
Abstract
Objective:
The aim of this randomized clinical trial was to evaluate the influence of root canal disinfection with a 940-nm diode laser on the intensity of pain after endodontic retreatment.
Background data:
Microorganisms are the most common causes of tooth pain. Therefore, clinical studies are needed to explore the effect of disinfection techniques on postoperative pain.
Methods:
Eighty-four patients scheduled for endodontic retreatment were allocated to two groups in a 1:1 ratio (n = 42 each). After root canal filling removal and chemomechanical procedures, the root canals were disinfected with a 940-nm diode laser in one group [laser disinfection (LD) group]. In the other group, a mock application of laser was made with the power off [pseudo-laser disinfection (PLD) group]. All retreatment procedures were completed in a single visit. The patients assessed their pain levels at 24, 48, and 72 h after retreatment using a numeric rating scale. The number of analgesic pills used during this period was also recorded. The collected data were statistically analyzed using Mann–Whitney U and Wilcoxon tests.
Results:
Postoperative pain on the first 2 days was significantly lesser in the LD group than in the PLD group (p < 0.05), and the difference became insignificant on the third day (p > 0.05). Moreover, analgesic intake over 3 days and pain on percussion on the fourth day were significantly lesser in the LD group than in the PLD group (p < 0.05).
Conclusions:
Elimination of microorganisms from root canals is important for preventing postoperative complications. Our findings suggest that diode LD can reduce postoperative pain and provide comfort after endodontic retreatment.
This study is registered in
Introduction
The prevention and control of postoperative pain are important to ensure the patient's comfort and satisfaction. Endodontic retreatment has been claimed to be a contributing factor for post-treatment complications. In previous studies, the rate of flare-ups was higher for patients who underwent endodontic retreatment than for those who underwent initial endodontic treatment. 1 –4
Pain after endodontic treatment can be caused by mechanical, chemical, and/or microbial damage to the pulpal or periradicular tissues. However, microorganisms and their products are considered the major and most common causes of postoperative pain. 5,6 Unfortunately, it is difficult to completely eliminate microorganisms from the root canal system using conventional chemomechanical procedures. 7 –9 In endodontic retreatment, disinfection becomes much more difficult because of the resistant strains of bacteria settled in the root canal system. Some of these bacteria can resist root canal irrigants/disinfectants, survive in the tough environmental conditions in filled canals for years, and cause persistent periradicular lesions. 10 –13
In routine endodontic practice, sodium hypochlorite (NaOCl) is the most commonly used irrigant because of its broad antimicrobial activity and ability to dissolve organic matter. 14 However, the penetration ability of this irrigant is limited, and it cannot always act on the bacteria located in inaccessible areas such as dentinal tubules and anatomical complexities in root canals. 15,16
Over the last decade, diode lasers have gained widespread acceptance in the field of laser-assisted endodontics, and several studies have performed deep disinfection of the root canal through diode laser irradiation. 17 –20 Diode lasers (810, 940, and 980 nm wavelengths) exhibit high water transmission, which allows them to interact with the microorganisms located in the deeper layers of dentinal tubules. 18,21,22 A recent study 23 showed that 940 nm diode laser has extremely high bactericidal effect on most resistant endodontic pathogen Enterococcus faecalis even at the 1000-μm depth of dentine.
On the basis of the fact that microorganisms are the most common causes of pain, the present study aimed to evaluate the effect of root canal disinfection with a 940-nm diode laser in addition to conventional irrigation on the intensity of pain after endodontic retreatment. To the best of our knowledge, there is no similar study published in the literature.
Materials and Methods
This placebo-controlled, parallel-arm randomized clinical trial was approved by the ethics committee at our institution (number: 01-29.11.2017). All participants read and signed an informed consent form with details about the risks and benefits of the treatment.
Sample size calculation
Sample size calculation based on data obtained from a pilot study indicated that 35 patients would be required per group (alpha error = 0.05, power = 0.8, effect size = 1). After considering the possibility of dropouts during mechanical procedures or the follow-up period, we included 84 patients in our study (42 patients per group).
Patient selection and randomization
We screened 495 patients aged 18–52 years who were referred to the Department of Endodontics. Endodontic treatment failure was determined during routine radiographic examinations. Root canal obturation and the periapical status of the teeth were determined through periapical radiographs obtained using the parallel technique. We only included asymptomatic single-rooted teeth with an initial root canal filling that exhibited chronic periapical infection (minimum size of lesion, 2 × 2 mm). We eliminated cases of ongoing healing by ensuring that the root canal fillings were ≥4 years old. The exclusion criteria were as follows: teeth with root canal fillings placed <4 years ago, overfilled teeth, teeth with intraradicular posts, teeth with sinus tracts, antibiotic consumption within the last 1 month, analgesic consumption within the last 5 days, systemic disease, pregnancy, trauma history, traumatic occlusion, presence of other teeth requiring endodontic treatment, and extensive crown destruction preventing rubber dam isolation.We selected 84 patients who matched the abovementioned criteria from the 495 patients and randomly allocated them to two groups in a 1:1 ratio (Fig. 1). To ensure randomization, a graduate student blinded to the study procedure allocated the patients by asking each one to choose one of the sealed envelopes containing the group codes.
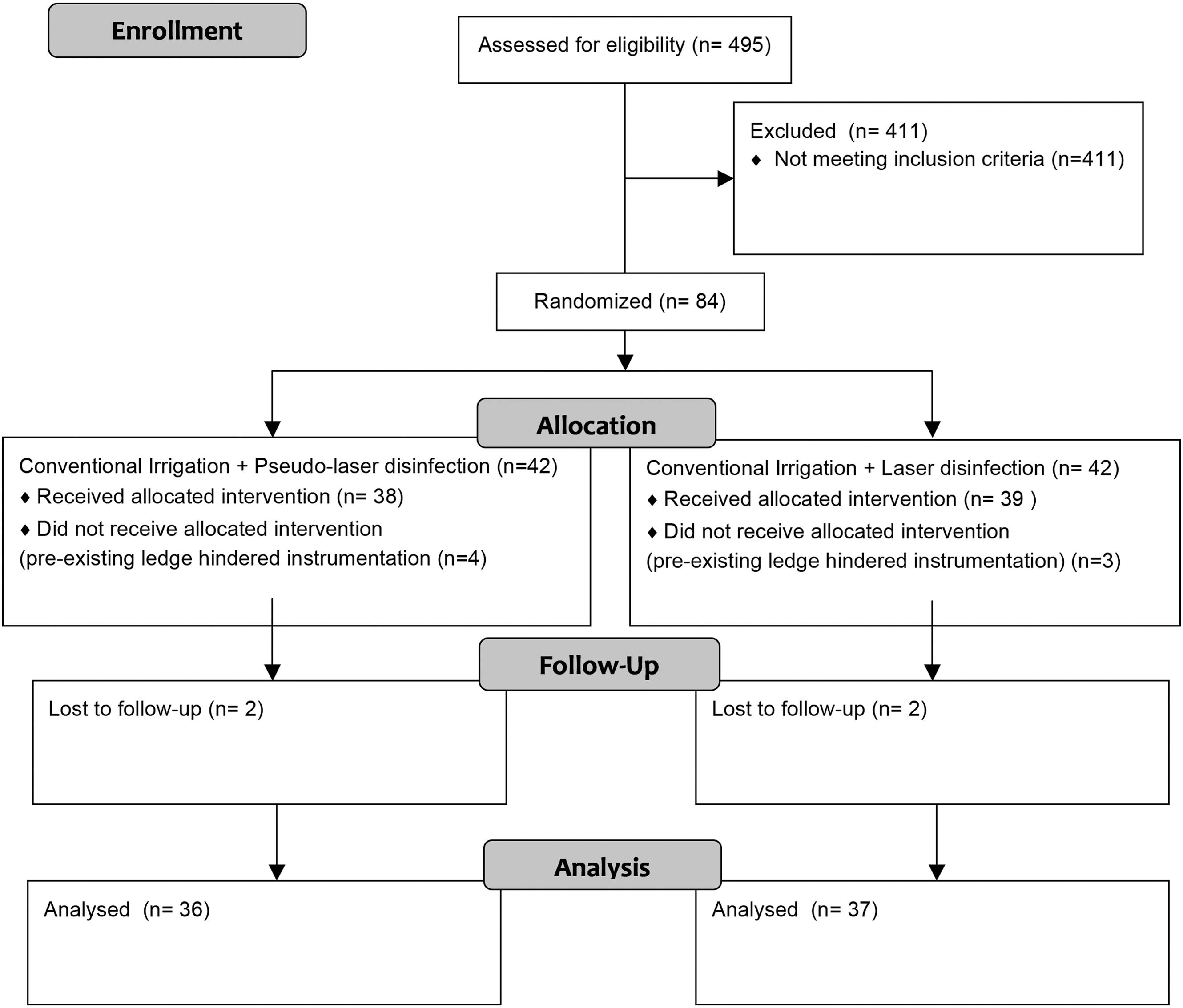
The consolidated standards of reporting trials flow diagram for randomized clinical trials.
Treatment protocol
A single operator blinded to the group allocation (M.K.) performed all chemomechanical procedures as described below. After local anesthetic (4% articaine with 1:100,000 epinephrine) infiltration and rubber dam isolation, the operator removed coronal restorations, located the canal orifices, and removed the canal fillings using ProTaper Universal Retreatment files (Dentsply Maillefer, Ballaigues, Switzerland) according to the manufacturer's instructions. D1 (size 30, 0.09 taper), D2 (size 25, 0.08 taper), and D3 (size 20, 0.07 taper) files were consecutively used in a crown-down manner in conjunction with an X-Smart endomotor (Dentsply Maillefer, Ballaigues, Switzerland), with a rotational speed of 500 rpm and a torque of 2 N/cm. The operator determined the working lengths using an apex locator (Propex Pixi; Dentsply Maillefer) and confirmed them on periapical radiographs. When the D3 file easily reached the working length and no further filling material was observed on the instrument or in the irrigant, removal of the root canal filling was considered complete. No solvent was used during the procedure. K-files up to #40 or #60 were used for further apical enlargement depending on the type and dimensions of the tooth. The operator maintained apical foramen patency with a #10K-file during shaping and cleaning procedures.
During mechanical procedures, the operator irrigated the canals with 2% NaOCl using a 30-gauge, side-opening needle (Max-i-Probe; Dentsply Rinn, Elgin, IL) placed 3 mm short of the working length each time we changed the file. A total of 15 mL was delivered in each canal. The smear layer was removed with 3 mL of 17% EDTA, and 5 mL of 2% NaOCl was used for the final irrigation. The canals were dried with paper points.
Subsequently, a second operator (O.G.S.) who received the sealed envelopes containing the group codes performed laser disinfection (LD) as described below.
Laser disinfection (LD) group
After excluding three patients with preexisting ledges that hindered access to the apical third of the canals, the operator disinfected the canals of the remaining 39 teeth using a 940-nm diode laser (Ezlase; Biolase, San Clemente, CA). Laser energy was delivered through a 200-μm fiber tip (E2 Endo Tip; Biolase) with an output power of 1 W in the continuous mode. The operator placed the laser tip at the working length and irradiated the canals at a speed of 2 mm/sec, with circling movements from the apical to the most coronal part of the root canal. This procedure was repeated four times for each canal, with a 20-sec interval between applications.
Pseudo-laser disinfection (PLD) group
After excluding four patients with preexisting ledges that hindered access to the apical third of the canals, the operator placed the diode laser tip at the working length and performed the same procedure described for the LD group without turning on the power switch (n = 38).
The patient and operator wore protective glasses during all laser applications.
We filled all canals with gutta percha points and epoxy resin-based root canal sealer (MM-Seal; Micro-Mega, Besançon, France) using the cold lateral compaction technique, following which we restored the crowns using a two-step self-etch adhesive (Clearfil SE Bond; Kuraray, Tokyo, Japan) and hybride composite resin (Filtek Z250, 3M ESPE, St. Paul, MN). All patients received an analgesic (ibuprofen 400 mg every 6 h) prescription for use when required.
Assessment of postoperative pain and pain on percussion
We used an 11-item numeric rating scale (NRS) for pain assessment after treatment. This NRS is a segmented numeric version of the visual analog scale. The respondent selects a whole number from 0 to 10 that best reflects the intensity of their pain, with 0 representing no pain and 10 representing the worst imaginable pain. 24,25
All patients were asked to provide their ratings on the first, second, and third postoperative days. They were also requested to record the number of analgesic pills consumed each day during this period. The pain scale forms were collected at the second appointment, which was scheduled on the fourth day. In the same session, we evaluated pain on percussion by tapping the retreated tooth in the vertical direction using a load limited to the weight of the mirror. The patient's responses to percussion were quantified as follows: 0, no reaction or pain; 1, discomfort and mild or moderate pain; and 2, extensive discomfort, with the patient writhing and complaining of intense pain.
Statistical analyses
All statistical analyses were performed using SPSS 13.0 for windows (SPSS, Inc., Chicago, IL). Descriptive statistics is presented as mean ± standard deviation. The Mann–Whitney U test was used for comparison of values at the different time points between the two groups, while the Wilcoxon test was used for within-group comparisons among the different time points. The chi-square test was used to assess age and sex distribution in the two groups. A p-value of <0.05 was considered statistically significant.
Results
Demographic and clinical data for the 84 patients are presented in Table 1. The pseudo-laser disinfection (PLD) and LD groups showed no significant differences in age and sex (p > 0.05; Table 1).
Baseline Demographic and Clinical Features of Patients Undergoing Endodontic Retreatment With or Without Laser Disinfection
LD, laser disinfection; PLD, pseudo-laser disinfection.
Table 2 shows the postoperative pain scores, pain scores on percussion (fourth day), and analgesic consumption (over 3 days) for the two groups.
Mean Postoperative Pain Scores (Numeric Rating Scale), Number of Analgesic Pills Consumed, and Pain Scores on Percussion After Endodontic Retreatment With or Without Laser Disinfection
Different lower cases represent statistically significant difference in each group at different time periods (p < 0.05).
Represents statistically significant difference between two groups at the same time period (p < 0.05).
SD, standard deviation.
The pain scores on the first and second days after treatment were significantly lower for the LD group than for the PLD group (p = 0.036 and 0.016, respectively); the significance disappeared on the third day (p = 0.056). Both analgesic consumption and pain on percussion were significantly lesser in the LD group than in the PLD group (p = 0.008 and 0.008, respectively).
In the PLD group, postoperative pain was comparable between the first and second days after treatment (p = 0.097), and the pain on the third day was significantly lesser than that on the first 2 days (p = 0.000 and 0.001, respectively). In the LD group, there were no significant differences in pain scores among the 3 days (p > 0.05).
Discussion
The development of pain after endodontic retreatment is a frequent problem. Because microorganisms are the most common causative factors for post-treatment pain, the pain incidence may decrease if an effective antimicrobial strategy is used during treatment. 26 Accordingly, in the present study, we evaluated the effect of root canal disinfection with a 940-nm diode laser on pain after endodontic retreatment and found that this strategy reduced postoperative pain and provided comfort to the patient after the retreatment.
Diode lasers exhibit their antimicrobial effects through direct thermal action on pigmented bacterial membranes of endodontic pathogens or through the generation of short-term temperature increments in the bacterial microenvironment. 17,20,21 During intracanal irradiation with diode lasers, the temperature increase is reportedly in the range of 1°C–7°C, which is safe for the surrounding periodontal tissues. 27 –29 Nevertheless, to safely irradiate the entire canal wall and prevent hazardous temperature increments, we performed laser irradiation using circling movements. 30,31 A recent study 32 showed that leaving 20-sec passive cooling period between irradiation cycles of the 940 nm diode laser (1 W, continuous mode) allows temperature decrease on the external root surfaces. Therefore, we provided a 20-sec resting time between cycles. We performed diode LD after conventional chemomechanical irrigation and smear removal procedures because diode lasers cannot effectively remove the smear layer. 27,28,33
Similar to the follow-up duration in other studies, that in our study was 3 days. 34 –36 Postoperative pain usually occurs during the first 2 days after root canal treatment, and its intensity gradually decreases over time. 37 –39 Even in the present study, the pain scores for both groups were the highest on the first day and showed a daily decrease thereafter.
On the first 2 days after retreatment, the postoperative pain intensity was significantly lower in the LD group than in the PLD group. In addition, the percussion test performed on the fourth day revealed significantly lesser pain on percussion in the LD group than in the PLD group. Given that microorganisms are one of the major causes of postoperative pain, the low pain scores in the LD group can be attributed to the destructive effect of laser irradiation on bacterial species resistant to chemicals and the overall superior disinfection of the root canal system. Intracanal disinfection with a laser may have a positive effect on bacteria present beyond the root apex. 40 On the third day, the difference in postoperative pain between the LD and PLD groups became insignificant, although the pain score for the LD group was lower. This finding can be attributed to the natural process of pain reduction in both groups.
In the field of endodontics, a flare-up refers to the development of severe pain and/or swelling after intracanal procedures. In the present study, NRS scores of 8, 9, and 10 were considered to represent severe pain and, consequently, a flare-up. The overall incidence of flare-ups was 2.7% and 13.8% in the LD and PLD groups, respectively. These values are consistent with previously reported endodontic flare-up values of 1.4–16%. 1,3,26,41,42 However, it should be noted that the incidence in the LD group in our study is close to the lowest incidence reported in previous studies, whereas the value for the PLD group is close to the maximum value reported.
Analgesic consumption was significantly higher in the PLD group than in the LD group. In the former group, eight patients with NRS scores of 6–10 and two patients with an NRS score of 3 took analgesic pills, while in the LD group, one patient with an NRS score of 2 and one with an NRS score of 8 reported analgesic consumption. In general, analgesic use was directly proportional to the severity of pain; mostly patients who experienced high levels of pain took analgesics.
Although sex and age are believed to influence postoperative pain perception, 43 –46 studies 41,47,48 have also reported no such association. We believe that the effect of these two variables was minimal in our study because the age and sex distributions were statistically equal in the two groups.
Although we took maximum efforts to simulate an actual clinical setup, our study has some inevitable limitations. The final apical preparation sizes could not be standardized because each tooth has its own specific dimensions that vary among patients. Moreover, pain perception is subjective, and the different pain thresholds of the participants may have affected the pain scores. In addition, endodontic retreatment involves a multi-step complex process chain, and each step has the potential to cause pain.
The strength of our study lies in its design. It was a placebo-controlled, parallel-arm randomized controlled clinical trial. To minimize bias, the participants, researcher performing the chemomechanical procedures, and statistician were blinded to the patient groups. Only the researcher performing LD was aware of the groups because of the nature of the required work.
In conclusion, within the study limitations, the findings suggest that root canal disinfection with a 940-nm diode laser subsequent to routine chemomechanical procedures can efficiently reduce pain and provide comfort to the patient after endodontic retreatment. To the best of our knowledge, this is the first study of its kind. Further studies should explore the effects of different wavelengths of diode lasers on postoperative pain control.
Footnotes
Acknowledgments
The authors gratefully acknowledge Prof. Dr. Siddik Keskin for performing the statistical analysis.
Author Disclosure Statement
No competing financial interests exist.