
Abstract
Objective:
The aim of this research is to study skin autofluorescence and the associations between skin glycated proteins and clinical characteristics of healthy and unhealthy subjects for noninvasive screening of diabetes and cardiovascular disease (CVD) risks.
Background data:
Accumulated advanced glycation endproducts (AGEs) promote increased oxidative stress and inflammation, as well as cross-linking of proteins leading to tissue damage and several diseases, including diabetes.
Materials and methods:
One hundred and four subjects with or without diabetes and stroke aged 20–80 years and with Fitzpatrick skin type (I to IV) participated in this study. The fluorescence spectrometer was used to illuminate a skin surface of 1 cm2. The skin of forearm was positioned on the spectrometer to assess skin AGEs. Anthropometric data and body composition also were evaluated.
Results:
Elevated skin autofluorescence was found in subjects >50 years old, as well as in patients with insulin resistance (IR), diabetes, and stroke. There was a positive correlation between the skin autofluorescence and age (r = 0.7, p = 0.0001), body mass index (BMI) (r = 0.5, p = 0.001), body fat (r = 0.5, p = 0.0001), waist circumference (r = 0.45, p = 0.001), and systolic blood pressure (BP) (r = 0.45, p = 0.0001).
Conclusions:
Elevated skin autofluorescence can provide a noninvasive screening of diabetes and CVD risks.
Introduction
Maillard reaction denotes a nonenzymatic glycation process. It is a series of complex biochemical reactions, including the Schiff's base (interaction between the aldehyde group of glucose and amino group on proteins, lipids, and nucleic acids), the Amadori's product (the initial Schiff's base undergoes rearrangements to a stable ketoamine, leading to reactive carbonyl compounds), and formation of advanced glycation endproducts (AGEs), such as pentosidine, carboxymethyllysine, and glucosepane. 1,2
AGEs are formed during normal life cycle stages. However, an accelerated AGEs deposition/formation is found in patients with diabetes due to biophysical, biochemical, molecular, and functional changes. Then, AGEs may be used as biomarker for diabetes due to elevated glycation level. 3 Accumulated AGEs promote increased oxidative stress and inflammation, as well as cross-linking of proteins, which lead to tissue damage and several diseases, including micro- and macrovascular dysfunction. Vascular complication contributes to neuropathy, nephropathy, retinopathy, myocardial infarction, and stroke. Therefore, accumulated AGEs may be used as biomarker for cardiovascular diseases (CVDs) due to accelerated atherosclerotic process. 4
Glycated hemoglobin (HbA1c) is an invasive technique (blood test) of metabolic control analysis for prevention and/or early treatment of diabetes and its complications. Moreover, this technique is expensive and time consuming, as well as require laboratory environment and specialized professionals. Another invasive technique to assess the AGEs is skin biopsies for immunohistochemistry analysis. 2 However, glycated proteins can be assessed by noninvasive optical systems, as the fluorescence and Raman spectroscopies of skin. 5,6 Several studies 7 –9 have shown significative correlation between HbA1c and skin autofluorescence.
The light–matter interaction has been used in the biophysical, biochemical, and molecular biology studies. The fluorescence phenomenon is based on principles of quantum physics and chemistry. There are electronic transitions between fundamental and excited states in which the molecule absorbs and re-emits energy at a longer wavelength. The relaxation phenomenon of excited molecules is an internal conversion of electronic energy in the molecule to rotational and vibrational modes, characterizing a broad band of the fluorescence spectrum. The fluorophores absorb light at a given wavelength and, at few nanoseconds, emit light at a different (longer) wavelength. 10 A fluorescent molecule is characterized by their specific excitation/emission peaks. Then, the structure and composition of biological tissues may be investigated by fluorescence techniques. The main skin endogenous fluorophores are tryptophan, nicotinamide adenine dinucleotides (NAD and NADH), collagen cross-links (for example, pentosidine), elastin, and keratin, which may be assessed by autofluorescence. 5
For reduction of morbidity and mortality of diabetic patients and CVD patients, a rapid screening is necessary for prevention and intervention programs. Given the importance of the theme, the AGEs as biomarker for risk of diabetes and CVDs by skin autofluorescence need to be better investigated. The aim of this research is to study skin autofluorescence and the associations between skin glycated proteins and clinical characteristics of healthy and unhealthy subjects for noninvasive screening of diabetes and CVD risks.
Materials and Methods
This study was approved by the Ethics Committee of the Federal University of São Carlos (UFSCar) in São Carlos, Brazil (approval no. 1.891.369). All subjects provided written informed consent and agreed to participate in the study.
One hundred and thirty subjects were invited to participate in the cross-sectional study. Inclusion criteria were subjects with or without stroke (hemiplegia) and/or diabetes (types 1 and 2) aged 20–80 years. The health conditions [insulin resistance (IR), diabetes, and stroke] were defined during anamnesis and physical examination. Subjects who self-reported that their doctor had told them they had IR or diabetes were defined as having an IR or diabetes diagnosis. Exclusion criteria were subjects with Fitzpatrick skin types V and VI,
11
bedridden patients, psychiatric and malignant diseases, as well as injuries in forearm skin. Twenty-six subjects did not attend due to exclusion criteria (n = 22) or a change of mind about participating (n = 4). Therefore, 104 subjects (n = 104) were separated into nine groups according to age range and health conditions: Group 20–30 years old: nondiabetic subjects and without stroke aged 20–30 years (n = 18); Group 30–40 years old: nondiabetic subjects and without stroke aged 30–40 years (n = 10); Group 40–50 years old: nondiabetic subjects and without stroke aged 40–50 years (n = 14); Group 50–60 years old: nondiabetic subjects and without stroke aged 50–60 years (n = 12); Group >60 years old: nondiabetic subjects and without stroke more than the age of 60 years (n = 11); Group IR: subjects with IR, but without stroke (n = 8); Group diabetes: subjects with diabetes, but without stroke (n = 13); Group stroke: nondiabetic subjects with stroke (n = 13); Group stroke plus diabetes: subjects with stroke and diabetes (n = 6).
After anamnesis, skin autofluorescence and clinical and anthropometric characteristics were carried out in a laboratory at an air temperature between 22°C and 24°C and a relative humidity between 50% and 60%, at the same time of day. The clinical procedure is shown in Fig. 1.

Clinical procedure.
Skin Autofluorescence
The skin of forearm was cleaned with 70% alcohol, dried, and positioned on the spectrometer to analyze skin glycated protein. The fluorescence spectrometer (AGE Reader, DiagnOptics Technologies B.V., The Netherlands) was used to illuminate a skin surface of 1 cm2 safeguarded against environmental light. According to Meerwaldt et al., 12 Mulder et al. 13 and Koetsier et al., 14 this system includes an LED excitation source between 300 and 420 nm with a peak at ∼350 nm, intensity <1 mW/cm2, and an emission measured in the 420–600 nm range by a fiber optics CCD spectrometer. Skin autofluorescence was calculated by a ratio between the light emission intensity (420–600 nm) and light excitation intensity (300–420 nm), multiplied by 100 and expressed in arbitrary units (a.u.). The autofluorescence signal was normalized by the reflection intensity of the excitation LED to correct effects of the skin color, according to the manufacturer. Three measurements were performed to obtain an average score. In addition, the AGE Reader software indicates cardiovascular (CV) risk through a color map based on skin autofluorescence score and age range [green: no increased CV risk (normal); yellow: limited increase of CV risk (risk I); orange: increased CV risk (risk II), and; red: definite CV risk (risk III)].
Assessment of Clinical and Anthropometric Characteristics
Clinical and anthropometric characteristics were measured as previously described. 15 Anthropometric data were used to determine the body mass index [BMI, body weight (kg) divided by height (m)2] and waist hip ratio [WHR, waist circumference (cm) divided by hip circumference (cm)]. Percentage body fat was determined through bipolar electrical bioimpedance of the upper limbs (OMRON®, Kyoto, Japan). The systolic and diastolic blood pressures (BPs) were measured by the auscultatory method using an aneroid sphygmomanometer and a stethoscope during rest. To monitor the heart rate (HR) during rest, a pulse oximeter (Moriya, Sao Paulo, Brazil) was used.
Statistical analysis
Measurements were shown by mean and standard deviations. Statistica for Windows Release 7 software (Statsoft, Inc., Tulsa, Ok) was used for statistical analysis and the significance level was set at 5% (p < 0.05). The Shapiro–Wilk test was used to analyze normality. The Kruskal–Wallis test was used for intergroup comparisons. The Spearman's correlation coefficient was used to investigate the relationship between the key variables. In addition, multiple logistic regression analysis was also performed, considering skin autofluorescene as dependent variable.
Results
Clinical characteristics, skin autofluorescence, and CV risk are shown in Table 1. Skin autofluorescence score showed a significantly negative effect of AGEs in subjects >50 years old, as well as in patients with IR, diabetes, and stroke (Fig. 2, p < 0.05)
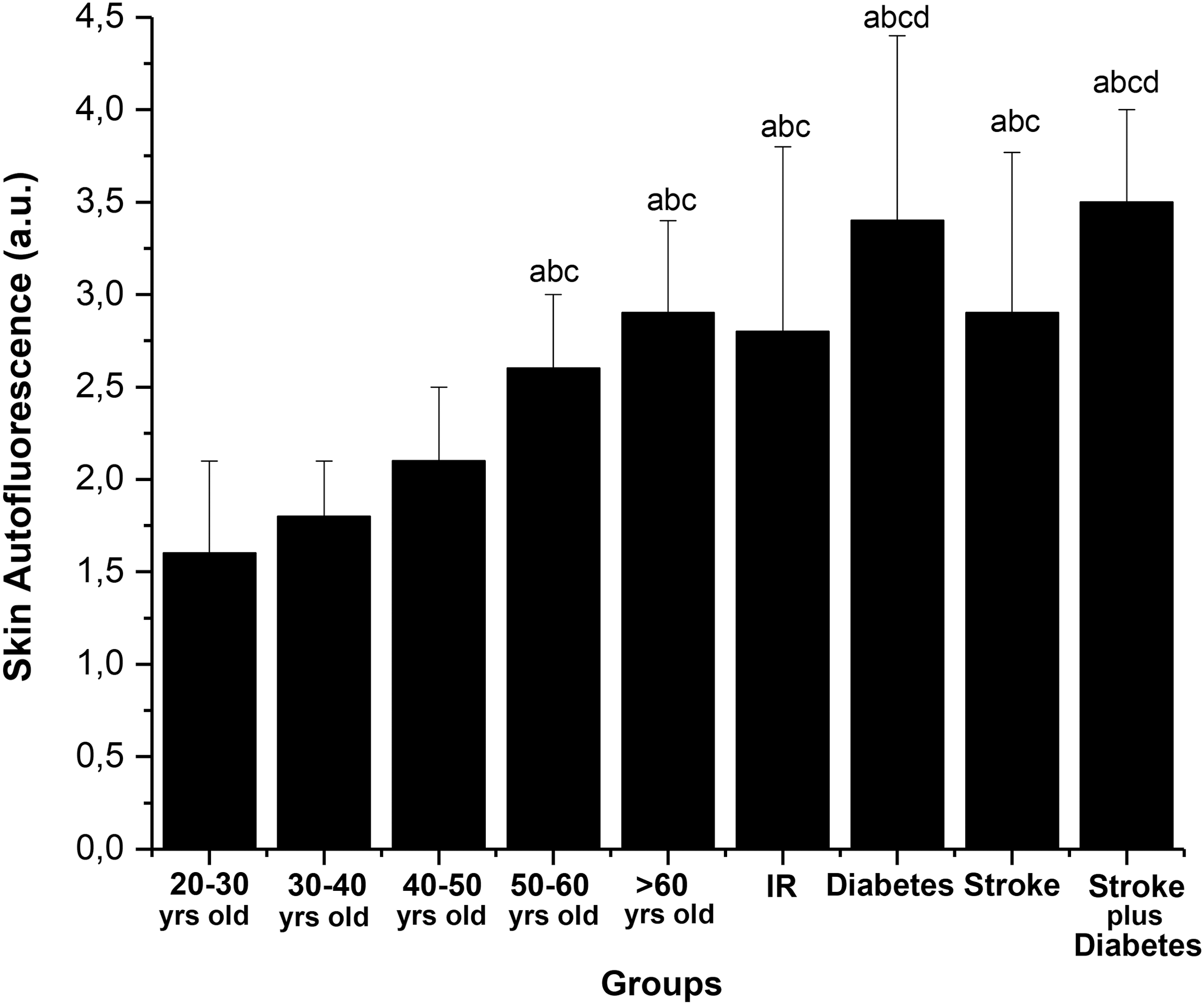
Skin autofluorescence. For the values of mean and standard deviation, the letters a, b, c, and d denote, respectively, significant differences compared with the groups 20–30 years old, 30–40 years old, 40–50 years old, and 50–60 years old (Kruskal–Wallis, p < 0.05). IR, insulin resistance.
Clinical Characteristics, Skin Autofluorescence, and Cardiovascular Risk
For the values of mean and standard deviation, the letters a, b, c, d, e, f, and g denote, respectively, significant differences compared with the groups 20–30 years old, 30–40 years old, 40–50 years old, 50–60 years old, >60 years old, IR, and diabetes (Kruskal–Wallis, p < 0.05).
BP, blood pressure; CV, cardiovascular; IR, insulin resistance.
Demographic characteristics, CV risk factors, and life habits are listed in Table 2. Regarding anthropometric characteristics, the >60 years old, IR, diabetes, stroke, and stroke plus diabetes groups showed values significantly higher (p < 0.05) for body mass, BMI, waist circumference, hip circumference, WHR, and body fat (Table 3).
Demographic Characteristics, Cardiovascular Risk Factors, and Life Habits
Anthropometric Characteristics
For the values of mean and standard deviation, the letters a, b, c, d, e, f, and g denote, respectively, significant differences compared with the groups 20–30 years old, 30–40 years old, 40–50 years old, 50–60 years old, >60 years old, IR, and diabetes (Kruskal–Wallis, p < 0.05). Reference values: BMI of 30 kg/m2 or higher indicates obesity; BMI between 18.5 and 29.9 kg/m2 indicates nonobesity; central obesity is defined as waist circumference ≥88 cm for women and ≥102 cm for men; WHR >0.8 indicates central (android) fat; WHR between 0.68 and 0.8 indicates peripheral (gynoid) fat.
BMI, body mass index; WHR, waist hip ratio.
The relationship between the key variables is shown in Figs. 3 and 4. There was a strong and positive correlation between the skin autofluorescence and age (r = 0.7, p = 0.0001). There were also moderate and positive correlations between skin autofluorescence and BMI (r = 0.5, p = 0.001), body fat (r = 0.5, p = 0.0001), waist (r = 0.45, p = 0.001), and systolic BP (r = 0.45, p = 0.0001). Multiple logistic regression analysis was performed, considering the skin autofluorescence as dependent variable. It showed a correlation with age (p = 0.00001), body mass (p = 0.01), and BMI (p = 0.02).
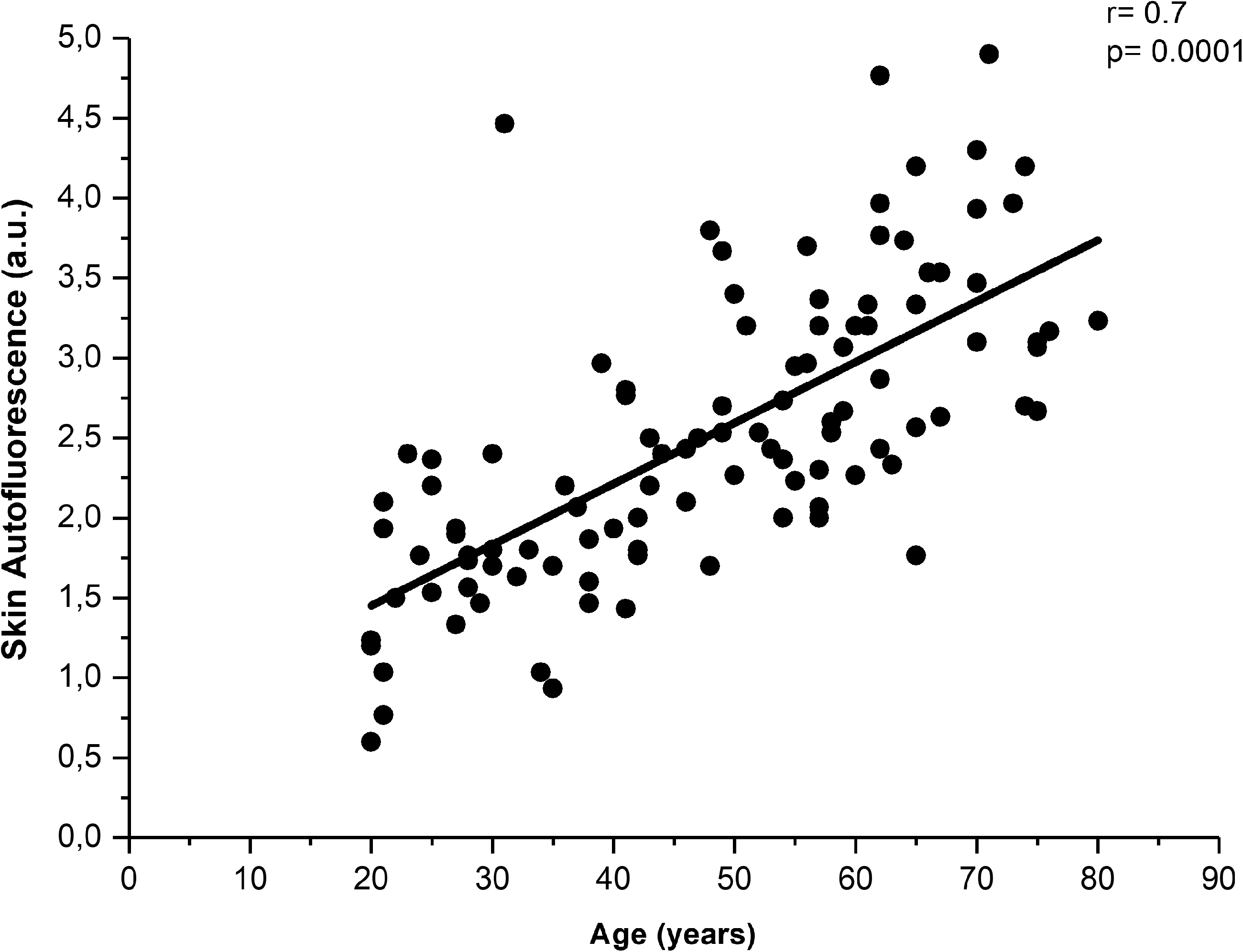
Strong and positive correlation between variables. Skin autofluorescence as a function of age in 104 subjects. The regression lines represent both the average of the skin autofluorescence and age. The regression was strong, positive, and statistically significant (p < 0.05), indicating elevated skin autofluorescence and chronological aging.

Moderate and positive correlations between variables. Skin autofluorescence as a function of BMI
Discussion
This study used noninvasive measurements for clinical practice and showed that subjects >50 years old, as well as patients with IR, diabetes, and stroke have elevated skin glycated proteins, developing features that can lead to the metabolic syndrome (MetS) and CVD. MetS is evidenced by central obesity, IR, diabetes, hypertension, and dyslipidemia. Diagnosis of the MetS is given when at least three of the five mentioned criteria are found. 16,17 In this context, our results showed that age, BMI, body fat, waist circumference, and systolic BP had a positive correlation with skin autofluorescence. In addition, there is a higher prevalence of central obesity, hypertension, and dyslipdemia in subjects >50 years old, as well as in patients with IR, diabetes, and stroke.
Several clinical trials show that the skin autofluorescence has positive correlations with fasting blood glucose, 18 HbA1c, 19 cholesterol, triglycerides, and creatinine. 20 In skin biopsy, there was positive correlation between skin autofluorescence and AGEs levels (pentosidine, carboxymethyl-lysine, and carboxyethyllysine) in human skin biopsy. 12 Similar results were found in an animal model, using porcine skin. 3 AGEs are formed during weeks or months, involving condensations, rearrangements, and oxidative changes until reaching an irreversible stage of AGEs. Therefore, our study shows that an accumulated AGEs skin leads to an elevated skin autofluorescence and it correlates with MetS. 21
Skin autofluorescence is strongly influenced by age. 13 Then, there was larger skin AGEs content according to increase in age from 20 to 80 years. It indicates increased risk of diabetes, MetS, and CVD mainly for subjects >50 years old due to chronological aging, which lead to structural and functional changes (in skin, CV, muscle, bone, and other systems) together with reduced total energy expenditure and increase of fat body percentage.
Elevated waist circumference, WHR, BMI, and body fat indicate central obesity. These cardiometabolic risk factors in nondiabetic subjects enhance oxidative stress, leading to IR, β cell dysfunction, and diabetes. 21 In our study, nondiabetic subjects >50 years old show clinical features to develop diabetes that together with elevated skin AGEs assessed by fluorescence may predict diabetes risk. Moreover, diabetic subjects with and without stroke also showed higher skin autofluorescence due to accelerated accumulation of AGEs that occur due to hyperglycemia and oxidative stress, promoting noninvasive diabetes screening. In this context, AGEs fluorescence is considered a biomarker for risk of diabetes patients.
AGEs are found in several body compartments, such as in skin, eye lens, urine, cartilage, and blood. AGEs induce tissue damage mainly through formation of cross-linking between proteins, for example, keratin, collagen, and elastin. Thus, the formation of cross-links between proteins in the extracellular matrix contributes to vascular occlusion and changes in the walls of blood vessels, for example, stiffening. Further, the intracellular formation of AGEs involves intermediate products of glucose metabolism, altering the structure and function of proteins. Another mechanism of deleterious effects is evidenced by changes in the immune system, including interaction of AGEs with receptors (e.g. receptors for AGEs) that may activate proinflammatory cytokines and coagulant systems. 22 In addition to the interaction of AGEs with proteins, glycation reactions can also occur, for example, with low-density lipoprotein (LDL) phospholipids, leading to functional alterations and oxidative changes, thus, glycated LDL stimulates the synthesis of cholesterol in cells, which results in the formation of free radicals and cellular oxidative stress. These action mechanisms accelerate the atherosclerotic process. 2 The carotid and/or coronary atherosclerosis can result in myocardial infarction and stroke. In this context, elevated skin autofluorescence found in our study, mainly in patients with diabetes and stroke, indicates accumulated skin AGEs, and it reflects CVD or CVD risk. Interestingly, hypertension also shows relationship with skin autofluorescence, possibly due to vascular alteration, including occlusion and stiffening 23 as well as inhibition of nitric oxide-mediated vasodilatation. 24
AGEs are also found in the industrialized food or common food with processing methods of broiling, searing, and frying. Some examples are cookies, chocolate, coffee, and french fries. Coincidentally, some of these foods contain high amounts of saturated fat. Another source of AGEs is tobacco, which also promotes oxidative stress. Then, food and life habits could potentially contribute for IR, diabetes, and CVD. 25 Then, larger BMI, body fat, and waist circumference may also reflect an inadequate consumption of food AGEs, which lead to central obesity and accumulated skin AGEs as evidenced by autofluorescence. 26 Tobacco did not influence the current study, because only one subject was a smoker. Regarding sedentarism, the prevalence was higher in patients with stroke, possibly due to disability. Sedentary lifestyle also did not influence this study.
Therefore, the correlation between AGEs and age explains only part of the results, indicating chronological aging. Regarding another part of the results, skin autofluorescence was similar between middle-aged or elderly subjects and patients with IR or stroke, indicating diabetes risk. Diabetic patients with and without stroke showed higher skin autofluorescence than healthy adults, due to highly accelerated AGEs, indicating diabetes diagnosis. In addition, correlations between AGEs and clinical variables (BMI, body fat, waist, and systolic BP) converge to indicate MetS and CVD risks. Although these variables are not valid for a clinical decision, the correlations contribute to a better understanding of the pathophysiological aspects.
Finally, this noninvasive screening can be made by different health professionals in various places, for example, clinics, pharmacies, gymnasiums, schools, and public events to reach a larger number of people, mainly subjects without clinically manifest diabetes and CVD. However, after screening, a more specific test should be performed to diagnose.
Conclusions
Skin autofluorescence is a noninvasive, fast, and safe procedure. This testing does not need fasting and the measurements can be performed outside the laboratory environment without generating any pain. Moreover, another advantage is that systems based on LEDs for fluorescence spectroscopy have a low operational cost. Elevated skin AGEs and development of features that can lead to MetS and CVDs were found in subjects >50 years old, as well as in patients with IR, diabetes, and stroke. Then, elevated skin autofluorescence is a biomarker for the noninvasive screening of diabetes and CVD risks.
Footnotes
Acknowledgments
We would like to thank the São Paulo Research Foundation (FAPESP)—grant nos. 2013/14001-9 and 2013/07276-1 (CEPOF–CEPID Program).
Author Disclosure Statement
The authors declare that they have no conflict of interest.