
Abstract
Objective:
A review of photobiomodulation (PBM) in Alzheimer's dementia is submitted. The addition of PBM in neurodegenerative diseases is a dual modality that is at present gaining traction as it is safe, antiviral, and anti-inflammatory for treating neurodegeneration with photons that stimulate mitochondria increasing adenosine triphosphate and proteasomes increasing misfolded protein removal. Neurofeedback provides neural plasticity with an increase in brain-derived nerve factor mRNA and an increase in dendrite production and density in the hippocampus coupled with overall growth in dendrites, density, and neuronal survival.
Background:
Alzheimer's disease pathophysiology is the accumulation of hyperphosphorylated tau protein neurofibrillary tangles and subsequently amyloid-beta (Aβ) plaques. PBM and neurobiofeedback (NBF)address the multiple gene expression and upregulation of multiple pathogenic pathway inflammation, reactive oxidative stress, mitochondrial disorders, insulin resistance, methylation defects, regulation of neuroprotective factors, and regional hypoperfusion of the brain. There is no human evidence to suggest a clinical therapeutic benefit from using consistent light sources while significantly increasing safety concerns.
Methods:
A PBM test with early- to mid-Alzheimer's was reported in 2017, consisting of a double-blind, placebo-controlled trial in a small pilot group of early- to mid-dementia subjects under Institutional Review Board (IRB)-approved Food and Drug Administration (FDA) Clinical Trial.
Results:
PBM-treated subjects showed that active treatment subjects tended to show greater improvement in the functioning of the executive: clock drawing, immediate recall, practical memory, and visual attention and task switching (Trails A&B). A larger study using the CerebroLite helmet in Temple Texas again of subjects in a double-blind, placebo-controlled IRB-approved FDA Clinical Trial demonstrated gain in memory and cognition by increased clock drawing.
Conclusions:
Next-generation trials with the Cognitolite for Parkinson's disease subjects will incorporate the insights regarding significant bilateral occipital hypocoherence deficits gained from the quantitative EEG analyses. Future applications will integrate noninvasive stimulation delivery, including full-body and transcranial and infrared light with pulsed electromagnetic frequencies.
Introduction
Photobiomodulation (PBM) in neurodisorders and especially Alzheimer's disease (AD) has had a number of publications recently. This article reviews our publications in this field and those of other investigators. The addition of PBM and neurofeedback in neurodegenerative diseases is a dual modality that is at present gaining traction. PBM is a safe and potent antiviral to herpes labialis with U.S. Patent 5500009A in 1996, and an antibacterial, anti-inflammatory agent for treating functional neurodegenerative, inflammatory, and infection-based conditions
1
–3
PBM therapy in Alzheimer's dementia has reached over 10 citations in
Quantitative electroencephalograph-based biofeedback training, also called neurofeedback, supports neural connectivity renormalization. The combination of the two approaches shows promise as a method to safely and effectively stop disease progression, preventing further neuronal damage and facilitating removal of neurofibrillary plaques and tangles while training renormalization of intra- and interhemispheric communication.
Berman et al. previously described the historical background and action mechanisms underlying the effects of PBM and EEG biofeedback (neurofeedback) training. 4 Near-infrared (NIR) light has been shown to support healing and improved motor, cognitive, behavioral, and metabolic functioning. 5 Combining the two approaches with functional and integrative biomedical treatments, for example, stem cell therapy, gene therapy, and optogenetically delivered chemotherapy (localized optical modulation of selected genes via photo-excitable ion channels), constitutes a systemic intervention strategy that can further enhance the effective delivery of precision medicine. See Fig. 1 below for images of brain treated by PBM and quantitative EEG (QEEG) neurofeedback.
Dr. Marvin Berman with QEEG Cap. Images of brain PBM and QEEG neurofeedback. PBM, photobiomodoulation; QEEG, quantitative EEG. (Images: Open Image QEEG Shutterstock, Internet).
Bredesen has addressed the present functional medical approach for evaluating and treating dementia, and the focus is on current measurement techniques such as QEEG and NIR spectroscopy. 6 There is a growing trend toward neurophysiological integration with noninvasive neurotherapeutic methods to influence healthy functioning positively. Neurodegenerative disorders are good candidates for such strategies of intervention. Research was conducted on the multi-determined causes of functional, neurocognitive, and behavioral challenges by Bredesen. 6 The following list represents Bredesen's main diagnostic components for assessing and treating dementia patients. Biomarkers with an X also respond to transcranial PBM positively (Table 1).
Diagnostic Components of Bredesen Assessing and Treating Dementia Patients
Functional and inflammatory biomarkers associated with neurodegenerative disorders with indicators that respond positively to transcranial near-infrared PBM.
Aβ, amyloid-beta; ADNP, activity dependent neuroprotective protein; A/G, albumin/globulin; APP, amyloid precursor protein; BDNF, brain-derived nerve factor; CBF, cerebral blood flow; GABA, gamma aminobutyric acid; G-CSF, granulocyte colony-stimulating factor; GSH, glutathione; NGF, nerve growth factor; NMDA, N-methyl-d-aspartic acid; PBM, photobiomodulation.
Bradford et al. 2019. 2
Neurodegeneration Pathophysiology
AD etiology and pathogenesis are complex, with many risk factors for viruses, genes, and the environment, including stress and insulin resistance. Multiple gene expressions and upregulation of multiple pathogenic pathways result in deposition of amyloid-beta (Aβ) peptide, tau hyperphosphorylation, inflammation, reactive oxygen species (ROS), mitochondrial disorders, insulin resistance, methylation defects, and regulation of neuroprotective factors and regional hypoperfusion of the brain. Tau and Aβ antibody therapy, vaccines, and other methods for tau and/or amyloid reduction were unsuccessful after extensive pharmaceutical and biotic treatment. 7
The present AD pathophysiology is the accumulation of hyperphosphorylated tau protein neurofibrillary tangles (NFTs) and subsequently Aβ plaques. A common feature of many neurodegenerative diseases, including Alzheimer's, is this accumulation of misfolded protein aggregates. 8 Most protein degradation is caused by the ubiquitin/proteasome pathway. AB accumulation affects the system of ubiquitin and proteasome. 9 Myeku demonstrated that tau-driven 26S proteasome impairment and cognitive dysfunction in a mouse model can be prevented early in disease by activating cAMP-PKA signaling and represent key components that underlie PBM's mechanism of action, resulting in increased mitochondrial adenosine triphosphate (ATP) and proteasomal clearance of tau and Aβ in mouse models regarding developing AD. 10
In Indianapolis, Eli Lilly announced a major change to their closely watched clinical trial for the drug solanezumab for Alzheimer's, which failed to reach statistical significance. 11 “A major challenge of such trials is how to measure the drug's benefits,” says Dennis Selkoe, a neurologist at Brigham and Women's Hospital in Boston, who was not involved in the Lilly trial. “Although people with early Alzheimer's may show mild memory impairment and problems with attention and focus, they can often follow recipes, make a cup of coffee, or drive a car,” says Selkoe. Throughout an 18-month clinical trial, such abilities are unlikely to change much. Animal studies often show improvement in therapy long before there is any benefit to human clinical trials. 12 A recent report on animal models used NIR PBM in the K369I tau transgenic model for the development of NFTs and the amyloid precursor proteins (APPs)/PSEN1dE9 transgenic model (APP/PS1) for the development of amyloid plaques. 13 DNA methyltransferase 3A (DNMT3A) is one of two essential human de novo DNA methyltransferases for cellular development and differentiation of transcription regulation. There is growing evidence that RNA plays a role in directing DNA methylation within mammalian cells to specific genomic locations. Two modes of DNMT3A in vitro RNA regulation have been described here. A single-stranded molecule of RNA that is antisense to the promoter of E-cadherin binds in a structurally dependent manner tightly to the catalytic domain causing a powerful inhibition of DNMT3A activity. Two other RNA molecules that bind specifically in in vitro modulation of RNA DNMT3A activity support in vivo data interacting with DNMT3A for transcription regulation. 14 This mechanism can be used to observe that NIR light regulates transcription of DNMT3A outside the catalytic domain at an allosteric site, causing no catalytic change. Although in vitro modulation of DNMT3A is considered by some to be controversial, Alzforum, on October 23, 2018, devoted a full discussion “Islands of Mutated Neurons Dot the Brain in Alzheimer's. Are they Bad for Us?” This was supported by five references and methylation on the topic of a previous publication of one of the authors (T.W. Nichols) on defects in “Hyperphosphorylation of Tau Protein in Down's Dementia and Alzheimer's Disease; Methylation and Implications in Prevention and Therapy in Alzheimer's Disease and Parkinson's,” published in 2012. See Fig. 2 below for transcription factors involved in low-level light therapy (LLLT).
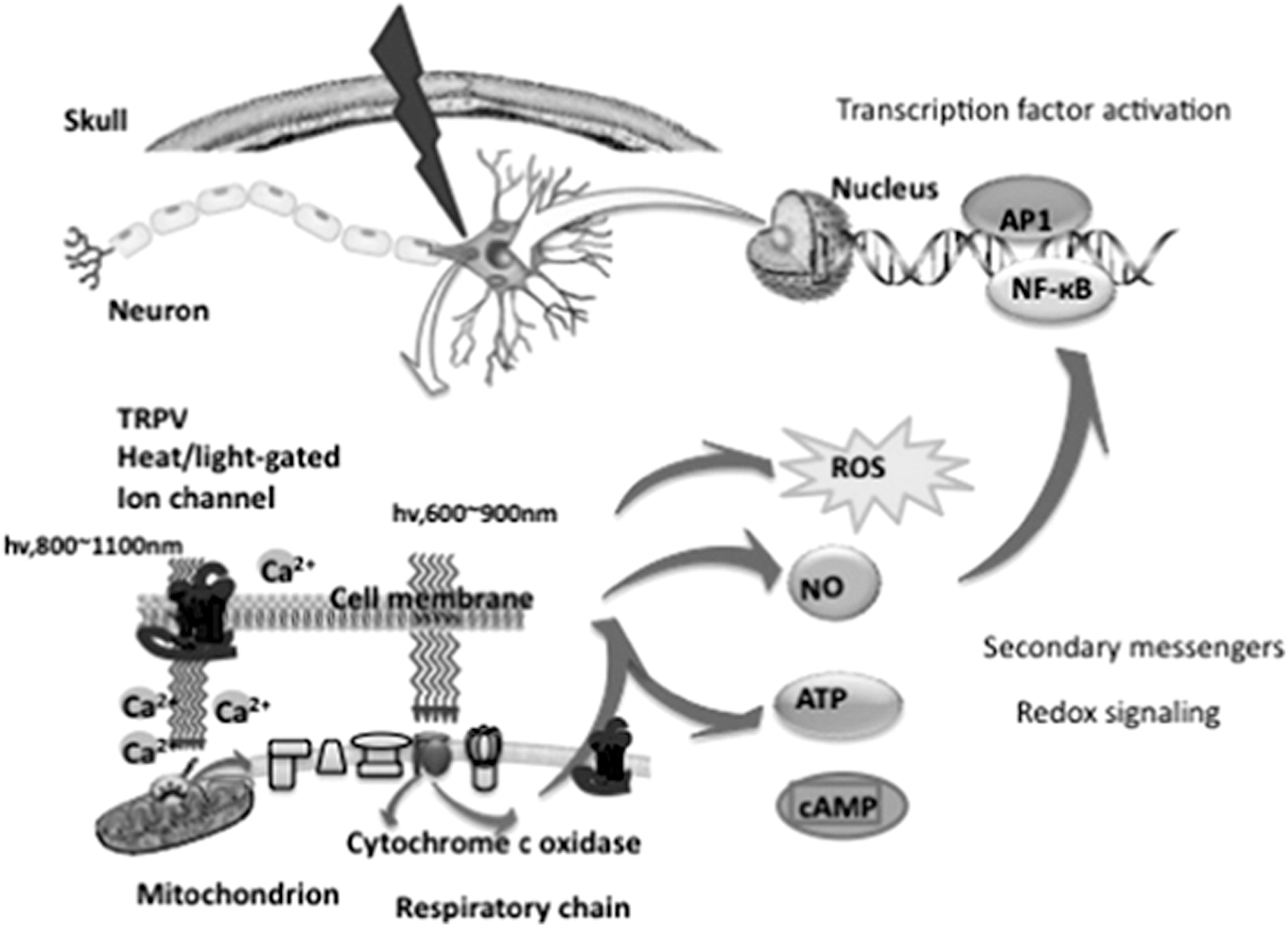
Transcription factor activation molecular and intracellular mechanisms of transcranial low-level laser (light) or PBM. Ca2+, calcium ions; cAMP, cyclic adenosine monophosphate; NF-kB, nuclear factor kappa B; NO, nitric oxide; PBM, photobiomodulation; ROS, reactive oxygen species; TRPV, transient vanilloid potential receptor. 5
Although there is at present no evidence that NIR light regulation of site-specific subtelomeric DNA methylation may affect DNA methylation, blue light optokinetically has been shown to selectively increase methylation at subtelomeric CpG sites at the six chromosome ends examined by Choudhury et al. This blue-light activation resulted in a progressive increase in the length of telomeres over three generations of replications of HeLa cells. They concluded that targeting DNMT3A at subtelometric DNA sites increases methylation in a HeLa cell model at specific genomic sites. 15
PBM therapy
Initially, low-level laser therapy was the term used to describe the therapeutic use of intensive monochromatic light energy with PBM becoming the more comprehensive laser and light emitting diode (LED) light energy terminology. There is no human evidence to suggest a clinical therapeutic benefit from using consistent light source (LEDs or LLLT) low-level laser therapy, while significantly increasing safety concerns, for example, tissue heating related damage is increasing (Table 2).
Wavelength and Pathological Effect of Low-Level Light
In particular, in the marketing of PBM applications and devices, there are numerous instances of laser- and LED-based treatment conflating. Therefore, we advocate exclusively the development of LED-based technology for transcranial and intraocular self-administered applications. Our advocacy is also in response to the growing recognition that a significant proportion of modern health care assessment and intervention service delivery is shifting from face-to-face office-based structure to telemedicine- and cloud-based applications. 16
A search for the world's medical literature (250 + trials) of pharmacotherapeutic agents for Alzheimer's treatment does not provide any long-term improvements published. 17 Naeser and Hamblin previously published PBM studies using low-level NIR stimulation in the treatment of traumatic brain injury (TBI) in 2015. NIR light passes readily through the scalp and skull and arrives at the upper 1–5 cm of the brain. The primary photoreceptors for (600–950 nm) red and NIR light are in the terminal link of the mitochondrial respiratory chain. 18
Rich in mitochondria, cortical neurons have increased biochemical pathways such as increased ATP and ROS-activated signaling pathways. PBM is based on light's ability to alter cell metabolism as it is absorbed in particular by general hemoproteins and cytochrome c oxidase (COX). 19 The regulation of gene expression and the behavior of neurotransmitters in the hippocampus and other brain regions, typically associated with memory disorders, shows to be effective PBM targets. Most notable was the increase in brain-derived nerve factor mRNA and the increase in dendrite production and density in the hippocampus coupled with overall growth in dendrites, density, and neuronal survival (Meng 2013), and further supported by Grillo et al., 20 Ojha (2011), and Bradford (2007), and the increasing production of molecular chaperones (Doggett and Chazot, 2013). 7
NIR PBM decreases synaptic vulnerability to Aβ
Comerta and researchers at Galveston University of Texas worked on synaptic dysfunction due to disruption of the binding of Aβ and tau oligomers, one of the earliest impairments in AD. They reported that a group of people called nondemented with Alzheimer's neuropathology (NDAN) who had Aβ oligomer at the synapses, but had cognitive function retention, differentiated from a group of demented AD subjects. They showed that these nondemented individuals displayed similar levels of soluble Aβ oligomers throughout their central nervous system, but their synapses were devoid of Aβ oligomers, suggesting that NDAN subjects are somehow resistant to Aβ oligomers. They investigated NIR light's ability to decrease synaptic susceptibility to Aβ oligomer binding, thus increasing synaptic functioning. They used wild-type (Wt) mice in the hippocampus of PBM-treated mice in the presence and absence of Aβ oligomers to determine the impact of NIR light treatment on the binding of Aβ oligomers to isolated synaptosomes and long-term potentiation. Findings included significantly reduced Aβ1–42 at the synapses of the 6-month-old Tg2576 mice that overexpressed human APP. 21
These changes coincided with post-PBM synaptic mitochondrial longevity and increase in both Wt and Tg2576 and CD-1 mouse models (Michalikova, 2007, Ennaceur, 2006). This study provides additional evidence to support NIR light therapy as a viable treatment for AD (Camerota, 2017) that specific PBM protocols can effectively reduce synaptic vulnerability to damaging Aβ oligomers. These and other findings, particularly work by Chazot and colleagues at Sunderland University and Durham University, helped further clarify the mechanism of action underlying PBM's biochemistry. See Fig. 3 below. 7
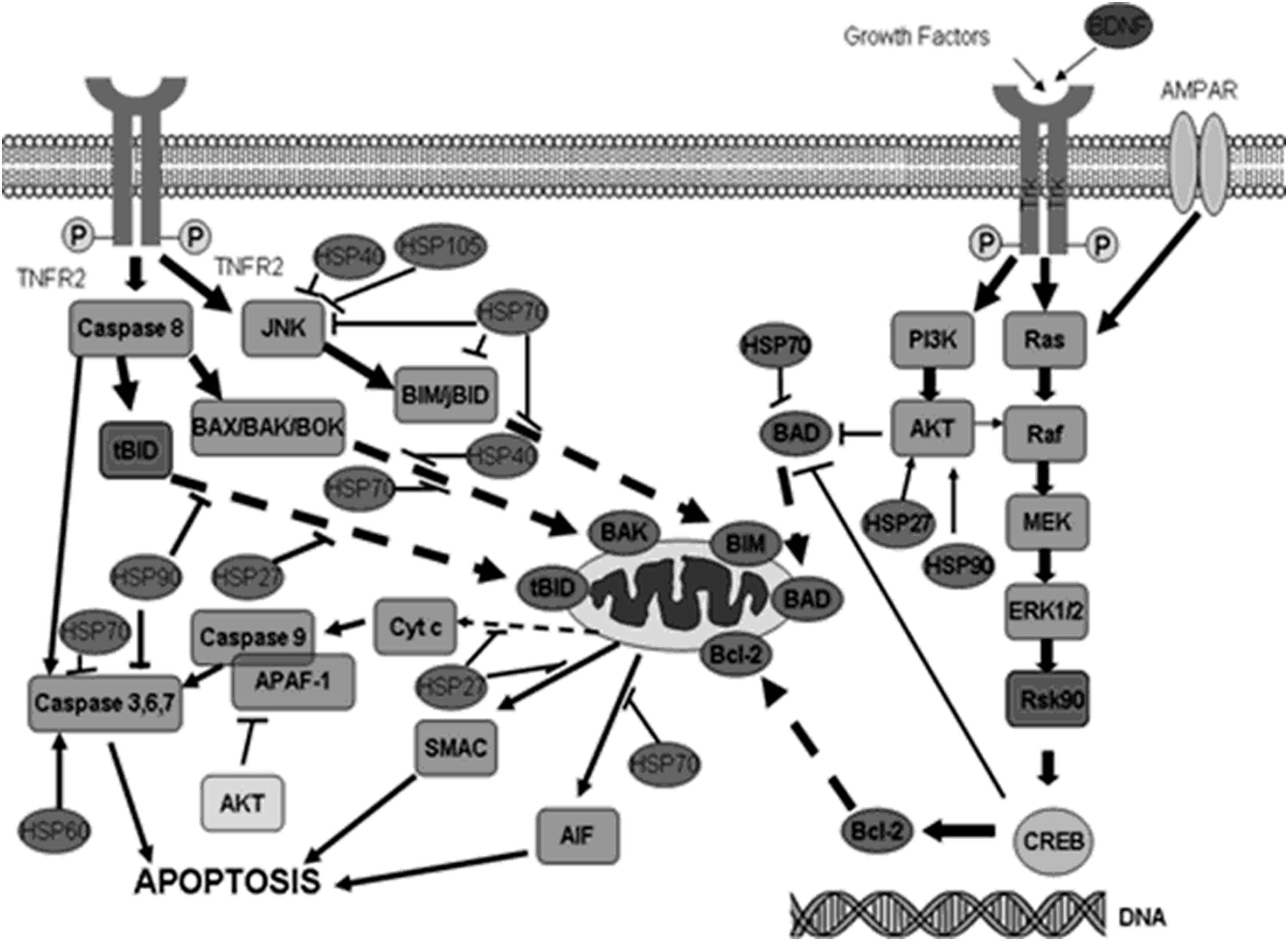
PBM mechanism of action (unpublished and published material from Grillo et al. 20 ). A range of selective HSPs have been shown to be upregulated following in vivo treatment of Alzheimer's mice (HSP27, 60, 70, 90, 105) (Grillo and Chazot; Duggett and Chazot, unpublished; Schirmera, 2016, in press), 20 highlighting the role of these proteins in mitochondrial function, apoptosis, and protein folding mediated by chaperon. HSP, heat shock protein.
Human PBM trials started by Naeser and Hamblin 18 reported 11 chronic TBI patients whose cognition improved after treatment with red and NIR LEDs applied transcranially to the forehead and scalp at 10 min per area and nasally red light at 18 outpatient sessions. Neuropsychological testing for executive function at 1, 2, and after 18 LED treatments showed improvement in the Stroop test.
Researchers at the University of Sunderland 20 reported using noninvasive 1072 nm pulsed (10 Hz) stimulation on an animal model of dementia (TASTPM mice). This was the first peer-reviewed publication that described the use of this higher wavelength as a potential method of treatment. Here we see a decrease in the number of placebo (no light) small plaques versus active 6-min exposures over two consecutive days, twice a week over 5 months. 20
Cell line (lymphocytes exposed to UVA) and pretreated neurons in culture were then exposed to varying concentrations of nitric oxide in the original bench studies. 2 Subsequent media attention (Derbyshire, 2008) caught the attention of Quietmind Foundation researchers who studied the effect of noninvasive brainwave biofeedback training on cognitive and behavioral symptoms in subjects with early- to mid-stage dementia (Berman and Frederick, 2009). In 2011, the present first author and colleagues at the Quietmind Foundation started a collaboration with the inventor of the first PBM helmet (Cognitolite, is a fourth generation), Gordon Dougal, MD, BSEE, a physician and electronic engineer in the United Kingdom who conduct the first PBM treatment for cognitive and behavioral symptoms of dementia in human clinical trials. The transcranial and intraocular Cognitolite PBM system provides ∼600 mw of 1065–1075 nm of 10 Hz pulsed photic stimulation. The present experimental protocol for dementia and Parkinson's called for two, daily, 5-min stimulation sessions at 5–6-h AM/PM intervals. Treatment protocols now use the fifth-generation device design (CerebroLite) helmet at 1068 nm (see Table 3), collaboratively developed with Gordon Dougal, MD, BSEE, at Maculume Ltd. since 2008, and tested by the research group at Quietmind Foundation (QMF) with the goal of integrating neurofeedback training and PBM into a neurotherapeutic application that can simultaneously improve tissue-level pathology and abnormal neural connectivity. 22
PHOTOB 2019 Light Emitting Diode
Pilot Clinical Trials of NIR Helmet in Alzheimer's
A pilot PBM test with early- to mid-Alzheimer's reported in 2017, consisting of a double-blind, placebo-controlled trial of (n = 11) 6 active, 3 controls, and 2 dropouts, evaluated the effect of 28 consecutive, 6-min NIR stimulation transcranial sessions. 22 Several local continuing care communities recruited patients using print and online media. All subjects were independently diagnosed with probable Alzheimer's dementia by a neurologist by means of the criteria of NIA-OA. Testing included Mini-Mental Status Examination (MMSE), QEEG, and Alzheimer's Disease Assessment Scale-Cognitive (ADAS-Cog) on the first day of treatment and within 3 days of completing the 28 consecutive 6-min daily exposure sessions required. Surface cortical perfusion was measured before and after each transcranial and intraocular exposure using NIR spectroscopy (FP1 and FP2) in which a 2-min baseline was recorded using near-surface infrared spectroscopy developed with Biocomp Research Hemoencephalography (Toomim, 2000) and Bioexplorer software (Janow, 2002). After each session, QEEG changes were recorded and described in greater detail elsewhere. 23
The most significant changes in transcortical electrical activity have been the normalization of central alpha (8–12 Hz) amplitudes and delta (0–4 Hz) and theta (4–8 Hz) hypocoherence and phase lag, that is, internodal correlation. 24 Improved delta and theta are associated with improved alertness and attention in the sleep architecture, and reduced alpha may result in reduced anxiety. John Nash, PhD, and Fonseca et al. recently commented that, “Delta waves are wide geographically and raise wide neuronal regions closer to the threshold, with the rapid waves riding on the delta's large ocean swells. This widespread integration of frontal systems is caused by a lack of delta; it also prevents effective sleep start and restoration of sleep.” 24
See Fig. 4 below for image of NIR helmet.
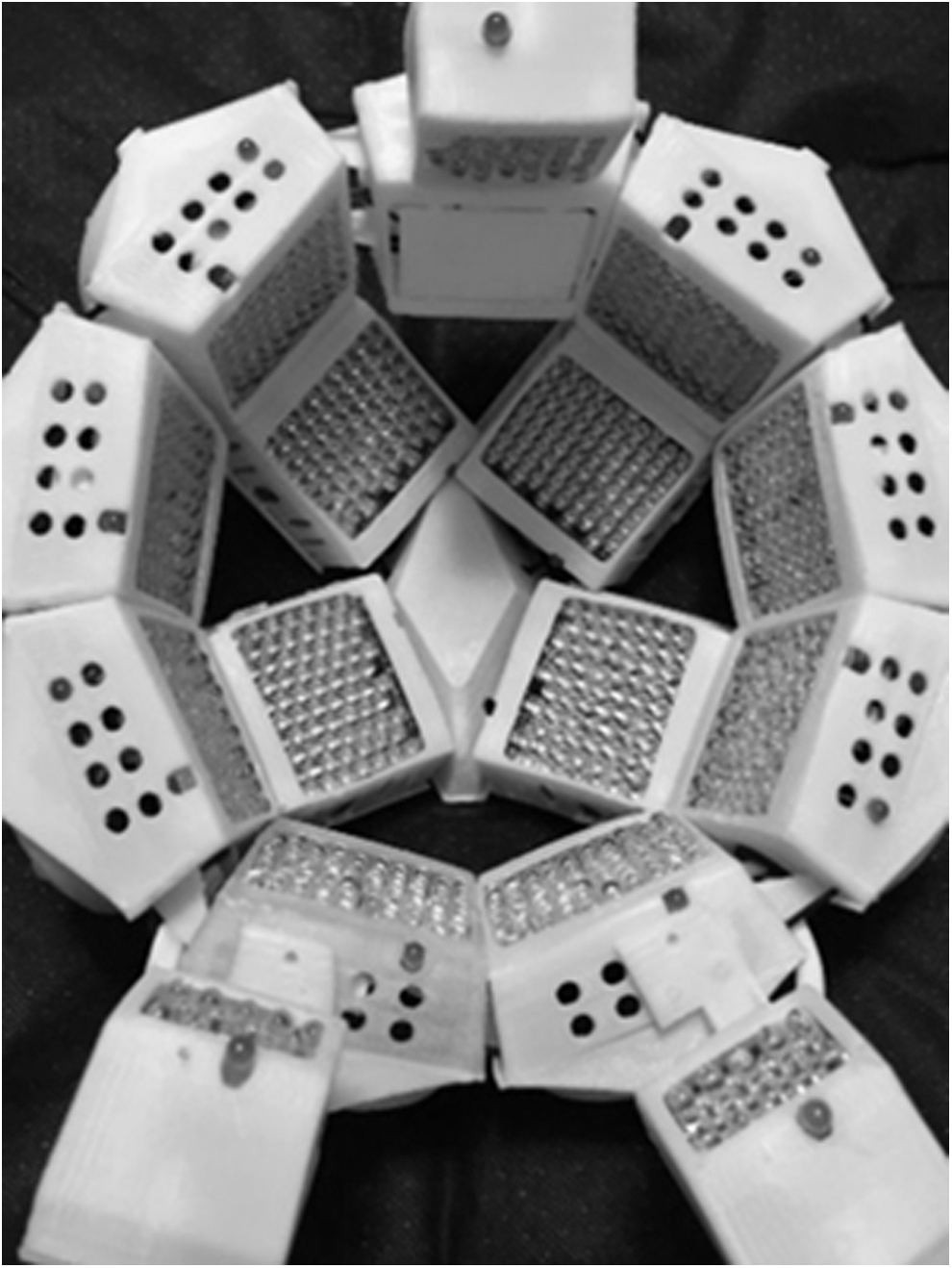
Inside view. Near-infrared LED helmet. CerebroLite transcranial intraocular 1068 nm PBM system. LED, light emitting diode.
PHOTOB parameter table: The irradiance or power density measured in 2.6 mw/cm2. The wavelength of the light is 1068 nm at 32 J/cm2, and duration of each treatment session, preferably measured in seconds, is 5 min, twice daily, for 56 total doses.
The substantial impact that PBM can have on both power and coherence aspects of electrophysiological activity is quite apparent and this can serve as noninvasively determined biomarkers discriminating between various neurodegenerative disorders, including Parkinson's. See Fig. 5 below for QEEG changes before NIR stimulation.

QEEG changes
Clock Draw Pretest and Digit Span Measure
Results showed that active treatment subjects tended to show greater improvement in the functioning of the executive: clock drawing, immediate recall, practical memory, and visual attention and task switching (Trails A&B) (Fig. 6). Because of the sample size, statistical significance could not be achieved. Clock drawing improvements showed moderate sensitivity and specificity to detect executive cognitive dysfunction even with normal MMSE in people (Nichols and Berman, 2017). 4
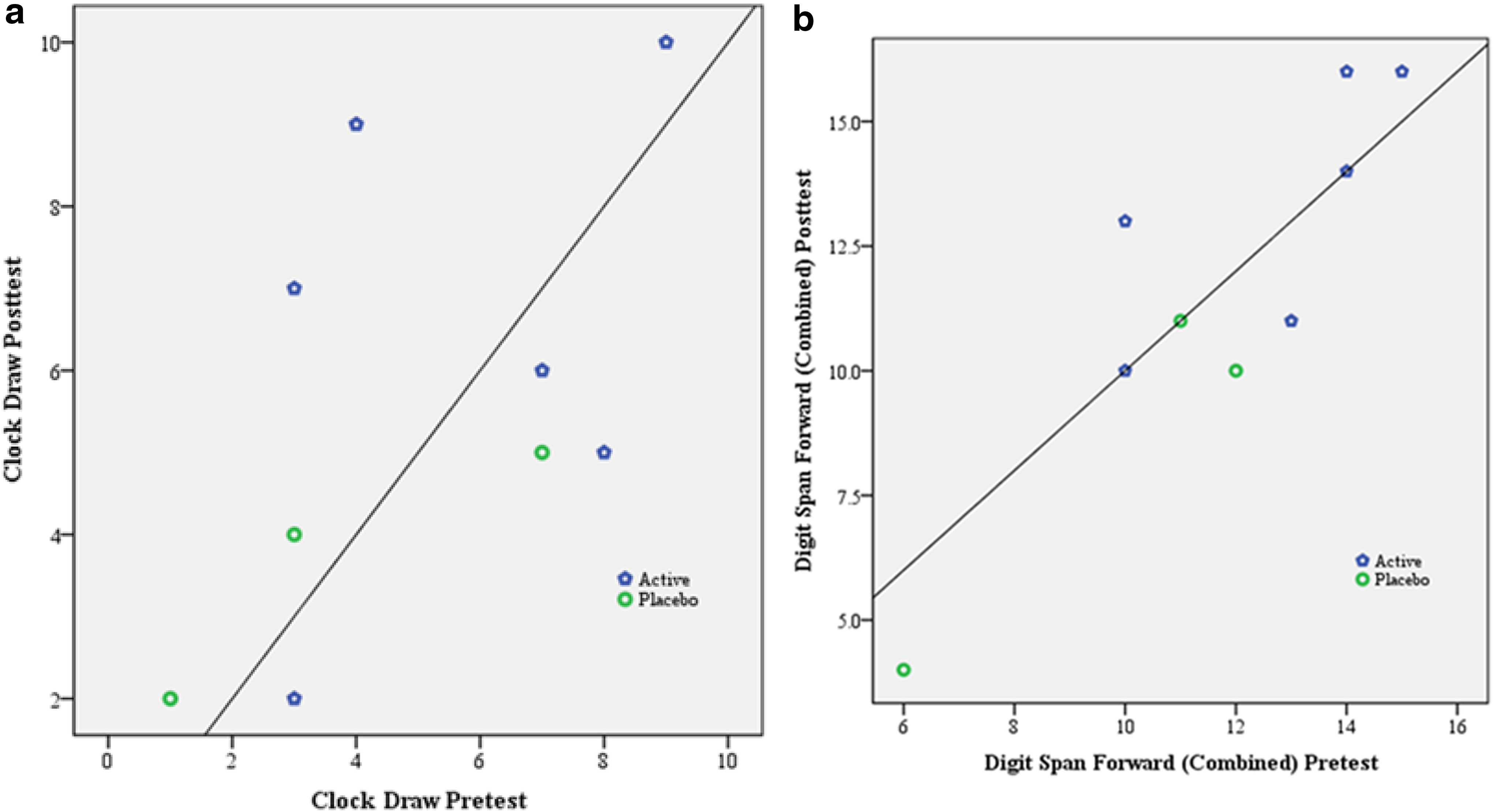
Graphs comparing active and placebo clock drawing and digit span forward scores.
Dr. Jason Huang, Chairman, Department of Neurosurgery, Baylor Scott & White Health (BSWH) Temple, TX, conducted a recently completed replication study. A Texas A&M Health Science Center affiliate and postdoctoral fellow and study coordinator Damir Nizamutdinov, PhD, approved the 1068 nm CerebroLite device as a safety trial. Ethics approval was obtained and recruitment began in June 2017 as a single-center, double-blind, randomized, placebo-controlled trial in April 2018. Subjects (n = 12, 4 active and placebo 8) were all from the Plummer Movement Disorders Center of BSWH, Temple, TX. The study was “to determine the effectiveness of this new light stimulation helmet on executive functioning (attention, working memory, learning and remembering strategies, planning, organizing, self-monitoring, inhibition, and flexible thinking) in subjects diagnosed with early-stage dementia.” Therefore, since all subjects were drawn from the patient pool of the Movement Disorders Center, all subjects were doubly diagnosed with Parkinson's disease so that they could serendipitously evaluate the PBM treatment on memory and cognitive functions of subjects, motor planning, coordination, and expressiveness of behavior.
Pilot PBM Study Results: Pre/Postactive and Placebo QEEG Analysis
Baylor Scott & White Pilot PBM study results are shown in Fig. 7. Pre/postactive and placebo QEEGs are from a new unpublished ongoing trial of PBM in dementia in Temple Texas (Fig. 8).

Baylor Scott & White Pilot PBM study results. Pre/postactive and placebo QEEGs.
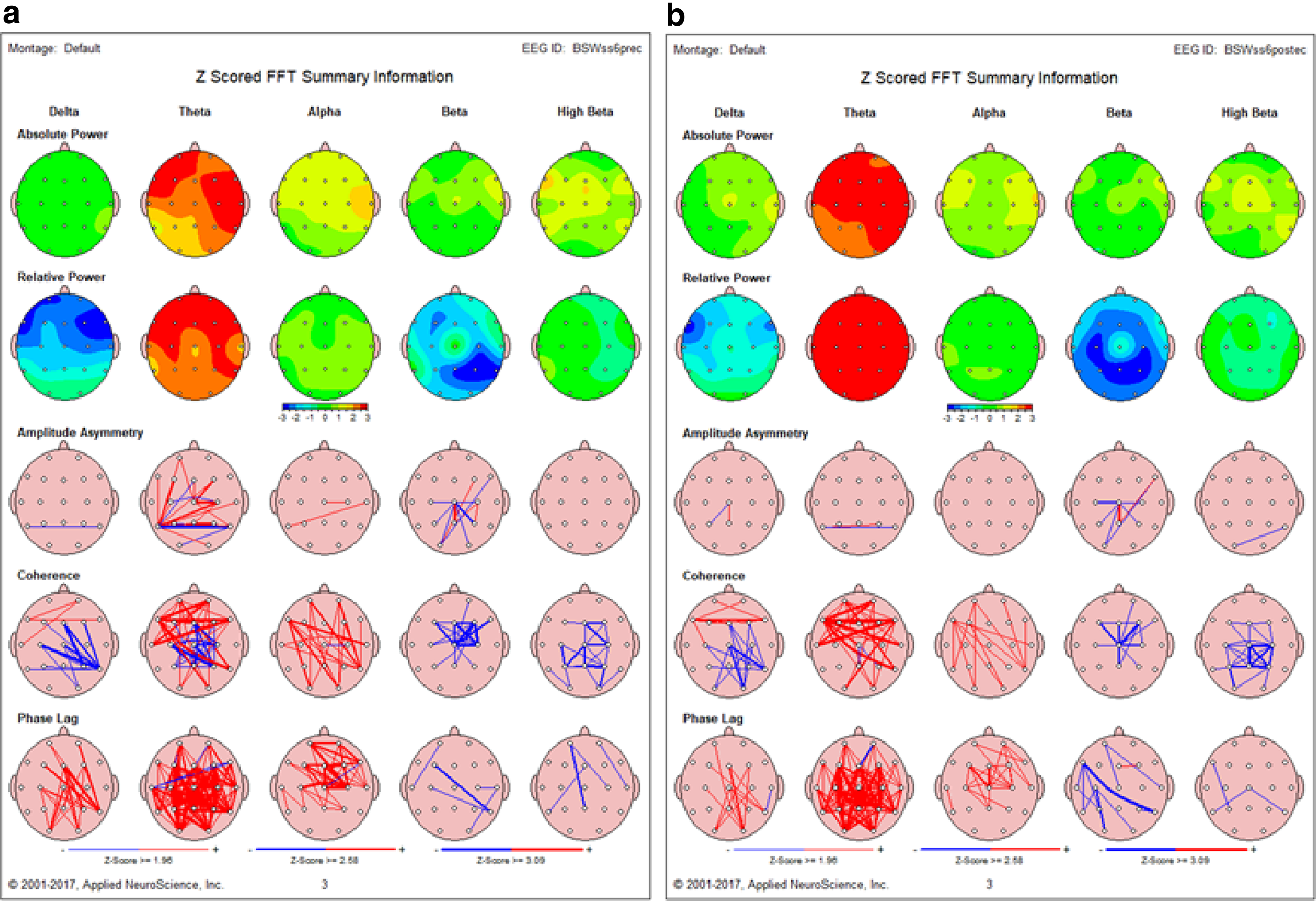
Active treatment pre/post QEEG summary analysis.
These findings, which highlight the impact of PBM on amplitude reduction but little to no effect on neural connectivity, underline the need for an intervention strategy to reduce inflammation, enhance regional cerebral perfusion, and ATP and interhemispheric and higher order network connectivity that is directly affected by neurofeedback training.
Neuropsychological Testing Results
In addition to the QEEG, MMSE, ADAS-Cog, Auditory Verbal Learning Test, Category Fluency Test, Trail Making, Boston Naming, and WAIS-R digital symbol substitution, Clock Drawing Test is a standard tool for procedural and practical memory evaluation.
Examples of two active treatment subjects below show significant improvement. See Fig. 9 below for clock drawing pretreatment and post-treatment. Next-generation trials with the CerebroLite for Parkinson's disease subjects will incorporate the insights regarding significant bilateral occipital hypocoherence deficits gained from the QEEG analyses. Stimulation protocols will focus more stimulation toward the occiput by reversing the ocular device's ocular arrays to stimulate the foramen and thereby increasing the level of PBM stimulation to the substantia nigra where it is shown that large numbers of dopamine neurons are negatively affected. 5 Use of this technique has improved gait, bradykinesia, and cognitive-behavioral responsiveness in clinical practice especially in combination with intensive neurofeedback training to correct bilateral occipital hypocoherence.

Clock drawings. Clock Drawing Test is a standard tool for evaluation of procedural and praxis memory. Clock drawing has been found to be moderately sensitive and specific for detecting executive cognitive dysfunction in people even with normal MMSE (Angela et al.).
39
Similar results were obtained using the transcranial and intranasal 810 nm 10 Hz pulsed PBM technology developed by Vielight's Neuro Alpha. In a randomized placebo-controlled trial, Saltmarche (2016) studied 19 subjects with varying degrees of dementia using a combination of transcranial (PBM) and intranasal (PBM) to investigate the effect of the Vielight Neuro system on subjects with dementia and mild cognitive impairment. To investigate the effects of PBM on memory and cognition, this was a single-blind study. With a follow-up period of 4 weeks, subjects with impaired memory/cognition were randomized to active and sham treatments over 12 weeks. They were evaluated with scales of MMSE and ADAS-Cog. The protocol involved in clinical use of a combined transcranial/intranasal PBM device and in-home use of an intranasal device-only PBM device and daily experiences were noted in a journal by participants/caregivers. Researchers noted that active participants with moderate-to-severe impairment (MMSE scores 5–24) showed substantial improvements after 12 weeks (5-point MMSE score). A significant improvement in ADAS-Cog scores has also been observed. They also reported better sleep, less angry outbursts and wandering, and decreasing anxiety. During the 4-week follow-up period of no-treatment, symptom declines were noted. Participants with mild-to-normal impairment (MMSE scores 25 to 30) in both active and sham subgroups showed improvements, demonstrating that the phenomena may reflect passive sensory stimulation that may occur in clinically controlled trials. 25
Applying Directed Energy in Alzheimer's Treatment
PBM is one of the several noninvasive methods of influencing core biological functions, including transcranial magnetic and pulsed electromagnetic fields and transcranial ultrasound that are being used in studying and treating a wide range of functional and metabolic disorders. 26,27 The application of neuromodulation in Alzheimer's was first reported by Nichols and Pearce (2006) using moderate magnetic field therapy to treat AD. Their report in the Society for Neuroscience involved magnetic therapy of 0.5 Tesla using two large and strong nonpulsing DC electromagnet fields' stimulation with the subject lying between two large electromagnets. The treatment produced a temporary increase in the magnetic force on the atoms of the body resulting in a higher velocity and precession of certain orbiting electrons, thereby increasing electron transfer and chemical reactions. 28 AD is a neurodegenerative disease secondary to oxidative stress, associated with genetic and environmental factors such as exposure to pesticides and heavy metals with subsequent depletion of mitochondrial protective enzymes, superoxide dismutase, and glutathione via free radical toxicity. 29
This along with gene expression demonstrated by Wang, Che, Du, Ha, and Yarema at Hopkins has shown that by modulating cell signaling and differentiation, thousands of genes could be regulated up and down by moderate magnetic fields in two human embryonic stem cell lines. 30 NASA researchers have also shown that picoTesla magnetic fields in human neuronal cell results vary in similar molecular genetic changes regarding growth potential as measured by gene chip analysis of 10,000 genes. 31
Pulsed Frequency Significance in PBM
When applying PBM to many biological systems, the pulsed wave (PW) mode was reported to be more effective than the continuous wave mode. The reason for PW-PBM's higher efficiency is poorly understood, however, hereafter for treatment with PBM, Kim and associates recently suggest using delayed luminescence (DL) as a reporter for mitochondrial activity. DL originates primarily from reactive oxygen species (ROS) and ATP transmission chain systems with mitochondrial electron. DL's decline time depends on the pulse frequencies of applied light that correlate with human dental pulp stem cell (hDPSC) biological responses. Using low-power light, the wavelength of which is 810 nm and 38 mJ/cm2 of energy density, a pulse frequency of 300-Hz prolonged the DL pattern and increased alkaline phosphatase activity. They also analyzed morphological mitochondrial changes and their volume density and found evidence to support physiological mitochondrial changes with an increase in length, not number, from PBM treatment. Their data suggest a new methodology to determine the efficacy of PBM in differentiating hDPSCs and the specific pulse frequency. One of the most important findings in this study is that pulsing PBM brings differential biological consequences according to the pulsing frequency. The DL lifetime was longer after PW-PBM irradiation, and the effects of rotenone, antimicrobial antibodies (AMA), and N acetylcysteine (NAC) depended on the pulse frequency. Whereas cells treated with 30–300-Hz PW-PBM had higher and longer lasting DL in all cases, and cells treated with lower or higher frequency PW-PBM showed big changes when complex III blocking agents AMA and NAC were added. DL signals were more affected by a complex III blocking agent (AMA) than by a complex I blocking agent (rotenone). The authors assumed that the different wavelengths of light originated from this difference. Many studies used UV-VIS light, and flavins or nicotinamide adenine dinucleotide was their target molecule. The target molecules should be different because they used NIR light in this study. Cytochrome c and COX are known to absorb longer wavelength light, including NIR, which supports the role of complex III in NIR-induced DL25 neurons. Excited or metastable-state cytochrome c could bind with complex III forward or backward depending on the environmental conditions, as observed. 32
Conclusions
As evidence of its effectiveness continues to appear in peer-reviewed literature, PBM applications continue to evolve. Approximately 5300 to 6300 studies containing the search terms “photobiomodulation therapy,” “low level laser therapy,” and “low level light therapy” are shown in the PubMed database. Clinical applications will continue to evolve from the clinical research focus of the Quietmind Foundation on the design and development of at-home and day treatment programs for neurodegenerative and neuropsychiatric disorder treatment. The integration of PBM tissue-level treatment and neurofeedback for neural connectivity renormalization is rooted in the understanding that, “in the final analysis, the only part of our being that holds a relationship with the external world is the nervous system” (Feldenkrais, 1949). The benefits of a more efficiently (robustly adaptive) functioning central nervous system that interacts within a healthier biochemical ecosystem can be leveraged in this way. It is hoped that by adopting a systems-centered approach, we are enhancing our ability to address the etiological complexities inherent in neurodegenerative disorders and to design direct clinical service models within our health delivery systems more successfully that can support the development of neurodegenerative treatment and prevention strategy. 33
Collective efforts within and between the relevant disciplines are now focused on design, engineering, and development of algorithms to integrate neurophysiological (LORETA z-score neurofeedback), cardiodiagnostic (heart rate variability), and frequency-specific, targeted energy and PBM to deliver scalable, safe, reliable and effective, home-based, and affordable neurotherapeutic treatment solutions. Such programs would increase health at the tissue level, thereby enhancing neurophysiological sensitivity that is enhancing the ability to discriminate similarities and differences and functional health, resulting in improved neurocognitive functioning. Heart rate variability (HRV) consistency and EEG consistency and phase-related activity can then be used as a measure of broad systemic flexibility and, as such, a neuromarker that relates to our capacity for adaptive responsiveness. 34
Neurotherapeutic techniques that measure evoked EEG dominant frequency activity can be used to guide treatment, first by introducing pulsed electromagnetic stimulation below conscious awareness level and monitoring changes in dominant frequency activity. Operationally understood as its approximation of randomness, this real-time dominant frequency variability can then be evaluated and combined with the normalization of EEG amplitude, consistency, phase lock, and phase reset. 35,36
PBM not only increases mitochondrial energy but also may increase bioenergetics of DNA epigenetics such as methylation, histone modifications, and chromatin structure. Such epigenetic factors of AD have recently been reviewed. 37
Antiviral effects of PBM at 1072 nm in herpes labialis have been demonstrated in a double-blind study and are significant since herpes simplex has been demonstrated to induce AD-related neuronal production and accumulation of Aβ, hyperphosphorylation of tau proteins, dysregulation of calcium homeostasis, and impaired autophagy. 38
Future applications will integrate noninvasive stimulation delivery, including full-body and transcranial and infrared light with pulsed electromagnetic frequencies. Ultrasound, microcurrent, pulsed electromagnetic fields, infra-low electromagnetic energy, and digitally transformed analog sound may be added, as new research demonstrates their additional uses and power to the therapeutic enterprise.
Footnotes
Acknowledgments
The authors have not received any government or foundation grants in support of this article. The authors have Intellectual Property via U.S. Patents for PBM with NBF (M.H.B.) and Moderate Magnetic Fields in Gene Expression (T.W.N.), respectively.
Author Disclosure Statement
No competing financial interests exist.