
Abstract
Objective:
The aim of this article was to describe and discuss a clinical case in which the Nd:YAG laser and a desensitizing agent were associated in a protocol for dentin hypersensitivity (DH) in teeth with molar-incisor hypomineralization (MIH).
Background data:
DH is a common condition among the population, being one of the main reasons for patients to seek for a dental treatment. MIH can be considered a condition that induces DH.
Methods:
The patient was referred for evaluation, complaining of hypersensitivity during eating or drinking cold foods. Clinical evaluation revealed the presence of MIH on the first lower molars. Aiming to treat DH, two strategies for dentin desensitization were associated: the use of a high-power laser (Nd:YAG laser, 1.064 nm; Lares Research), with a 300 μm quartz optical fiber, 1 W of power, 100 mJ of energy, 10 Hz of repetition rate, and 85 J/cm2 of energy density, followed by the application of two layers of a desensitizing agent (Gluma Desensitizer).
Results:
DH was evaluated immediately, after 1 week and after 1 month of the treatment. Clinical outcomes were satisfactory, confirming the efficacy and considerable durability of the protocol used for the reduction of DH originated from MIH.
Conclusions:
The association of Nd:YAG laser and a desensitizing agent for controlling DH was effective, showing to be an interesting protocol.
Introduction
Dentin hypersensitivity (DH) is a common condition among the population, being one of the main reasons for the patients to seek for a dental treatment. 1 –4 It is defined as a short, sharp pain from an exposed dentin with dentinal tubules susceptive to external stimuli and that cannot be ascribed to any other form of dental defect or pathology. 2,5,6
According to Brännström et al., dentin exposure with a subsequent opening of dentinal tubules allows the fluid to flow in or out of the tubules, while the incidence of stimuli (thermal, evaporative, tactile, osmotic, or chemical), activating baroreceptors in the pulp, results in the generation of impulses and perception of sensorineural pain. 7
Loss of enamel leading to a coronal or root dentin exposure with opened dentin tubules can be induced by the combination of various factors, such as inappropriate or poor oral hygiene, periodontal therapy, nonbacterial acid exposure, excessive occlusal force, or premature occlusion, and all them are related to DH. 8
Another condition that can induce DH is related with hypomineralization. Molar incisor hypomineralization (MIH) refers to enamel hypomineralization of systemic origin, affecting one to four permanent first molars of the permanent dentition and frequently associated with affected incisors. 9 Teeth with MIH show soft and porous enamel, with high degree of brittleness, and can be more prone to breakdown. Lesions may progress and cause dentin exposure, which can be very sensitive to air flow, and cold and warm and mechanical stimuli. 9,10
The literature shows a considerable prevalence of MIH, in special in Brazilian population, where the highest prevalence percentage was found. The prevalence varies from 3% to 25% in Europe, 11 2.9% to 13.5% in Africa, 12,13 and 2.8% in China. 14 In Brazil, studies have shown a prevalence varying from 2.5% to 40%. 15,16 The etiology of MIH is thought to be multi-factorial and has not been totally defined, possibly due to its complexity, involving exposure to medical and/or environmental conditions during pregnancy or in the first years of life. 17,18 Systemic changes during odontogenesis during the perinatal period or first years of life could result in changes on the dental enamel formation. 19,20 Perinatal complications in the last trimester, low birth weight, lack of oxygen in the birth moment, metabolic disorders of calcium and phosphate, asthma, respiratory tract infections, otitis media, use of antibiotics, high fever history, tonsillectomy, and exposure to environmental pollutants are mentioned as possible etiological factors for this alteration. 19 –22 Therefore, it is extremely important to give attention to the prevention/treatment of MIH-affected teeth, including strategies to treat DH presented in this dental condition.
The use of desensitizer agents to occlude the dentinal tubules—isolating the tubule contents from the oral environment and preventing the flow and movement of the tubular fluid—or the use of chemical agents to desensitize sensory nerves that are able to block the transmission of noxious stimuli of dentinal tubules into the central nervous system can be the strategy to manage DH. 6,23,24
In this context, in-office products can be an effective alternative, since the market offers a wide choice of complex desensitizing agents, with immediate and long-term effects when compared with at-home products. However, the frequency of application is low and may present certainly longevity, requiring more frequent visits to the dentist. 23,25
One potential method for the treatment of DH, suggested since 1985, is the use of photobiomodulation therapy with low-power lasers and/or high-power lasers. 26,27 The literature reports that the laser with the best in vitro and clinical results for the treatment of DH is the high-power laser, more specifically the Nd:YAG laser. 28,29 Its mechanism of action consists of the increase in temperature induced on the dental surface, generating melting and resolidification of the structures, which results in the obliteration and/or reduction of the diameter of the dentinal tubules. It can also reduce DH by leading to the depolarization of the pulp nerve fibers. 30
Some authors have evaluated the effectiveness of Nd:YAG and Er:YAG lasers and concluded that the Nd:YAG laser is superior in relation to patients' pain reduction and also to dentin tubular occlusion. 31,32 Other studies show that the Nd:YAG laser presented immediate and long-term results, without adverse effects in the treatment of DH. 29
Another widely used in-office treatment option is desensitizing agents, as the Gluma Desensitizer. This product has been considered the “gold standard” of the treatments of the office and been used as positive control in some studies, since it presents satisfactory results for the treatment of DH. Among its components are hydroxyethylmethacrylate (HEMA) and 5% glutaraldehyde. Its mechanism of action is based on the coagulation reaction of plasma proteins of the tubular fluid when in contact with glutaraldehyde. This reaction causes precipitations that reduce tubular diameter and are responsible for the polymerization of HEMA, blocking the dentinal tubules. 33 A study in which this desensitizing agent was used revealed almost a complete obliteration of dentinal tubules and significant reduction in pain levels after application, for both air and probe stimulation. 29
Considering the decrease in dentin permeability caused by the desensitizing agent Gluma desensitizer and the action of the Nd:YAG laser, the association between them may present even more favorable and long-lasting results for the treatment of DH.
In view of the above, the aim of this article was to describe and discuss a clinical case in which the Nd:YAG laser and the Gluma Desensitizer agent were associated on a protocol for DH in teeth with MIH.
Clinical Case
An 8-year-old male patient, accompanied by his parents, attended the Special Laboratory of Lasers in Dentistry (LELO) from the School of Dentistry, University of São Paulo, reporting hypersensitivity in teeth when ingesting cold food and drinks.
Through a complete medical history questionnaire, the parents reported that the patient, when around 2 years of age, presented stomach bacterium infection and was hospitalized for 5 days, with a clinical condition of high fever, diarrhea, dehydration, and weight loss.
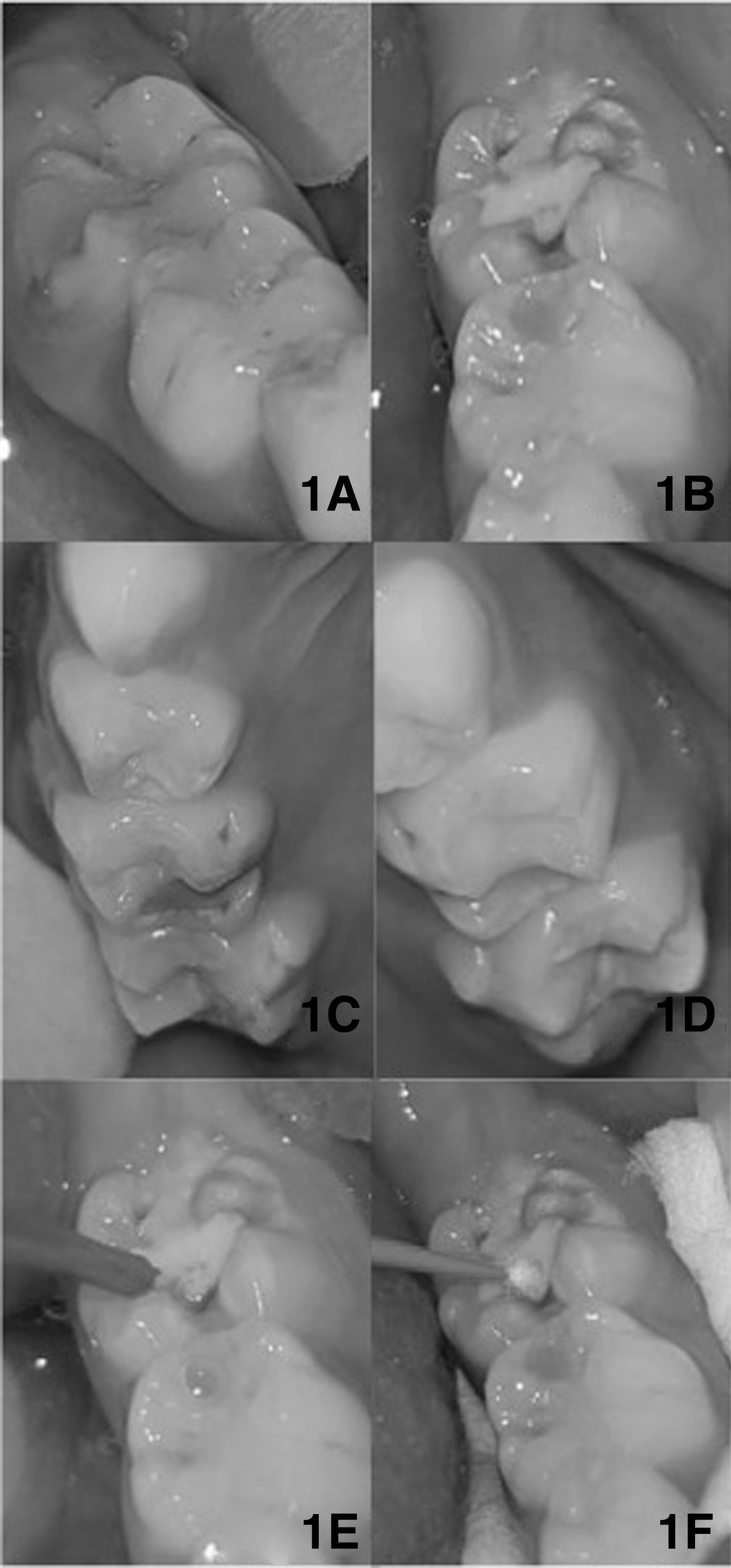
Clinical examination revealed that the inferior first molars presented absence of enamel structure with subsequent brownish spots in some regions of the occlusal surface, possibly characterizing MIH (right inferior molar presented a composite resin restoration at the occlusal-vestibular surfaces and left inferior molar was with partially fractured ionomeric sealant) (Fig. 1A, B). A similar MIH characteristic was observed on superior molars, although not so evident (Fig. 1C, D). As no clinical characteristics of hypomineralization were found on central incisor, the diagnosis of MIH is not definite.
Before any treatment, an approval consent was signed by the child's parents and all possible questions were answered. After initial hypersensitivity test on inferior molars using a gentle air flow from the triple syringe over the surface, the patient reported pain level of 8 on a numerical scale of 0–10 (Visual Analogue Scale). These data represent a high level of DH.
A protocol to treat DH was then performed, associating two techniques/strategies: high-power laser, using the Nd:YAG laser (Power Laser; Lares Research, San Clemente, CA—1.064 nm), followed by the application of a desensitizing agent (Gluma desensitizer). First, four Nd:YAG laser irradiations were performed at the hypomineralized area: two irradiations scanning the surface in the mesiodistal direction and two in the occlusogingival direction, using a 300 μm quartz optical fiber, with 1 W of power, 100 mJ of energy, 10 Hz of repetition rate, and 85 J/cm2 of energy density (Fig. 1E). The detailed description of laser irradiation can be found in Table 1. After irradiating all hypomineralized areas, the air sensitivity test using the triple syringe was performed once again and the patient reported a pain level of 2 on a numerical scale of 0–10.
Parameters of the Nd:YAG Laser Used in the Clinical Case
After laser irradiation, two layers of a desensitizing agent (Gluma Desensitizer; Kulzer GmbH, Hanau, Germany) were applied with the aid of a disposable brush (Microbrush; KG Sorensen, Cotia-SP, Brazil), according to the manufacturer's recommendations (Fig. 1F). Once again, the air sensitivity test using the triple syringe was performed and the patient reported a pain level of 0 on a numerical scale of 0–10.
A follow-up of 1 week and 1 month after treatment conclusion was done and the patient reported a pain level varying between 1 and 3 in 1 week and 2 in 1 month, using a numerical scale of 0–10.
Discussion
The etiology and mechanism of MIH development remain relatively unknown and undefined. It is a fairly new condition, but it is known that MIH occurs more frequently in children with a history of systemic complications in the first years of life, such as respiratory problems, episodes of high fever, and the use of antibiotic medication. 19 –21 The diagnosis of this clinical case was made under clinical examination, assessing the clinical characteristics described in the literature and associating it with the medical history reported by the patient's parents. The period in which the infectious condition occurred, as well as the signs and symptoms (high fever) reported, coincided with the maturation period of the organic matrix of the impacted molars. Management of MIH includes preventive procedures, such as fluoride varnishes (indicated only in cases where there is no structural tooth loss), conservative procedures (infiltrant resin and glass ionomer cements), or invasive restorations, both with removal of the affected area. 34
DH is a common complication in MIH 35 and the initial pain level reported by the patient in this clinical case was considerably high (pain level of 8), making oral hygiene and feeding a difficult task. If not treated, these teeth can create problems for the patient according to Jälevik and Klingberg. Children with MIH, during dental examination, usually open their mouths reluctantly and react intensely to air blowing, making the treatment not easy. Untreated surfaces will result in possible faster progression of tissue loss and consequently more DH. 36
The treatment for DH in teeth with MIH is generally performed as palliative, based on the conventional protocol of topical applications of fluoride or, when considering the existing loss of dental structure caused by MIH, in combination with the crown covering with glass ionomer cements or composite resins. However, there is no established protocol in the literature for the treatment of DH on teeth with MIH. Therefore, this article proposes the association of two techniques, Nd:YAG laser irradiation and a desensitizing agent (Gluma Desensitizer), both already reported on the literature for the treatment of DH in other kind of substrates like erosive and abrasive affected teeth. 29,31,37,38
In this clinical case, immediately after the Nd:YAG laser irradiation, the pain level decreased significantly (pain level reported as 2), but was not completely eliminated. Perhaps this fact can be explained by previous studies that reported a nonhomogeneous melting formed by the Nd:YAG laser irradiation and the possible presence of untreated areas. 39,40 Therefore, limitations exist on the clinical protocol for laser irradiation, not guarantying that all dentinal tubules were occluded. This fact may explain why the patient, even after irradiation with the Nd:YAG laser, still reported pain (pain level 2). However, when applying the Gluma desensitizing agent immediately after laser irradiation, pain was reduced to 0. If tubules were not sealed by means of the resolidification process caused by the Nd:YAG laser, this could be complemented by the desensitizing agent action, reducing the number of open dentin tubules to the maximum extent. Farmakis et al. also showed a combined approach for the treatment of DH with great potential to improve the success. 41 The authors used a bioglass combined with Nd:YAG laser irradiation and suggested this combined treatment as an alternative for DH management in other types of substrate. 41
The pain level obtained immediately after the application of the Gluma desensitizing agent (pain level 0) corroborates with others clinical studies that showed the potential of this product to obliterating dentinal tubules, reducing pain levels immediately after treatment. 29,39 Authors have also reported the maintenance of reduced pain level over the course of time (6- and 18-month post-treatment). 29,39
Some hypothesis can be raised for the increase in pain level during the follow-up period. It can be related to the possible removal of the desensitizer agent due to mechanical impact during feeding and brushing, even the layer formed by laser could be no longer term resistant. However, the interaction of these products with hypomineralized tooth surface and its maintenance over time have not been explored and explained by the literature. For another kind of substrate like erosive and abrasive teeth conditions, the literature shows positive results; for those, some clinical studies using the same desensitizing agent (Gluma Desensitizer) have shown a decrease in DH immediately after its application and also when re-evaluated after some months. 29,39
Until now, the interaction of this product with hypomineralized teeth surface and its maintenance over time have not been clearly explored and explained by the literature. Regarding laser irradiation, it is reported that Nd:YAG laser can have an analgesic effect when compared with the other high-power lasers. This most probably occurs because the irradiation may temporarily alter the final part of the sensory axons and block both the C and αA fibers, thereby decreasing the levels of pain. 42 There are still no reports on how long this effect remains. This clinical case suggests that the effect can be transitory, since there was an increase in pain level during the second and third evaluation periods (1 week and 1 month).
DH on teeth with MIH can be considered a difficult condition to be treated in dentistry, because of the difficulty of measuring pain, choice of material and most suitable technique, and the uncertain prognosis. It is necessary to consider the severity of the DH and the MIH before choosing a treatment, and it is also necessary to use correct and safe protocols. Conservative approach should be used as the first line of option before invasive treatments, such as composite resin restorations or crowns.
Considering the relativity effectiveness and low complexity of the associated technique proposed in this clinical case, the treatment with high-power laser associated with a desensitizing agent can be considered a conservative and appropriate alternative for the treatment of DH on teeth with MIH, provided that the correct protocols, based on scientific evidence, are used. However, we should consider the need of studies evaluating the interaction of the laser with this kind of substrate, reduction of DH, and maintenance of the long-term treatment.
Conclusions
The use of Nd:YAG laser and a desensitizing agent for the treatment of DH originating from MIH demonstrated to be effective in reducing the pain levels immediately and up to 1 month after treatment, without discomfort or adverse reactions for the patient.
Footnotes
Acknowledgments
The authors would like to express their gratitude to the Special Laboratory of Lasers in Dentistry (LELO) from the Department of Restorative Dentistry, School of Dentistry of USP and FAPESP (São Paulo Research Foundation).
Author Disclosure Statement
No competing financial interests exist.