
Abstract
Background:
Diode lasers have been used for implant decontamination. However, the use of initiated or noninitiated tips remains unevaluated to verify potential photothermal risks.
Objective:
To assess the photothermal effects of defocused-initiated versus noninitiated irradiation.
Materials and methods:
A dental implant (3.5 × 11 mm) was placed into an artificial bone, an infrabony defect was created to simulate a four-wall peri-implant defect. Irradiation was performed using pulsed diode lasers of 940, 975, and 980 nm. The laser tips were positioned parallel to the implant (maximum 2W pulsed mode). The implant was irradiated for 30 sec using noninitiated, cork-, and blue paper-initiated tips. Temperature differences were observed at the apical and coronal regions of the implant. The data were statistically evaluated and compared using one-way analysis of variance and Tukey tests.
Results:
The average temperature increase and the amount of time that it took to yield the critical temperature were comparable at the coronal level for the 940 and 975 nm diode lasers (p > 0.05). For the 980 nm laser, blue-initiated tip had the highest temperature increase (22.4°C), followed by cork (18.8°C) and noninitiated tip (17.3°C). The critical threshold at the coronal portion for the 980 nm laser was reached in 11.5, 8.79, and 6.46 sec for the blue paper-, cork-, and noninitiated tips, respectively. The 975 and 980 nm lasers had average temperature increases, comparable among the blue paper-, cork-, and noninitiated tips at the apical level (p > 0.05). Apically, for the 940 nm, the noninitiated tip had the highest temperature increase (5.57°C), followed by the cork- (4.96°C) and blue paper-initiated tip (4.54°C).
Conclusions:
The initiator does not affect the temperatures produced during implant decontamination although noninitiated diode lasers may overheat (within 30 sec) than initiated tips. There is minimal risk of overheating at the apical portion. It seems that the 940 nm diode is the safest of the evaluated laser systems.
Introduction
Implant treatment has an impact on oral health related to quality-of-life improvement especially for complete edentulous patients. 1 Recent studies showed implant survival rate of near 97% after 9 years (1.4% of implants as early failures and 2.0% of implants as late implant loss). 2 The success is dependent on the following criteria as established by Albrektsson et al., 3 such as absence of mobility, <0.2 mm of bone loss annually after the first year of placement, lack of peri-implant radiolucency, and absence of persistent and irreversible signs and symptoms.
However, peri-implant diseases can lead to implant failure. Peri-implantitis is defined as an inflammatory process around the implant, which includes both soft tissue inflammation and progressive loss of supporting bone beyond biological bone remodeling. 4,5
The recent World Workshop held by the American Academy of Periodontology and the European Federation of Periodontology concluded that peri-implantitis presents evidence of visual inflammatory changes in the peri-implant soft tissues combined with bleeding on probing and/or suppuration, increasing probing depths compared with the baseline (time of placement of the prosthesis) and progressive bone loss. An assessment of the yearly rate of bone loss was recommended. 6
Treatment of peri-implantitis includes surgical and nonsurgical techniques and combination techniques. 7 –11 Surgical techniques are preferred because the implant surface is exposed and a more exhaustive decontamination is achieved. 7 –11 The surgical treatment involves accessing the site of infection and debriding the implant surface in three ways: (1) mechanically through curettes and/or air abrasives; (2) chemically with root conditioners, disinfectants, and antibiotics or, lastly; (3) through phototherapy using laser irradiation (carbon dioxide, diode, and Er:YAG). 8 A combination of the different modalities can also be used for decontamination. Lasers have been used clinically for implant decontamination 12 –14 providing good results in clinical case series.
Diode lasers with wavelengths ranging between 810 and 980 nm have been used for soft tissue surgery, providing excellent coagulation and may be used for treatment of peri-implant diseases. 15 –17 A systematic review by Kotsakis et al. 18 reported that based on the limited currently available information, any superiority of laser treatment in comparison with conventional treatment of peri-implantitis could not be identified. The available studies reviewed had great heterogeneity to conclude a single treatment of choice for implant surface decontamination for the surgical treatment of peri-implantitis. 19 However, the laser offers a novel technical approach that is completely different from the conventional mechanical debridement, with several advantageous effects. With better understanding of the characteristics of laser light, as well as the development of laser devices, the role of light energy in periodontal and peri-implant treatment is expected to rapidly expand in the clinical evidence for the promotion of periodontal wound healing and tissue regeneration. 17 Since laser dentistry has been developed extensively in the last few years, there is a need for a comprehensive review to re-evaluate the efficacy of laser therapy. Diode lasers have been used extensively and there is a lot of required understanding for the use of initiated versus noninitiated fiberoptic as well as thermal effects on the tissues. Only a recent ex vivo study in soft tissues 20 was focused on this aim. However, the thermal effects of diode lasers on dental implants are currenly under active research. Initiated tips can be used to coagulate and biomodulate peri-implant defects, and noninitiated tips can detoxify implant surface topography. Since diode laser tips have an impact of heat transfer on tissues, there is a need to evaluate the effect of initiated or noninitiated tips on the implant body temperature during diode irradiation. The initiation of the fiber tip is achieved when the tip of the laser touches a dark chromophore. As soft tissue absorbs energy, it results in heat production and thus a rise in tissue temperature. It has been shown that initiators are effective for activation. To investigate the photothermal effects of tip initiation on the implant surface, the diode laser was investigated in conjunction with implant irradiation.
Materials and Methods
The entire procedure was performed, by the same clinician, with experience in laser-assisted peri-implant surgical procedures as well as laser irradiation.
Model of experimental peri-implantitis
A 3.5 × 11 mm dental implant (Ankylos®; Dentsply Implants, Waltham, MA) was placed into an artificial bovine bone block (BoneSim®; Newaygo, MI). An infrabony defect of 5 mm depth, 3 mm width, and 3 mm height was created with water irrigation using a high-speed handpiece and diamond bur. Additional bone was removed circumferentially at the apical portion to enable access for thermocouple placement.
Implant surface irradiation
To measure temperature differences, two thermocouples were attached to the implant surface (T-Type Probe; ADInstruments, Inc., Colorado Springs, CO). The first thermocouple was attached to the coronal portion of the implant (within the implant body through the implant cover screw) and the second was attached lateral to the apical third of the implant. The thermocouples were connected to a data acquisition device and a personal computer, which enabled the temperatures to be read constantly (ADInstruments PowerLab 4/35 system and ADInstruments LabChart Software).
Irradiation of the implant surface and peri-implant bone was performed (n = 15 irradiations per group) using three diode laser systems with the following wavelengths: (1) 940 nm (EPIC 10, Irvine, CA), (2) 975 nm (Alta, Walpole, MA), and (3) 980 nm (KaVo, GENTLEray, Biberach, Germany). The pulse widths for the 940, 975, and 980 nm diode lasers were 20, 25, and 25 ms, respectively. The fiber used with all the lasers had 300 μm diameter at the active tip.
The diode lasers were positioned parallel to the implant surface during irradiation (since the glass fiber could not be placed differently within the infrabony defect of 5 mm) with a maximum of 2W in pulsed mode (Fig. 1). Each laser had three initiation groups: noninitiated (control), cork-, and blue articulating paper initiation. Fifteen cycles of irradiation were conducted for each group. All laser irradiations were performed using the standard safety measures in the laboratory (according to ANSI Z136.3, 2005). 21
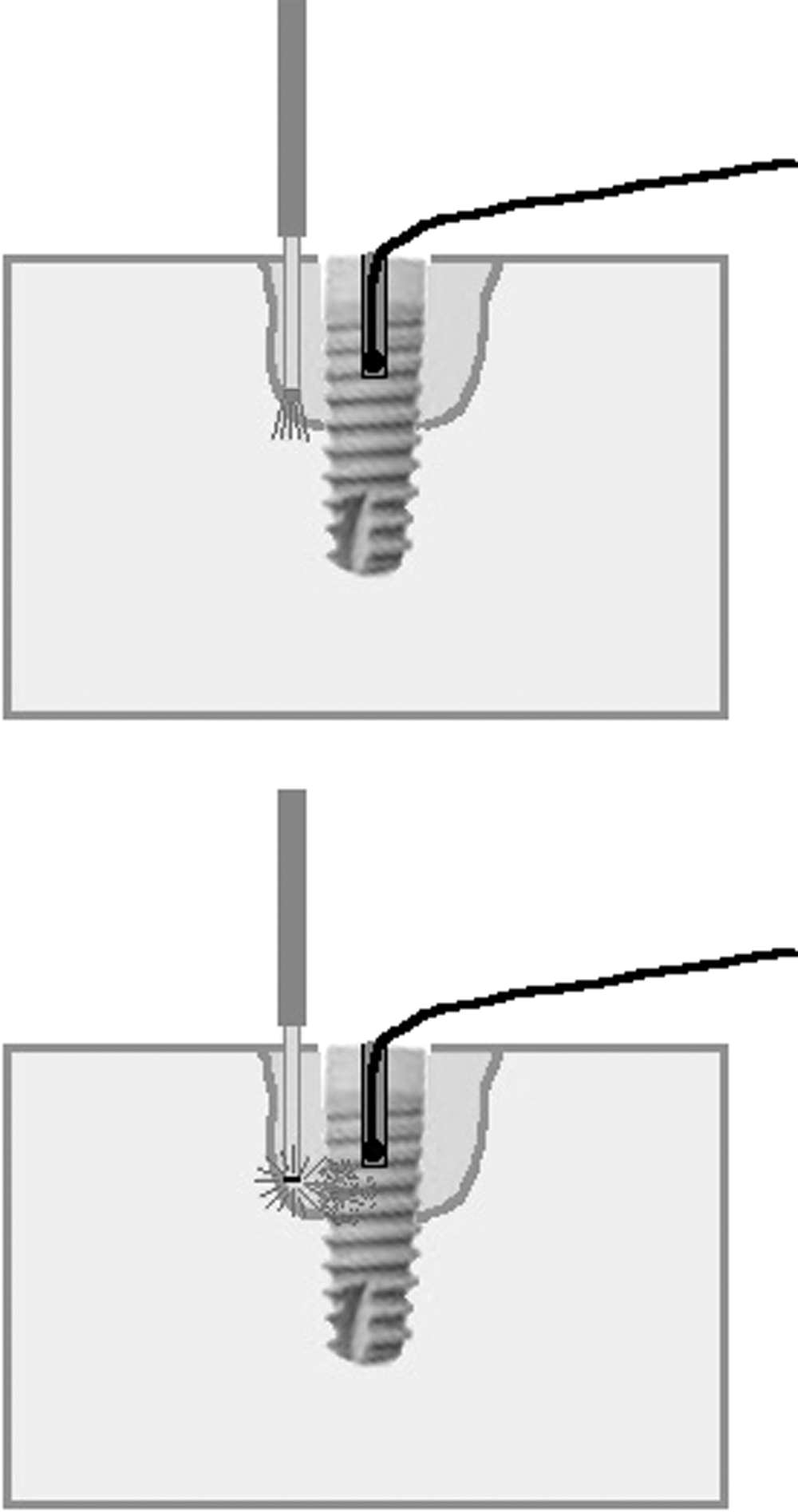
Concept of the diode laser irradiation without initiated tip (above) and with initiated tip (below) providing temperature (heat) transfer to the implant body.
Before irradiation, the implant was placed on a flat bench top (Fig. 2). The initial temperature was monitored and recorded for both thermocouples. The infrabony defect was then irradiated for 30 sec. After irradiation, the implant was cooled using a combination of water and air cooling, until the apical and coronal thermocouples reached their respective preinitiation temperature.

Experimental setting irradiating peri-implant bony defect using a diode laser.
Statistical analysis
The resulting data were calculated using statistical software (SPSS, Inc., Chicago, IL). The data were analyzed using a one-way analysis of variance and then Tukey honestly significant difference (HSD) for comparisons among groups. Level of significance was set at p < 0.05.
Results
The mean temperature differences at the apical level are shown in Fig. 3. The 975 nm diode laser exhibited the greatest temperature change, followed by the 980 and 940 nm diode laser, respectively. Only the 940 nm diode laser had statistically significant differences (lowest temperature rise) among the noninitiated, cork-, and blue paper-initiated tip (p < 0.05; Table 1).

Average temperature change (°C) at the apical level (n = 15 irradiations per group) after 30 sec of irradiation demonstrating the lowest temperature increase for the 940 nm diode laser independent of the use of initiators.
Temperature Changes During Implant Irradiation with Diode Lasers
CT, critical threshold; SD, standard deviation.
The mean temperature differences and the average time to reach critical threshold at the coronal level are shown in Figs. 4 and 5, respectively. At the coronal level, the 975 nm diode laser had the greatest temperature increase (p < 0.05) followed by the 980 and 940 nm diode laser (Fig. 4). The average amount of time to reach critical threshold (10°C) was longest for the 940 nm diode laser and shortest for the 975 nm diode laser (p < 0.05; Fig. 5; Table 1).
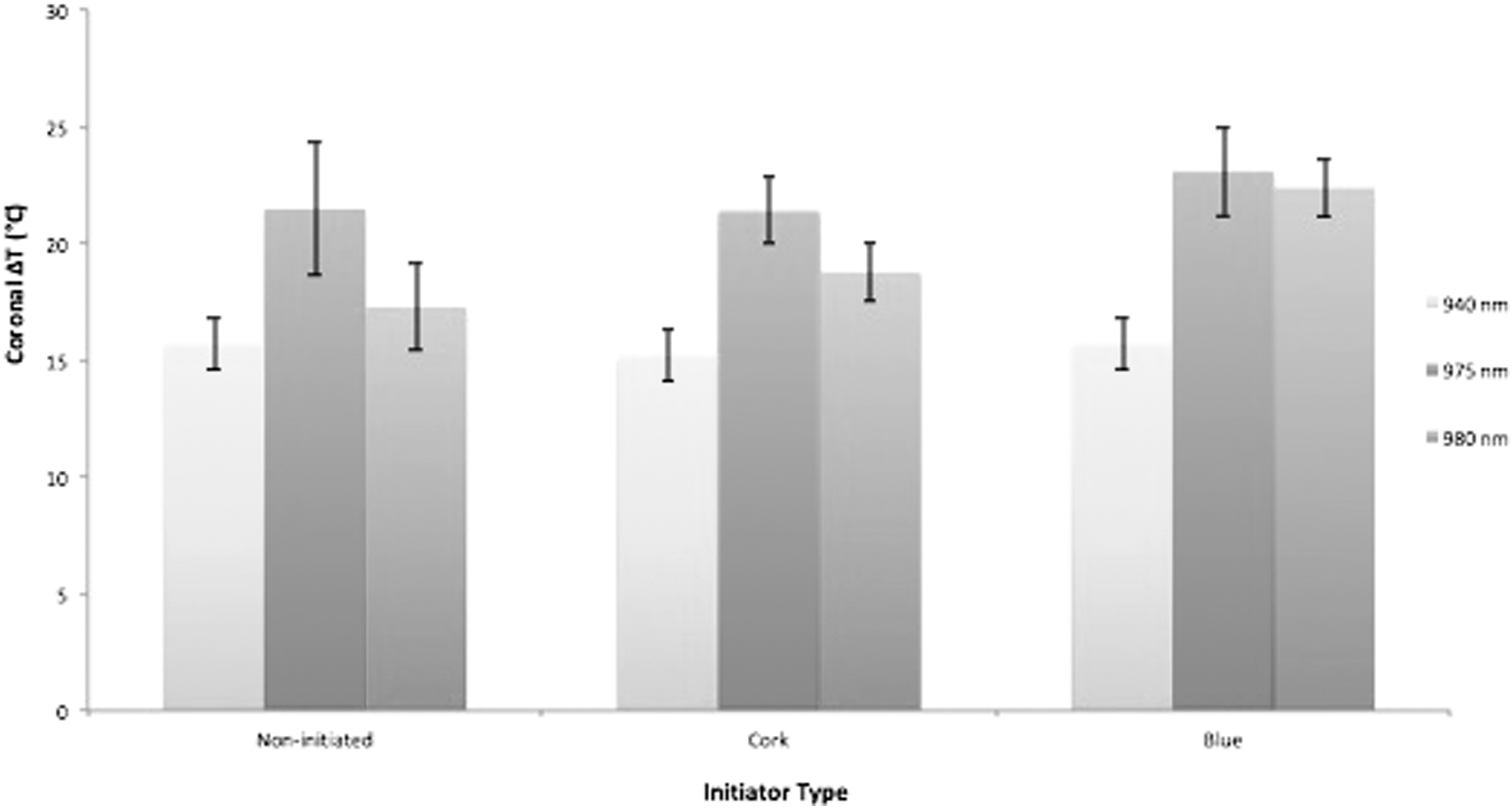
Average temperature change (°C) at the coronal level (n = 15 irradiations per group) after 30 sec of irradiation, demonstrating the lowest temperature increase for the 940 nm diode laser independent of the use of initiators.
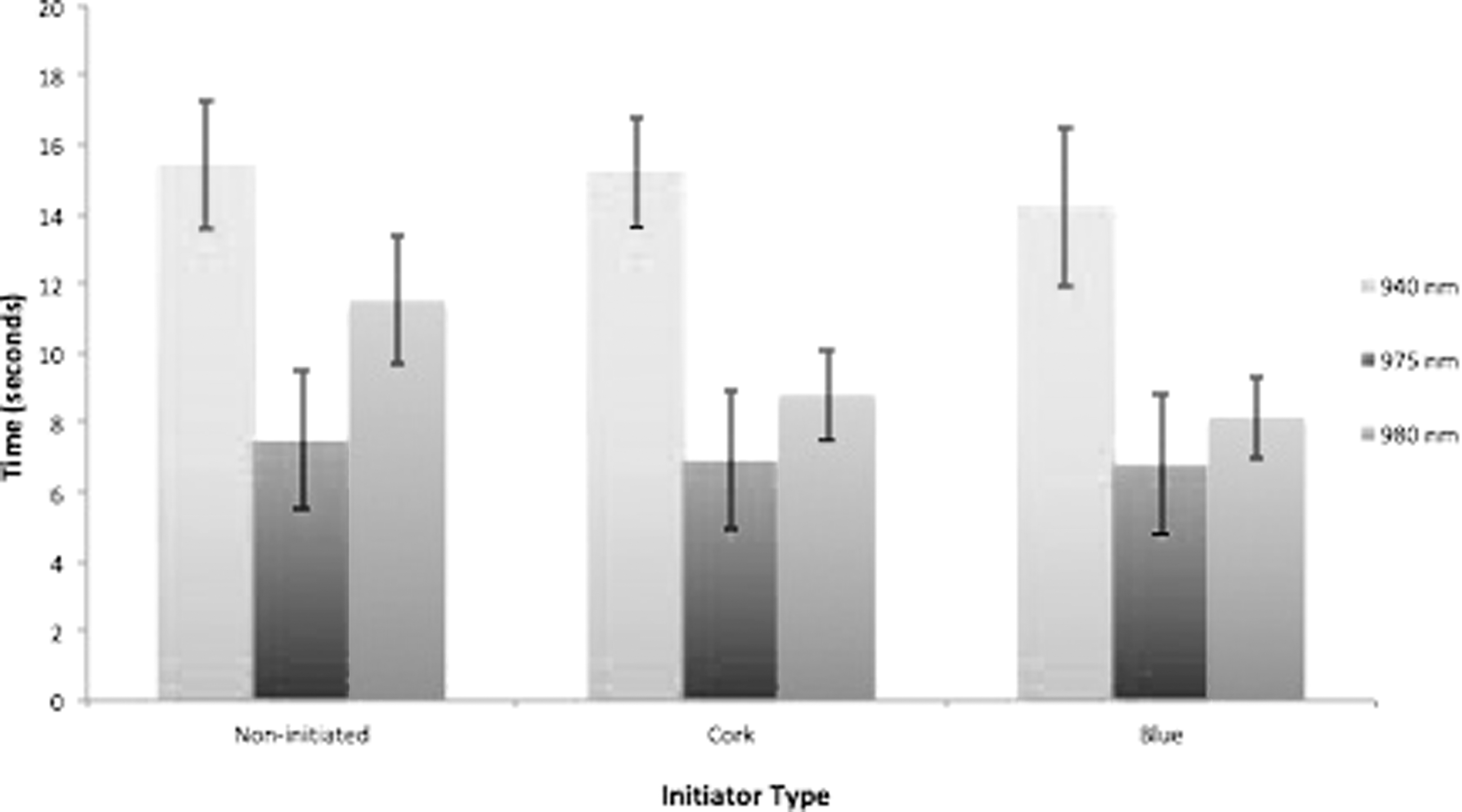
Average time to reach critical threshold (Δ10°C) in 2W pulsed mode (n = 15 irradiations per group), demonstrating that this time is longer using 940 nm diode laser (safest method).
Unlike the 980 nm diode laser, the average temperature increase and amount of time that it took to yield the critical temperature threshold were not statistically significant (p > 0.05) at the coronal level for the 940 and 975 nm diode lasers (Table 1) among noninitiated, cork-, and blue-initiated tips.
Discussion
The present data showed increase of the temperature over the critical threshold of 10°C in the coronal implant site for all the diode laser wavelengths within the tested irradiation period of 30 sec. This may have dramatic effects in clinical cases, where the defect morphology presents some bone in contact with the implant in the coronal part of the implant, and this temperature is high for a period longer than one 1 min critical threshold. This is the critical threshold according to previous studies. 22 –24
The safest wavelength in this indication seems to be the 940 nm diode laser using initiated and noninitiated tips due to the effect that this wavelength does not penetrate the titanium body and further increasing the temperature in the dramatic level.
Recent studies evaluated the temperature increase in soft tissues (ex vivo). 20 Both the power settings of the diode laser and type of initiator used affect the degree to which the temperature of the soft tissue increases during incisions and have to be considered for the safety in soft tissue applications. These studies showed that blue articulating paper seems to be the safest method of fiber initiation, as compared with the other initiators and no initiator providing the best cutting efficiency. 20 However, this study is not focused on the cutting efficiency but on the decontamination of implant surface and peri-implant bone defect biomodulation due to thermal effects (heat transfer). In terms of safety parameters, we were able to evaluate the temperature changes in the implant body in an in vitro model. Previous data from our laboratory showed that diode lasers may increase temperatures over the critical threshold compared with other wavelengths 25 –27 and also showed ex vivo (in bovine ribs) the dramatic increase of temperature using noninitiated diode lasers within an irradiation period of 60 sec. The present results are in correspondence with the data from the previous studies. 26,27 Specifically, Geminiani et al. 26 showed that the 810 nm laser reached the critical threshold after only 14 sec in continuous wave mode (c.w.) and 28 sec in pulsed mode and that the 980 nm laser reached the critical threshold faster after only 12 sec in c.w. and in 23 sec in pulsed mode. Leja et al. 27 recorded increase of temperature during 60 sec of irradiation using 1W diode laser in a pulsed mode of 6°C and 8°C for 810 and 980 nm, respectively. In case of 1W continuous power, this temperature increase was 12°C versus 32°C, respectively.
Similarly, Valente et al. 28 showed the use of 810 nm diode laser as a safest method compared with 980 nm or Nd:YAG laser. The use of 980 nm diode laser with 1W power seems to duplicate the increase of implant temperature compared with the use of 810 nm laser.
Other studies by Rios et al. 29 evaluated the 968 nm diode laser and showed that the effect of air is fundamental to decrease the implant temperature during diode irradiation.
Other ex vivo studies were performed in porcine bone blocks with implants in a 37°C water bath and evaluated the temperature increase during irradiation using different diode lasers. The results of this study suggest that the use of these diode lasers does not cause a harmful increase in temperature when used under conditions similar to those of the human body. 28 Other studies also showed that the use of both diode laser wavelengths (810 and 980 nm) in implant surface decontamination was efficacious regardless of the use of photosensitization (with indocyanine green dye) and without dangerous increase of temperature. 30
All these studies do not focus on the effects of the use of initiated or noninitiated tips like the present study. There is no doubt that further studies with bacteria should be performed to evaluate the antimicrobial effect of diode lasers in the peri-implant defects using initiated and not initiated tips.
The present in vitro study provides required information about the parameters and guidelines to establish a safe protocol of laser therapy in the treatment of peri-implantitis. It aims to evaluate the temperature change induced by irradiation from diode lasers with different initiated tips. More studies in clinical settings should be developed following these guidelines for safety, as well as diode laser wavelength to establish an evidence-based protocol for the clinical practice.
Conclusions
Within the limitations of the study, it can be concluded that the initiator does not affect the maximum temperatures produced during dental implant surface decontamination, although noninitiated diode laser-initiated tips may overheat faster (within 30 sec) than initiated tips. There is minimal risk of overheating at the apical portion of the implant. In terms of overheating risk, it seems that the 940 nm diode laser is the safest of the evaluated diode laser systems.
Footnotes
Author Disclosure Statement
No competing financial interests exist.