
Abstract
Objective:
Given the tremendous progress in biophotonics applications in biology and engineering, we sought to examine the evidence for the use of low-dose biophotonics treatments, termed photobiomodulation (PBM) therapy, in pediatric dentistry.
Background:
PBM therapy has been noted to alleviate pain and inflammation while promoting tissue healing and regeneration. These basic processes contribute to the fundamental etiopathogenesis of various oral diseases, and hence, there is now a growing list of potential clinical applications with PBM therapy in children.
Materials and methods:
An exhaustive literature search was conducted for PBM studies in pediatric dentistry that includes patients up to 21 years of age. An analysis of the quality of the included studies was also performed to evaluate the rigor of the evidence. Specific emphasis was placed on the treatment efficacy on the relevant specified outcomes for individual applications.
Results:
From a total of over 420 initial hits, 19 studies were deemed suitable for inclusion in this review. Among them, PBM therapy has been used in pediatric dentistry for prevention and treatment of oral mucositis associated with oncotherapy (chemotherapy, radiation, and transplants), for postsurgical oral pain and for pulpotomies. Overall, all studies reported therapeutic benefits, and no adverse effects were reported.
Conclusions:
This review noted that PBM therapy is a safe and effective treatment modality for various clinical applications in pediatric dentistry. Despite potential positive publication bias, there appears to be clear evidence of clinical benefit with this treatment, and we recommend well-designed randomized, placebo-controlled human clinical trial be pursued.
Introduction
Photobiomodulation (PBM) is the term, today universally accepted, to define a wide range of low-parameter laser applications, in the visible and infrared range of the electromagnetic spectrum that is capable of alleviating pain and inflammation while promoting wound healing and tissue regeneration. The term “PBM” was formally adopted by the field that was considered most suitable to replace a plethora of older terms such as “Low-Level Light/Laser Therapy” (LLLT), “Biostimulation,” “Photostimulation,” “soft laser,” and “cold laser” among many others that have been used since the 1970s. 1 –3 Endre Mester, a Hungarian physician, performed the very first animal studies of PBM therapy in 1960s. He was examining the possible carcinogenic effects of the coherent light (ruby laser, wavelength of 694.3 nm) in animal models. Contrary to their expectations, they were surprised to find that laser treatments at very low-energy densities (1 J/cm2) were capable of promoting phagocytosis of bacteria by leukocytes, improve hemoglobin synthesis, and stimulating wound healing and tissue repair, especially in healing of ulcerative lesions unresponsive to conventional therapies. 4,5
The broad clinical impact of PBM therapy extends to its ability to stimulate healing in both soft tissues such as mucosa and skin as well as mineralized tissues such as bone and teeth. A better understanding of the biological responses to PBM therapy has outlined three discrete cellular mechanisms involving the cytochrome c oxidase in the mitochondria, light-sensitive receptors on the cell membrane, and an extracellular latent growth factor complex, TGF-β1. 6 These discrete mechanisms have been down to modulate the specific PBM therapeutic benefits on pain, inflammation, and wound healing. These effects, together with the noninvasive nature of the treatment, absence of any known side effects or adverse events, and relatively fast learning curve for the operator are some of the reasons PBM is gaining tremendous popularity.
The term “Pediatric dentistry,” once called “Pedodontics,” is the branch of dentistry dealing with children from birth through adolescence. The Forsyth Dental Infirmary for Children opened in Boston in 1914 to provide dental treatment for children and is considered the first institution of its kind in the world that is uniquely dedicated to clinical dental care for children. 7 A major limitation with these groups of patients treated is related to the anxiety and fear of dentistry, especially with special needs. 8 Hence, novel noninvasive technologies can alleviate pain and anxiety and facilitate improved relationship between dentist and the patient along with reinforcing an overall positive attitude toward oral health. 9,10 The aim of this work was to critically analyze the peer-reviewed literature describing the use of PBM treatments in pediatric dentistry and outline the evidence and clinical treatment parameters.
Materials and Methods
Search strategy
The review strategy followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). To access relevant articles, an electronic search in Medline (PubMed), Google Scholar, Science Direct, and Cochrane Controlled Register of Trials (Central) were performed. English language published articles were looked for using the following keywords: “Laser PBM” [MeSH]) OR Low Level Laser Therapy [MeSH] OR “Laser Biomodulation” [MeSH] OR “Photobiomodulation” [MeSH] AND “Pediatric Dentistry” [MeSH]). The search performed using the “age” filter to limit the publications involving subjects up to 21 years as per the determination of pediatric age published by the American Academy of Pediatrics. 11
A second search was performed, with the same kind of filter, for every topic found in the first search: “pulpotomy,” “oral mucositis,” “postoperative oral pain,” “oral herpetic lesion,” and “oral aphthous lesion.” Two reviewers (E.M. and C.F.) have contributed to the search and evaluated the article database and checked the reference list of relevant articles and previous reviews on the subject: initial article selection was done examining titles and abstracts of all selected articles. The full texts of potentially suitable articles were obtained for final assessment according to the exclusion and inclusion criteria. The following data were extracted from the studies: study design, sample size, mean age or ages range, laser characteristics (wavelength, frequency, energy density, power, power density, time of application, and number of sessions), evaluation criteria, and success rate. Mean values, standard deviations, and sample size were also extracted from the articles where they were reported. Where fluences and power densities were not reported, the authors (E.M. and C.F.) calculated them on the basis of other reported parameters. In addition, a manual search of the table of contents from 2000 to current issues of all major dental laser journals, including Lasers in Medical Science; Photodiagnosis and Photodynamic Therapy; Photobiomodulation, Photomedicine, and Laser Surgery; Laser in Surgery and Medicine, and Photochemistry and Photobiology B. The references in all final articles identified for the review were also cross-examined for relevance.
Inclusion criteria
All the original in vivo studies applying PBM or low-level laser on patients younger than 21 years of age were included in this study. All animal studies and in vitro studies were excluded, as well as case reports, guideline articles, and reviews. The inclusion criteria were as follows: (1) human clinical studies utilizing PBM treatments with/without a control or placebo treatment group; (2) participants with age ≤21 years; (3) studies where outcomes were clearly described, for example, intensity and duration of pain using the visual analog scale (VAS), Numeric Rating Scale, or other types of questionnaires; and (4) studies published in English. Following further discussions among reviewers on the initial search results, all relevant clinical studies even without controls or placebo were included in this review due to the very limited number of publications available.
Exclusion criteria
The exclusion criteria were as follows: (1) studies in vitro or in animals; (2) studies that used high-power lasers; and (3) literature reviews, case reports, letter to editors, unpublished theses, or abstracts of meeting presentations.
Data summary, quality, and meta-analyses
Any discrepancies were resolved by discussion or consultation with a third reviewer (J.P.R. and P.A.). Methodological quality of included studies was realized on the basis of Cochrane's collaboration tool analyzing selection bias (adequate random sequence generation and allocation concealment), performance bias (adequate participant and personnel blinding), attrition bias (acceptable and described dropout rate), reporting bias (no selective outcome reporting), and detection bias (adequate outcome assessor blinding). 12
Meta-analysis was performed with Review Manager Software (5.0.16 Version). Results, as for example pain intensity, reported as continuous data with standard mean difference were calculated and pooled using the weighted mean difference and 95% confidence interval (CI), for dichotomous data, as for example incidence of oral mucositis (OM), data were synthesized using odds ratio as the effect measure with its 95% CI.
Results
Study selection
The PubMed Search Provided 294 hits, Google Scholar search 402 hits, Cochrane Search 41 hits, and Science Direct 84 hits. Following the initial screening of titles and abstracts and final screening of full texts, 19 articles completely fulfilled the inclusion criteria of this study (Fig. 1). All original data are summarized to enable optimal illustration of key data (Tables 1 –4). Furthermore, all laser parameters, particularly Fluence and Irradiance (Fig. 2), were summarized (Tables 5 –7) and methodological quality of all included studies described (Fig. 3 or Tables 8). 11

Screening of titles and abstracts and final screening of full texts to obtain the 19 articles completely fulfilling the inclusion criteria.
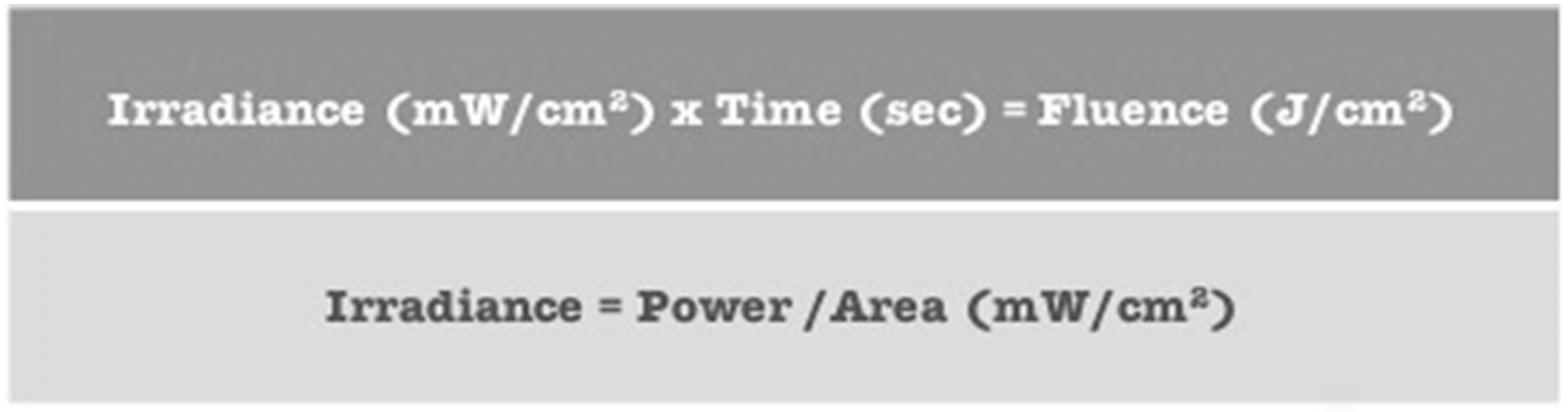
Laser parameters, particularly fluence, and irradiance.
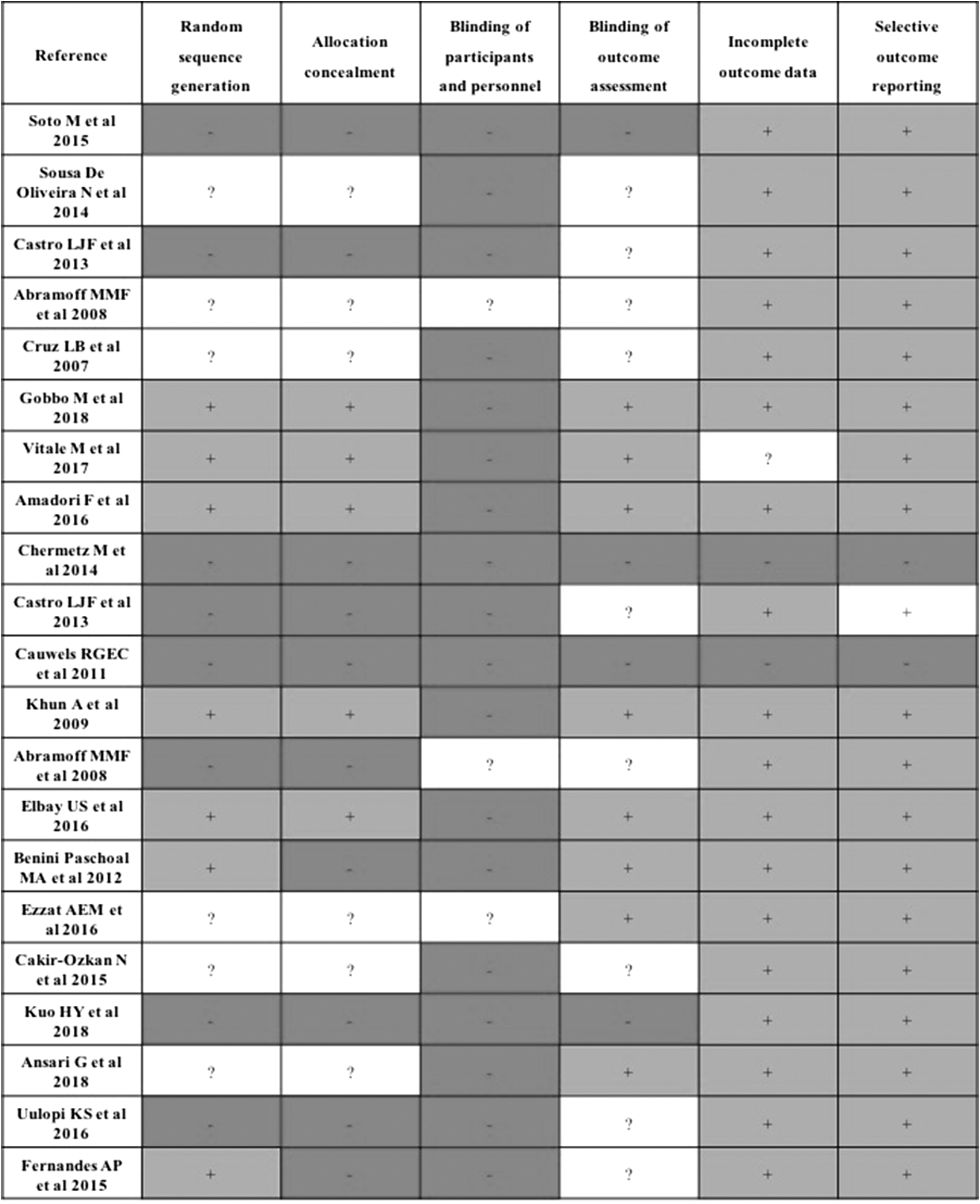
Methodological analysis of all included studies described.
Baseline Characteristics of Included Studies on Prevention of Oral Mucositis
p Lower than 0.05 for comparison laser versus control.
CT, controlled trial; CTher, chemotherapy; d, days; FMS, functional Mucositis Score; HCT, hematopoietic cells transplantation; HSCT, hematopoietic stem cells transplant; LEL, low-energy laser; LLLT, low-level laser therapy; M, male; OM, oral mucositis; RCT, randomized controlled trial; SD, standard deviation; W, woman.
Baseline Characteristics of Included Studies on Treatment of Oral Mucositis
p Lower than 0.05 for comparison laser versus control.
CTher, chemotherapy; HSCT, hematopoietic stem cells transplant; RCT, randomized controlled trial; VAS, visual analog scale.
Baseline Characteristics of Included Studies on Postoperative Pain
p Lower than 0.05 for comparison laser versus control.
Baseline Characteristics of Included Studies on Pulpotomy
CH, calcium hydroxide; FC, diluted formocresol; CH preceded by LLLT (LLLT + CH), calcium-enriched mixture cement CEM; MTA, mineral trioxide aggregate.
p Lower than 0.05 for comparison laser versus control.
Laser Parameters of Included Studies on Prevention and Treatment of Oral Mucositis
CT, chemotherapy; CW, continuous wave; PW, pulsed-wave.
Laser Parameters of Included Studies on Postoperative Pain
Laser Parameters of Included Studies on Pulpotomy
Methodological Quality of Included Studies on Prevention and Treatment of Oral Mucositis on the Basis of Cochrane's Collaboration Tool Analyzing Selection Bias of Included Studies
Quality of the included studies
The most frequently unsatisfactory methodological criteria were the blinding of participants and personnel: the 85.7% of the included studies were at high risk and the remaining 14.3% were unclear, while the blinding of the evaluation was at high risk for the 19% and unclear for the 43% (Fig. 3). Among the selection bias, random sequence allocation was at high risk in the 38% and unclear in the 28.5%, while allocation concealment was at high risk in 47.6% and unclear in 28.5%. Blinding outcome assessment was unclear in the most part of the studies (42.85%). Among attrition bias, incomplete data outcome was at low risk for the most part of included studies (85.7%), and among reporting bias, selective outcome reporting was at low risk for the 90.5% of included studies.
Laser source, parameters, and frequency of treatments
All the devices used in the included studies were diode lasers, in particular near infrared laser devices with wavelengths of 830 and 970 nm, and were the most used for analyzed trials, followed by visible red light at 660 nm. Power density or fluence was not fully described in all the studies, even if for some study, the reported parameters allowed reviewers to calculate them based on these equations (Fig. 2). Another consideration to make is that the frequently reported fluence is theoretical because it is calculated on the basis of the fiber or handpiece diameter but not on the spot area (in defocalized mode) or on the treated area (in scanning mode).
For all the included treatments, the application was only at intraoral level, except on the prevention of mucositis, for the study of Soto et al., 13 the application was at 19 intraoral and 6 extraoral points, and for the study of Abramoff et al., 14 the application was also involving labial commissures. For the prevention of OM, treatment was performed starting at day 1 of chemotherapy or conditioning every day until day 5, 13 –17 while for OM, treatment was performed at the appearance of OM every day. 14,16 –21 For OM prevention, PBM duration was variable between 10 and 54 sec per point, 13,14 while for OM treatment, PBM duration was variable between 2016 and 230 sec. 21 In study performed to check the effect of PBM on postsurgical or postextractive pain, the application of laser, varying between 1724 and 60 sec 25 –27 per application point, was realized every 24–48 h, starting from immediate postsurgical time until eight treatments. 24 –27 For pulpotomy, a single laser-assisted procedure was performed in all studies and the duration of laser application was variable between 10 28,29 and 135 sec. 30,31
PBM for prevention and therapy for oral mucositis
Prevention of OM
Out of the five studies on prevention of OM included in this review, four 13 –16 reported a positive effect with a reduction of incidence and grading of OM for laser groups compared with control groups and in three out the four studies in a statistically significative way (Fig. 4). 13 –15 Only the study of Cruz et al. 17 did not describe an evidence of benefit from the prophylactic use of PBM in children and adolescents with cancer treated with chemotherapy when optimal dental and oral care were provided. 17
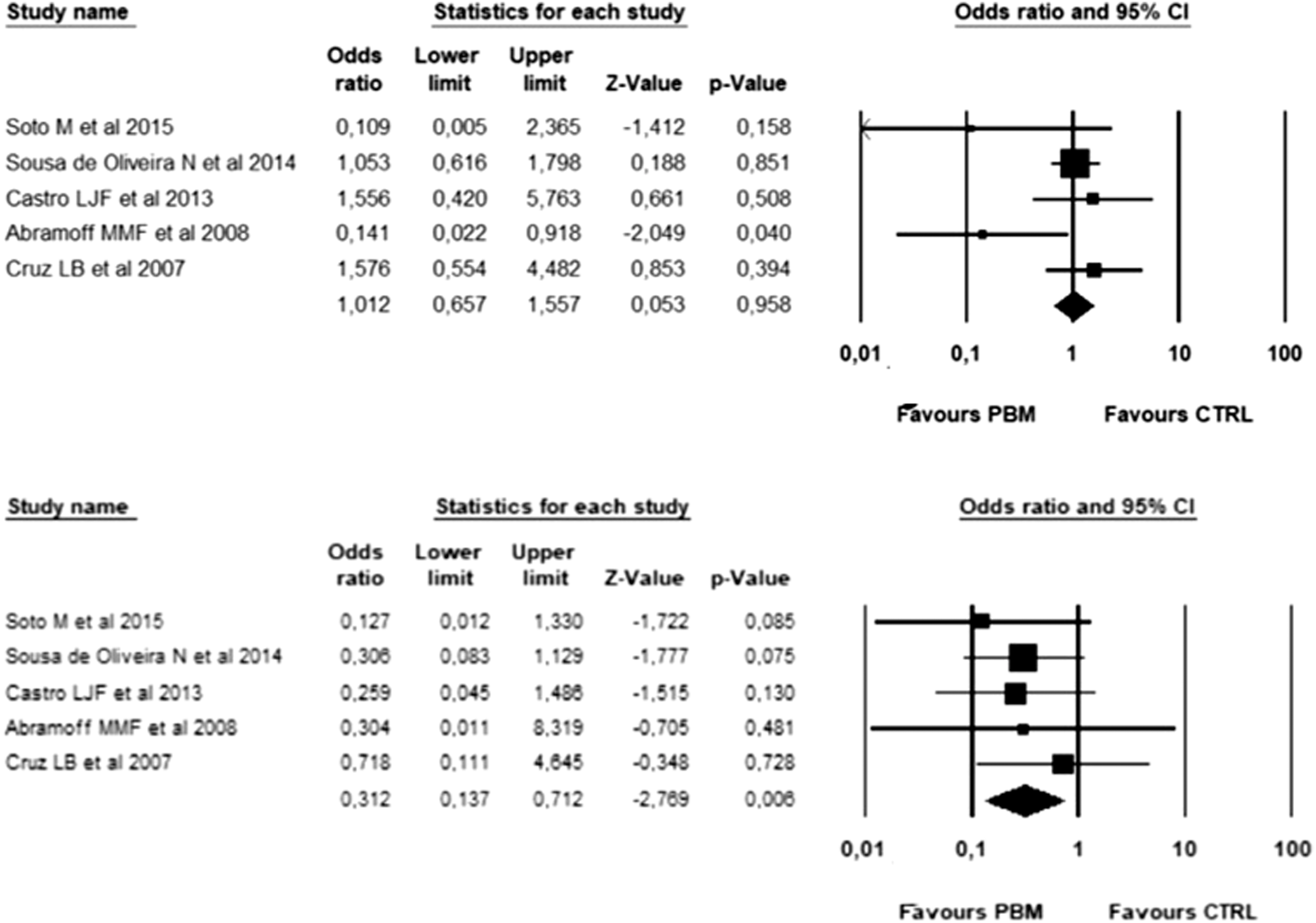
Meta-analysis for PBM in prevention protocols for OM: results for incidence of OM (upper) and for incidence of Grade 3 and 4 of OM (lower). OM, oral mucositis; PBM, photobiomodulation.
Treatment of OM
All nine studies on treatment of OM included in this review reported positive effect for PBM on grading, 14,16,18 –20 pain, 18 –21 and duration 23 of OM, and in three of them a statistically significative difference; 18,20,23 Chermetz et al. reported also an improved swallowing. Results for analysis in depth are reported in Fig. 5. 21

Meta-analysis for PBM in treatment protocols for OM: effects on pain evaluated by VAS at 7 days. VAS, visual analog scale.
PBM therapy to alleviate postoperative pain
Two of the four included studies 24,25 did not describe a significative difference in postoperative pain of treated and not treated adolescent following primary molar or premolar extraction (Fig. 6). Conversely Ezzat et al. 26 described a statistical difference in pain evaluated with a VAS at different times of evaluation, precisely in the first 3 days after the secondary palatal operations. Only Çakir-Özkan et al. 27 analyzed the bone density after mandibular midline distraction with a difference at 12 weeks relevant also from a statistical point of view. Analysis in depth was realized for postoperative pain 1 day after surgery for the studies of Ezzat et al. 26 and Elbay et al. 25 (Fig. 6).
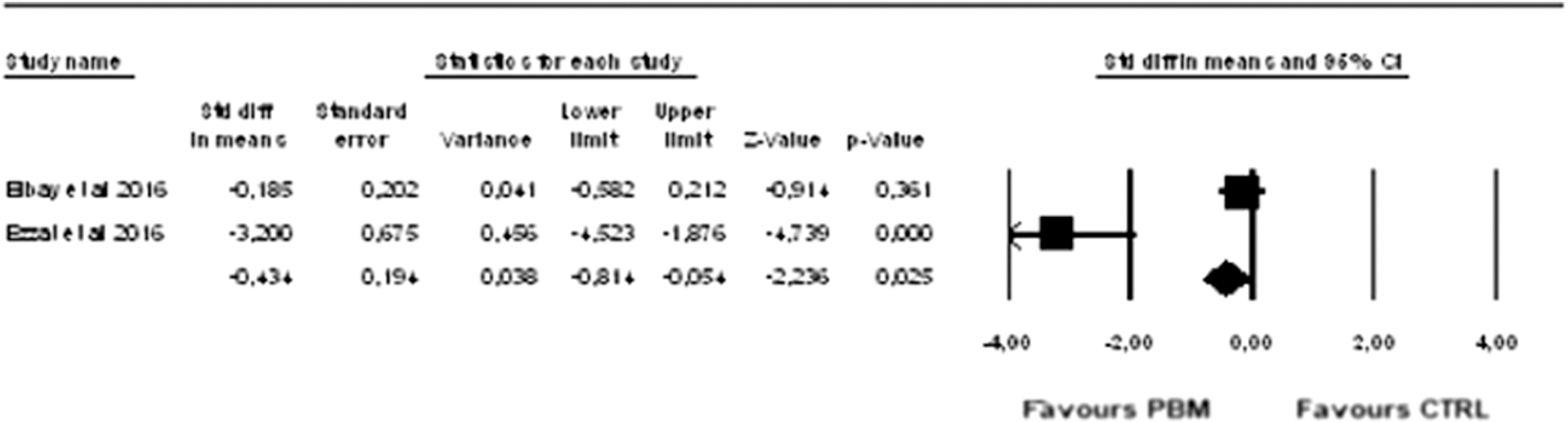
Meta-analysis for PBM in treatment protocols for postoperative pain: effects on pain evaluated by VAS at the first day after surgery.
PBM treatments for pulp healing
Only the study of Fernandes et al. 29 described the effectiveness of the pulp treatment adding PBM to calcium hydroxide even if without statistically significant differences. Uloopi et al. 28 described PBM as a complementary step to pulpotomy procedure in the comparison between PBM and mineral trioxide aggregate, while Ansari et al. 30 and Kuo et al. 31 did not describe any difference by adding or not adding PBM (Fig. 7).

Meta-analysis for PBM in pulp treatment protocols: effects on clinical (upper) and radiological (lower) success at 12 months after treatment.
Discussion
The present systematic review included randomized clinical trials to evaluate the performance of PBM when used in pediatric dentistry. The studies presented in these systematic reviews and meta-analysis showed that PBM is a technique, which may represent a great help also when used in the field of the pediatric dentistry. In fact, the literature reports a large number of publications, where the success of this technique is statistically significant and the absence of side effects and contraindications is confirmed, this being a strong indication to use PBM for this kind of patients.
The clinical applications of PBM in pediatric dentistry analyzed in this study included its utilization in the fields of the treatment and prevention of OM, control of postsurgical oral pain, and its use for pulpotomy procedures. The most interesting and clinically useful aspect concerning PBM is represented by the choice of the parameters to use: in fact, in the field of PBM is necessary not to exceed a certain energy to avoid the possibility of provoking opposite effects, according to the Arndt-Schultz law; 32 unfortunately, several of the analyzed studies did not report power density, a fluence used, and in many other articles these parameters were calculated only on the basis of the fiber diameter, and this, particularly when laser is not used in contact mode, does not correspond to the real evaluation.
The devices of all the studies were diode lasers, which are solid-state semiconductor lasers typically using a combination of Gallium (Ga), Arsenide (Ar), and other elements such as Aluminum (Al), and Indium (In), to change electrical energy into light energy, emitting both in visible and near infrared portions of the electromagnetic spectrum. In almost all the articles, laser device was used intraorally, while the modes were both in continuous wave and pulsed; in the majority of the cases, the handpiece was positioned not in contact with the tissues and maintained perpendicular to it for reducing the quantity of the reflected energy of the beam. In none of the studies were reported the side effects or incidents related to the use of laser device, and this aspect is very important for confirming the safety of PBM, when using with the respect of the ANSI safety rules, which are mandatory to be observed by operators, nurses, and patients. The highest number among the publications of this study is with regard to the utilization of PBM for the treatment and the prevention of chemo- and radio-induced OM, while less articles are referred to utilization of PBM for the pulpotomy in the primary teeth. Other different applications of PBM in pedodontics, such as its utilization for controlling the gag reflex in children during intraoral radiography or for treating Recurrent Labial Herpes Simplex, were not taken in consideration due to the low number of publications (one for each of the topics).
Conclusions
In summary, the present systematic review demonstrated the positive effects of PBM utilization in pediatric dentistry with the different protocols and light parameters described in the analyzed articles. Therefore, more future clinical researches will be necessary to further explore the efficacy of PBM in pediatric dentistry, also by enlarging the indications and the fields of utilization.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding provided for this article.