
Abstract
Objective:
The purpose of this study is to evaluate the efficacy of CO2 laser vaporization therapy for oral lichen planus (OLP) refractory to conservative treatments.
Methods:
The study group comprised 16 patients with clinically and histologically diagnosed OLP. They underwent conservative treatment for 3 months using an adrenal cortex hormone ointment and azulene sulfonate sodium hydrate gargle. Patients who showed no improvement with conservative treatment underwent CO2 laser vaporization therapy (3 W, continuous-wave mode). The assessment was performed using the numerical rating scale (NRS) as a subjective indicator and the Thongprasom sign score (TSS) as an objective indicator of OLP. These two scales were recorded during examinations performed before treatment and then at 7 days, 1, 3, and 6 months, and 1 year after irradiation. Differences between preirradiation and each point of time after irradiation were tested by Wilcoxon's signed-rank tests.
Results:
Laser irradiation was administered to 9 patients with 11 sites. The NRS score and TSS decreased at all 11 sites (100%) and 10 sites (90.9%) at 1 year after irradiation compared with preirradiation scores. The NRS score and TSS were statistically lower (p < 0.05) at 1 and 3 months (short-term) and 6 months and 1 year (mid-long-term) after irradiation than the preirradiation scores. There were no patients with malignant transformation during the study period.
Conclusions:
These single-arm clinical trial results show the efficacy of CO2 laser vaporization therapy for OLP refractory to conservative treatment.
Introduction
Oral lichen planus (OLP) is a very common refractory chronic inflammatory disease of the oral mucosa and is considered to be a precancerous condition. 1 –3 Although many studies on this disease have been conducted worldwide, its onset mechanism remains largely unclear, 4 and currently, there is no established curative treatment. Therefore, the long-term use of conservative treatments—such as topical application of adrenal cortex hormone ointment and the use of a gargle—is often selected. 1,2 However, as many patients are refractory to conservative treatment, eating disturbance due to pain and burning sensation, 5 long-term patient anxiety associated with a risk of malignant transformation, 6 and having to commute to a hospital result in decreased quality of life. To date, several reports have described new treatments—including various pharmacotherapies 7 and photodynamic therapy (PDT) 8 —but at present, such treatments have not gained widespread popularity due to the instability of effects, need for specific equipment and drugs, and complicated techniques involved. Therefore, there is an urgent need for development of a new simple method for OLP treatment that can improve subjective symptoms and facilitate early healing of OLP.
Until now, several reports have emerged indicating that CO2 laser vaporization therapy helps eradicate OLP and relieve pain. 9 –12 Further, Mucke et al. reported that in erosive OLP, malignant transformation was lower in the group that underwent CO2 laser irradiation than in the group that received symptomatic treatment—such as medications—alone. 13 A CO2 laser is frequently used in the surgical treatment of oral mucosal disease as it acts superficially, has excellent hemostatic ability, is easy to use, and causes little heat damage to surrounding tissues. 14 –16 However, there are a few reports on laser treatment for OLP, and few prospective studies have been conducted.
In the present study, we included patients with clinically and histopathologically diagnosed OLP and conducted a prospective, single-arm intervention study on CO2 laser vaporization therapy to examine its effectiveness.
Methods
Study sample
The study sample comprised 16 patients with clinically and pathologically diagnosed OLP who were examined at the Kobe University Hospital Department of Oral and Maxillofacial Surgery during the 3-year, 7-month period from April 2013 to December 2016 and they had 18 sites in them. There were 2 males and 14 females aged 46–75 years, with a mean age of 62.0 years. The onset site was the buccal mucosa in 14 patients at 15 sites and gingiva in 3 patients at 3 sites, while the clinical appearance (modified from the Andreasen classification 17 ) was of the reticular type at 10 sites, erosive type at 2 sites, papular type at 1 site, and complex type (reticular erosive) at 5 sites.
Study design
As shown in Fig. 1, histological testing was performed for all OLP patients clinically diagnosed using the Andreasen classification. As defined by the World Health Organization (WHO) and other studies, 18 –20 the pathological diagnostic criteria include hyperkeratosis and parakeratosis of the mucosal epithelium, flattening of or serrated changes in the epithelial pedicle, basement cell hydropic degeneration, zonal lymphocyte invasion directly below basement cells, and appearance of civatte bodies. After obtaining informed consent with reference to a flow chart of the present study (Fig. 1), those with clinically and histologically diagnosed OLP lesions underwent continuous conservative treatment for 3 months using an adrenal cortex hormone ointment and azulene sulfonate sodium hydrate gargle. Of patients who showed no improvement, 9 patients with entire 11 sites who consented to participate in the clinical study underwent laser therapy. A CO2 laser (Bell laser; Takara Belmont Corp., Osaka, Japan) was used in this clinical examination. After administration of a local anesthetic, the entire lesion was evenly vaporized in defocused mode until it was carbonized with 3 W using a continuous-wave mode to a depth of ∼1–2 mm (parameter: Table 1). After treatment, antibiotics and analgesics were administered for 3 days. For post-treatment evaluation, we referred to the study design by Buajeeb et al. 21 and used the numerical rating scale (NRS) as an indicator of subjective symptoms, including pain, and the Thongprasom sign score (TSS) as an objective indicator of OLP. 9 Further, the TSS is a scale specific to OLP, in which symptoms are divided according to grades of 0–5; the grades are as follows: grade 0: no lesion; grade 1: mild, reticular, white striae without erythema; grade 2: reticular, white striae with an atrophic area of ≤1 cm 2 ; grade 3: reticular, white striae with an atrophic area of ≥1 cm 2 ; grade 4: reticular, white striae with an erosive area of ≤1 cm 2 ; and grade 5: reticular, white striae with an erosive area of ≥1 cm 2 . These two scales were recorded during examinations performed before treatment and then at 7 days, 1 month, 3 months, 6 months, and 1 year after irradiation (Fig. 2). Further, the TSS at 7 days after irradiation was considered impossible to evaluate because it was during recovery (recorded as X in Table 2).
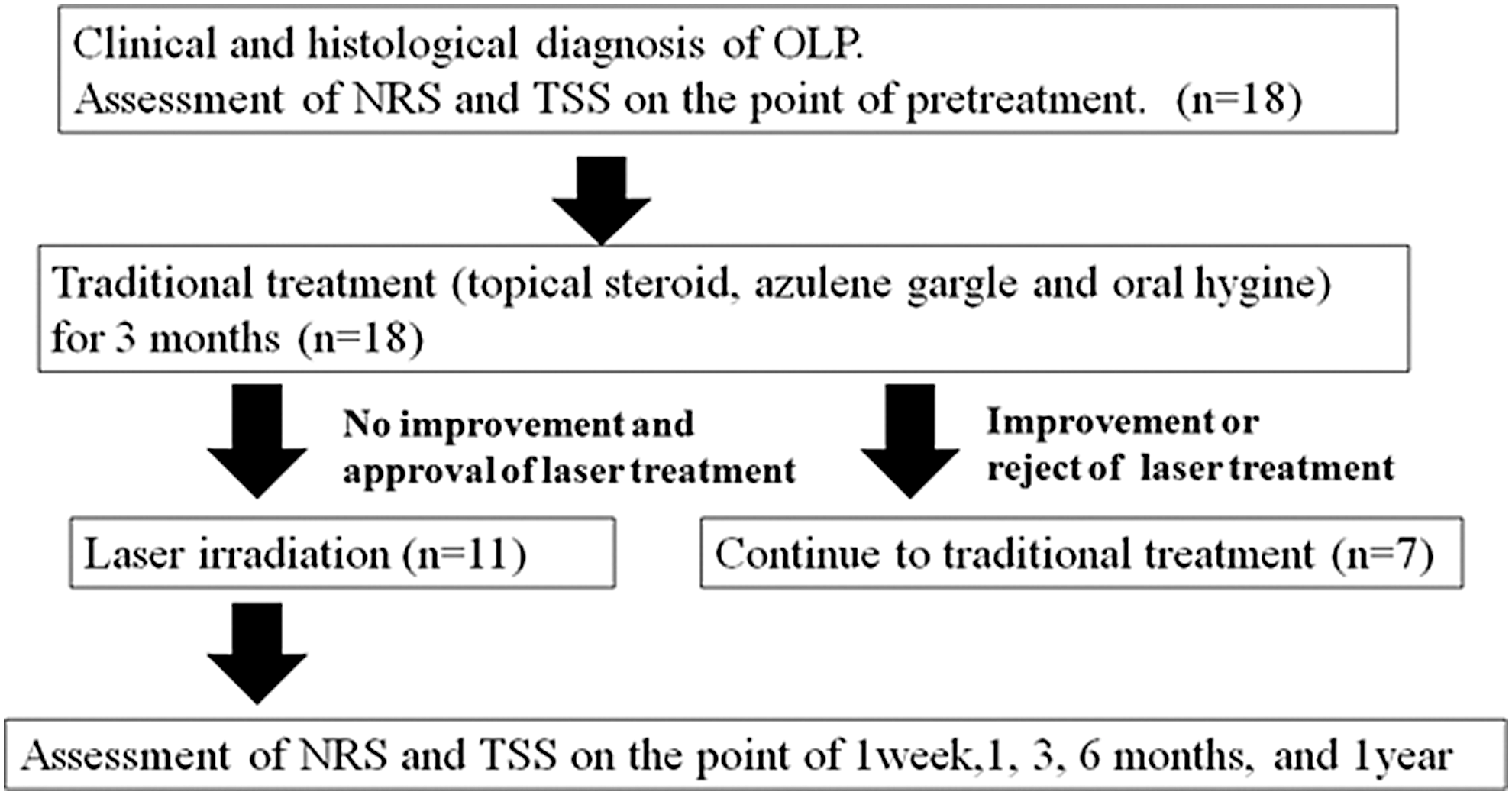
Flow diagram of prospective study.
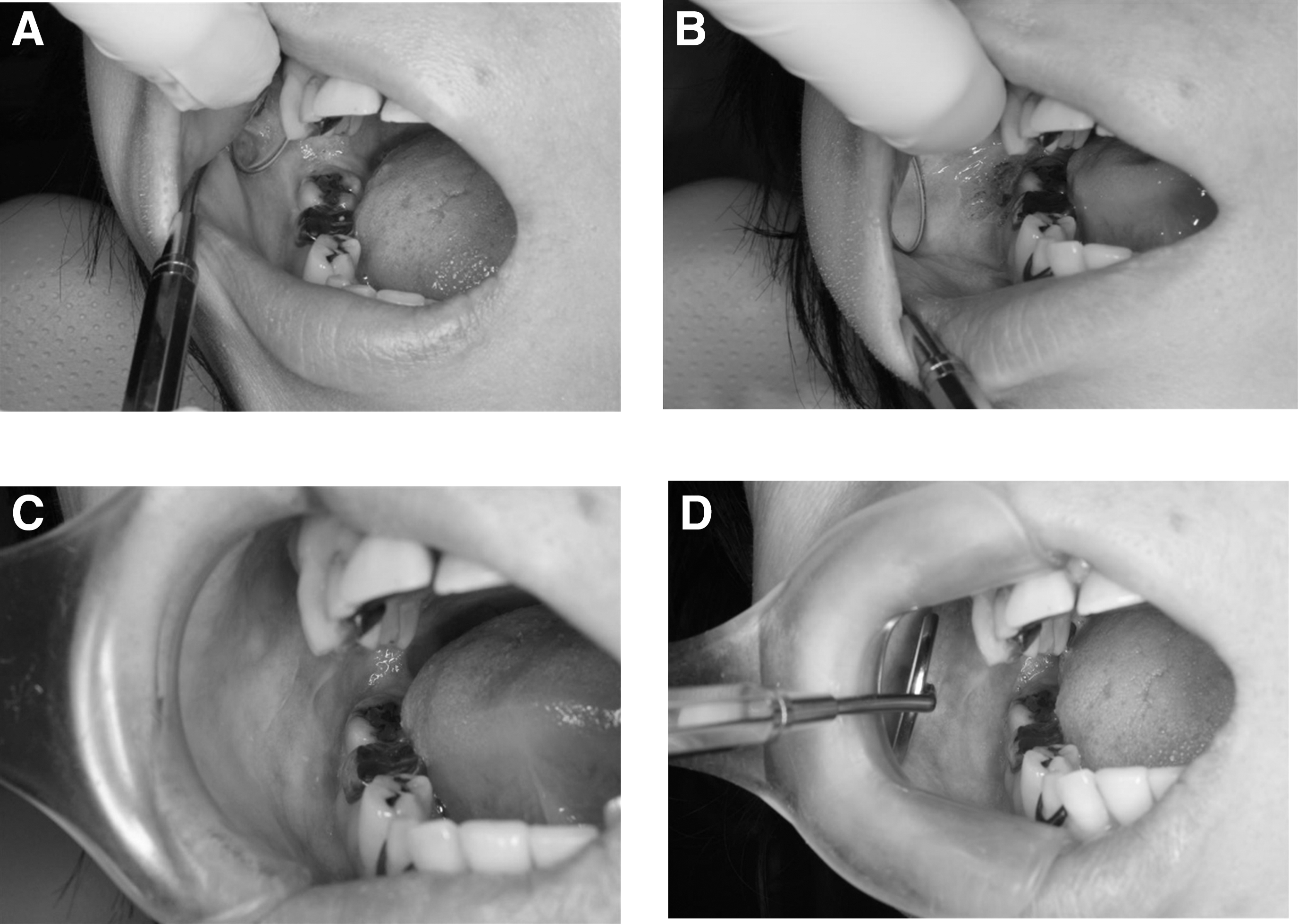
Clinical aspects of OLP of right buccal from preoperative stage to 1 year following CO2 laser vaporization therapy.
Irradiation Parameters
Clinical Data of the Prospective Study Population and Two Scales of the Assessment
X means impossible records of TSS.
NRS, numerical rating scale; TSS, Thongprasom sign score.
Clinical diagnosis, tissue biopsy, evaluation at the time of laser irradiation, and follow-up observation were performed or managed by three oral surgeons specializing in oral mucosal disease who were also laser specialists. Further, the pathological diagnosis was limited to several pathological diagnosis specialists. The present clinical study was performed with the approval of the Ethics Review Board of Kobe University Hospital (April 2013, approval no.: 1416).
Statistical analysis
For statistical evaluations of the efficacy of laser irradiation, values of the NRS score and TSS were examined by Wilcoxon's signed-rank test before treatment and then at 1 month, 3 months, 6 months, and 1 year following treatment. A difference between each phase and the preoperative period was deemed statistically significant at p < 0.05.
Results
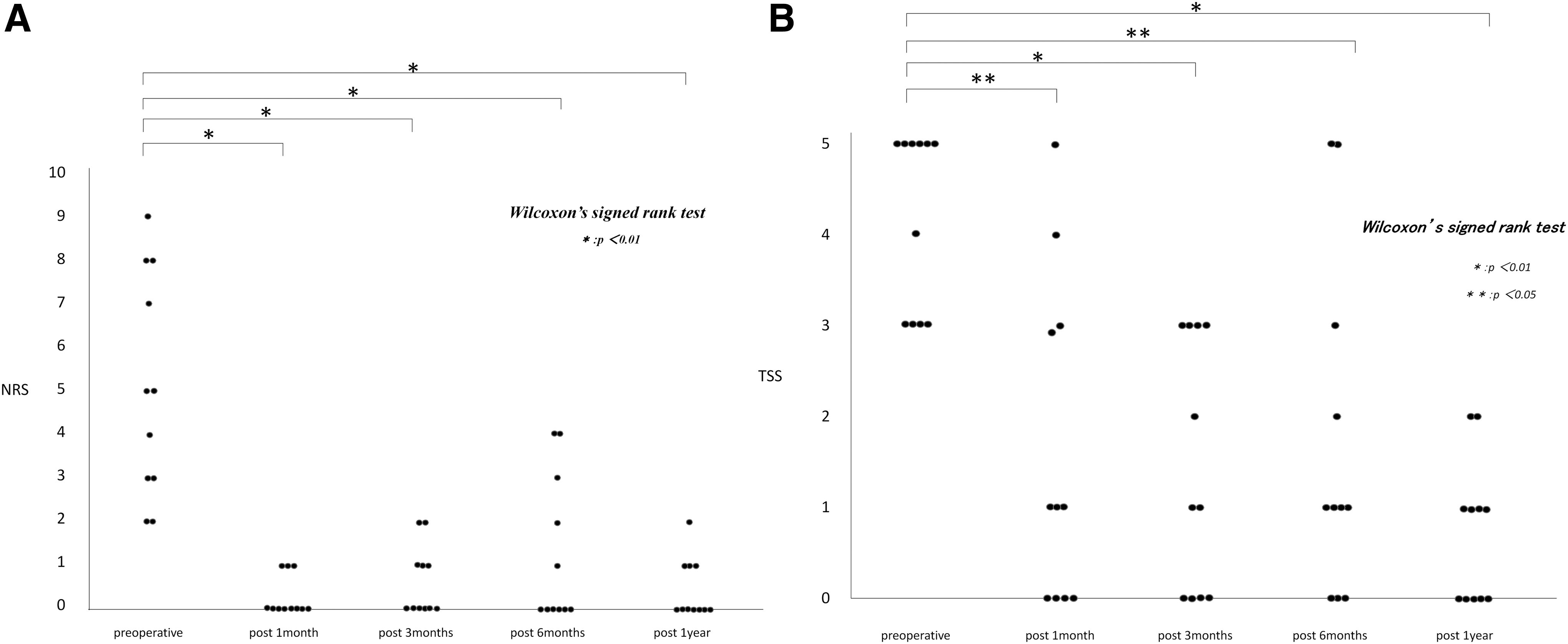
The present study included 16 patients with clinically and pathologically diagnosed OLP, with 18 sites in them. All patents underwent conservative treatment. Seven patients with seven sites showed an improvement in symptoms or refused laser irradiation and were thus excluded from the laser treatment group (Table 2 and Fig. 1). Laser irradiation was administered to nine patients with 11 sites, and the NRS score decreased at 5 of the 11 sites (45.5%) at day 7 compared with the preirradiation scores and at all 11 sites (100%) at 1 month, 3 months, and 1 year after irradiation (Table 2 and Fig. 1). The TSS decreased at eight sites (72.7%) at 1 month after irradiation compared with the preirradiation scores and at least nine sites (81.8%) from 3 months to 1 year after irradiation. Further, the NRS score and TSS at 1 year after irradiation showed a complete recovery of zero in three sites (27.3%). Wilcoxon's signed-rank test revealed that the mean NRS score and TSS were statistically lower (p < 0.05) at 1 and 3 months (short-term evaluation period) and at 6 months and 1 year (mid-long-term evaluation period) after irradiation than the preirradiation scores (Fig. 3). There were no patients with malignant transformation during the study period.
Score of NRS
Discussion
Study subjects
According to the WHO classification, 18 OLP is considered to be a clinical pathology with a significantly high risk of malignant transformation to squamous cell carcinoma (precancerous state) as is the case in oral submucosal fibrosis, systemic lupus erythematosus, Plummer–Vinson syndrome, and oral syphilis. Malignant transformation of OLP reportedly occurs in 0.07–5.8% of cases 2 ; thus, control of the disease is considered very important. However, according to the reports, 22,23 it is difficult to distinguish OLP and an oral lichenoid lesion (OLL) based on a histopathological diagnosis. An OLL is a structural change assumed or confirmed to be caused by a metal allergy, graft-versus-host disease, drugs, and systemic disease. van der Meji et al. 24 reported that of lesions diagnosed as OLP, all lesions that developed malignant transformation that did not clinically and pathologically satisfy the diagnostic criteria of OLP were retrospectively found to be OLLs. Thus, OLLs might be more likely to undergo malignant transformation than OLP or OLP might have changed from OLLs into a state likely to undergo malignant transformation. Therefore, OLP diagnosis, differentiation, and malignant transformation are largely unclear. We believe that this contributed to there being only a small number of interventional studies on new treatments and the difficulty in establishing a standard treatment.
Effectiveness of CO2 laser vaporization therapy for OLP
On performing laser irradiation, a statistically significant difference was observed in the NRS score and TSS at each time point from 1 month to 1 year after irradiation compared with preirradiation scores. Therefore, an improvement in subjective symptoms and the clinical inspective condition was considered possible in the short term, and it appeared that in the mid-term too, treatment would make exacerbation of OLP unlikely.
Regarding the evaluation period following laser irradiation, at 1 month after irradiation, subjects with a relatively large lesion area might still be in the process of being healed, suggesting that setting the short-term evaluation period to 2–3 months was appropriate. There was no statistically significant difference in the mean NRS score (p = 0.082) at 7 days after irradiation compared with preirradiation scores; however, the NRS score at this stage took into account wound pain following laser irradiation and was not derived from OLP; thus, with the present treatment, administration of analgesics was thought to be necessary after 7 days of irradiation. In cases ② and ⑪, despite an improvement shown at 3 months after irradiation, the TSS at 6 months after irradiation was equal or greater than the score measured before irradiation; after 1 year had passed, the TSS had decreased in both patients (Table 2). Therefore, the stability of symptoms following laser irradiation may be affected by other factors, including oral hygiene. In the present study, there were no set criteria for determining recurrence. However, if recurrence was to be defined as the TSS at 1 year equal to or greater than the preirradiation score, this would indicate recurrence in one patient at one site (9.1%). However, as this site showed an improvement in the NRS score, we believe that the effectiveness of the treatment cannot be entirely ruled out. van der Hem et al. 9 reported that recurrence without pain following CO2 laser vaporization therapy for OLP occurred in 38% of cases and that recurrence with pain occurred in 15%; in our study, compared with these results, there was less pain and a lower rate of recurrence. However, as in the study by van der Hem et al. where the follow-up observation period lasted several years, it might have been better if a long-term follow-up of recurrence and malignant transformation was conducted in the present study.
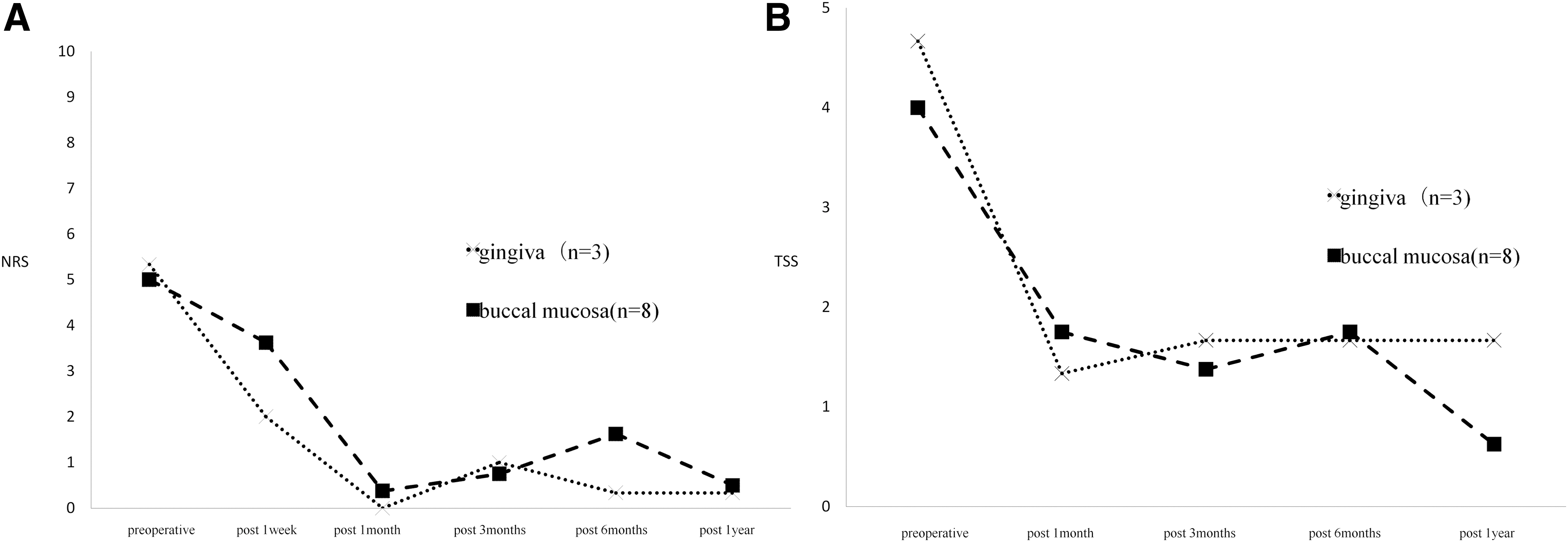
Upon examination of lesion site (buccal mucosa and gingiva), on the basis of results of the mean NRS score and TSS, the effects were found to be somewhat greater for gingiva. There was, however, a bias in the number of subjects, which makes this difficult to verify (Fig. 4). When results were examined by clinical appearance, no major differences were observed in the change in the mean NRS score. While the mean TSS tended to show exacerbation of the clinical inspective condition in the complex type, in this respect too, there was a bias in the number of subjects, making it difficult to verify (Fig. 5). In the present study, OLP lesions of ∼2 mm from the superficial layer of the mucosa were treated by efficient vaporization in order from the superficial layer with a CO2 laser at wavelength of 10.6 μm. To avoid remnants of nonirradiated sites, we selected the continuous-wave mode, which emits a continuous laser beam. Further, to prevent residual lesions and reach a sufficient depth, we believe that performing irradiation using a technique integrating regular horizontal irradiation and overlapping irradiation, as described in a book, 25 led to effective results.
The mean scores of NRS
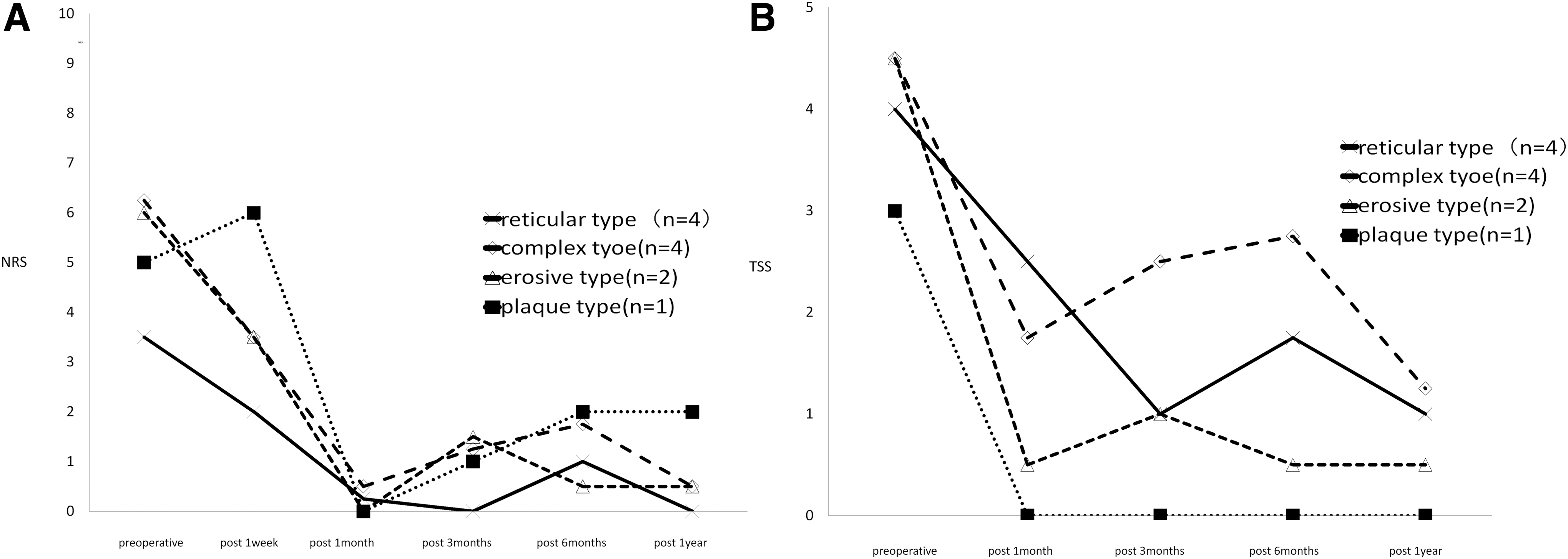
The mean scores of NRS
Comparison with other treatment methods and possibility of popularizing this treatment
The CO2 laser has high energy efficiency for tissues with high water content and is mostly absorbed at about 200 μm from the irradiated surface. CO2 laser is thought to be a suitable device for clinical use because of its property and adequate depth of tissue penetration for the OLP in the buccal mucosa and gingival mucosal surface in the oral cavity. Moreover, it has less harmful effects on deep tissues, such as bones, periosteum, muscles, nerves, and blood vessels.
On comparing recent reports, Ito et al. reported that conservative treatment using topical application of various drugs resulted in good control in ∼70% of patients and required 2–6 weeks. 5 In the present study, subjective symptoms improved at 1 year after irradiation in all patients, while ∼90% of patients showed an improvement in their clinical inspective condition. Therefore, we consider these to be better results than those. Further, Sobaniec et al. 8 reported that PDT resulted in recovery or partial recovery with lesion shrinkage in 81% of cases. However, PDT specifically eradicates cancer cells by primarily clustering tumor-affinity photosensitizers and by excitation of light. As application of PDT for OLP is considered as being technically complicated and requiring several treatments, this treatment is not originally indicated for OLP and appears unlikely to become popular. In contrast, CO2 laser therapy can be administered at many institutions, and because the procedure is simple, it is likely to become more widespread. We believe that it has the following advantage: for OLP patients with residual lesions or recurrence, repeat treatment is easily administered. Further, as noted above, while some patients showed no improvement in the TSS in the present study, all patients showed an improvement in the NRS score; therefore, at this point in time, all patients received several benefits. However, for patients with recurrence and pain, we are considering performing repeat biopsy and repeat irradiation.
Requirements of performing CO2 laser therapy for OLP and future outlooks
In the present study, we primarily reported that a new simple treatment that can alleviate subjective symptoms and achieve early recovery is anticipated; however, as mentioned above, differentiation with OLLs and other mucosal diseases is necessary, and there is a risk of malignant transformation and exacerbation, which, we believe, should be avoided by performing simple laser irradiation for OLP. Necessary conditions when administering the present treatment include an environment where related departments can cooperate, thereby enabling an adequate pathological diagnosis of OLP, and where expert knowledge and experience in treating oral mucosal diseases and performing laser therapy can be provided. Further, as the present study included a small study sample with a short follow-up observation period, we believe that a larger study sample with long-term follow-up observation is needed going forward.
Conclusions
We conducted a single-arm clinical trial of CO2 laser vaporization therapy for OLP, in which we examined subjective symptoms and the objective pathological condition for 1 year following irradiation to evaluate its effectiveness.
Footnotes
Acknowledgments
This work was supported, in part, by a grant of the Tanaka (cancer and orphan disease) Foundation from the Osaka Community Foundation.
Author Disclosure Statement
No competing financial interests exist.