
Abstract
Objective:
Ultrapulse CO2 laser has been used for several decades for removal of xanthelasma lesions. However, most studies to date have focused on Caucasian patients (skin types I-II). We sought to assess the efficacy and complications of CO2 laser therapy for xanthelasma palpebrarum (XP) in Chinese patients (skin types III-IV).
Methods:
Data of 38 patients with xanthelasma who received CO2 laser treatment between December 2013 and January 2016 at our hospital were retrospectively analyzed. Patients were followed up for 9 months.
Results:
Recurrence occurred in 19/38 (50%) patients. Recurrence was significantly more common in patients with multiple lesions (15/24; 62.5%) than in patients with single lesions (4/14; 28.6%). At 3 months after treatment, the complication rate was 63.16%. The complications included hypopigmentation (23/24; 95.8%) and scarring (1/24; 4.2%). In all patients, the hypopigmentation had disappeared by end of the 9-month follow-up.
Conclusions:
Ultrapulse CO2 laser appears to be capable of completely removing XP in patients with medium skin type III-IV. The most common complication is hypopigmentation, but this resolves with time.
Introduction
Xanthelasma palpebrarum (XP) occurs in the periorbital area and is the most common type of xanthoma. Xanthomas result from lipid deposition in the skin, and are considered to be the manifestation of a metabolic disorder. The pathogenesis may be associated with genetic and environmental factors. XP typically presents as yellow or orange, plaque-like or flat, soft, semisolid, or calcareous skin lesions with irregular boundaries. 1
The prevalence of XP is 0.3–4% in Western countries, with women and older persons tending to have relatively higher prevalence. 2 There has been much research on the relationship between XP and dyslipidemia, but no consensus has emerged. Elias et al. found isolated hypertriglyceridemia in 10% of XP patients. 3 Zak et al. reported dyslipidemia in up to 50% of their XP patients and advised that XP lesions should never be ignored in clinical practice. 4 In a large sample of 46,531 Chinese (27,658 men and 18,873 women) undergoing physical examination, Wang et al. found the prevalence of XP to be 1.2% (women 1.16% and men 1.22%), and reported that 50% of these individuals also had high blood lipid levels. 5
Histopathologic studies show that the lesions mainly consist of fibrotic foam cells, giant cells, and chronic inflammatory cells. 6 The condition is benign, but the lesions are permanent and progressive, and can cause serious cosmetic problems if not completely removed. Early removal is desirable because large lesions are disfiguring and more difficult to remove.
Several treatments are available for removal of XP lesions, including surgical excision, various forms of laser ablation, and chemical peeling. 7 Each method has its advantages. Recurrence of lesions at the primary site or at new sites is a common problem. Recurrence at the primary site is often due to incomplete removal. This typically occurs because of intraoperative bleeding obstructing the view of the surgeon during surgical excision. Laser ablation avoids this problem by achieving superior hemostasis. 8
Various types of lasers (argon, erbium:yttrium-argon-garnet, pulsed dye, and CO2 lasers) have been used for ablation of XP. Among these, the ultrapulse CO2 laser is regarded as the gold standard. It has demonstrated excellent results in Caucasian skin types, but there are limited data on its efficacy in Asians. In this retrospective study, we aimed to determine the efficacy of ultrapulse CO2 laser treatment of XP in Chinese patients (Fitzpatrick skin types III-IV) 9 treated during the past 2 years at our hospital, and to study the recurrence rate and complications following treatment.
Methods
This retrospective study was performed in conformance with the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Joint Shantou International Eye Center (JSIEC) of Shantou University and Chinese University of Hong Kong. The need for informed consent was waived in view of the retrospective nature of the study.
Patients
A total of 38 patients (36 females and 2 males) with a total of 73 XPs (size: 0.02–3.15 cm 2 ), who underwent CO2 laser therapy in our hospital between December 2013 and January 2016, were included in this retrospective study. All patients had skin types III–IV. The mean age of the patients was 43.16 ± 9.48 years (range, 24–66 years). At presentation, 14/38 (36.84%) patients had single lesions and 24/38 (63.16%) had multiple lesions. Among the 38 patients, 3 presented with recurrence after a prior treatment (1 after surgical excision and 2 after chemical peeling). Treatment was with the UltraPulse Encore CO2 surgical laser system (Lumenis, Inc., San Jose, CA). The settings were as follows: light source; CO2 gas; wavelength, 10,600 nm; and one session using the super pulse (SP) mode (Table 1). While 37 patients received a single session of treatment, 1 patient with multiple large lesions received two sessions of laser therapy.
Parameter Settings of Treatment by Ultrapulse CO2 Laser
Therapeutic procedure and assessment
Patients were warned to keep their eyes closed and remain still during the entire treatment.
Surface anesthesia was achieved with a lidocaine cream compound (25 mg of prilocaine +25 mg of lidocaine per gram) applied around the XP lesions. After 20–60 min (per the patient's decision), the cream was wiped off and 2% lidocaine was infiltrated around the lesion. For larger lesions, to prevent bleeding, 2% lidocaine with adrenaline (1:10,000) was used.
Parameter settings were as follows: delivery system (1.0-mm focused incisional handpiece); spot diameter, 1 mm; SP mode; energy, 150 mJ; power, 2.0 W; rate, 13.3 Hz; fluence, 19.1 J/cm 2 ; timed exposure, 10 ms/pulse; and repeat delay, 0.3 and 0.1 sec. Typically, the boundaries were cut first, using a 0.3-sec delay, to completely expose the lesion. Then, the tissue was vaporized layer by layer, using a 0.1-sec delay. The charred tissue was gently removed with a saline-soaked cotton ball, which also served to keep the lower layer hydrated. The treatment ended when the yellowish fatty tissues had been completely removed, and the normal pink tissues underneath were exposed. The repeat delay of the pulse was increased when the therapy reached the bottom of the lesion to help reduce the risk of bleeding.
Immediately after treatment, 0.5% chlortetracycline hydrochloride eye ointment was applied at the treated site. The patient was advised to keep the wound dry and clean and to continue application of ointment until scabbing occurred, which typically took about 1 week.
Patients were reviewed at 1 week and 3, 6, and 9 months after treatment. At each visit, recurrence, complications, and patient satisfaction were recorded. Patient satisfaction was assessed with a visual analog scale.
Statistical analysis
We separated the patients into a large-lesion group and a small-lesion group using the median XP size as the cutoff. The chi-square test was used to compare recurrence rates between the single-lesion group and the multiple-lesion group and the hypopigmentation rate between the larger and smaller size groups. All tests were two tailed; statistical significance was at p ≤ 0.05. SPSS 19.0 (IBM Corp., Armonk, NY) was used for statistical analysis.
Results
Distribution of XP lesions
The commonest sites of XP lesions were the inner canthus (66/73; 90.4%) and the upper eyelid (54/73; 74.0%). Lesion location did not vary significantly between the single-lesion group and the multiple-lesion group.
Recurrence and complications
Recurrence occurred in 19/38 (50%) patients. Recurrence was at the original site in 11/19 (57.9%) patients and at other periorbital sites in 8/19 (42.1%) patients. The recurrence rate was significantly higher in the multiple-lesion group (15/24; 62.5%) than in the single-lesion group (4/14; 28.6%) (p < 0.04; Table 2).
Recurrence of Xanthelasma and Incidence of Hypopigmentation in the Single-Lesion and Multiple-Lesion Groups
At 3 months after treatment, 24/38 (63.2%) patients had complications: hypopigmentation in 23/24 (95.8%) patients and scarring in 1/24 (4.2%) patients. No other complication was observed. We separated the patients into a large-lesion group and a small-lesion group, using the median XP size (0.10 cm 2 ; interquartile range, 0.19 cm 2 ) as the cutoff, and compared the difference in the occurrence of hypopigmentation between the groups. Hypopigmentation was significantly more common in the large-lesion group than in the small-lesion group (79% [30/38] vs. 40% [14/35]; χ2 = 11.54; p = 0.001).
The complication rate was lower at 6 and 9 months after treatment: obvious hypopigmentation was present in 11/38 (29.0%) patients at 6 months and in 7/38 (18.4%) patients at 9 months. A corresponding increase in the proportion of patients expressing satisfaction was noted: 50% at 3 months, 68% at 6 months, and 77% at 9 months.
Discussion
This study aimed to assess the efficacy of ultrapulse CO2 laser ablation for treatment of XP in Chinese patients and the complications following treatment. We found the modality to be capable of removing XP lesions in the short term. However, recurrence occurred in 50% of patients. Slowly resolving hypopigmentation at the treated site appears to be common in skin types III-IV.
With a wavelength of 10,600 nm in the mid-infrared region, CO2 laser energy is well absorbed by water. The high water content of the skin makes CO2 laser ideal for precise and safe ablation of skin lesions. CO2 laser can seal off blood vessels with diameter <0.5 mm through a thermal coagulation effect, 10 and therefore, bleeding rarely occurs during ablation of XP lesions, which have small and few blood vessels. In this study, bleeding was noted during clearing of the basal layers of the XP lesions. This is to be expected because dermal tissue, which is rich in blood vessels of different diameters, is exposed as the basal layers are cleared. The number and size of the exposed blood vessels tend to be more in larger lesions. Bleeding can interfere with visualization of the operative field and lead to incomplete removal of the lesion and delayed healing.
In our hospital, to prevent intraoperative bleeding, 2% lidocaine with adrenaline (1:10,000) is used for local anesthesia during ablation of large lesions. The boundaries of the lesions are first cut using a 0.3-sec repeat delay pulse to expose the lesion by removing the epidermis. Then, the tissue is rapidly vaporized layer by layer, using a 0.1-sec delay pulse. The repeat delay time is reset to 0.3 sec when treating the lowest layers of the lesions; this slows the therapy and helps prevent bleeding. If bleeding does occur, the blood vessels adjacent to the hemorrhagic spot are sealed first using the CO2 laser, and the bleeding is gradually controlled. Attempting to control the bleeding more rapidly by direct application of the laser at the hemorrhagic spot would be at the risk of enlarging the damaged area and aggravating bleeding. Prolonging therapy time helps control bleeding, and does not seem to be associated with any adverse effect or increase in patient anxiety.
In this study, the complication rate was 63.2% at the end of 3 months, with hypopigmentation being the most common complication. Hypopigmentation was significantly more common in patients with larger lesions than in patients with smaller lesions (79% vs. 40%). However, it should be noted that hypopigmentation was seen in almost half of the patients with small lesions, indicating that not just lesion size but also the depth of treatment may influence the development of hypopigmentation. Skin coloration is largely determined by melanin production by melanocytes. 9 Melanocytes in the basal layer of the epidermis can be destroyed by laser treatment, 11 and hypopigmentation will occur when the treatment depth reaches the dermal layer, regardless of the size of the XP lesions.
Hypopigmentation following CO2 laser therapy can occur in all skin types, but the incidence is low in patients with skin types I-II. 12 The high incidence of hypopigmentation in our sample may be because the skin types of our patients were darker, resulting in a higher contrast with the hypopigmented area. However, it must be mentioned that studies on the darkest patients (skin types V-VI) have also reported low incidence of hypopigmentation. 13 Darker skin types have more active melanophores or chromatogenesis cells than lighter skin types, 9 and recovery may occur rapidly due to the strong production of melanin by melanocytes in the adjacent areas.
Thus, two factors may contribute to the relatively high incidence of hypopigmentation in patients with medium skin types (III-IV): (1) the high contrast with surrounding normal skin and (2) the limited compensatory ability of the melanocytes in the adjacent areas, leading to a longer recovery time. In this study, the hypopigmentation took 6–9 months to resolve completely. This type of dynamic change was also clearly observed in one patient in the single-lesion group, who experienced recurrence in another periorbital area (Fig. 1). Patient satisfaction with the treatment reflected the gradual improvement in hypopigmentation: 50% at 3 months after treatment, 68% at 6 months, and 77% at 9 months.
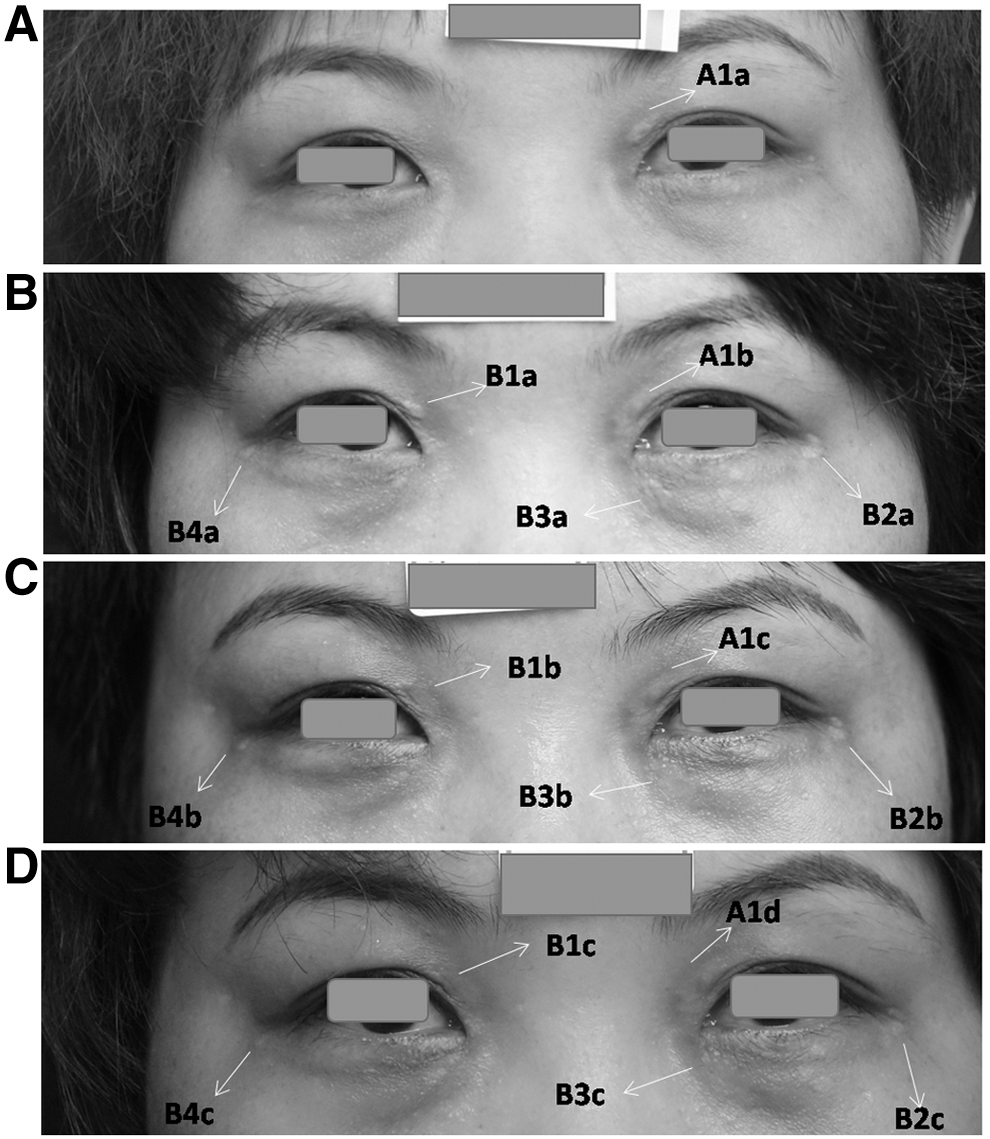
Photographs showing the changes over time in one patient who suffered recurrence. A patient in the single-lesion group suffered recurrence at both the original location and another periorbital area. Hypopigmentation was seen at all treated sites, but resolved slowly over time.
Recurrence of XP has been reported to be related to factors such as blood lipid level and the type of therapy. However, some studies have also shown that only a small proportion of XP patients have abnormal blood lipid levels, and that reduction of cholesterol levels does not always prevent recurrence. 14 Using the same CO2 laser therapy for XP, Esmat et al. compared the SP mode (single session) with the fractional mode (3–5 sessions at monthly intervals) and found that the SP mode is more effective for removal of lesions, but increases the possibility of scarring and recurrence. The authors offered the explanation that the SP mode removed both the deposited lipids and the underlying dermal component that is susceptible to lipid deposition. The recurrence rate was still increased compared to that in the fractional mode, which cleared the dermal component slowly over several months. 15
Goel et al. compared ultrapulse CO2 laser with trichloroacetic acid peeling for the treatment of XP and reported no difference between the two in efficacy or recurrence rate. 16 Thus, it appears that blood lipid levels and mode of therapy have only a weak relationship with recurrence of XP. In our study, CO2 laser was used mainly in the SP mode in a single treatment session, and complete removal was achieved in all patients. However, the overall recurrence rate was 50%, with the rate being higher in those with multiple lesions than in those with single lesions (62.5% vs. 28.6%). The recurrence rate at the original lesion location (57.8%) was not significantly lower than the rate at other locations (42.1%), suggesting that complete clearance does not necessarily reduce recurrence. However, this hypothesis requires assessment in controlled studies.
Thus, we believe that recurrence is more closely related to patient characteristics than to the type of therapy. Wang et al. demonstrated that intralesional injection of XP with the antitumor antibiotic pingyangmycin effectively reduced the lesion size in Chinese patients. 16 We suggest that combination therapy should be assessed, such as the use of an initial injection followed by a suitable laser ablation or other therapies, thus individualizing the therapy for better results.
The limited follow-up in this study did not allow us to assess long-term complications. Other limitations include the limited sample size and the retrospective single-institution nature of the study.
Conclusions
Ultrapulse CO2 laser can effectively remove XP lesions. However, given the long period of hypopigmentation at the treated site, CO2 laser may not be the best choice for Chinese patients with skin types III-IV. Other methods can be used to clear XP lesions, but none of these methods is more effective. Combination treatments need to be explored further.
Footnotes
Acknowledgments
I would like to express my gratitude to all those who helped me during the writing of this article. I am deeply indebted to my colleague Yu-Zhou Gu who offered valuable suggestions on the statistical work.
Author Disclosure Statement
No external funding was received for this study. No competing financial interests exist.