
Abstract
Objective:
To clinically evaluate the effect of the violet light-emitted diode (LED) light (405–410 nm) associated to in-office dental bleaching with 35% carbamide peroxide, on tooth color change and sensitivity. Participant's satisfaction after treatment was also evaluated.
Materials and methods:
A total of 50 participants were selected and randomized into a treatment group (n = 25): G1–two bleaching sessions of 30 min each, with 7-day interval (D0 and D7); G2—two bleaching sessions (same protocol as G1) associated with violet LED light, 30 min each session. The color evaluation was performed before and after 7 days of the second session (D0 and D14); the medium third of buccal surface of canine and central incisor teeth were evaluated under VITA Shade Guide and spectrophotometry (subjective and objective). Tooth sensitivity was evaluated immediately after the treatment and after 48 h of each bleaching session (D0, D2, D7, and D9), and a self-perception questionnaire was applied on D14.
Results:
Data were subjected to nonparametric Mann–Whitney test and both canine and central incisor teeth presented color change. Group G2 showed significantly more change than G1. Fisher's exact test showed no statistically significant dental sensitivity differences between groups. Both groups reported a high level of satisfaction but chi-square test showed statistically higher satisfied patients with dental bleaching in G2 than G1.
Conclusions:
The violet LED light (405–410 nm) could improve dental bleaching effectiveness, without sensitivity increase.
Introduction
Esthetics has been increasingly gaining prominence in dentistry, reflecting a growing demand of patients in search for a better appearance, assuming a harmonic white smile as a highly relevant aspect. 1
Frequently, vital teeth present color alterations that may compromise esthetics. Among the cosmetic procedures used to remove the pigments, dental bleaching is the least invasive treatment. 2 This method is widely used because of its effectiveness and safety for dental hard tissue compared with prosthetic treatment. 3 However, the underlying effects of this technique on dental hard tissues remain controversial. 2
The in-office bleaching procedure uses chemical substances with high potential for free oxygen radicals release, such as hydrogen peroxide (HP) or one of its precursors, notably carbamide peroxide (CP). Free radicals diffuse through the enamel and dentin and because they are extremely electrophilic and unstable they attack most organic molecules, and the target molecules are pigments. 2,4 Then, pigments are disrupted into small molecules creating a successful whitening action. However, the bleaching process is slow and high concentrations of HP are necessary for in-office treatment. In this process, HP can break down carbon backbones of enamel and dentin proteins impairing elastic modulus, microhardness, and toughness. In addition, HP concentration increased on pulp may induce adverse clinical effects such as dental sensitivity. 2,4 –6
Thus, various devices at different wavelength spectra and radiation energies, such as halogen, light-emitted diodes (LEDs), diode lasers, argon lasers, and plasma arc lamps have been suggested as an adjunctive tool to accelerate HP decomposition by thermal and physical processes. 5,7 –11 However, as an alternative to the conventional bleaching treatment with HP-based agents, a new LED device using violet wavelength (405–410 nm) has been introduced. 12 –14 This wavelength coincides with the absorption pike of the pigmented molecules of the dentin. According to Zanin, the pigmented molecules are photosensitive and highly reactive at this wavelength. 8,13 Being so, the interaction of the light and the pigment occurs selectively and the device light is capable to break the macromolecules into smaller molecules. Because of the fact that pigment molecules are physically broken, side effects caused by chemical agents used in the conventional technique are avoided. 8,9,10,14 Lago et al. reported a clinical case applying the violet LED in a young patient's teeth in three 30-min sessions with interval of 7 days and teeth bleached from A3 to A1 (corresponding to 9 units on VITA Shade Guide). 9
Although the bleaching agents could be dispensable when using a violet LED, its association to this new light source (405–410 nm) is expected to improve the bleaching process.
Klaric et al. reported in an in vitro study the effect of 405 nm violet LED on dental bleaching associated with different concentrations of HP and CP on hydroxyapatite pastilles. The same results were obtained with the protocols that associated violet LEDs with 38% HP or 30% CP. 15
de Souza Rastelli et al. demonstrated, in a clinical report, that in-office dental bleaching was successfully achieved with 10% CP associated with violet LED irradiation for 30 min and no dental sensitivity was recorded. 10
However, considering its recent introduction in the market and that there are still few studies in the literature, more laboratorial and clinical investigations on the effectiveness and side effects are required on the single use of the violet LED or in association with HP based products. In addition, the self-perception of patients should be taken in account, and it is a poorly explored subject in the literature.
Objective
The objective of this clinical study was to evaluate the effectiveness of a violet LED light (405–410 nm) associated to the dental bleaching treatment with 35% CP gel, on dental color changes, dental sensitivity, and patients' satisfaction.
Materials and Methods
This study was approved by the research ethics committee of School of Dentistry of University of São Paulo (Protocol no. 1.981.756). The experimental design is in accordance to CONSORT
16
and project was registered at
Experimental design
This study was a blind, parallel, and randomized study that included 50 participants (n = 25), selected among the patients of the Special Laboratory of Lasers in Dentistry (LELO-FOUSP). The primary outcome of this study was the tooth color change, evaluated by spectrophotometric (objective) tests. Secondary outcomes were color alteration evaluated by VITA Shade Guide (subjective), dental sensitivity, and patients' satisfaction. The factor under study was the effectiveness of violet LED light (Bright Max Whitening BMW, MMOptics, São Carlos, SP, Brazil). The LED has 1.2 W, produced by four super Violet LEDs light emitters (each of 300 mW) with wavelength 405–410 nm, irradiance 112 mW/cm2, target area 10.7 cm2, and total energy/session 1440 J.
Sample calculation
The primary outcome of this study was the tooth color change. The sample calculation was based on previous studies, reporting that two clinical sessions of in-office dental bleaching reduce ∼7 ± 2 units on VITA Shade Guide. 17,18 To detect the difference of 2 unities between the means of two pairs of groups, the minimum sample size calculated was of 17 participants per study group, with a power of 80% and an alpha of 5%.
Patient selection
A total of 63 patients were interviewed and clinically examined to assess whether they met the inclusion criteria of this study (Fig. 1). Inclusion criteria were as follows: patients age from 20 to 35 years, all the teeth, without restorations or caries on anterior teeth, with canine tooth color A2 (according to VITA classical scale) or darker. Exclusion criteria were as follows: patients presenting teeth discolorations by tetracycline, fluorosis, bruxism, orthodontic treatment with fixed devices, endodontic treatments or with restorations on anterior teeth, smokers or with systematic use of alcohol, historic of self-referenced sensitivity, systematic use of analgesics or anti-inflammatory drugs, periodontal disease, presenting systemic pathologies, and pregnant or at breastfeeding period. Fifty eligible participants (n = 25) were selected among the patients of the Special Laboratory of Lasers in Dentistry (LELO-FOUSP). Written informed consent was obtained from all patients after explanation of the nature and possible risks involved with this study. Participants were randomized using Excel software (Microsoft, Seattle, WA) into the treatment groups (n = 25): G1—in-office bleaching without light and G2—in-office bleaching with violet LED light (405–410 nm), both performed with 35% CP.
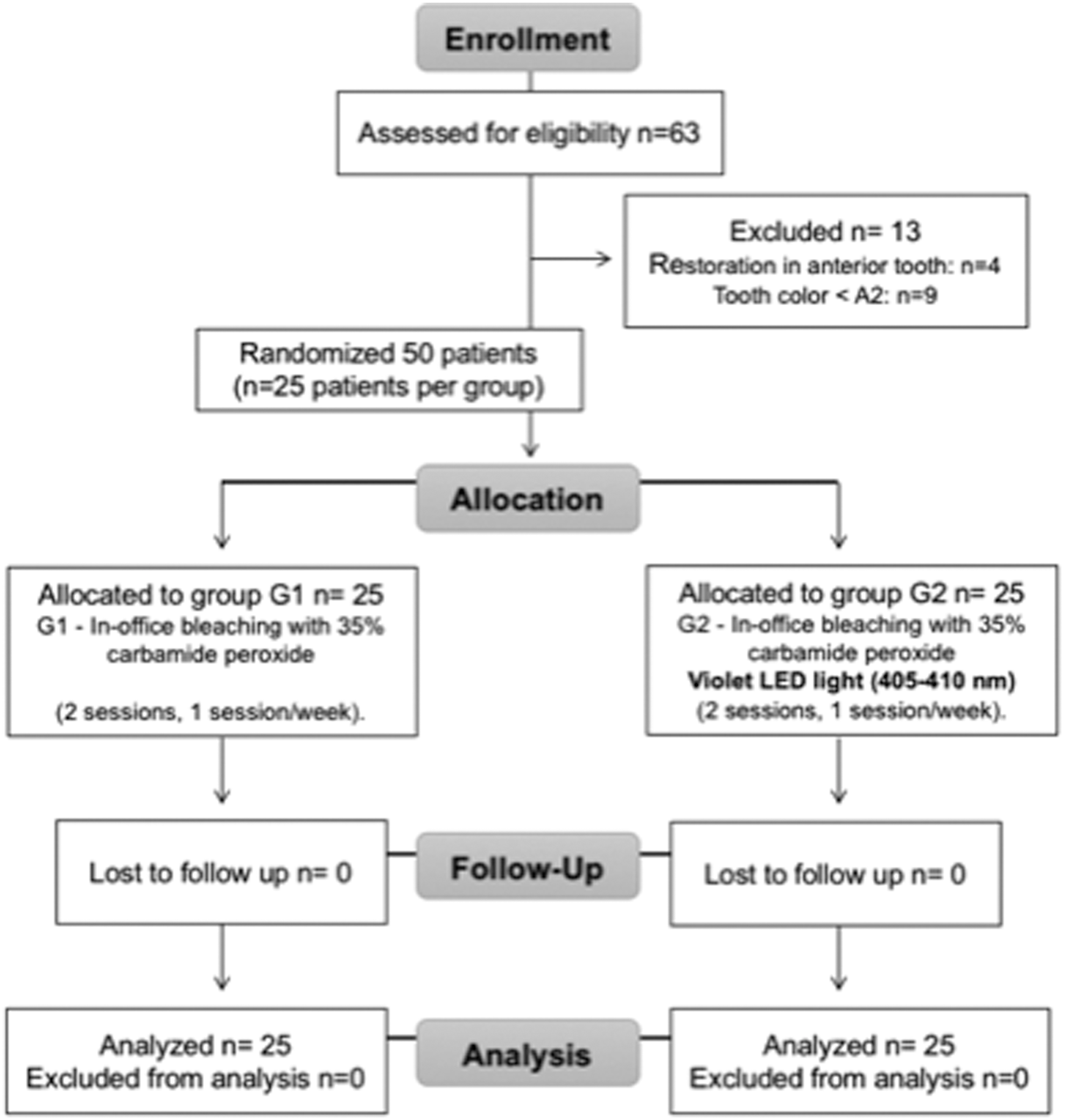
Flow chart.
Seven days before dental bleaching (lead-in period), all teeth were cleaned with a rubber cup at low speed using fine pumice powder and water of each patient, and they received a dental hygiene kit to be used during the study (Colgate Twister Fresh® toothbrush, a fluoride dentifrice Colgate Maxima Protecao Anti-Carie® with 1.500 ppm F-, and a dental floss Colgate; Colgate-Palmolive, Osasco, SP, Brazil) and instructions of oral hygiene. Mouthwash with dental or other products was not allowed during the study.
Intervention: in-office dental bleaching
All participants received the dental bleaching intervention with a 35% CP gel with sodium fluoride and potassium nitrate (Formula e Ação, São Paulo, SP, Brazil). After baseline color measurements (D0), participants' eyes were protected with glasses with black lens, and a gingival barrier (TopDam; FGM, Joinville, SC, Brazil) was applied to protect soft tissues. The bleaching gel (35% CP, pH = 4.0; Formula e Ação) was applied on the buccal face of incisors, canines, and premolars. Violet LED light source (405–410 nm) was positioned 8 mm from buccal surface of bleached teeth. In group G1, violet LED light device remained in mode “off” for 30 min, and in Group G2 the light was applied for 60 sec, with a 30-sec interval, repeating this sequence 20 times (total time of bleaching was of 30 min). After 7 days, the participants returned and the same treatment was performed.
Tooth color evaluation
Before beginning the bleaching treatment, the shade of the upper canine and central incisive teeth of all 50 participants was recorded by a trained blind clinician, using the VITA Color Scale (VITA Zahnfabrik, Bad Sackingen, Germany). Teeth color was evaluated by two methods, a subjective method using the VITA Shade Guide arranged by value, and an objective method using a spectrophotometer (VITA Easyshade; Vident, Brea, CA). Baseline data were evaluated immediately before bleaching treatment (D0) and the final evaluation was made 7 days after the second treatment session (D14).
To the subjective evaluation, the trained blind clinician assessed the color shade with the VITA Shade Guide arranged by lightness (value). Shade guide units (SGU) were arranged from B1 (lightest color) to C4 (darkest color), corresponding to a grade of whitening from 1 to 16, in which smaller number means the tooth was lighter comparing with the medium third of buccal surface from upper canine and upper central incisive teeth. 18,19 Further, the clinician proceeded with the objective evaluation with the VITA Easyshade spectrophotometer. A maxillary silicon (high viscous, Variotime; Heraeus Kulzer GmbH, Germany) impression was taken of each subject to construct a positioning jig with a window (4 mm in diameter) on the labial surface of the canine and central incisive teeth to ensure proper positioning of the colorimeter. The tip of spectrophotometer was attached to silicon matrix and each tooth color was assessed. 19,20
Tooth sensitivity evaluation
To evaluate the degree of dental sensitivity reported by participants, the visual analogue scale (VAS) was used. Scale is represented by a horizontal line of 10 cm (100 mm), limited by two expressions in its extremes, with the sayings “no sensitivity” and “maximum sensitivity.” This enabled to establish the sensitivity degree immediately after each bleaching clinical session and 48 h after its conclusion (D0, D2, D7, and D9). Participants were oriented to draw a vertical line on the horizontal line of pain scale, representing their dental sensitivity (spontaneous) at each evaluation time. 18,19,21
Treatment satisfaction evaluation
Seven days after the end of bleaching treatment (D14), the participants received a nine questions questionnaire and self-perception of treatment was compared. 22 The questionnaire was completed under the supervision of an examiner who was available to answer any questions of the participants.
Statistical analyses
Data were compiled per group of treatment, considering average, standard deviation, median, minimum and maximum values for variables with numeric distribution, and number and percentage of patients for categorical variables. Changes in color between D0 and D14 were calculated as the number of SGU that the tooth changed toward the lighter end of the shade guide, using the nonparametric Mann–Whitney test to canine and central incisor teeth, measured using the ranked VITA scale in scores to subjective and objective evaluations. As few participants reported tooth sensitivity, it was considered as a dichotomic variable (absence and presence), using the VAS, where score 0 was classified as absence and scores 1–10 as presence of sensitivity (1–10). Fisher's exact test was used for comparison. Treatment satisfaction was compared using the chi-square test. Statistical significance was considered for values of p < 0.05. Calculations were made using Minitab software, version 16.1.
Results
This study included 50 participants, 25 in each treatment group. Participants' ages ranged between 20 and 39 years, with an average of 27.6 ± 4.7 years). Most participants were women (78%) but no statistical significant on gender distribution was observed between groups (p = 0.73) (Table 1).
Participants' Demographic Data, Distribution of Age and Gender
Max, maximum; Min, minimum; SD, standard deviation.
Regarding tooth color change, statistically significant differences were observed between groups G1 and G2, for central incisors and canines. Group G2 showed higher color change than G1 (p < 0.001) (Tables 2 and 3).
Teeth Color Mean (Standard Deviation), from Subjective Evaluation, and Color Change According to Ranked VITA Shade Guide, and Results from Mann–Whitney Test
Teeth Color Mean (Standard Deviation), from Objective Evaluation, and Color Change According to Ranked VITA Shade Guide, and Results from Mann–Whitney Test
Only 2 (8%) participants, both from the group treated with violet LED device (G2), reported some sensitivity on D7, a score 5 and a score 6 in the VAS. No statistically significant difference between groups (p = 0.490) was found.
In general, patients were satisfied with bleaching treatment, and no side effects such as gingival irritation that could be bleaching related were described. Statistical significant differences were observed on question 2a and 2b, in which participants of group G2 showed a higher level of satisfaction with treatment than participants of group G1 (p < 0.001) (Table 4).
Description of Satisfaction Questionnaire, Statistical Significant Differences Between Groups were Observed on Question 2a and 2b by Chi-Square Test
Discussion
The use of different light sources in association with photosensitive bleaching agents has been widely purposed by many authors to obtain a faster and effective outcome. In this clinical study a violet LED light (405–410 nm) was associated to a low-concentration bleaching agent aiming to improve in-office bleaching outcome, reduce dental sensitivity, and increase patient self-esteem. The 35% CP was selected for in-office bleaching. 5,15 The rate of decomposition and the type of active oxygen formed are dependent on the temperature and concentration of the peroxide, and on the pH, but 35% CP release ∼11.8% of HP and urea that is responsible for pH increase. 2,4
Klaric et al. reported best results using a 38% HP or 30% CP in a single 30-min application associated to a 405 nm violet LED device. The study considered the use of specially made pastilles of hydroxylapatite immersed in green tea for 8 h and randomly divided into four groups, according to the type of light source applied (30 min) bleaching treatment: LED 405 (400 mW/cm2), organic light-emitting diode (OLED) (400–760 nm, 200 mW/cm2), and femtosecond laser (770 nm, 800 mW/cm2), or no light source (control group). Each group was treated with five bleaching gels: 10%, 16%, and 30% CP, and 25% and 38% HP. Changes in tooth color were determined by red–green–blue (RGB) colorimeter and ultraviolet–visible–near-infrared (UV/Vis/NIR) spectroscopy. When the LED 405 was applied, 38% HP demonstrated the higher increase in RGB index values (median of 2008), followed by 30% CP (1900), 25% HP (1758), 16% CP (1033), and 10% CP (760). 15 It seems contradictory because 30% CP releases 11.8% and showed best results compared with 25% HP; however, the presence of urea raises the pH and a large amount of the most reactive free radical perhydroxyl is released and bleaching reaction is more potent. 4 Then, the choice for CP seems to be more rational to avoid side effects such as dental sensitivity, because less concentration of the active bleaching agent is used.
Group G1 showed a mean color reduction of 0.8 units for central incisors and 1.0 unit for canines. Although some authors report higher changes in color, it is important to consider that the bleaching protocol in this study used a low-concentration bleaching agent that was applied for 30 min, in two sessions (7-day interval), consisting of a very light protocol. Reis et al. evaluated two protocols in two bleaching sessions, applying 35% HP for 40 min or 20% HP for 50 min, and observed a change of 8 and 6 SGU, respectively, with statistical difference. 18
In group G2, the use of violet LED light device resulted in statistically significant higher change in tooth color changes than G1; central incisors teeth reduced a mean of 2.8 units and canines a mean of 6.1 units. It was evident that dental bleaching with violet LED light device was more effective. The effectiveness is related to the ability of violet wavelength (405–410 nm) to react with pigmented molecules, followed by a physical reaction of disruption and reduction of low-molecular-weight pigment molecules. 8,9,12,14 This single ability was demonstrated by Lago et al. 9 in association with a 10% CP bleaching agent.
Effectiveness of different light devices in dental bleaching has extensively been investigated. However, it is not possible to compare these results, because of the lack of equality in irradiation parameters methodology and evaluations. 23 However, it seems that our results are at least in agreement with literature that describes the adjunctive effect of light on improving dental bleaching effectiveness. Kossatz et al. reported statistical significant bleaching using a 35% HP gel in three 2-min applications associating LED/laser device of 4.8 compared with 3.8 units in the group without light application. 17 Kuzekanani and Walsh obtained good results with visible green KTP laser (532 nm) combined with a rhodamine-B photosensitizer 50% HP applied to the teeth and activated four cycles of 30 sec. 24 Vildósola et al. reported different results between objective and subjective shade evaluation methods. 25
Evaluation by shade guide is considered subjective and the spectrophotometer is objective, so disagreements between these methods could be expected. Because of the inherent subjectivity of the shade-guide evaluations, the primary outcome considered for this study was the color change measured by the spectrophotometer. 26 The use of spectrophotometers is considered the most effective method for color assessment and color changes over time because of its higher accuracy compared with visual scales. 25 –27 Slightly numerical differences can be observed comparing the objective and subjective results; nevertheless, the statistical results are in agreement.
By the way, the comparison of the tooth with VITA Shade Guides is the most used clinical method. The value-oriented shade guide gives clinically relevant results, with a perceivable difference in tooth color. However, the selection of the matching shade tab is subjective, not predictably reproducible, and is influenced by such factors as surrounding lighting and eye fatigue. 3,28 The use of a spectrophotometer also has its advantages and drawbacks; it gives more objective results than shade tabs, but it is affected by tooth translucency, tooth contour, tooth texture, difficulties in repeatable tooth repositioning, and need for a flat surface. 28 In addition, it is criticized because small increments of change that could perhaps be measured by instruments would not necessarily indicate a clinically significant result. 29
The VITA Easyshade spectrophotometer works with color space and provides a three-dimensional representation (L*, a* and b*) for the perception of color stimuli and returns the shade to the closest VITA shade tab. The system variables are L*, which is the luminance that represents the difference between light (L* = 100) and dark (L* = 0); a* and b* represents the color values on the red-green axis and blue-yellow axis, respectively. Luo et al. observed good correlation (Spearman) with the subjective and objective data suggesting that the changes in the color parameters and indices obtained from digital imaging were similar to each other compared with clinical scores. 30
A control placebo gel was not included in this study because it is well known that CP bleach teeth significantly more than placebo materials. 29 The patients were aware that bleaching treatment could be associated with violet LED light (405–410 nm), but had no previous bleaching experience or affiliations with violet LED device. No suggestion about side effects also as dental sensitivity was made.
Tooth sensitivity is one of the most common side effects of bleaching treatment, this phenomenon directly depends on the bleaching agent penetration on the pulp, its concentration, and the application time. 21,29 Therefore, tooth sensitivity may also vary with the different factors that affect its passage into the pulp, such as presence of dental cracks, dentin exposure, or pulp chamber dimensions. Thus, pulp sensory nerves can trigger increased response to stimuli, such as cold drinks, until the inflammation subsides. Therefore, high-concentration agents used in in-office procedures usually generate discomfort. Tooth sensitivity normally persists for up to 4 days after conclusion of the bleaching treatment, but longer periods of sensitivity have been reported. 21,29 The VAS data in this study was not able to qualify that the degree of dental sensitivity resulted from the protocol used, because only two participants in group 2 (HP+violet LED) reported dental sensitivity, and can be described with a low incidence of 8%. The low incidence may be explained by the hard exclusion criteria and the option for a low-concentration bleaching agent. Reis et al. reported the incidence of dental sensitivity only in 26.7% of patients submitted for two sessions of in-office dental bleaching with 35% HP for 40 min and 16.7% to the participants treated with 20% HP for 50 min with no statistical differences between them. 18 The use of light in dental bleaching is still a controversy on sensitivity field. Some studies reported higher sensitivity after in-office bleaching in association with light because of heating bleaching agents and accelerate free radical release, using devices like high-power level lasers, in contrast with other studies that use low-level lasers aiming to prevent dental sensitivity. 7,8,17,19,24,28,29
In this context, the use of violet LED has been presented in the clinical scenario as a good alternative to perform dental bleaching. In two sessions of 30 min, the employed protocol resulted in a color change of 2.2 units for central incisors and 5.6 units for canines, and 8% of dental sensitivity. Greater outcomes related to participants' satisfaction were observed in the group in which the violet LED was applied.
A clinically significant bleaching result comes from the clear patient perception of difference in tooth color. 29 In this study, patients of G2 treated in association with 35% CP and violet LED reported to be very satisfied immediately and 14 days after treatment. However, patients in G1 treated only with 35% CP expressed to be partially satisfied because treatment did not achieve the desired bleaching. These differences could be explained because many patients are interested in saving time and obtaining quicker results, which was achieved in the G2 protocol with violet LED. However, 96% of G1 and 100% of G2 patients would bleach teeth again, and the use of this light system associated with a low concentration of the bleaching agent was found to be a good option to fulfill the rising demand for esthetics, promoting efficient tooth bleaching without side effects during and post-treatment. 12 In addition, the G2 protocol could be an alternative for patients with teeth resistant to bleaching and/or with discoloration darker than A2.
Conclusions
Dental bleaching using violet LED light was significantly more efficient than the group without violet LED light.
Patients' satisfaction evaluation regarding bleaching results was significantly higher in the group that used violet LED light.
No significant sensitivity was observed during and in postoperative period.
Footnotes
Author Disclosure Statement
The authors have no competing interests, financial or any personal relationship that may inappropriately affect the integrity of the research reported.
Funding Information
There was no funding provided for this article.