
Abstract
Objective:
The aim of this study was to evaluate and compare the reparative and inhibitory effects of a light-emitting diode-mediated photobiomodulation (PBM) and of a low-intensity pulsed ultrasound (LIPUS) on orthodontically induced inflammatory root resorption (OIIRR).
Materials and methods:
Forty-nine Wistar rats were divided into four groups: untreated group (negative control), group treated with orthodontic appliances (positive control), PBM-treated group (wavelength: 618 nm, output power density: 20 mW/cm2), and LIPUS-treated group (frequency: 1.5% ± 5% MHz, pulse repetition ratio: 1.0% ± 10% kHz, effect area: 3.88% ± 1% cm2 and intensity: 30% ± 30% mW/cm2). OIIRR was induced experimentally in rats for 14 days with an applied force of 100g, and therapeutic approaches were performed concurrently. At the end of the experiment, upper first molar teeth of rats were prepared for genetic analysis, scanning electron microscopy, hematoxylin and eosin staining, and tartrate-resistant acid phosphatase staining. Kruskal–Wallis and post hoc Dunn's tests were performed.
Results:
Number of osteoclasts (p < 0.01), number of resorption lacunae and resorption area ratio (p < 0.001) decreased and number of total cells (p < 0.001) increased with the PBM and LIPUS applications when compared with the positive control group. Receptor activator of nuclear factor kappa B ligand (RANKL) levels of PBM and LIPUS groups were lower (p < 0.001), and osteoprotegerin (OPG) levels were higher (p < 0.001) than the positive control group. Cyclooxygenase-2 (Cox-2) expression significantly decreased with LIPUS and PBM administrations (p < 0.05). No significant difference was observed among PBM and LIPUS groups.
Conclusions:
PBM and LIPUS applications showed marked inhibitory and reparative effects on OIIRR by modulating the OPG/RANKL ratio, Cox-2 expression, and cell differentiation of osteoblasts and osteoclasts.
Introduction
O
PBM, also known as low-level laser (LLL) therapy, has become a widespread method in medicine and dentistry due to its biostimulating effects on metabolic activity. The LLL and LED sources that generate near-infrared radiation, are accepted therapeutic tools due to their beneficial effects on collagen synthesis, osteoblast proliferation, enhanced tissue regeneration, and wound healing. 1,3 It was proven that LED lights with physical characteristics of wavelengths within the far-red to near-infrared range (600–1000 nm), and a minimal energy density of 4 J/cm 2 , could be used to stimulate the photoreceptor cytochrome c oxidase, which mediates ATP production. 4
LIPUS provides formative and reparative effects on tissues, 5,6 and an acceleration of wound healing by enhancing permeability of cellular membranes and blood vessels, intracellular massage, cellular pressure, and angiogenesis stimulation effects. 7 The reparative effect of LIPUS on hard tissues is achieved through the piezoelectric effect with the support of other athermal effects, such as microstream and acoustic stream in addition to an anti-inflammatory action. 7
Both PBM and LIPUS have been shown to exert reparative effects at the celluler level on cementoblasts and odontoblasts, like osteoblasts. 5,8
Although current literature has demonstrated some of the beneficial effects of PBM and LIPUS on OIIRR, the comparison of the therapeutic effects of PBM and LIPUS on repair and/or the prevention of OIIRR at the molecular, cellular, and macroscopic levels have not been investigated before. Evaluation of the reparative alterations at the level of cellular initiators such as mRNA expression of osteoprotegerin (OPG), receptor activator of nuclear factor kappa B ligand (RANKL), and cyclooxygenase-2 (Cox-2) may offer detailed explanation for the cellular metabolism of PBM and LIPUS applications. Therefore, the aim of this study was to evaluate and to compare the reparative and/or inhibitory effects of PBM and LIPUS applications on OIIRR in rats through real-time polymerase chain reaction (PCR) analysis, scanning electron microscopy (SEM) analysis, hematoxylin and eosin staining and TRAP staining analyses.
Materials and Methods
The experiment protocol was approved by The Local Ethics Committee for Animal Experiments of Erciyes University (approval number: 11/136).
Animals in groups
Forty-nine healthy, 12-week-old male Wistar rats, with an average weight of about 252.9 ± 10.7g, were divided randomly into four groups. The rats of the negative control group (n = 7) received no treatment while the positive control group (n = 14) was subjected to high orthodontic forces only. The PBM-treated group of animals (n = 14) and the LIPUS subjected animals (n = 14) received high orthodontic forces and therapeutics during the 14 day experiment. The rats were fed with a standard pellet diet and tap water ad libitum.
Appliance design
Rats were anesthetized with an intraperitoneal injection of 1.0 mg/kg ketamin hydrochloride (Gedeon Richter Ltd., Budapest, Hungary) and 0.5 mg/kg xylazine (Rompoun Bayer, Leverkusen, Germany) combination. Orthodontic force-loading was achieved by a modified technique described by Brudvik and Rygh (Fig. 1). 9 Ni-Ti coil springs (The International Orthodontics, Houston) were attached to the upper first molars and incisor teeth of rats. The springs were activated to deliver a force of 100g, 10 as checked during experimentation.
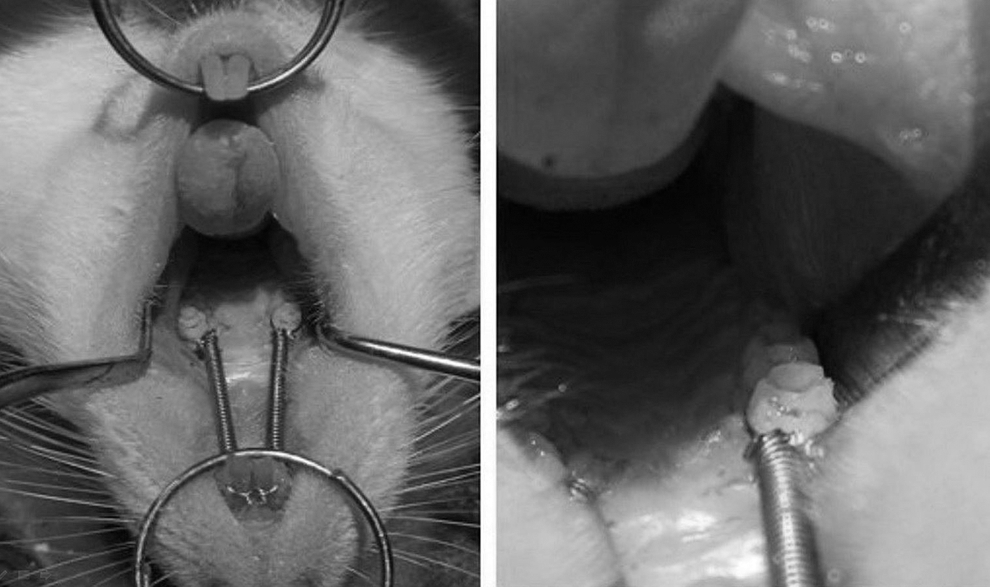
The experimental design for orthodontically induced root resorption on rats. Ni-Ti closed coil spring along between the upper incisor and upper first molar teeth.
LED-mediated PBM therapy
The PBM group of animals received PBM by using an OsseoPulse® LED device (Biolux Research Ltd., Vancouver, Canada) for 20 min/d in 14 days. The wavelength of the LED device was 618 nm and the output power density was 20 mW/cm 2 . Irradiation was applied transcutaneously for 10 min on the right and for 10 min on the left side. Energy density of 12 J/cm 2 was obtained within the related region (Table 1). Immobility of the test animal was provided by general anesthesia for 20 min in total. 1
Light-Emitting Diode Device Parameters
Low-intensity pulsed ultrasound therapy
The LIPUS group of animals was treated 30 min/d for 14 consecutive days with a Sonic Accelerated Fracture Healing System (SAFHS; Exogen, Smith Nephew) device at a frequency of a 1.5% ± 5% MHz, 1.0% ± 10% kHz pulse repetition ratio, 3.88% ± 1% cm 2 effect area, and 30% ± 30% mW/cm 2 intensity. During the applications, the animals' heads were fixed for 15 min at the right and for 15 min at the left side. 6 Transducer device was brought into contact with the cheek skin at the upper first molar teeth.
All animals were euthanized at the 15th day using an overdose of anesthetic (200 mg/kg sodium-pentobarbital pentol, Abbot, ABD).
Histological preparation and histomorphometric evaluation
Right and left tooth-bearing segments of the maxilla were dissected and fixed in 10% formalin. After the histological procedures, the mesiobuccal root of the first molars were sectioned serially at 5-μm intervals and stained with hematoxylin and eosin (H&E; Fig. 2) and tartrate-resistant acid phosphatase (TRAP; Fig. 3).

Histological findings of hematoxylin-eosin staining of mesiobuccal root of the upper first molar teeth on sagittal plane in the PC
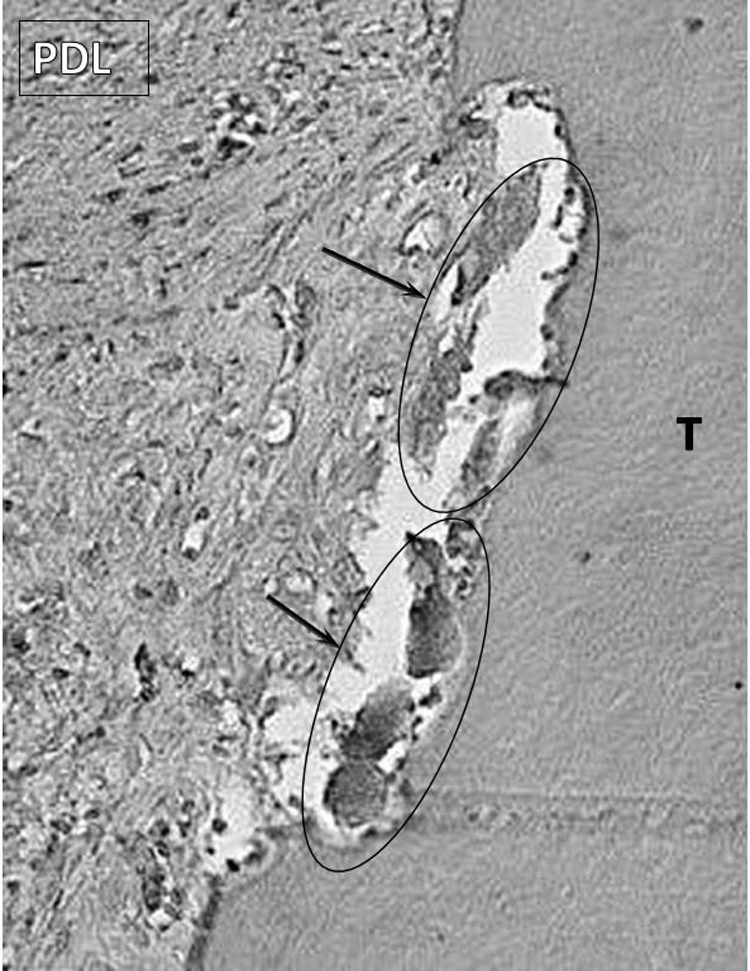
TRAP staining of mesiobuccal root of the upper first molar teeth on sagittal plane in control group sample indicate osteoclastic cells (TRAP+) in resorption lacunae ( × 200). Arrows indicate the areas including osteoclastic cells. PDL indicates periodontal ligament, T, tooth; TRAP, tartrate-resistant acid phosphatase.
A grid superimposition method was used to calculate the percentage of root resorption, number of total cells [stainable periodontal ligament (PDL) cells], and number of osteoclastic cells of PDL on H&E and TRAP staining images. 11 The resorption area ratio (RAR) was calculated through dividing the number of grids overlapped with resorption lacunae by the grids of the entire root surface excluding the pulp area. 11 Bigger grids were used for calculating the number of total cells of PDL. The TRAP staining slides were evaluated in the same histomorphometric analysis method with the H&E slides.
Preparation of specimens for SEM
The right and left upper first molar teeth were cut as a block, including its surrounding bone and the alveolar bone, which was removed gently to prevent root surface damage. The teeth were submerged in 1% sodium hypochlorite. The specimens were centrifuged at 1000 rpm and were dried for 1 week in a 40°C incubator, then were placed on a retainer, plated with gold, and observed with an SEM LEO 440 device (SEM; Leo 440; M/s Leo Electron Microscopy, Cambridge, UK). Examinations were performed on the mesial surfaces of the mesio-buccal roots of the maxillary first molars at 100 × magnification (Fig. 4) and measurements were performed with ImageJ (1.47v; Java1.6.0, Research Services Branch). Meanwhile, 300 × , 500 × , and 1000 × magnification views were also examined to identify the repaired cement layers (Fig. 5).
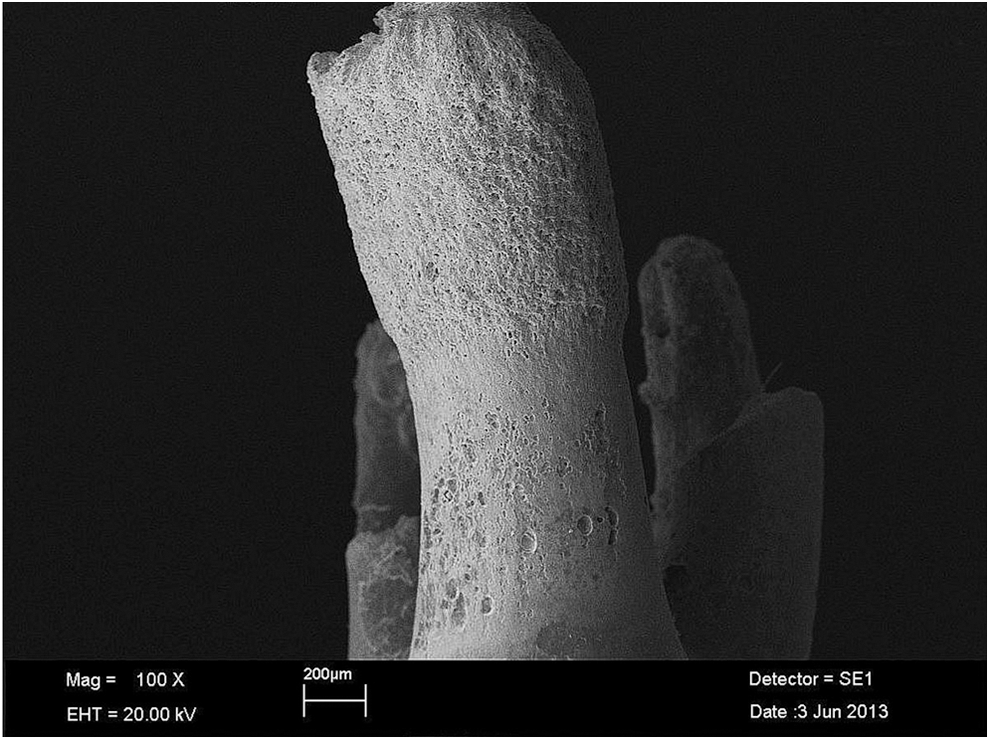
The resorption area evaluation on the SEM images of the mesio-buccal root's surfaces of the control group rats' maxillary first molars at 100 × magnification. SEM, scanning electron microscopy.
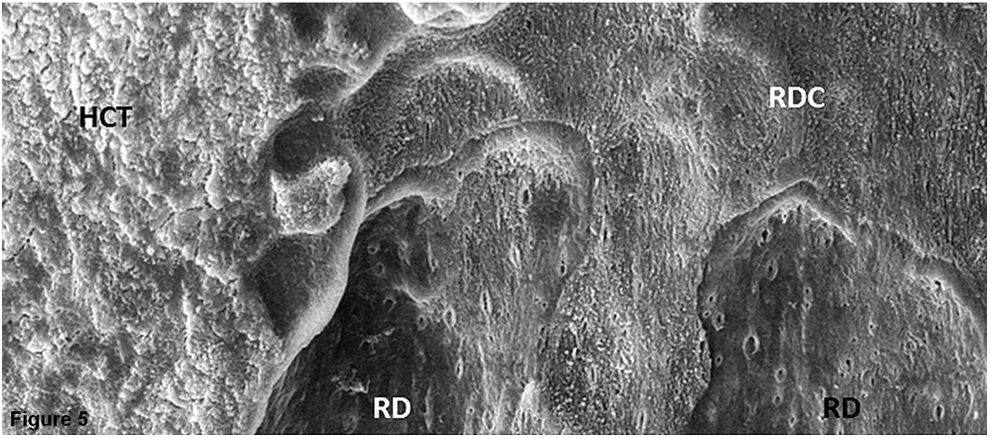
The resorption image on SEM analysis. RDC indicates resorptions progressed to the dentin-cement border; RD, resorptions deepened into the dentin. HCT, healthy cement tissue.
The percentages of root resorption were calculated through the proportion of resorption lacunae area and the whole root surface area, and were evaluated as the SEM RAR.
Determining the expression levels of OPG, RANKL, and Cox-2
The extracted teeth containing PDL tissue on their roots were placed in a mRNA fixation solution. RNA were isolated from samples using a QIAamp RNA Blood Mini Kit (QIAGEN–52304). Tooth samples were homogenized in 300 μL Buffer RTL-β-Mercaptoethanol mix for 3 min and nonhomogenized tooth materials were removed. RNA isolates were dissolved in 30 μL RNase-free water. cDNA was synthesized from RNA isolates with a First Strand cDNA Synthesis Kit (K1612; Thermo Scientific). The obtained material was analyzed with real-time PCR [Rotor-Gene Q 6plex (QIAGEN, Valencia, CA)] for OPG, RANKL, and Cox-2 mRNA expression assessment using ACTB house keeping gene for the internal control (Table 2).
Primers and Probes Used in Real-Time Polymerase Chain Reaction
Cox-2, cyclooxygenase-2; OPG, osteoprotegerin; RANKL, receptor activator of nuclear factor kappa B ligand.
Statistical analysis
All statistical analyses were performed using the Statistical Package for Social Sciences v.20.0 program (SPSS for Windows; SPSS, Inc., Chicago, IL). The Shapiro-Wilk W test was used to test the data for normality. Since data were not normally distributed, the comparisons of the parameters among groups were performed using Kruskal–Wallis test and for the multiple comparisons, post hoc Dunn's test was used. Differences were considered to be significant when p < 0.05.
Results
Histological and histomorphometric analyses
The histomorphometric analyses showed that LIPUS and PBM applications increased the number of total cells in the PDL significantly when compared with the positive and negative control groups (p < 0.001). There was no statistically significant difference between cellular proliferation levels regarding LIPUS and PBM applications (Fig. 6).

Bar graph representation of number of total cells (mean/SD) in LIPUS, LED-mediated PBM, PC, and NC groups, different letters indicate statistically significant differences among groups at significance level of p < 0.001.
The highest RAR value was observed at positive control group while LIPUS and PBM decreased RAR significantly (p < 0.001, Fig. 7). Similarly, the number of resorption lacunae (NRL) values were observed to be lower in the LIPUS and PBM groups when compared with the positive control group (Fig. 8). The reparative and/or inhibitory effects of the LIPUS (RAR: 0.04 ± 0.02, NRL: 3.0 ± 0.02) and PBM (RAR: 0.04 ± 0.02, NRL: 2.86 ± 0.7) applications were found to be at similar levels in terms of the RAR evaluations (Table 3).
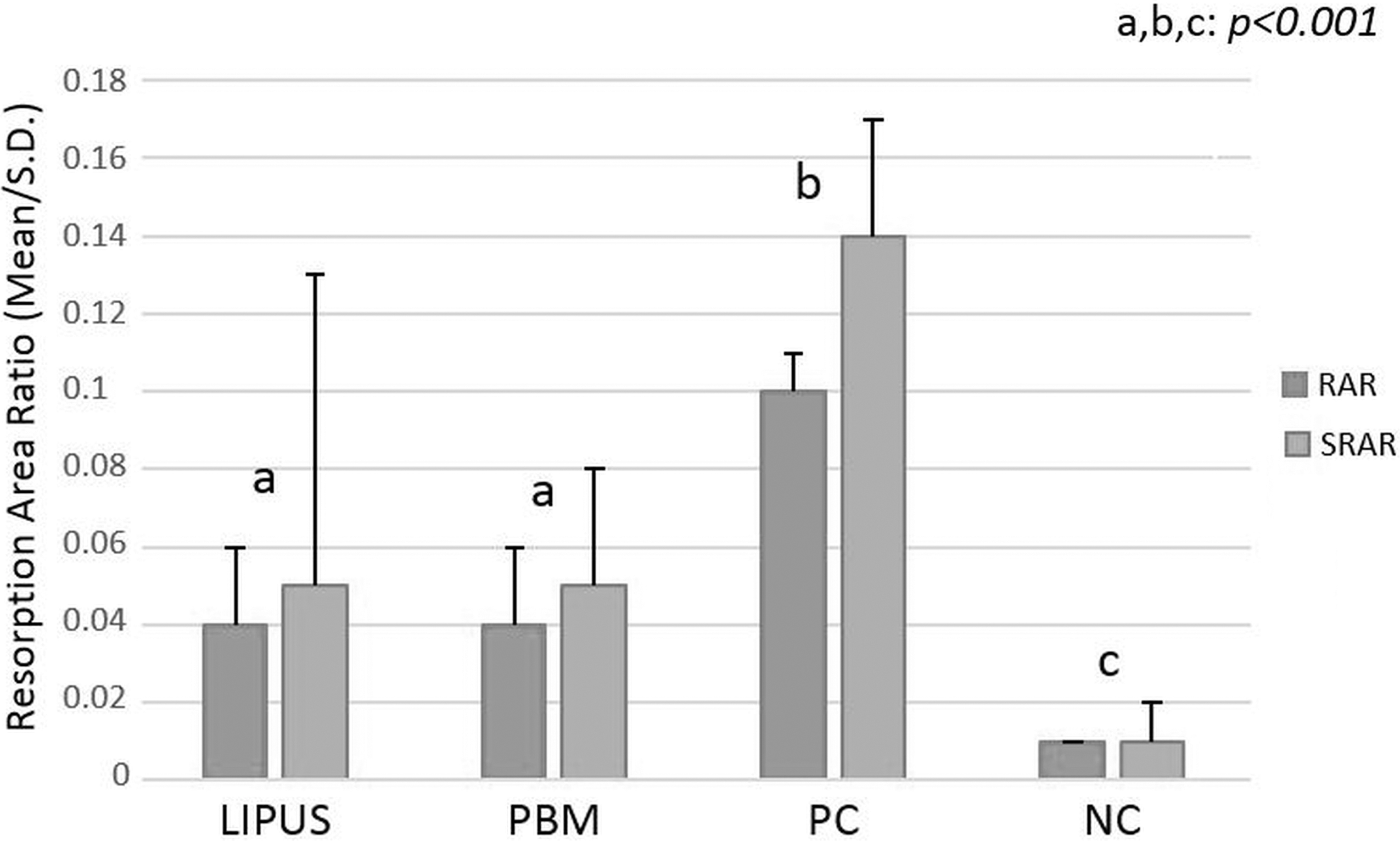
Bar graph representation of RAR (mean/SD) and SEM resorption area ratio (SRAR, mean/SD) in LIPUS, LED-mediated PBM, PC, and NC groups, different letters indicate statistically significant differences among groups at significance level of p < 0.001. LIPUS, low-intensity-pulsed ultrasound; NC, negative control; PBM, photobiomodulation; PC, positive control; RAR, resorption area ratio.
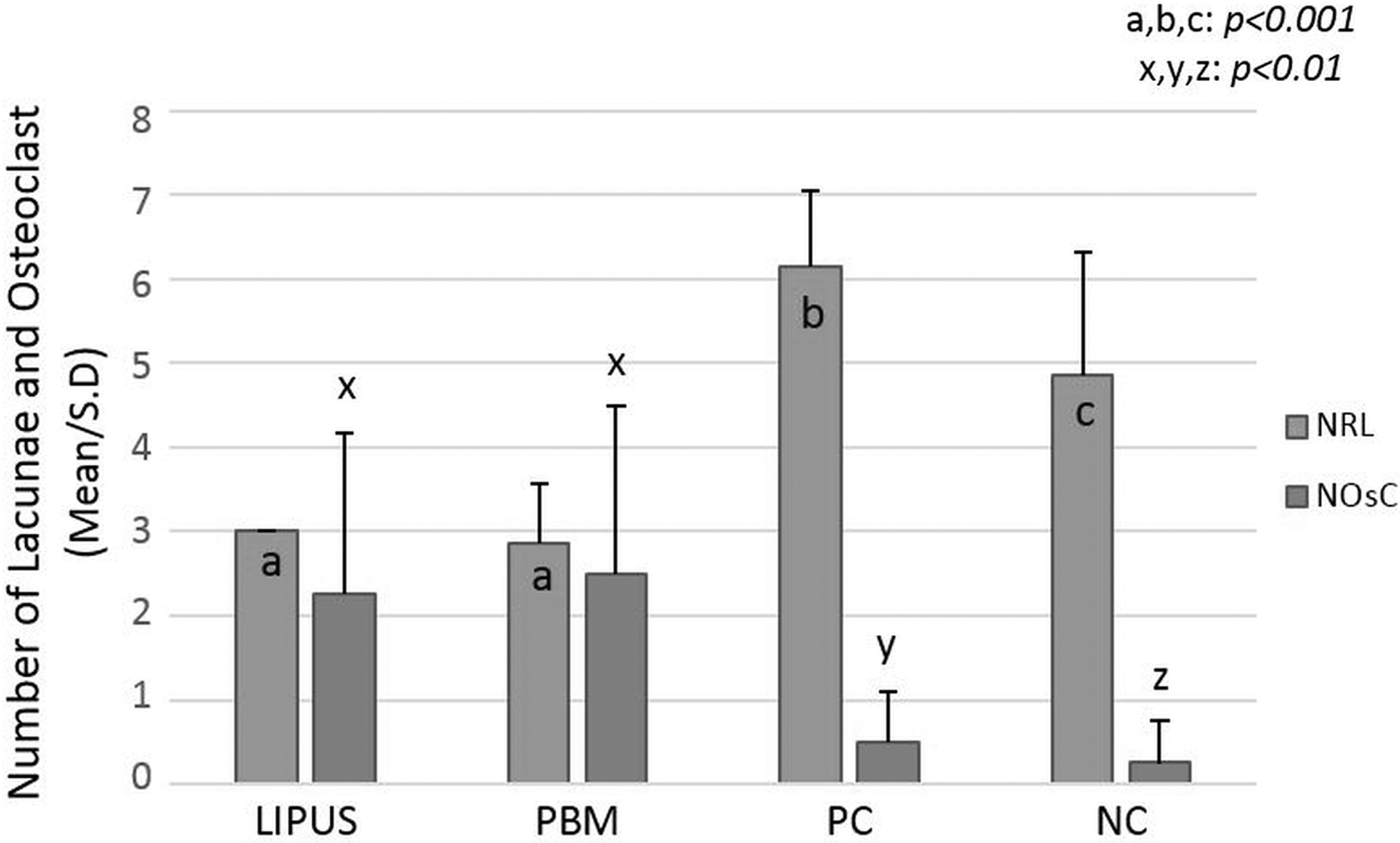
Bar graph representation of number of lacunae (NRL, mean/SD) and number of osteoclastic cell (NOsC, mean/SD) in LIPUS, LED-mediated PBM, PC, and NC groups, different letters indicate statistically significant differences among groups at significance level of p < 0.001 for a,b,c, and significance level of p < 0.01 for x,y,z. LIPUS, low-intensity-pulsed ultrasound; NC, negative control; PBM, photobiomodulation; PC, positive control.
Comparison of Variables Between Groups
There is statistically significant difference at p < 0.05.
Groups with different letters are significantly different from each other.
Cox-2, cyclooxygenase; LIPUS, low-intensity-pulsed ultrasound; NC, negative control; NOsC, number of osteoclastic cell; NRL, number of resorption lacunae; NTC, number of total cell; OPG, osteoprotegerin; PBM, photobiomodulation; PC, positive control; RANKL, receptor activator of nuclear factor kappa B ligand; RAR, resorption area ratio; SEM, scanning electron microscopy; SRAR, SEM RAR.
Except the negative control group, all groups displayed osteoclasts or osteoclastic cytoplasm at the PDL as a result of TRAP staining. The TRAP results indicated that significantly fewer cells stained positive in the LIPUS and PBM-treated groups than in the positive control group (p < 0.01, Table 3, Fig. 8). The osteoclastic concentration was higher at the alveolar area in the LIPUS and PBM-tested groups, while osteoclasts were located at the root surface in the positive contol group.
SEM analysis
The resorption lacunae ratio investigated with the SEM analysis showed that the positive control group (0.14 ± 0.03) had the highest value, while the lowest value was observed in the negative control group (0.01 ± 0.01). The reparative and/or inhibitory effects of the LIPUS and PBM treatments were similar, as stated in the SEM RAR evaluation (Table 3, Fig. 7).
Expression levels of OPG, RANKL, and Cox-2
OPG mRNA levels significantly increased with LIPUS and PBM applications when compared with the positive and negative control groups (p < 0.001, Fig. 9). The highest RANKL expression was observed in the positive control group because of the higher orthodontic force (Fig. 9). However, LIPUS and PBM decreased RANKL expression when compared with the positive control group. The degrees of Cox-2 expression also significantly decreased with LIPUS and PBM administrations at similar levels (p < 0.05, Table 3, Fig. 9).

Bar graph representation of OPG, RANKL, and Cox-2 mRNA expression (mean/SD) in LIPUS LED-mediated PBM, PC, and NC groups, different letters indicate statistically significant differences among groups at significance level of p < 0.001 for a,b,c and significance level of p < 0.05 for x,y,z. Cox-2, cyclooxygenase-2; LIPUS, low-intensity-pulsed ultrasound; NC, negative control; OPG, osteoprotegerin; PBM, photobiomodulation; PC, positive control; RANKL, receptor activator of nuclear factor kappa B ligand.
Discussion
During the orthodontic treatment, severe root resorption cases may force the clinician to focus on repairing and/or inhibiting of OIIRR more than many other priorities. In this situation, selection of the most effective modality for repairing and/or inhibiting of OIIRR may become a main requirement for clinicians.
The results of the present study demonstrated that the number of cells at the PDL increased with the application of PBM through the biostimulation of cell proliferation. At the same time, the number of osteoclasts in the PBM group was fewer than in the positive control group, which supports the assumption that increasing cells were nonresorptive cells. Ozawa et al. 3 found that PBM application stimulates proliferation and differentiation of osteoblasts from precursor cell lines, which is consistent with the result of the present study with increased cell number. Also, Fonseca et al. 2 reported an increase in fibroblastic cells with the PBM application in the root resorption model on rats.
Further, in the PBM group OPG mRNA levels were found to be higher while RANKL and Cox-2 levels were lower. The higher OPG level supports the enhancement of osteoblast proliferation through the positive effects of this biomarker. On the other hand, the lower RANKL and Cox-2 levels may explain the lower osteoclast cell count because of their biological functions. Xu et al. 12 investigated the effects of PBM on calvarial bone cells and reported enhanced OPG, declined RANKL mRNA levels, and increased osteoblast proliferation, in addition to decreased osteoclastogenesis caused by altering the related biomarker levels. Fujita et al. 13 and Altan et al. 14 investigated the effects of PBM application on the orthodontic tooth movement rate, and they reported a response of accelerated tooth movement due to increased RANK and RANKL levels. These different periodontal tissue responses to the PBM applications can be attributed to different experimental designs and expecting different therapeutic responses from PBM. In our study, higher forces than the optimal force limits that were not suitable for orthodontic tooth movement were applied to create experimental root resorption on teeth. This experimental root resorption model, which was not setup for orthodontic tooth movement, is not proper to assess the effects of treatment modalities on the rate of tooth movement. When an appropriate force level for tooth movement is applied without causing a destructive inflammatory process, the metabolic activity may rise to accelerate orthodontic tooth movement, and osteoclastic activity may increase to such an extent that the tissues can not be damaged. However, in inflammatory root resorption models, severe or intolerable forces already begin to damage related tissues. In this situation, PBM biostimulation may serve as an inhibitor of inflammation or the protection mechanism for those related tissues. The anti-inflammatory effects of PBM applications were also reported previously. 15 Findings show that the PGE2, TNF, IL 1b, and and Cox-2 levels declined due to the anti-inflammatory effect of PBM. 15 Also as a result of the present study, osteoclasts were observed to be usually close to the alveolar bone margins instead of the root surface areas. This situation gives rise to the thought that cellular activation was redirected to reduce the destruction effect of high orthodontic forces on root surfaces and the repositioning of existing cell groups were interpreted with anti-inflammatory effect of PBM.
The results of Kim et al. 16 also support this anti-inflammatory effects of PBM application. They found that periodic PBM application after corticision around a moving tooth decreased the tooth movement rate because of increased osteoblastic and decreased osteoclastic activity while PBM increased osteoclastic activity in the normal orthodontic tooth movement group. 16 These results suggest that PBM may accelerate metabolic activity in the direction of metabolic requirements. The reparative and/or inhibitory effects of the PBM application on OIIRR were observed with clear results regarding decreased resorption areas and resorption lacunae numbers. The findings of Fonseca et al. 2 also demonstrated that LED-mediated LLLs decreased the RAR when compared with the control group.
The results of this study revealed a significantly higher PDL cellularity in the LIPUS-treated group. This result is consistent with the findings of Dalla-Bona et al. 5 and Inubushi et al., 6 which indicated increased proliferation and differentiation of cementoblasts, enhancing OPG, collagen, and alkalen phospatase expressions. Increased OPG mRNA levels also support the enhanced numbers of total cell consistently with previous studies. 5,17,18 In addition, the decreased number of osteoclasts, reduced RANKL and Cox-2 mRNA levels in the LIPUS-treated group were also similar to the findings in literature. 17,18 Increased reparative cell numbers and decreased osteoclastic cells should provide inhibitory and/or reparative influences through LIPUS by its anabolic effects on OIIRR. 5,6 As expected, the reduced resorption lacunae and RARs on the histological slides and the SEM examinations were observed to have significantly different results than in the control groups. Liu et al. 17 suggested that the LIPUS application regulates osteoclast differentiation and stimulates a reparative effect on orthodontically induced root resorption in rats. El-Bialy et al. 19 and Al-Daghreer et al. 20 also reported a significant decrease in the areas of resorption and the NRL in the LIPUS-exposed teeth.
In summary, the reparation and inhibition of OIIRR provided by LIPUS and PBM applications were found similar in the investigated aspects. This result may be explained such that different external energy transfer via photons or acoustic waves created similar biological stimulation with the appropriate dosages and application methods. If future clinical studies support these experimental findings, clinicians may prefer the appropriate one from these modalities for their clinic usage according to ease of supply, ease of administration, or cost regardless of their reparative efficacy.
Conclusions
The applications of LED-mediated PBM and low-intensity pulsed ultrasound have similar reparative and inhibitory effects on OIIRR in rats with regulating the OPG/RANKL ratio, Cox-2 expression, osteoblastic, and osteoclastic activity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.