
Abstract
Objective:
To evaluate the long-term effects of intense pulsed light (IPL) combined with meibomian gland expression (MGX) in the treatment of meibomian gland dysfunction (MGD).
Background:
Although IPL has been proven to be effective in the treatment of MGD, any report regarding its long-term efficacy is unavailable by now.
Methods:
The randomly selected study eye received a series of three IPL treatments that were applied directly on eyelids with an interval of 4 weeks (treatment energy, 14–16 J/cm2). The control eye received three sham IPL treatments (0 J/cm2). MGX was performed on both eyes. Meibomian gland yielding secretion score (MGYSS) and tear film break-up time (TBUT) were evaluated at baseline and at 1, 3, 6, and 9 months after treatments.
Results:
In the study eyes, MGYSS of both the upper and lower eyelids and TBUT improved at 1, 3, 6 months after treatments (p < 0.01). MGYSS in lower eyelids continued to improve at 9 months (p < 0.05). The changes in MGYSS and TBUT after treatment were larger in the study eyes than in the control eyes at 1, 3, 6 months (p < 0.01), but no difference at 9 months (p > 0.05). The percentage improvement in the MGYSS of lower eyelids after treatment was higher than that of upper eyelids.
Conclusions:
Three consecutive IPL treatments combined with MGX improved MG secretion function and TBUT by 6 months after treatment in MGD patients. The improvement in MG secretion function was greater in the lower eyelid than in the upper eyelid.
Introduction
M
Intense pulsed light (IPL) treatment involves the use of a xenon flash lamp emitting light at wavelengths ranging from 500 to 1200 nm, which are selectively absorbed by various chromophores (such as hemoglobin, melanin, and water). Along with light, the lamp also produces heat. IPL is widely used in dermatology and cosmetic fields to treat conditions such as facial telangiectasia, facial rosacea, pigmented lesions, and excessive hair growth through selective photothermolysis to destroy vascular structures, bacteria, pigments, and hair follicles, and inhibition of inflammatory mediators. 6,7 In 2002, Dr Toyos serendipitously observed that the symptoms of MGD and related dry eye were relieved in patients who had undergone IPL treatment for facial rosacea. 8 Since then, other ophthalmologists have studied the efficacy of IPL treatment for MGD/dry eye. Several retrospective studies and a few prospective studies have shown that three to four treatment sessions of IPL applied on the cheeks near the inferior periocular area can relieve the symptoms of MGD, improve meibomian gland secretion, and lengthen tear break-up time (TBUT) in MGD/dry eye patients. 8 –14 The proposed mechanisms underlying these effects are meibum softening by the thermal effect of IPL, 15 ablation of telangiectasia, which results in a decrease in inflammatory factors, and reduction of bacteria and other microorganisms. 16,17 However, the long-term efficacy of IPL treatment has not yet been studied.
In our previous study, we modified the currently used IPL treatment method and evaluated the short-term effects of our modified treatment protocol. 18 In our method, IPL was applied directly on the upper and lower eyelids, while the cornea and sclera were under protection. MGX was performed after IPL treatment.
In our previous study, the treated eyes showed an improvement in both meibomian gland secretion function and TBUT on the 28th day after the first treatment session, and these parameters continued to improve over the course of the treatment. Further, no serious adverse ocular and dermal effects were detected during the study.
In the present study, we aimed to determine the long-term efficacy of the combined IPL treatment and MGX protocol we devised in our earlier study. We followed up the MGD patients who had undergone a series of three IPL treatments in our previous study for 9 months.
Materials and Methods
Ethics and consent
This prospective, randomized, double-masked, controlled study was approved by the ethics committee of Peking University First Hospital (no. 2015[1009]). The clinical trial was registered in Chinese Clinical Trial Registry (registration no. ChiCRT-INR-16010256). The study was conducted following the tenets of the Declaration of Helsinki. Written consent was obtained from all participants before their inclusion in the clinical trial.
Patients
Patients were recruited from the Department of Ophthalmology of Peking University First Hospital between January 2016 and April 2017. The inclusion criteria were as follows: (1) age above 18 years, (2) Standard Patient Evaluation of Eye Dryness (SPEED) questionnaire score of at least 6 for both eyes, (3) meibomian gland yielding secretion score (MGYSS) of no more than 12 for the lower eyelid, and (4) Fitzpatrick skin type 1–4. 19 The exclusion criteria included the following: (1) any intraocular inflammation, ocular surgery, or ocular trauma in the past 6 months, (2) ocular infection or allergy, (3) any eyelid structural abnormality, (4) any systematic diseases that may lead to dry eye disease, (5) tanning in the 4 weeks before enrolment, (6) skin cancer or pigmented lesion in the treatment zone, and (7) pregnancy or lactation.
Forty-four MGD patients satisfied the selection criteria and enrolled in this study. All of the participants signed the informed consent form and underwent three treatment sessions of our modified IPL plus Max protocol. Of these, 28 patients completed the entire 9-month follow-up assessment and were included in this study.
Treatment procedure
One eye was randomly selected as the study eye according to a computer-generated randomization program; the fellow eye served as the control eye. The study eye received three IPL treatments at 4-week intervals, while the control eye received a sham IPL treatment. Both eyes were treated with MGX and artificial tears.
After washing face with cosmetic face cleanser, the eyelid skin was numbed with a topical anesthetic (compound lidocaine cream; Ziguang Pharmaceutical Co. Ltd., Beijing, China). After 30 min, the numbing cream was wiped away. A drop of 0.4% oxybuprocaine hydrochloride (Benoxil; Santen Pharmaceutical Co. Ltd, Osaka, Japan) was instilled into the conjunctival sac, and another drop was instilled 5 min later.
A layer of cooled ultrasound gel was applied on the upper and lower eyelid skin. A Jaeger lid plate (Suzhou Mingren Medical Equipment Co. Ltd., Suzhou, China) was placed in the conjunctival sac to fully occlude the cornea and sclera during the treatment. An M22 IPL system with optimal pulse technology (Lumenis Ltd., Tel Aviv, Israel) was used in our study. It has a xenon lamp emitting IPL at 515–1200 nm and a 560-nm filter. The optimal pulse technology makes IPL pulses more stable and highly repeatable. For the study eye, the fluence of the IPL system was set to 14–16 J/cm2 depending on the Fitzpatrick skin type of the patient. A dermatologist applied a series of 12 overlapping IPL pulses directly on the upper and lower eyelids (Fig. 1). The distance between IPL pulses and the eyelid margin was 2–3 mm. For the control eye, the fluence was set to 0 J/cm2.
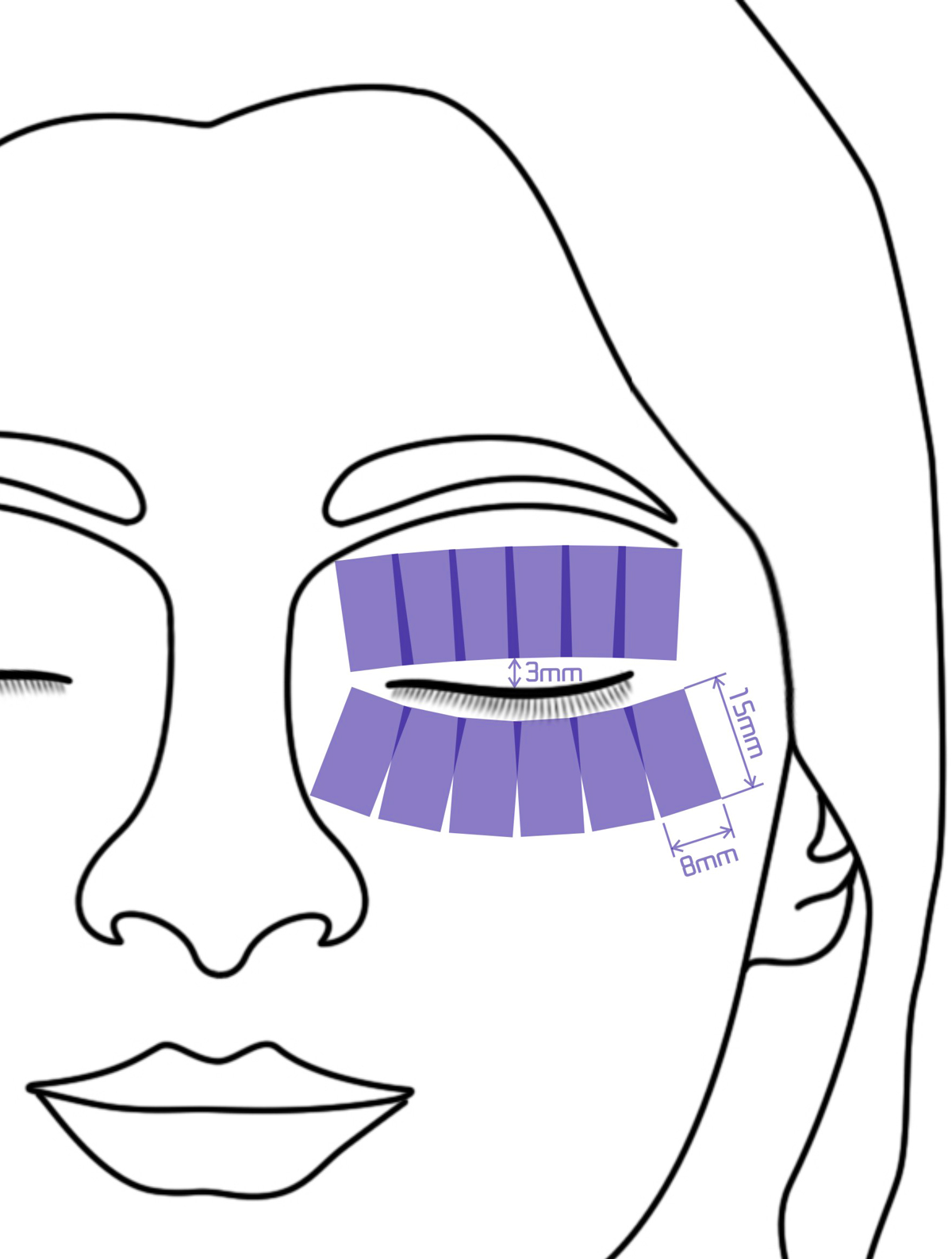
IPL treatment zone including 12 overlapping periocular areas, each of which measures 8 × 15 mm. IPL, intense pulsed light.
After removal of the ultrasound gel, an ophthalmologist performed MGX on the upper and lower eyelids using the Arita meibomian gland compressor (Katena Products, Inc., Denville, NJ). After the procedure, patients were instructed to use artificial tears (Systane Lubricant Eye Drops; Alcon Laboratories, Inc., Fort Worth, TX) on both eyes whenever they felt it necessary, but no more than three times a day.
The complete therapy included three treatment sessions performed at 4-week intervals. The clinicians who performed the treatments were not involved in the subsequent examination process to minimize bias. The patients were examined at baseline and at 1, 3, 6, and 9 months after the treatment. The following examinations were performed in the order given: SPEED questionnaire, TBUT, corneal fluorescein staining (CFS), and meibomian gland assessment.
Primary outcome measure
The primary outcome measure was the MGYSS, which reflected the meibomian gland secretion function. The MGYSS was measured using a meibomian gland evaluator (MGE; Tear Science, Inc., Morrisville, NC) according to the Lane protocol. 20 Fifteen glands of temporal, central, and nasal regions in both upper and lower eyelids were evaluated. For each of these glands, the secretion was graded as follows: 0, no secretion; 1, inspissated/toothpaste consistency; 2, cloudy liquid secretion; and 3, clear liquid secretion. The scores were then summed to a single MGYSS, termed u-MGYSS for the upper eyelid and l-MGYSS for the lower eyelid. The MGYSS thus ranged from 0 to 45.
Secondary outcome measures
Tear film break-up time
A fluorescein sodium strip (Jingming New Technological Development Co. Ltd., Tianjin, China) was moistened with sterile saline, and fluorescein was gently instilled into the lower bulbar conjunctiva taking care not to cause any eye irritation. The patient was asked to blink naturally several times and then to stare straight ahead without blinking. The time between the last complete blink and the first appearance of a dry spot or a disruption in the tear film was observed and recorded under a slit lamp microscope with a cobalt blue light filter. The procedure was performed three times, and the average value was acquired for each eye.
SPEED score
The SPEED questionnaire 21 was used to evaluate the severity and frequency of MGD-related dry eye symptoms. The SPEED score ranges between 0 and 28.
CFS score
After TBUT measurement, the CFS score was calculated. The cornea was divided into four quadrants. Each quadrant was graded from 0 to 3 using the criteria 22 issued by the Corneal Disease Group of the Ophthalmological Society in 2013: 0, no punctate staining; 1, 1–30 punctate lesions; 2, >30 punctate lesions but no confluent lesions; and 3, confluent lesions or ulcer. The total CFS score of the four quadrants ranged from 0 to 12.
Statistical analysis
Statistical analysis was performed with SPSS 20.0 (IBM Corporation, Armonk, NY). Descriptive statistics are presented as means ± standard deviations. Outcome measures before and after treatment were analyzed using the Friedman two-way analysis of variance, with the pairwise Wilcoxon test for post hoc testing. Differences between study and control eyes were analyzed using the pairwise Wilcoxon test. Statistical significance was set at the α = 0.05 level.
Results
General information
A total of 28 patients, including 10 men and 18 women, completed the entire therapy and follow-up assessment protocol and were included in the analysis. The average age of the patients was 42.17 ± 17.62 years (range, 24–78 years). In the study, 8, 18, and 2 participants were of Fitzpatrick type 2, 3, 4 separately. The study eye (15 right eyes and 13 left eyes) received three IPL treatments performed at 4-week intervals, while the control eye (13 right eyes and 15 left eyes) received a sham IPL treatment. Both eyes were treated with MGX and artificial tears.
Primary outcome measure
The results of the MYGSS are presented in Figure 2 and Table 1. The u-MYGSS did not differ between the study eyes (10.21 ± 7.46) and the control eyes (11.18 ± 9.341) at baseline (p = 0.542). In the study eyes, the u-MYGSS significantly increased compared to the baseline at 1, 3, and 6 months after the treatment (p < 0.01), but did not further increase at 9 months (p > 0.05). In the control eyes, the u-MGYSS did not significantly improve after treatment (p > 0.05; Fig. 2). The changes in the u-MYGSS after treatment compared to the baseline were significantly higher in the study eyes than in the control eyes at 1, 3, 6, and 9 months (p = 0.001, 0.002, 0.002, 0.042, respectively).
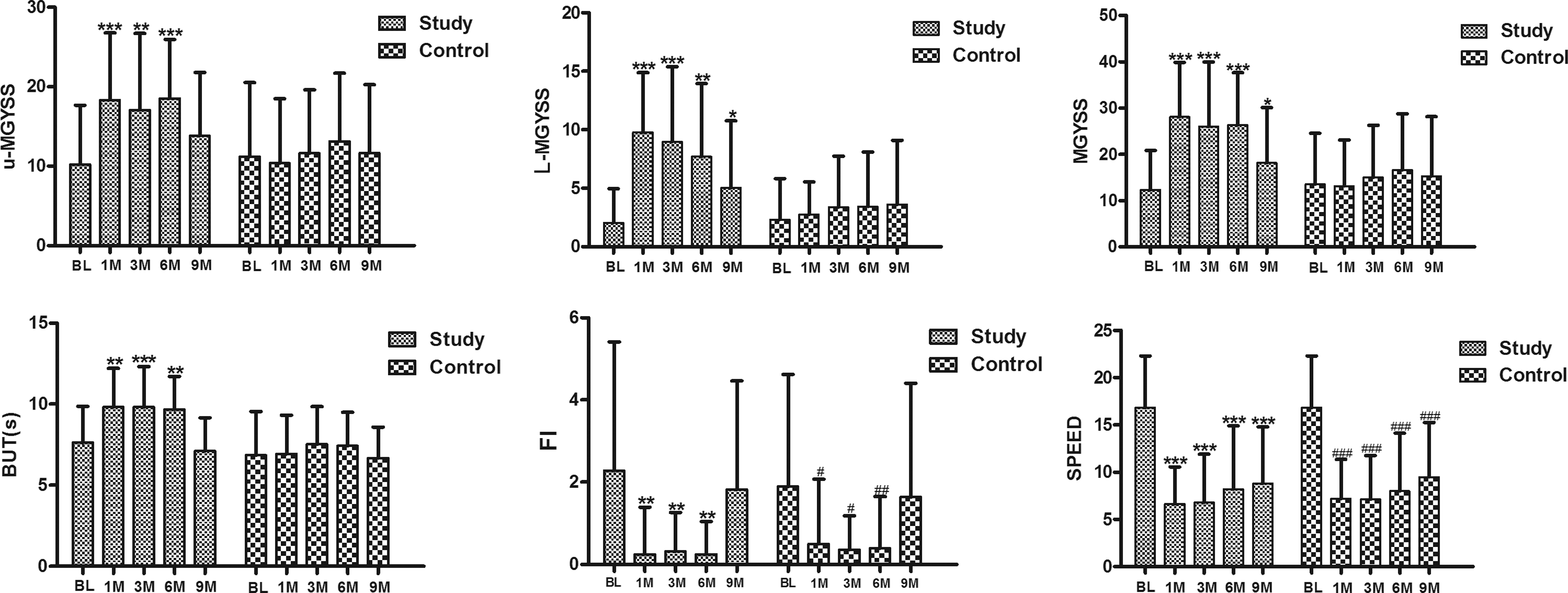
Longitudinal analysis of MGYSS, TBUT, SPEED scores, and CFS scores in the study and control eyes (*# p < 0.05, **## p < 0.01, ***### p < 0.001 compared to the baseline). CFS, corneal fluorescein staining; MGYSS, meibomian gland yielding secretion score; TBUT, tear film break-up time; SPEED, standard patient evaluation of eye dryness.
BL, baseline; CFS, corneal fluorescein staining; M, months; MGYSS, meibomian gland yielding secretion score; TBUT, tear film break-up time; SPEED, standard patient evaluation of eye dryness.
The l-MYGSS also did not differ between the study eyes (2.04 ± 2.937) and the control eyes (2.32 ± 3.497) at baseline (p = 0.775). In the study eyes, the l-MYGSS significantly increased at 1, 3, 6, and 9 months after treatment (p < 0.05). In the control eyes, the l-MGYSS showed no significant improvement after treatment (p > 0.05; Fig. 2). The changes in l-MYGSS after treatment were significantly higher in the study eyes than in the control eyes at 1, 3, and 6 months (p < 0.001), but no difference was seen at 9 months (p = 0.127; Table 1). The percentage improvement compared to the baseline in l-MGYSS at 1, 3, 6, and 9 months after treatment was 377.9%, 339.7%, 278.4%, and 147.0%, respectively, while that in u-MGYSS was 79.4%, 67.2%, 81.2%, and 35.4%, respectively (Table 1).
Secondary outcome measures
Tear film break-up time
The results of TBUT are presented in Fig 2 and Table 1. At baseline, TBUT did not differ between the study (7.64 ± 2.231 sec) and control eyes (6.86 ± 2.690 sec; p = 0.088). In the study eyes, TBUT significantly increased compared to the baseline at 1, 3, and 6 months after the treatment (p < 0.01, < 0.001, 0.01, respectively). TBUT values returned to baseline at 9 months (p > 0.05). In the control eyes, TBUT showed no significant improvement after treatment (p > 0.05; Fig. 2). The changes in TBUT were significantly higher in the study eyes than in the control eyes at 1, 3, and 6 months after treatment (p = 0.001, 0.003, 0.005, respectively), but no difference was observed at 9 months (p = 0.759; Table 1).
SPEED score
Statistically significant improvements in SPEED scores were observed in both the study and control eyes after treatment at each assessment time point (p < 0.05; Fig. 2). There were no significant differences in SPEED scores between the study and control eyes (Table 1).
CFS score
Statistically significant improvements in CFS scores were observed in both the study and control eyes until 6 months after treatment (p < 0.05; Fig. 2). Moreover, the CFS scores did not differ between the study and control eyes (Table 1).
Discussion
In this study, IPL treatment applied directly on the eyelids combined with MGX provided sustained relief for at least 6 months to MGD patients by improving meibomian gland secretion function, increasing TBUT, and improving symptoms and the ocular surface.
MGD is a common cause of evaporative dry eye and a highly prevalent ocular surface disease. Current therapeutic approaches for MGD include physical treatments (like eyelid margin hygiene, eyelid hot compresses, MGX), drug therapy (artificial tears, anti-inflammatory drops, topical or oral antibiotics), and dietary therapy. 4,5 However, the effects of these treatments are transient and unsatisfactory, and thus, new therapeutic methods must be developed.
Since Dr Toyos first noticed an improvement in MGD/dry eye symptoms in a patient who underwent IPL treatment for rosacea, some retrospective and a few prospective studies have confirmed that IPL could safely and effectively relieve the signs and symptoms of MGD and related dry eye. 8 –14 Due to safety concerns, IPL was only applied on the cheeks adjacent to the lower eyelid under eye shield protection in these studies. 8 –14 Further, these studies only evaluated the immediate and short-term effects of IPL treatment. The long-term efficacy of IPL treatment has not yet been studied.
In our previous study, we modified the IPL treatment method by applying IPL directly on both the upper and lower eyelids with full protection and after MGX. The short-term results showed that IPL on the eyelids combined with MGX was safe and yielded effects more rapidly. 18
To further evaluate the long-term efficacy of IPL treatment applied directly on the eyelids combined with MGX in MGD patients and to identify evidence for determining the retreatment period, we followed up the patients in our previous study for 9 months after the therapy. We found that both u-MGYSS and l-MGYSS significantly improved in the study eyes at 1, 3, and 6 months after the treatment. At 9 months, the l-MGYSS continued to improve, while the u-MGYSS showed no further improvement after the initial treatment. These results indicated that the treatment effects could last for at least 6 months. It is worth noting that the u-MGYSS was five times higher than the l-MGYSS at baseline. This is consistent with the results of other studies, which have shown that meibomian gland loss is more obvious in the lower eyelids than in the upper eyelids. 23,24 These results may be attributable to gravity leading to meibum stagnation in the glandular ducts and orifices in the lower eyelid. 23,24 Further, in the tear gradient theory proposed by Bron 25 et al., tear evaporation leads to an increase in solute concentration, including pro-inflammatory protein concentration in the tear meniscus. The resultant protein accumulation is related to MGD formation. The tear meniscus in the upper eyelids is smaller than that in the lower eyelids due to gravity and eyelid movement and, consequently, contains fewer inflammatory factors. The results of our previous study showed decreased inflammatory factors in the tear film after IPL treatment in MGD patients. 26 Maybe reducing the accumulation of inflammatory molecules is the reason why IPL treatment is more effective for the lower eyelids.
In our study, the percentage improvement compared to baseline in the l-MGYSS was 377.9%, 339.7%, 278.4%, and 147.0% at 1, 3, 6, and 9 months after the treatment, respectively, while the corresponding improvements in the u-MGYSS were 79.4%, 67.2%, 81.2%, and 35.4%. As the percentage improvement in the l-MGYSS at 9 months was still 147%, we conclude that a series of three IPL treatments combined with MGX produced a greater improvement in meibomian gland secretion function in the lower eyelids than in the upper eyelids.
The TBUT results were similar to the MGYSS results. TBUT was improved in the study eyes at 1, 3, and 6 months and did not improve further at 9 months, indicating that the treatment effects lasted 6 months after treatment. Significant improvement in CFS scores was observed until 6 months after the treatment, but this improvement did not differ between the study and control eyes. This may be because MGX itself is also effective in helping to repair the corneal surface.
Interestingly, we found a statistically significant improvement in SPEED scores until 9 months after treatment, and the improvement did not differ between the study and control eyes. This may be attributable to two reasons: (1) MGX itself is also effective in relieving the symptoms of MGD and related dry eye; and (2) the SPEED questionnaire is a subjective survey, and our study was designed as a double-blind study. We found that the results of a recently published prospective and placebo-controlled study of IPL treatment for MGD conducted by Craig et al. 12 were similar. Although only one eye was treated with IPL, and the other served as a control, SPEED scores improved to similar degrees in both eyes. So there may exist a complicated connection between the signs and symptoms of MGD and related dry eye; psychological effects may also have had an impact. At present though, this finding is difficult to explain, and further investigation is required.
The long-term results of the present study combined with the short-term results of our previous study show that IPL treatment applied directly on the eyelids combined with MGX is safe, effective, and provides rapid and sustained relief (for at least 6 months) to MGD patients by improving meibomian gland secretion function, increasing TBUT, and improving symptoms and the ocular surface. Thus, this treatment is a novel alternative for MGD patients. The exact mechanisms underlying the observed effects of the treatment are unclear. Thermal effect seems to be the least impactful component of IPL treatment, because it could only explain short-term effects but not long-term effects if it works. 27
This study also provided an initial recommendation for the IPL retreatment period. On average, the therapy may need to be repeated at 6 months after three consecutive IPL treatments applied directly on the eyelids combined with MGX.
There are some limitations in this study. First, some patients were lost to follow-up due to various reasons. Only 28 patients completed the assessments; this might cause potential study bias and affect the representativeness of our sample. The sample size should be enlarged, and the loss to follow-up rate should be reduced in future studies. Second, the number of treatment sessions was fixed, and the treatment energy range (14–16 J/cm2) was relatively limited, which may have influenced the treatment outcomes. More personalized treatment will require adjustments to the IPL parameters/protocol to maximize the outcomes for different skin types, MGD severity, patient feedback, etc.
Conclusions
Three consecutive IPL treatments applied directly on the eyelids combined with MGX effectively and safely improved meibomian gland secretion function and increased TBUT in MGD patients, and these effects lasted 6 months after the treatments. The improvement in meibomian gland secretion function was greater in the lower eyelid than in the upper eyelid. IPL treatment directly on the eyelids combined with MGX provides a novel alternative for MGD treatment with relatively long-term effectiveness.
Summary
IPL therapy applied directly on the eyelids combined with MGX treated MGD effectively in a relatively long term.
Footnotes
Author Disclosure Statement
The authors have no potential conflicts of interest and financial support to disclose.