
Abstract
Objective:
We aimed to evaluate the efficacy of photobiomodulation (PBM), using an 635 nm diode laser, to provide pain relief for temporomandibular disorder (TMD).
Background data:
TMD involves a set of multiple clinical manifestations where pain is prevalent. Treatment ideally should be noninvasive and innocuous such as PBM.
Methods:
A randomized, placebo-controlled, clinically blinded trial was performed on 42 patients with painful TMD diagnosed according the Research Diagnostic Criteria for Temporomandibular Disorders. They were randomly placed into two groups: an intervention group (n = 22) subjected to the application of a 635 nm wavelength diode laser (using a 8-mm diameter handpiece in contact mode, delivering 8 J/cm2 over a period of 20 sec applied over the sensitive points where the pain was reported by the participants) and a placebo group (n = 20) following the same protocol but without laser activation. All patients received four sessions of treatment over 4 weeks. Personal pain perception, nonassisted pain-free maximum mouth opening and tenderness elicited during palpation of muscles were used as primary outcomes, evaluated at baseline and at follow-up 1 month later by blinded, calibrated evaluators.
Results:
There was a significant reduction in the degree of pain recorded in the laser group after treatment (0.63 ± 0.36) compared with the baseline evaluation (4.59 ± 2.36; p < 0.001), which was not observed in the placebo group. Reduction of pain during palpation of most masticatory muscles was significant following treatment in the intervention group. A significant increase in the nonassisted painless mouth opening was observed after treatment (42.14 ± 5.8 mm) compared with baseline values (36.73 ± 9.91 mm) only among the laser group (p = 0.007). There were no reported adverse events or side effects among the patients in the intervention group.
Conclusions:
Our results suggest that PBM using a 635 nm laser was effective on the remission of painful TMD, without complications.
Introduction
Temporomandibular disorders (TMD) are defined as a set of disorders affecting the masticatory muscles, temporomandibular joint (TMJ), and associated structures and characterized by the presence of pain, joint sounds, and/or limitation of mandibular movements. 1 –3 TMD is a group of several clinical conditions encompassing myofascial pain with or without limitation of mouth opening; displacement of disk with reduction or without reduction (with or without limitation of mouth opening) and also includes cases of arthralgia/osteoarthritis/or osteoarthrosis of the TMJ. 2 –4
TMD affect about 5–12% of the population with an annual incidence of 3.9% for pain-related TMD in the United States and have been reported to be more prevalent in females. 1,2,4 –6
TMD is probably the most common cause of pain of nondental origin in the maxillofacial region. 1,6 Pain is a major manifestation of TMD and can affect masticatory muscles, TMJ, and/or cervical region, or can present in the form of headaches or earaches. Other symptoms or signs can include tinnitus, vertigo, fatigue, and crepitation. Due to pain, discomfort or difficulty in performing mandibular movement's limitation of activities such as chewing, talking, swallowing, yawning, or smiling are common in patients with this condition. These may compromise the quality of life, sleep, and the psychological condition of the patient. 1,4,5,7
The etiology of TMD is multifactorial, often associated with trauma to the tissues caused by parafunctional habits, associated to anatomical (including occlusal and bone) alterations, local or systemic diseases, as well as psychosocial issues, including anxiety and also with heritable genetic events. 1,4,5,7,8
The correct diagnosis of TMD is fundamental for developing a good design of a treatment plan by a multidisciplinary team. Several treatment options are available, including elimination of parafunctional habits, occlusal splints, pharmacological agents, physical procedures involving postural and mandibular training, physical agents such as transcutaneous electrical nerve stimulation, ultrasound, acupuncture, and photobiomodulation (PBM). 9 –17
Lasers have been used in a variety of oral medicine procedures with several indications and when used with low power settings can produce photochemical and photobiological effects without causing any tissue ablation. 18,19 This is called PBM and includes the promotion of cellular functions (such as cellular growth and migration) or the modulation of any inflammatory response (resulting in a reduction of oedema and pain). 19 –22 PBM have been studied in TMD disorders with contradictory results and no study has addressed the usefulness of a 635 nm wavelength laser in painful TMD. 11 –18,22
This study aims to assess the efficacy of PBM with a 635 nm laser in the treatment of TMD-related pain in patients diagnosed with TMD as well as evaluation of its safety and patient's satisfaction level. Our hypothesis is that PBM using a 635 nm laser would be capable of decreasing pain related with TMD without significant complications in comparison with a placebo group.
Materials and Methods
Study population
A randomized, placebo-controlled, single-blinded clinical study was conducted with eligible patients over 18 years of age diagnosed with painful temporomandibular disorder between a period from March 2018 to October 2018 at the Oral Medicine Clinic of the University Institute of Health Sciences (IUCS), Oporto, Portugal. The study was authorized by the Ethical Committee of the University Institute of Health Sciences (No. 11/CE-IUCS/2018) and was performed according to the ethical guidelines of the Declaration of Helsinki. Full information of the study was given to all patients before obtaining a written informed consent for the participation in the study. Four questions were initially made for screening our patients: (1) presence of headaches more than once a week; (2) history of jaw trapped, or blocked, with limitation of opening of the mouth; (3) pain when opening the mouth or when chewing, perceived at least once per week; (4) pain in the face, TMJ or jaw, perceived at least once a week. On eliciting a positive response to one or more of these four questions, we administered a questionnaire (with a clinical examination) based in the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD). 3 The RDC/TMD has a biaxial approach, allowing, on the one hand, reliable measurement of the physical findings on Axis I and, on the other hand, evaluates the psychosocial status (depression, anxiety, and the relation of these factors to the physical symptoms) in Axis II, allowing the diagnosed evaluation of the dysfunction and related psychosocial conditions. 3 Patients who had a diagnosis of temporomandibular disorder with painful symptoms (with the presence of myofascial pain) based in the RDC/TMD criteria were included in the study.
Patients were excluded if: they did not report any of the features mentioned in the primary questionnaire; were not diagnosed with temporomandibular disorder, or who did not report pain (myofascial pain) after the clinical examination RDC axis I; if they were under another type of treatment for TMD (e.g., occlusal splints, pharmacological drugs, or head and neck surgery); had a neurological or a psychiatric disorder (evaluated by axis II of RDC/TMD); or could not attend the proposed treatment sessions or follow-up visits.
Of the 52 individuals initially selected to participate in this study, following the application of the inclusion and exclusion criteria, a final sample of 42 individuals were available for the analysis as shown on the flowchart (Fig. 1).
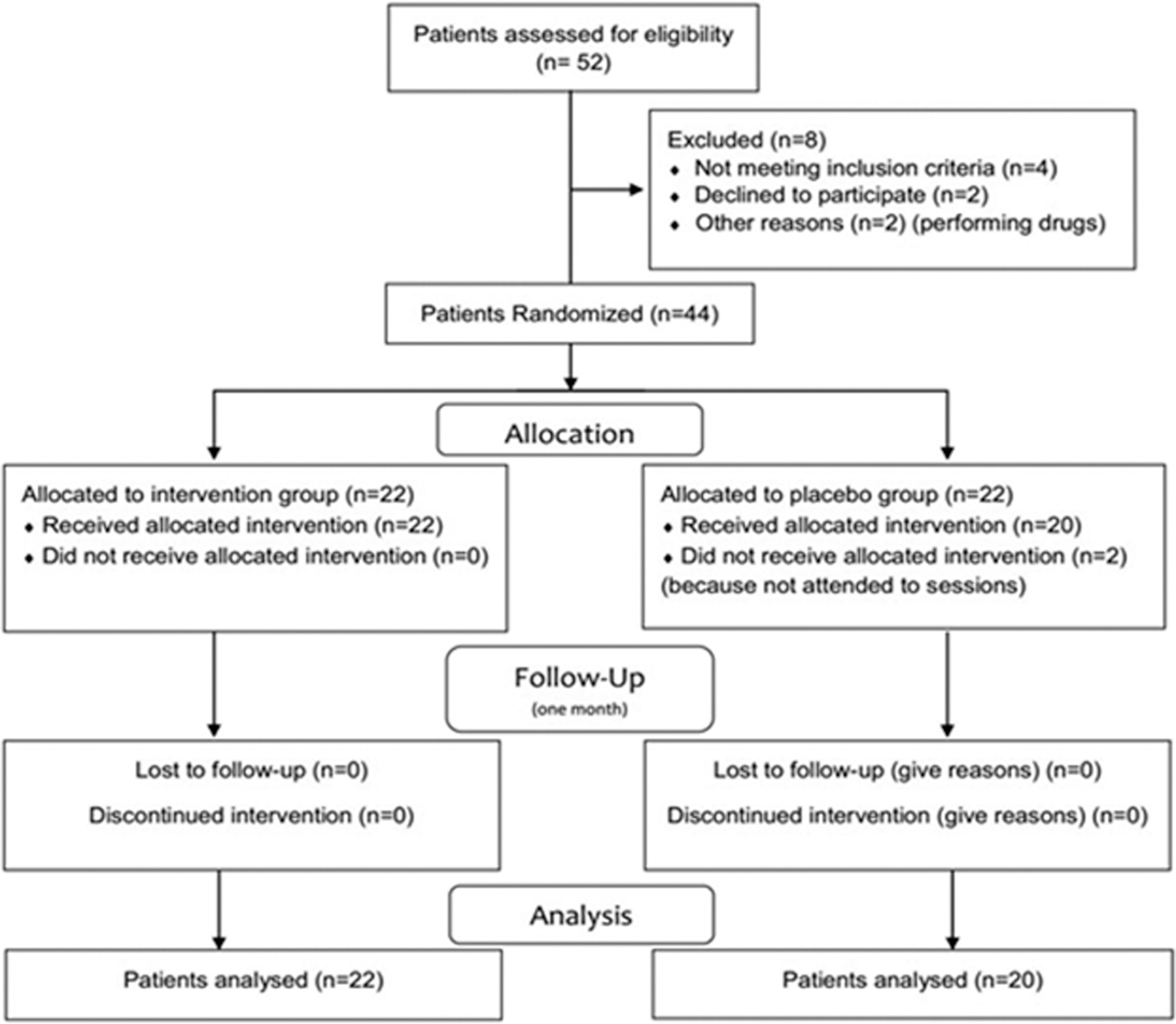
Flow-chart of the included patients.
Study groups and parameters used
Patients were randomly divided into two groups, an intervention laser group (n = 22) and the placebo group (n = 20 for analysis), using a lottery method performed during the diagnostic visit. For randomization, each patient selected a sealed envelope having a card corresponding to one of the possible groups and indicated by a code letter. The code was blinded to the patient and to the clinical evaluator. In the experimental group (laser group), a 635 nm wavelength diode laser (Lasotronix®, Diode Laser DiodeLX model SMART M; Żytnia, Piaseczno, Poland) was used with 200 mW in a continuous mode, using a handpiece with a cylindrical applicator with a diameter of 8 mm in contact mode, with a power density of 400 mW/cm2, delivering 8 J/cm2 on each application point, over a period of 20 sec. 23,24 Other laser parameters are listed in Table 1. The laser beam was applied over the sensitive points where the pain was reported by the participants as recorded in the diagnostic questionnaire. The laser application was performed over four sessions, during 4 consecutive weeks (one session per week). 25 All safety measures for protecting the patient, operator, and assistant were followed. The calibration of the output power of the laser was performed before the beginning of the study using a power meter device Ophir Nova II®, thermal head F150A, Israel. The placebo group received sham treatment with the procedure performed as same as the one performed in the experimental group, but without laser activation. This was using a handpiece with a spot of 8 mm applied over the areas where the patient reported pain. The placebo intervention was also performed in 4 sessions, during 4 consecutive weeks (one session per week).
Laser Parameters Used in the Intervention Laser Group
CW, continuous wave.
Evaluation criteria
A questionnaire included items related to demographic characteristics and to the clinical history of the patient. The Visual Analog Scale (VAS) was used to evaluate the personal TMD-related pain perception of the participants with 0 corresponding to “absence of pain” and 10 to the “worst pain ever felt.” With the RDC/TMD examination, additional data including nonassisted pain-free maximum mouth opening (recorded with a pachymeter in millimeters) and pain tenderness during palpation of the muscles (0–3 according to RDC/TMD) were evaluated and registered and used also as primary outcomes. We recorded any of complications during and after the treatments and the satisfaction (using a 0–10-point scale) of the patients as secondary outcomes. These evaluations were performed at diagnosis (baseline), and then were repeated 1 month after the last session of treatment by a trained and calibrated examiner, blinded to the group allocation.
Statistical analysis
Statistical analysis was performed using the SPSS® program, version 25.0. Data were analyzed through the use of descriptive statistical techniques and comparative analysis between groups. For the intragroup comparisons we used the Friedman test. The Mann–Whitney test was used for the comparisons between groups. The level of significance used for the statistical tests was 5%.
Results
Of the final 42 participants in the study, 32 (76.2%) were female, and 10 (23.8%) were male with a mean age of 27.4 (± 9.71) years. The duration of pain corresponded to 7.8 ± 5.9 years and the intensity of pain (VAS) was 4.52 ± 2.45, located on both sides of the face in 26 (61.9%) patients, right in 10 (23.8%), and left in 6 (14.3%) patients. At baseline before the treatment, during the extension of the vertical movements, nonassisted painless mouth opening was 37.38 ± 8.78 mm, right laterality movement was 13.02 ± 3.16 mm, left laterality 13.0 ± 2.87 mm, and protrusion of the jaw was 9.71 ± 3.61 mm.
Intergroup comparisons of outcome measures
At baseline there were no significant differences between demographic factors and clinical manifestations of TMD between the two treatment groups (p > 0.05) (Table 2).
Patient's Characteristics Included in the Study
SD, standard deviation; VAS, visual analog scale.
After treatment, there was a significant difference in the pain intensity between laser group (0.63 ± 0.36) and placebo group (4.05 ± 2.39; p < 0.001). We observed a higher nonassisted pain-free mouth opening in the laser group (42.14 ± 5.8 mm) compared with the placebo group (39.45 ± 5.3 mm), although this difference did not reach statistical significance (Table 3). Palpation of the muscles to assess pain revealed significant differences between the level of pain that was less in patients in the laser group compared with the placebo group in several groups of masticatory muscles, including the right temporal (posterior) (p = 0.030), right temporal (anterior) (p = 0.003), right and left masseter (body) (p = 0.001 and p = 0.03, respectively), right masseter (insertion; p = 0.011), right and left posterior mandibular region (p = 0.043 and p < 0.001, respectively), left submandibular region (p = 0.035), right and left TMJ-lateral pole (p < 0.001 and p = 0.006, respectively), left TMJ-posterior insertion (p = 0.029), and right and left lateral pterygoid superior to the retromolar area (p = 0.003 and p = 0.002, respectively) (Table 4).
Patient's Characteristics Before and After the Treatment
Significant p-values are indicated in bold numbers.
T1, baseline time; T2, 1 month after treatment.
Results of the Pain on Muscle Palpation Using Research Diagnostic Criteria for Temporomandibular Disorders
Significant p-values are indicated in bold numbers.
L, left; R, right; TMJ, temporomandibular joint.
Intragroup comparisons of outcome measures
In the placebo group, the pretreatment (baseline) mean pain value was 4.45 ± 2.6, and the posttreatment (T2) mean pain was 4.05 ± 2.39, with a level of significance above 5%. In the laser group, the degree of pain after the laser treatment (T2; 0.63 ± 0.36) was statistically lower than the degree of pain before treatment (T1; 4.59 ± 2.36; p < 0.001) (Table 3 and Fig. 2).

Boxplot of the patients submitted to laser or placebo intervention at baseline and 1 month after.
During the extension of the vertical movements, a significant increase in the nonassisted painless mouth opening was observed after the treatment (42.14 ± 5.8 mm) comparing with baseline values (36.73 ± 9.91 mm) for the laser group (p = 0.007), whereas in the placebo group any average increase in opening did not reach statistical significance (Table 3).
The mean pain values reported by participants during palpation of muscles on clinical examination of axis I are shown in Table 4. When comparing these values before and after treatment, a statistical difference was found for most groups of muscles in the laser group with reduction or elimination of pain on palpation. This did not occur in the placebo group for the majority of muscle groups (Table 4).
In the follow-up period (1 month after treatment) we assessed the patient satisfaction level (0–10 points) of the patients that were treated with laser and obtained a mean of 9.1 ± 1.1 compared with the value of 3.3 ± 1.4 for the patients of the control group (p < 0.001).
By a telephone interview, 3 months after treatment, we asked the level of pain experienced by the patients that were intervened with laser and it corresponded to 1.5 ± 0.59. This was still statistically significant compared with the level of pain before the treatment (p = 0.001). Regarding the satisfaction of the patients, the mean patient satisfaction level corresponded to 9.6 ± 0.85. Most of the patients (76.2%; n = 16) claimed that they were maintaining the successful outcomes after treatment, 14.3% (n = 3) were even better compared with the last follow-up and 9.5% (n = 2) were still feeling no improvement of their condition. One patient was lost to follow-up at 3 months.
Discussion
TMD involves a set of multiple clinical manifestations where pain is prevalent. 1 –6 For the treatment of TMD-associated pain, ideally, the first choice should be a conservative, noninvasive, and innocuous method, such as PBM therapy. In view of this, our main aim was to evaluate the efficacy of the PBM using a 635 nm wavelength diode laser in patients with pain related to TMD.
We observed a significant reduction on pain levels related with TMD, including the self-perception of pain, tenderness to palpation on masticatory muscles, an increase in the nonassisted painless mouth opening, and also a high level of patient satisfaction. This confirms our hypothesis that this protocol, using a 635 nm wavelength diode laser, was capable to decrease the TMD-related pain when compared with the placebo group without any complications.
Several studies have documented the positive effect of the PBM in TMD, including improvement of painful symptoms. 11,12,15 We observed a reduction on self-perception of pain after the treatment in the laser group but not in the placebo group. This pain reduction in a laser group in comparison with a placebo has been reported also by other authors. 22,26 –30 However, the reduction in pain has not been demonstrated in all studies 13 especially when compared with placebo groups. 25,31 –33 This could be as a result of different protocols, energy doses used, disease classifications, and/or different inclusion criteria.
We only irradiated the points where the patient experienced pain during palpation of the muscles during the clinical examination of the RDC/TMD. According to the data obtained in this study, the application of the laser at the points of greatest pain contributed to a significant reduction of pain in rest of muscles. This is in line with other studies. 27,29,34 –38 Gökçen-Röhlig et al. 36 in a study using an 820 nm diode laser reported a significant reduction of pain by palpation of the masticatory muscle and an increase in the pressure pain threshold. Moraes Maia et al. 37 observed a significant improvement in the pressure pain threshold only on 808 nm laser group compared with the placebo group, which remained 30 days after the treatment. Mazzetto et al. 26 observed a significant reduction on VAS values on pain related to muscle pressure in the 830 nm laser group, but not on placebo group especially after 30 days of the intervention. Demirkol et al., 29 using a 1064 nm Nd:YAG laser, have reported a significant reduction on pain muscle points after the PBM compared with the placebo group. Kulekcioglu et al. 38 observed a reduction on the laser treatment group only of pain in tender pressure muscle points.
Several studies report that PBM promoted a significant improvement in the limitation of mouth opening and masticatory function. 26 –28,30,35,36,38 Our results indicate that there was a significant improvement in the unattended painless opening for laser group with mean values higher than the reference value of the unattended painless opening (minimum of 40 mm) comparing before and after the treatment. We could suggest that this is related to the analgesic effect 22,25,31 that PBM offers permitting higher amplitude of opening movements. This is an important issue because one of the main goals of this laser treatment is pain relief. Of course, all possible causes of TMD must be addressed to promote definitive results. In addition, this treatment protocol may also be used with other treatment options.
PBM is used to stimulate cell proliferation and tissue regeneration or to modulate pain and inflammation process in cells and tissues. The biological mechanism of PBM has been described as a result of activation of several cellular cascade events, including the production of adenosine triphosphate in the mitochondrial respiratory chain and the increase of intracellular Ca++. These biological events contribute to consequent improvement of cell energy metabolism, an increase in blood supply to the tissues, the production of substances such as endorphins, and the inhibition of inflammatory mediators such as bradykinin or prostaglandins. 22,25
The photobiomodulating capacity on analgesic and anti-inflammatory effects could be related to several events. First, PBM can block off the depolarization of C-fiber afferents and acts as a stabilizing factor of the resting membrane potential, acting on the nerve endings and maintaining the analgesia period. 39 Second, PBM induces the production and release of beta-endorphins with consequent reduction of pain, and also promote a reduction in the amount of bradykinin, substance P, and prostaglandins, which leads to a decrease in inflammation and edema. Laser therapy also improves local circulation, including lymphatic and blood flow, promoting muscle relaxation in areas with muscular tension, thus promoting tissue analgesia. 22,25
Different wavelengths, energy doses, or protocols have been proposed to be effective in the management of TMD. The reported wavelengths used in PBM in TMD ranges in red to infrared spectrum and includes wavelength from 632 to 1064 nm wavelength lasers. The evidence of the ideal wavelength for these disorders is lacking. 13,22,29 Lasers in this wavelength spectrum have showed a sufficient penetration capacity although the tissues 22 with near-infrared or infrared region are described as having a higher penetration depth than a red wavelength region. 40 Nevertheless, some earlier studies specially on osteoarticular and chronic pain have reported an improvement of pain reduction outcome with the use of a red wavelength region. 41,42 In view of this, we hypothesized that this wavelength 635 nm could be beneficial and effective in pain relief in patients with painful TMD. In our sample, the 635 nm wavelength has shown to be an effective laser. To our knowledge, this is the first report of the use of this wavelength in TMD.
There is so far no evidence in the published literature for the optimal dose energy. 13 Low doses could be insufficient to promote beneficial effects and high doses could be harmful or even have a contrary effect. 22,43 The suggested fluencies applied in PBM therapy usually varies from 0.001 to 10 J/cm2 with some authors suggesting for myogenic conditions, a dose per point between 6 and 10 J/cm2. 21,44 Borges et al. 45 analyzing the effect of fluences of 8, 60, and 105 J/cm2 using an 830 nm AlGaAs laser on patients with TMD observed that only the 8 J/cm2 was capable of improving jaw movements. As observed in the present study, an energy dose of 8 J/cm2 was shown to be effective and safe in the present sample.
The number of sessions of treatment is also variable in the literature ranging from one session application 44 to 12 or more sessions distributed over several weeks. 22,35 Pain reduction has been reported between the second and fourth treatment sessions. 28,46 Moreover, it is important that this protocol should be easy and practical to use for both professionals and the patients. In view of this, we performed four sessions of treatment once a week, using 8 J/cm2 per point, observing that it was effective, but also of practical use. After the beginning of the treatment there was no loss of patients and the level of satisfaction of treated patients was very high. Moreover, in line with the majority of the studies it was safe without complications or adverse effects. 26 –29,36–38
Several studies have shown a pain reduction effect approximately at 30 days or more after the treatment. 27,29,34,37,47 We have therefore evaluated all our patients after 30 days of treatment. Moraes Maia et al., 37 in their study observed that both placebo and intervention groups experienced a reduction in pain intensity at the end of the last session, but after 30 days of treatment, this reduction was only maintained in the laser group. They also observed that the laser group showed an increase in the pressure pain threshold at the end of their treatment (p < 0.01), which remained for 30 days, but not in the placebo group. Oliveira et al., 48 showed a reduction in pain even at 6 months of follow-up. Nevertheless, showed in future studies, it would be interesting to analyze this effect for a longer follow-up period.
We acknowledge some limitations of our study such as the small number of patients recruited, short follow-up time, and the possible heterogeneous nature of our sample. Nevertheless, our sample composition, including the distribution of gender and age, is in line with reported studies. 30,34,36,37 We used the classical criteria for diagnosis of TMD, the RDC/TMD protocol, 3 although new actualization of this protocol, the new DC/TMD has been recently published. 4 However, for comparison with previous published studies we decided to use the RDC/TMD protocol. We recognize that some of our evaluation tools could be subjective such as the personal perception of pain but again they have been used in the majority of the reported studies with interesting results. Moreover, VAS scale and evaluating tenderness of muscles have been recommended by the American Dental Association (ADA). 29
Due to the expectations of patients been treated with a high-tech device, there may be interference in the results by a placebo effect. Thus, we chose to randomize the sample into two groups, one experimental and the other placebo, to guarantee the validity of the results. In this study, the power of the placebo effect was not demonstrated, since there was no significant reduction of pain, or opening jaws improvement that occurred in the laser group. This significant difference between groups showed that active laser therapy using a 635 nm wavelength diode laser was able to decrease the TMD-related pain and improve the amplitude of opening movements (without pain) in our sample.
Conclusions
The present study suggests that PBM with a 635 nm laser had a beneficial effect on the remission of painful symptoms associated with TMD, promoting also an increase in the mouth opening, and an improvement on masticatory-related pain. It has been shown to be a noninvasive therapy with no associated side effects and with a high level of patient satisfaction. More studies, evaluating protocols and comparing PBM with other forms of interventions should be undertaken to confirm the reproducibility of our data.
Footnotes
Acknowledgments
The authors would like to thank Prof. Saman Warnakulasuryia for the valuable help in the language review of this article.
Author Disclosure Statement
The authors declare that until the submission of this work there are no potential conflicts of interest and, also, no competing financial interests exist.
Ethics Approval and Informed Consent
The study was authorized by the Ethics Commission of the University Institute of Sciences of the Health (No. 11/CE-IUCS/2018). All procedures performed in this study were in accordance with the ethical standards of the same University and also with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. A full information of the study was given to all patients before obtaining an informed consent for the participation in the study. In the placebo group, a laser treatment was offered at the end of the study to the patients that still present TMD symptomatology.
Funding Information
The work was undertaken under the project LaserOral_CESPU_2018 from CESPU.