaces of 45 primary molars were assessed in this study. Teeth with caries, restorations, cracks, and defects on the buccal surfaces or fluorosis were excluded. After the teeth were cleaned and washed with fluoride-free pumice, they were stored in distilled water for 1 month until the experiment. When necessary, roots were sectioned 1 mm below the cementoenamel junction. The teeth were embedded in autopolymerizing acrylic resin (Meliodent; Bayer Dental, Newbury, United Kingdom) such that the buccal surfaces were exposed. The exposed surface was smoothened using wet 400-grit sandpaper to obtain a flat and uniform enamel surface. The teeth were covered with nail varnish, excluding a 3 × 3-mm window on the middle-third of the buccal surface.
Er:YAG laser irradiation
The teeth were divided into nine groups of five teeth each to evaluate the effects of laser treatment at different energy levels. An Er:YAG laser system (Fidelis Plus III; Fotona, Ljubljana, Slovenia) with a 50-μs laser pulse duration was used to irradiate the samples at a fixed wavelength of 2.94 μm; an energy pulse ranging from 200 to 300 mJ; and a pulse repetition rate of 2, 3, and 10 Hz. The roughening process was performed in the non-contact mode in accordance with the manufacturer's recommendations. Irradiation was manually performed from the reference point, with a laser spot diameter of 2 mm along the entire sample. The tip was maintained perpendicular to the enamel surface and was moved in one direction from right to left and forward to backward under water and air cooling.
All laser treatments were performed by the same operator (K.K.) to prevent inter-operator variations.
The nine groups were based on the power settings of the laser device as follows.
Group I: 0.40 W, 2 Hz, and 200 mJ
Group II: 0.60 W, 3 Hz, and 200 mJ
Group III: 2 W, 10 Hz, and 200 mJ
Group IV: 0.50 W, 2 Hz, and 250 mJ
Group V: 0.75 W, 3 Hz, and 250 mJ
Group VI: 2.5 W, 10 Hz, and 250 mJ
Group VII: 0.60 W, 2 Hz, and 300 mJ
Group VIII: 0.90 W, 3 Hz, and 300 mJ
Group IX: 3 W, 10 Hz, and 300 mJ
Energy dispersive X-ray spectroscopy
Before and after each laser irradiation, the wt% of Ca, P, Mg, Na, K, and F in an enamel area of 300 × 300 μm in all specimens was determined by energy dispersive X-ray spectroscopy (EDX) (Zeiss EVO LS 10; Carl Zeiss SMT. Ltd., Cambridge, United Kingdom).
Scanning electron microscopy
After laser irradiation, one specimen from each group was prepared for scanning electron microscopy (SEM; Zeiss EVO LS 10; Carl Zeiss SMT. Ltd.). After surface treatment, the specimens were sputter-coated (108 auto, Creessington Sputter Coater) with gold alloy under high vacuum. Subsequently, photomicrographs were obtained for analysis.
Statistical analyses
The obtained data were statistically analyzed using SPSS 22.0 for Windows (SPSS, Chicago, IL). The enamel mineral content before and after laser treatment in the nine groups was analyzed using one-way analysis of variance (ANOVA), and the comparison of means was performed using Tukey's honest significant difference multiple comparisons test. Statistical differences were determined at a 95% confidence level (p = 0.05).
Results
Table 2 lists the mean wt% of Ca, P, Mg, Na, K, and F and the Ca/P ratio in the primary tooth enamel before and after Er:YAG laser treatment in each group. One-way ANOVA showed that there were significant changes in the wt% of Ca, P, and F and the Ca/P ratio (p < 0.05) after laser treatment; whereas the wt% of Mg, Na, and K remained unaffected by laser treatment (p > 0.05).
Mean Percentage Weights of the Six Elements and Ca/P Ratio (Before and After Laser Applications) According to Groups (n = 5 per Group)
Groups with different letters are significantly different (p < 0.05).
Ca, calcium; Ca/P, calcium/phosphorous; F, fluoride; K, potassium; Mg, magnesium; Na, sodium.
Changes in the wt% of Ca, Mg, Na, P, F, and K and the Ca/P ratio showed no significant differences according to the laser energy level (p > 0.05).
SEM images of the enamel before and after Er:YAG laser treatment are shown in Figs. 1 –4. Deciduous enamel irradiated with different output energies exhibited a characteristic lava flow appearance (Figs. 2 –4). More surface irregularities were observed with the 250-mJ setting than with the 200-mJ setting. There was no evidence of enamel structure degradation, such as crater formation, although cracks were observed.
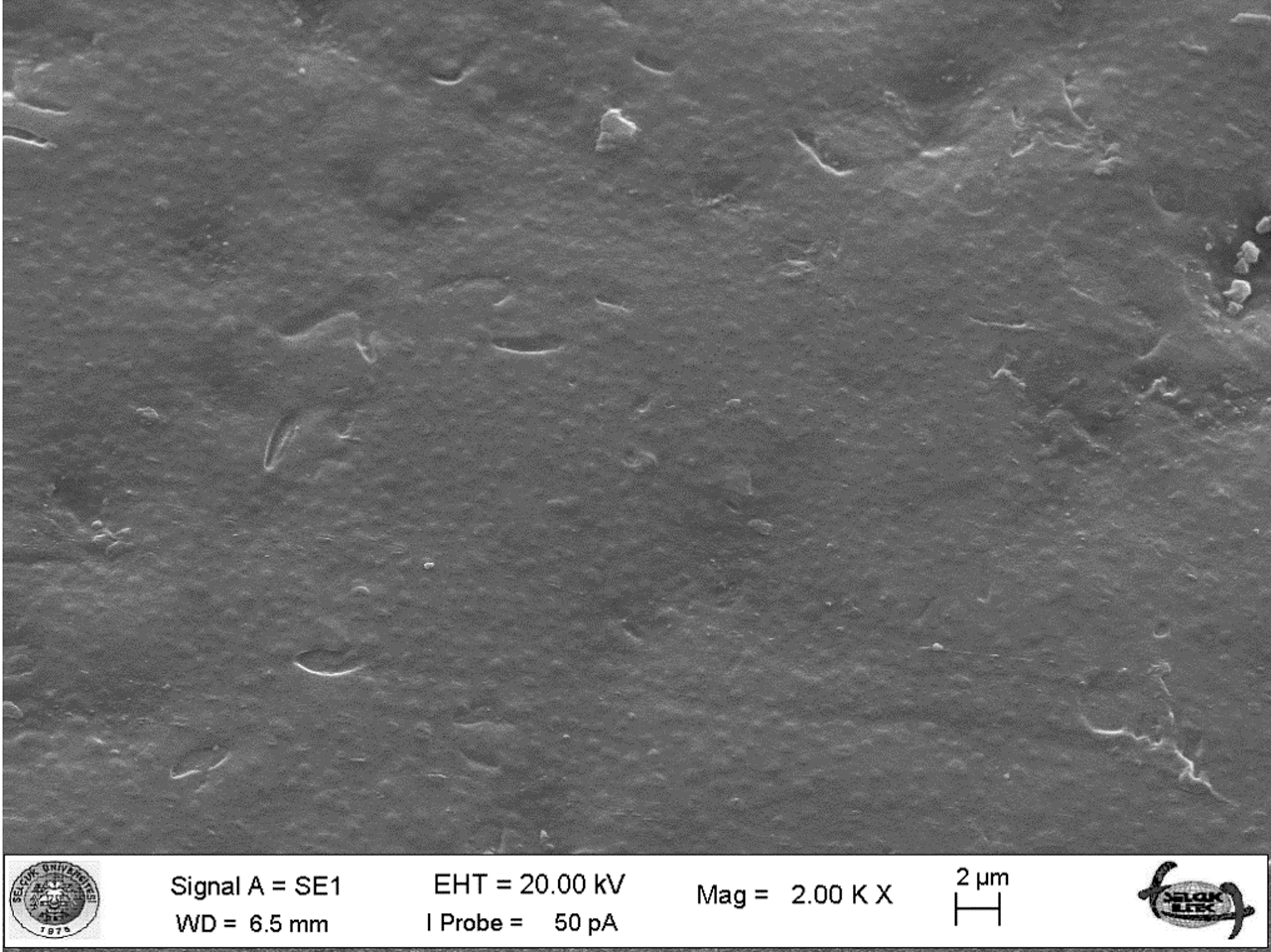
SEM micrograph of enamel surface in control group (original magnification 2.00K × ). Control group has a smooth area. SEM, scanning electron microscopy.
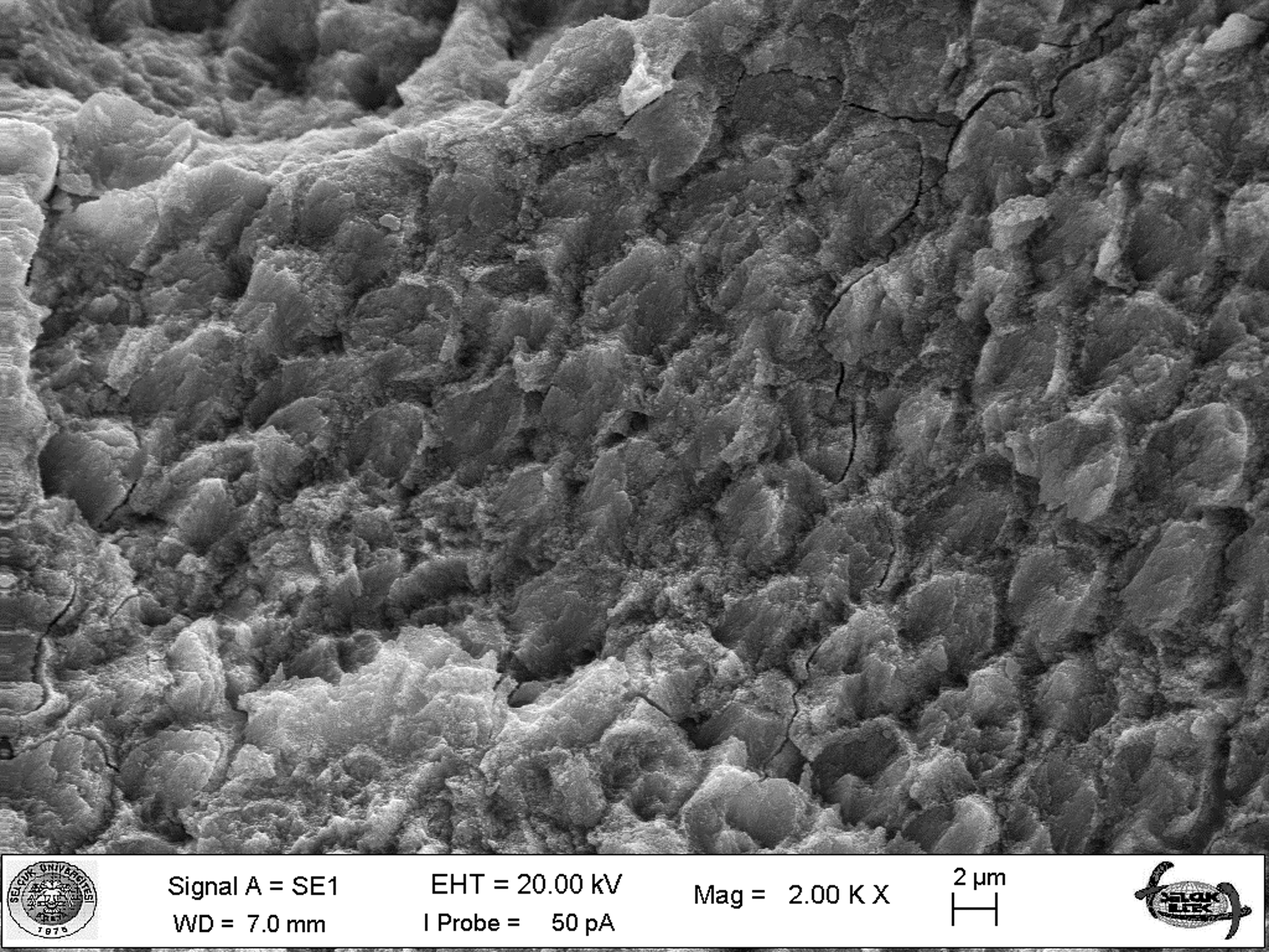
SEM micrograph of enamel surface irradiated at 200 mJ (original magnification 2.00K × ). A crack is evident crossing the area of the surface.
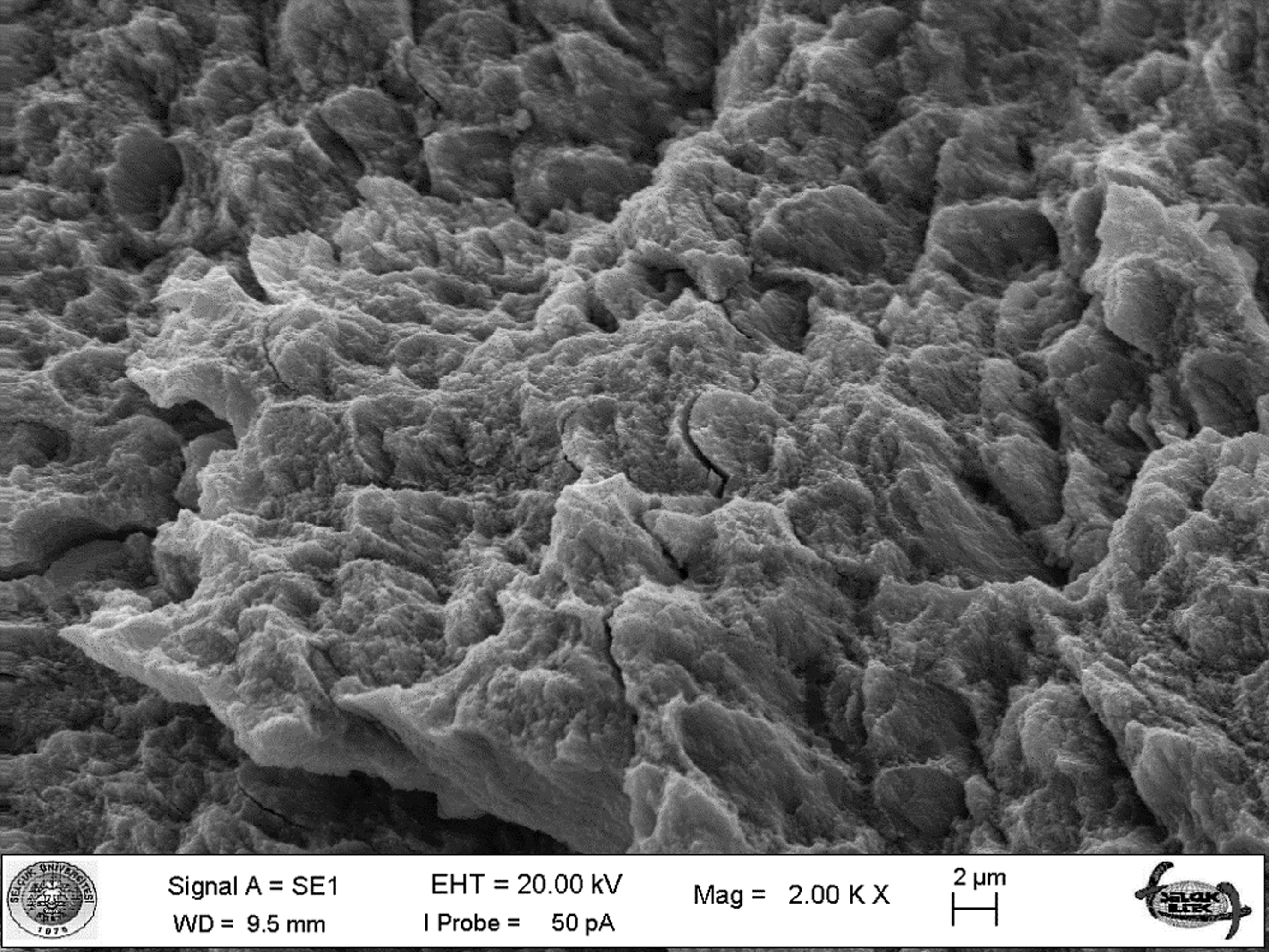
SEM micrograph of enamel surface irradiated at 250 mJ (original magnification 2.00K × ).
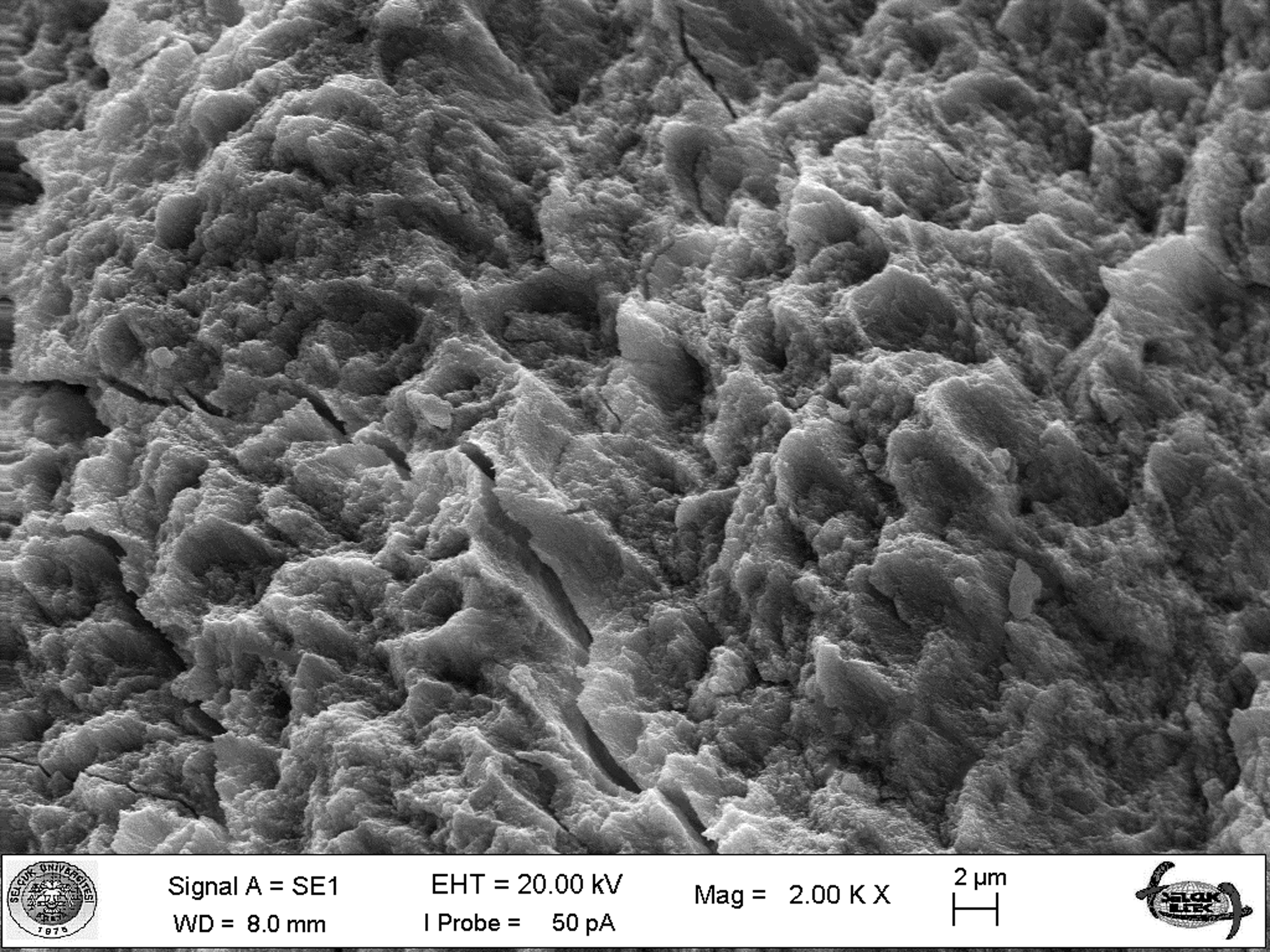
SEM micrograph of enamel surface irradiated at 300 mJ (original magnification 2.00K × ).
Discussion
In this study, we evaluated changes in the mineral content and morphology of primary tooth enamel after Er:YAG laser treatment at different power settings. The Ca/P ratios before and after laser irradiation in each group were also compared using EDX. We found that the mean wt% of Ca, P, and F and the Ca/P ratio were affected by laser irradiation. Therefore, the null hypothesis of the study was rejected.
It is important to motivate children to visit their dentists to prevent oral and dental diseases. Therefore, pediatric dentists must learn new and modern technologies. 13 Laser technology provides an opportunity for more efficient diagnosis and treatment of oral and dental soft and hard tissue conditions in children. Laser therapy is well accepted by children and parents because of its minimal invasiveness. 14 Studies have demonstrated that children are more cooperative during restorative, pulpal, and surgical treatments using lasers, and this significantly enhances the quality of care and improves the treatment process. 15 However, the use of the Er:YAG laser in both primary and permanent teeth may cause changes in the hard tissue morphology. According to Mortimer, the enamel of primary teeth is thinner than that of permanent teeth, and the level of mineralization is lower in the former than in the latter (89.7% in permanent tooth enamel, 80.6% in primary tooth enamel). 6 In this study, we aimed to determine Er:YAG laser-induced changes in primary tooth enamel. Laser etching causes chemical and morphological changes caused by heating of the enamel. It has been hypothesized that these changes occur because of fusion and melting of hydroxyapatite and/or subsequent sealing of the enamel. 16 The enamel surface temperature increases rapidly to 10,000°C during laser irradiation. The organic matrix in enamel evaporates and decomposes at temperatures of 400–800°C, and the protective effect of the organic matrix may decrease or even disappear when the enamel is heated above 1000°C. 17 Changes in the structure and composition of apatite crystals may cause alterations in the Ca/P ratio, and the use of air and/or water cooling during laser irradiation limits these effects. Perito et al. performed laser preparation under water cooling in their study to compare the effects of conventional and Er:YAG laser treatments on the acid resistance of enamel. 18 Similarly, other studies also used air and water cooling during laser treatment and observed that the Ca/P ratio in the experimental groups did not exhibit any significant changes after Er:YAG laser preparation. 9,19 However, in this study, the wt% of Ca and P and the Ca/P ratio in primary tooth enamel were found to increase after Er:YAG laser preparation. We believe that the morphology of primary tooth enamel is the reason for the discrepancy between our findings and previous findings. Dankner et al. reported that these changes are a consequence of melting and recrystallization processes. The use of different laser systems and examination methods is another reason for the different findings among studies. 20
The potential of various erbium laser wavelengths to increase the acid resistance of dental enamel has been demonstrated in vitro. 21 The surface produced by laser etching is claimed to be acid-resistant because of a modified Ca/P ratio, a decreased carbonate/phosphate ratio, and the formation of more stable and less acid-soluble compounds; these changes lower the susceptibility to acid attacks and decay. 22 –24 Er:YAG lasers have also been shown to increase the acid resistance of enamel. 25 In this study, the Ca/P ratio in primary tooth enamel increased after laser treatment. According to Díaz-Monroy et al. the acid resistance of enamel increased for teeth irradiated with 200 and 300 mJ, similar to the protocol in the our study. 26 This may have increased the acid resistance of the assessed primary teeth.
Some researchers have assessed the mineral content of the hard tissues in primary teeth treated by lasers. Guler et al. determined that laser treatment did not affect the mean wt% of Ca, K, Mg, Na, and P or the Ca/P ratio in the primary tooth dentin in any group. 11 Monghini et al. studied the effects of Er:YAG laser irradiation on primary tooth dentin and found that the dentin bond strength of adhesives was adversely affected. 12 Of late, researchers have been showing increasing interest in the chemical changes in enamel after Er:YAG laser irradiation. 27 The effects of the Er:YAG laser on the mineral content in primary tooth enamel have not been evaluated in previous studies. The degree of mineralization of primary tooth enamel is lower than that of permanent tooth enamel; therefore, the water content and energy absorption of the former are higher than those of the latter.
As opposed to the control group, irradiated groups showed statistically significant differences in the wt% of Ca and P during the experimental phases. The wt% of P showed a significant increase after irradiation, probably because of an increase in the pyrophosphate content caused by enamel heating. 23 The wt% of Ca also showed a significant increase after irradiation. Ca and P present in hydroxyapatite crystals are the major inorganic components of dental hard tissue. 28 These elements play an important role in the remineralization process for hydroxyapatite crystals. 29 In this study, the wt% of Mg, Na, and K remained unaffected by laser treatment. Mg is an important element, while Na and K are present in small amounts in the enamel structure.
Giusti et al. suggests that high laser energy parameters should be used to decrease the ablation time for primary teeth, which is a worthwhile goal with respect to treatment in children. 30 A shorter working time for pediatric patients results in more successful treatment rates. Although high laser energy levels decrease the chair time, the adverse effects on primary enamel and dentin should also be minimized. Therefore, we used many different laser (200, 250, 300 mJ) parameters in our study and found that these parameters were not associated with changes in the mineral content of primary tooth enamel. 30,31 These findings indicate that a high energy setting (300 mJ) can be used to decrease the chair time for pediatric patients.
SEM techniques, which are widely used in the field of materials science, are also used to evaluate dental morphology. In this study, primary enamel tissue was examined under high-resolution SEM combined with EDX for determination of mineral content and morphology. Several reports have shown the effects of ER:YAG laser irradiation on enamel morphology. Effects such as exposed enamel prisms, surface roughening, crater formation, surface rupture and fractures, melting, and carbonization have been observed after Er:YAG laser irradiation. 32 The strongly absorbed laser energy in enamel is converted to heat that suddenly boils the water present. This boiled water releases high-pressure steam that leads to ablation when the pressure exceeds the ultimate strength of the tooth. The ablated materials and their successive recoil force result in the formation of craters on the surface. Moreover, the irradiated surface becomes flaky with an irregularly serrated and microfissured morphology. 33 The irregularity of the enamel surface after Er:YAG laser irradiation can be compensated by the application of phosphoric acid, which attacks and regularizes the previously opened prisms. Thus, the enamel surface allows microinfiltration of the bonding agent. 34,35 The enamel surfaces in our study exhibited a characteristic lava flow appearance after irradiation at different output energies, like the findings of Kornblit et al. 32 Secilmis et al. assessed SEM images of Er Cr:YSGG laser-irradiated surfaces and found that surface irregularities and enamel exposure increased with an increase in the laser power level. 36 Similarly, more surface irregularities were observed with the 250-mJ setting than with the 200-mJ setting. There was no evidence of enamel structure degradation, such as crater formation, although cracks were observed, similar to the finding in the study by Secilmis et al. 36
Conclusions
Within the limitations of this study, we could draw the following conclusions.
Er:YAG laser treatment changes the wt% of Ca, P, and F and the Ca/P ratio in primary tooth enamel, whereas it does not affect the wt% of K, Mg, and Na.
Er:YAG laser-induced changes in the mineral content of primary tooth enamel are not influenced by the laser power setting.
Er:YAG laser treatment changes the surface morphology of primary tooth enamel.
Thus, Er:YAG laser irradiation can cause both structural and chemical changes in primary tooth enamel. These changes may affect the solubility and acid resistance of the enamel. In particular, laser treatment at different energy levels can increase the Ca and P content and the Ca/P ratio. Therefore, Er:YAG laser irradiation can be a promising treatment in pediatric dentistry. Further studies are required to determine laser-induced changes in primary tooth enamel and to investigate the effects of laser treatment on the acid resistance of primary tooth enamel.
Footnotes
Author Disclosure Statement
No competing financial interests exist.