
Abstract
Objective:
This proof-of-concept study was to investigate the relationship between photobiomodulation (PBM) and neuromuscular control.
Background:
The effects of concussion and repetitive head acceleration events (RHAEs) are associated with decreased motor control and balance. Simultaneous intranasal and transcranial PBM (itPBM) is emerging as a possible treatment for cognitive and psychological sequelae of brain injury with evidence of remote effects on other body systems.
Methods:
In total, 43 (39 male) participants, age 18–69 years (mean, 49.5; SD, 14.45), with a self-reported history of concussive and/or RHAE and complaints of their related effects (e.g., mood dysregulation, impaired cognition, and poor sleep quality), completed baseline and posttreatment motor assessments including clinical reaction time, grip strength, grooved pegboard, and the Mini Balance Evaluation Systems Test (MiniBEST). In the 8-week interim, participants self-administered itPBM treatments by wearing a headset comprising four near-infrared light-emitting diodes (LED) and a near-infrared LED nasal clip.
Results:
Posttreatment group averages in reaction time, MiniBEST reactive control subscores, and bilateral grip strength significantly improved with effect sizes of g = 0.75, g = 0.63, g = 0.22 (dominant hand), and g = 0.34 (nondominant hand), respectively.
Conclusion:
This study provides a framework for more robust studies and suggests that itPBM may serve as a noninvasive solution for improved neuromuscular health.
Introduction
Approximately 3.8 million sport- and recreation-related concussions occur annually in the United States. 1 The effects of concussion, including persistent long-term issues with concentration and physical skills, 2,3 is a growing concern. Equally concerning are the effects of repetitive head impacts (RHIs), also known as repetitive head acceleration events (RHAEs). RHAE has the same meaning as RHI; however, it is emerging as a preferred term because it inherently indicates that the brain is experiencing translational and/or rotational movement because of external forces regardless of the source (blast or mechanical blow) or location (head or body) of the impact forces. Although RHAE may include concussions or mild traumatic brain injury (mTBI), most do not result in any acute detectable clinical symptoms. However, the cumulative effect of RHAE, like concussion or mTBI, could progress to traumatic encephalopathy syndrome (TES), a clinical disorder associated with chronic traumatic encephalopathy (CTE). 4 An athlete may experience over 100 RHAEs per season. 5 –7 Although the athlete may be asymptomatic, RHAEs result in microstructural and functional changes in the brain similar to that seen in concussion or mTBI, 8 –10 leading to altered motor unit recruitment strategies, increased acute corticomotor inhibition, 11 and other neuromuscular impairments, such as reduced dynamic balance or reaction time, in the long-term. 12 –16
Photobiomodulation (PBM), more specifically simultaneous intranasal and transcranial PBM (itPBM), is emerging as a candidate for therapy in addressing the cognitive and psychological sequelae resulting from brain injury. 17,18 In transcranial PBM (tPBM), a headset is worn with light-emitting diodes (LEDs) positioned on the scalp to target cortical brain regions with primarily near-infrared (NIR) light (810 nm). In intranasal PBM (iPBM), an LED nasal applicator is positioned in a nostril where NIR photons can be absorbed by the capillaries in the nasal epithelium.
Mechanisms of PBM
Theories and evidence describing the mechanism of action of PBM for both brain and other tissues and are well documented. 17 –30 The prevailing hypothesis is that itPBM alleviates mitochondrial dysfunction related to the head insults. 17,31 Specifically, emitted photons are absorbed by the cytochrome c oxidase (CCO) enzyme in the mitochondrial electron transport chain, 20,22,32 which leads to a cascade of biochemical events along several pathways. The end results include enhanced energy production, increased cerebral blood and lymphatic flow, 30,33 the promotion of cell survival, 32 reduced excitotoxity and inflammation, and potentially increased angiogenesis, neurogenesis, and synaptogenesis. 25,29 PBM also stimulates the proliferation and mobilization of stem cells that release trophic factors that protect and repair neural tissue. 34 –36 Another theorized mechanism is the entrainment of neuro-oscillatory waves disrupted by concussion 37 –39 because of the pulsation of the light. 40
Some of these mechanisms may exhibit effects beyond the target organs, implying that PBM may affect nontargeted body systems. Studies employing remote PBM resulted in increased mobility, cognition, dynamic balance, and sense of smell in patients with Parkinson’s disease, 41 and cognitive capacity, changes in depression, weight, and blood pressure in mouse models. 42 To date, literature on itPBM affecting other systems in a population with RHAE exposure is sparse. However, a case study including a former professional football player exhibiting TES not only showed brain functional improvements, 43 but also reported gains in physical strength (Personal Communication, L. Carr, Aug. 2019), implying that mechanisms of itPBM may demonstrate a systemic effect resulting in improved or preserved neuromuscular health.
The purpose of this study was to examine effects of itPBM on neuromuscular health. As part of a larger proof-of-concept study to investigate the relationship of itPBM on brain connectivity, cognitive function, and psychological health in individuals exposed to RHAE, measures of neuromuscular health, including reaction time, dexterity, grip strength, and balance, were collected in former athletes with a self-reported history of RHAE. Grip strength, reaction time, and postural control are functional biomarkers of health and tend to decline with age. 44 –48 Regardless of participant age, we hypothesized that the light-stimulated processes provide additional benefits to systems subserving physical performance measures.
Methods
Participants
We enrolled 49 participants (45 males). Six did not complete the study for various reasons (e.g., unable to travel or loss of interest), leaving 43 (39 male) participants between the age of 18 and 69 years old (M = 49.5, SD = 14.45). All participants self-reported a history of mTBI and/or RHAEs, most because of participation in sports (recreational, high school, collegiate, and/or professional), and one as a result of intimate partner violence. Participants also reported at least one complaint commonly associated with effects of head impacts, for example, difficulty with mood regulation, memory, or sleep. Exclusion criteria included a history of neurological disease (i.e., dementia, stroke, epilepsy, tumor), history of severe psychiatric disorder (i.e., bipolar, schizophrenia, psychosis), and/or MRI contraindications. All enrollees signed informed consent documents approved by the Institutional Review Boards at the University of Utah and Wahlen VA Salt Lake City Healthcare System.
We administered the Ohio State University Traumatic Brain Injury Identification (OSU-TBI), 49 survey, during which participants self-reported the duration of participation in the activity that exposed them to RHAEs and the severity and number of head hits. All participants reported head impacts with at least momentary (5–30 sec) loss of consciousness and/or posttraumatic amnesia. No participants disclosed a history of mild complicated, moderate, or severe TBI; however, most described experiencing head impacts such as “stingers” or “getting their bell rung,” which may have been considered concussions had they been diagnosed (see Table 1 for a summary).
Participant Information
Not a personal memory; based on a family story of the participant being hit by a truck as a toddler. No other details are known.
Study design
This study was a nonrandomized proof-of-concept design that used active treatment only. Participants were assessed at two time points, prior to and 8–10 weeks after starting at-home itPBM treatments. The participants were instructed to maintain their normal routines and not start any new activities (e.g., resistance and/or balance training or brain training) during this time period.
Treatment protocol
For this study, participants self-administered itPBM with the Vielight Neuro Gamma PBM headset (Toronto, Canada) worn over the scalp and/or hair. The device has four LEDs, each emitting NIR light (810 nm), pulsating at 40 Hz (50% duty cycle) over a beam spot of 1 cm2, three with irradiance of 100 mW/cm2, and the fourth at 75 mW/cm2. The LEDs are placed to target cortical nodes of the default mode network: the midline bilateral medial prefrontal cortex, left and right angular gyrus areas, and midline bilateral precuneus (see Fig. 1). In addition, the device includes an intranasal probe with one LED emitting pulsed NIR light with irradiance of 25 mW/cm2 inside the nasal cavity targeting the olfactory bulbs and orbitofrontal cortex (see Table 2). Participants were instructed to administer a 20-min treatment every other day for 8 weeks and given a log sheet to track usage.
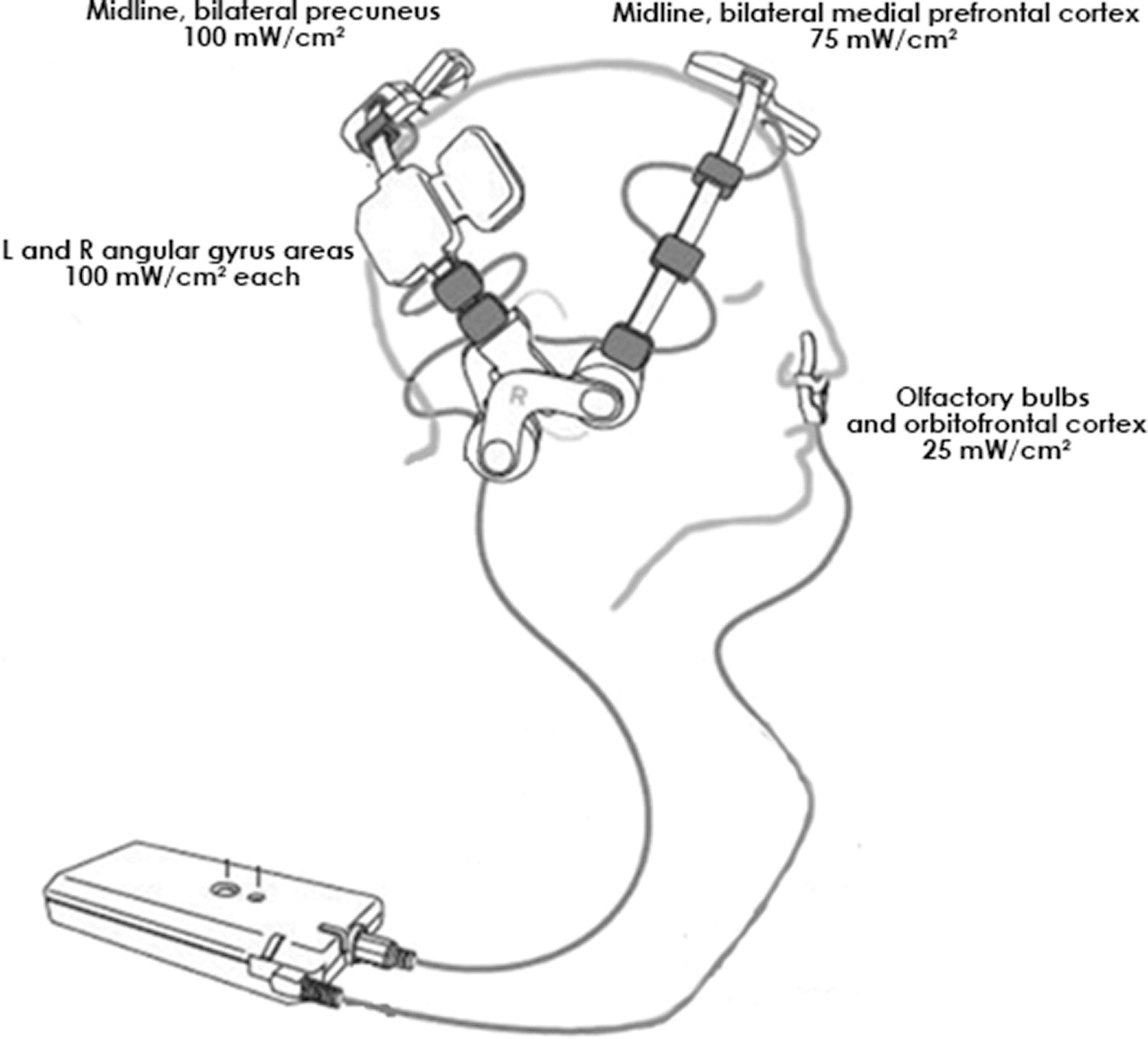
Placement of the itPBM device. The Vielight Neuro Gamma PBM headset fits over the scalp with the four near-infrared LEDs targeting cortical nodes of the default mode network: the medial prefrontal cortex, located high on the center front forehead area at the center front hairline; the bilateral parietal cortices located in the left and right angular gyrus areas; and the precuneus, located at the junction of the sagittal suture line with the left and right lambdoid suture lines. An intranasal applicator is positioned over capillaries in the nasal epithelium targeting olfactory bulbs and the orbitofrontal cortex. The headset’s four LEDs emit pulsed NIR light (810 nm), over a beam spot size of 1 cm2, three at an irradiance of 100 mW/cm2, and the fourth at 75 mW/cm2. The nasal applicator consists of one LED emitting pulsed NIR light at an irradiance of 25 mW/cm2. Image source: Vielight Neuro Gamma Operational Manual version 1.1; 17 April 2019, pg 8. Used with the permission from Vielight Inc. itPBM, intranasal and transcranial photobiomodulation; LED, light-emitting diode; NIR, near infrared
itPBM Specifications
itPBM, intranasal and transcranial photobiomodulation.
Clinical performance tests
The clinical performance tests included four assessments: clinical reaction time, grooved pegboard, grip strength, and the Mini Balance Evaluation Systems Test (MiniBEST). As previously noted, this study is part of a larger study; therefore, these assessments occurred in the same visit with cognitive and neuropsychological assessments and a brain MRI scan.
Clinical reaction time
The clinical reaction time test was administered according to the protocol described by Eckner et al., 50 Briefly, participants sat with the forearm of their dominant hand resting comfortably on a table and their hand extended past the edge of the surface with their thumb and fingers forming a “C,” similar to holding a cup. The examiner pinched one end of a 1.3-m-long marked stick embedded in a weighted rubber disk and suspended the disk between the fingers and thumb of the participant’s hand. The examiner released the stick and participant closed their hand to catch it as quickly as possible. The participant performed 10 total trials, with the first 2 used as practice. The distance the stick dropped was converted into a reaction time (in milliseconds) using the formula for a body falling under the influence of gravity (d = ½gt 2), where d is the distance, g is the acceleration due to gravity, and t is the time.
Grooved Pegboard Test
Manipulative dexterity was assessed using the Grooved Pegboard Test., 51 The metal board consists of 25 keyhole shaped slots with varying orientations, arranged in a 5 × 5 grid (Lafeyette Instruments, Lafayette, IN). Each peg has a 3-mm-diameter cylindrical shape, save for a ridge that runs along the length of the peg, such that the peg will only fit in the board if the ridge is aligned with the notch of a slot. Participants inserted pegs into the holes as quickly as possible in a row-by-row manner, completing the exercise once with each hand, starting with their dominant hand. We recorded the time the participants took to complete the task.
Grip strength
Grip strength was measured using a Jamar Plus Dynamometer (Performance Health, Chicago, IL). After adjusting the handle for proper grip, the participant held the dynamometer down at their side and squeezed the handle as hard as possible for 3 sec, completing three trials for each hand. We recorded the average force.
Mini Balance Evaluation Systems Test
The MiniBEST, 52 assessment includes 14 tasks across four domains: anticipatory postural adjustments, reactive postural control, sensory orientation, and dynamic gait., 53 Each task used a three-level ordinal scale to score, with a maximum total score of 28. Outcome measures included the overall miniBEST score and individual subscores for each domain.
Statistical analysis
Motor tests were scored per their respective standards. Data from some participants were excluded because of limb injuries that would affect test results (e.g., lacerations on fingertips). Shapiro–Wilk tests were used to evaluate normality of measurements for all continuous variables. Separate linear mixed-effect analyses were performed using the maximum likelihood method for parameter estimations. The response variables were the motor outcome measures, the fixed effects terms were “age” and “visit time” (with no interaction term), and random effects using random intercepts by “participant.” Normality was confirmed through examination of the residuals of each model. A Wilcoxon’s signed-rank test was used to evaluate change in performance on measures for non-normal variables. To control for multiple comparisons, the Benjamini–Hochberg false discovery rate procedure was employed for all null hypothesis tests, with the statistical significance threshold kept at α = 0.05. All p values are reported with 95% confidence intervals (CIs), and exact p values are reported for all nonparametric comparisons. For all comparisons, Hedges g is provided as a measure of effect size, where |g| ≥ 0.20, 0.50, and 0.80 are considered small, moderate, and large effects, respectively. 54,55 Statistical analyses were performed using Matlab R2021a (2021; College Station, TX: MathWorks).
Results
The protocol for itPBM intervention was 8 weeks; however, because of travel constraints or personal conflicts, some participants were unable to return for posttreatment testing until 10–12 weeks, during which time they continued the treatment. Reported compliance rate for itPBM usage was 92%. A summary of pre- and posttreatment assessment results is provided in Table 3. Pretreatment times for each hand on the grooved pegboard test, but not other measures, were associated with age. The fitted regression models were as follows: dominant hand time = 53.2 + 0.53 *age; nondominant hand time = 54.2 + 0.64*age. The overall regressions were statically significant [R 2 = 0.27, F(1,40) = 14.9, p = 0.0004; R 2 = 0.27, F(1,40) = 14.7, p = 0.0004, respectively.] Significant improvements related to treatment visits were seen in three of the four test domains (Table 4). Average reaction time improved by 19.39 ms (95% CI [12.24,26.54], p < 0.001) from pre- to posttreatment visits, with an effect size of 0.75, and was not influenced by age. Average dominant-hand grip strength increased from baseline by 2.70 kg (95% CI [0.89, 4.52], p = 0.003), whereas nondominant hand grip strength increased by 3.73 kg (95% [2.10, 5.36], p < 0.001) with small effect sizes (g = 0.22 and g = 0.35, respectively). These measures were unaffected by age. Also unaffected by age were the overall MiniBEST scores, which improved by an average of 1.32 points (95% CI [0.767, 1.88]) with a moderate effect (g = 0.51). A breakdown of MiniBEST subscores showed improvement and moderate effect in the reactive postural control domain (g = 0.63). Grooved pegboard times for each hand improved after treatment; however, the improvements were not statistically significant and time difference was affected by age (p < 0.001, bilaterally).
Wilcoxson’s Sign-Ranked Analysis of MiniBEST Subscores
Summary Statistics for Motor Assessments
GPB, Grooved Pegboard Test.
Mixed-Effects Linear Model Results
Discussion
After 8–12 weeks of itPBM treatments, participants experienced small to moderate effects in bilateral grip strength, reaction time, and reactive postural balance, but not dexterity.
These results are consistent with existing studies reporting improvements on motor measures after tPBM. For example, balance, gait, and grip performance improved in animal models of acute severe TBI. 56,57 In healthy young adults, finger tapping frequency improved in treatment groups after 5 min of laser tPBM (with total energy of 60 J/cm2) compared with sham groups. 58,59 Improvement in these biomarkers of health imply that PBM may address the pathology associated with RHAE-induced neuromuscular issues through its proposed mechanisms.
Head impacts decrease motor unit synchronization and recruitment because of increased excitotoxity 11 which may still be present in slowly progressing CTE resulting from RHEA. 60 PBM decreases excitotoxicity in in vitro animal models 61 –63 and if the same mechanism translates to human itPBM then we might attribute improvements in grip strength and balance to increased ability of the neuromuscular system to recruit and synchronize motor units.
Cortical electrophysiology associated with neural oscillations is disrupted by concussion 64,65 and can persist, likely because of damaged white matter circuitry. 39,66 –68 This disruption affects the synchronicity of the neural oscillations of the central nervous system, which modulate descending motor pathways. 69,70 itPBM delivery of pulsed light at 40 Hz possibly entrains gamma brain waves, a frequency involved in motor control. 67,69,70
Connectivity of cortical networks, which are disturbed in concussion, is vital for optimal motor control. PBM-related reductions in inflammation, along with increased energy production, cerebral blood flow, neurogenesis, and synaptogenesis, may contribute to neuroplastic changes to the structural and functional connectivity of the motor network, and thus recovered neuromuscular control. Some have suggested that tPBM and/or iPBM could improve motor performance in populations with Parkinson’s disease and Alzheimer’s disease by affecting these mechanisms. 27,71 –73 Although the itPBM treatments in the current study did not directly target regions in the motor cortex in the brain, results from remote PBM research studies where PBM was applied to an area distant from the cortical target (e.g., the abdomen), where significant beneficial results were observed 35,36,41 provide a plausible explanation for observed motor improvements.
Cognition, mood, and sleep positively correlate with measures of clinical motor outcomes. 74 –79 Thus, as itPBM-related recovery occur in these domains, 80,81 positive motor changes are likely to follow. Such changes were observed in this cohort in another arm of this study, 82 likely contributing to improvements in balance, grip strength, and reaction time.
It is important to note that although statistically significant, a 1.3-point improvement in MiniBEST scores are not necessarily clinically significant. However, 23% of participants in our study improved their scores by three or more points, with half of those improving by four or more points. Changes of 3.5 points on the MiniBEST constitute the detectable difference in a comparable population. 52 In addition, six of nine participants originally classified as moderately impaired were re-classified to normal-to-mild impairment. Similarly, improvements in grip strength of 2.7 and 3.7 kg in dominant and nondominant hands, respectively, were lower than estimates of meaningful changes of 5.0–6.5 kg. 83 However, in a cross-sectional study with almost 14,000 adults between the ages 50 and 70 years across 150 countries, an increase of 1 kg in grip strength was associated with a 6% higher score on a cognitive battery that assessed visuospatial abilities, episodic memory, and attention. 48
Although many of the significant results fall near, or just below, the threshold for clinically important change, the uniformly positive change toward better performance suggests these changes are not random. Further, these results may or may not be clinically meaningful given the 8-week duration and dosage, but longer interventions may demonstrate greater improvements. The low-risk, ease of use, and low cost indicate that longer itPBM interventions would be very feasible.
Limitations
This proof-of-concept study had a relatively small sample of predominantly male (39 of 43) participants. The design proved the feasibility of measuring changes before and after itPBM treatments; however, to attribute such changes definitively to the treatment, future studies with a larger sample size and a healthy control and/or sham group is necessary. An equitable male–female distribution is also necessary to investigate the influence of sex on treatment effect. The history of RHIs/acceleration events was self-reported; however, we remain confident in the reliability of the reports based on the information from Kerr et al. (2022) that indicates the stability of self-reported concussion. 84
itPBM treatments were self-administered. There was 92% compliance with the given treatment schedule, with several reported short periods of inconsistent use. In addition, all participants administered the itPBM treatment for an 8-week period; however, because of unforeseen events and/or the difficult timing of travel, some used the itPBM devices for up to 12 weeks. Participants were also instructed to maintain current routines; however, we did not strictly monitor or control for any modifications in fitness or reactional activities related to the motor outcomes of this study.
Conclusions
This study, which is a part of a larger study that included assessments of cognitive, psychological, and structural brain health, as well as neuromuscular health, supports our hypothesis that itPBM applied to the brain of individuals with chronic symptoms of RHAE has downstream effects on the neuromuscular system. Our results indicate that itPBM has small to moderate effects on grip strength, balance, and reaction time. It is not within the scope of this study to determine how PBM applied on the head acts on the distal parts of the neuromuscular system; however, motor unit recruitment resulting from reduction of excitotoxity, entrainment of disrupted neural oscillations that control descending pathways, and improved connectivity in the motor and cerebellar networks may be possible points of scrutiny in future work. Such work will also require more robust research designs to support this proof-of-concept study.
Footnotes
Acknowledgments
The authors gratefully acknowledge the participants of this study and their family members. The authors also acknowledge the thoughtful contribution of Dr. Margaret Naeser and Dr. H. Christian Davidson, and the technical support provided by Jessica Guinn, Stephani Debenham, Maria Gonzales, Cathy Taylor, Brandon Johnson, and Roger Kimball.
Authorship Confirmation/Contribution Statement
P.J.: Conceptualization, methodology, validation, formal analysis, investigation, data curation, writing—original draft, writing—review and editing, visualization, supervision, and project administration. P.F.: Conceptualization, methodology, software, formal analysis, resources, validation, data curation, and writing—review and editing. E.W.: Conceptualization, methodology, validation, investigation, resources, writing—review and editing, visualization, supervision, project administration, and funding acquisition. E.H.: Investigation, writing—original draft, writing—review and editing, visualization, and project Administration. H.R.: Investigation. C.V.: Investigation. R.P.: Investigation, writing—review and editing. A.M.: Investigation, software, writing—review and editing. N.K.: Investigation, writing—review and editing. E.R.: Investigation, writing—original draft, writing—review and editing. F.K.: Investigation. C.E.: Writing—review and editing. H.L.: Validation, writing—review and editing. M.N.: Writing—review and editing. D.T.: Investigation, writing—review and editing, project administration. C.M.: Editing. C.M.: Writing—review and editing. L.D.: Writing—review and editing. S.L.: Writing—review and editing. L.C.: Investigation, resources, project administration, and funding acquisition. D.F.T.: Conceptualization, methodology, validation, investigation, resources, visualization, supervision, project administration, and funding acquisition.
Author Disclosure Statement
L.C. serves as a consultant for Vielight, Inc. All other authors declare no direct conflicts of interest.
Funding Information
This research was supported in part by the Traumatic Brain Injury and Concussion Center PBM Fund and the Keith Rivera Fund. Vielight Inc. provided PBM equipment used in this study.