
Abstract
Objective:
To investigate effect of photobiomodulation (PBM) on nerve regeneration after neurotization with the Oberlin Procedure (ulnar fascicle to motor branch to biceps) to restore elbow flexion in patients with brachial plexus injury.
Materials and methods:
This prospective randomized controlled trial was conducted with 14 patients with high brachial plexus injury who underwent neurotization with the Oberlin Procedure to restore elbow flexion. The patients were randomly allocated to two groups of equal numbers: control group and PBM group. In this study, the PBM used has a wavelength of 808 nm, 50 mW power, continuous mode emission, 4 J/cm2 dosimetry, administered daily for 10 consecutive days, with an interval of 2 days (weekends). The outcome of surgery was assessed after 1, 2, 3, and 6 months. The nonparametric Mann–Whitney U-test and chi-square test were utilized to compare the results between both groups.
Results:
After 3 months postoperatively, more patients in the PBM group had demonstrated signs of reinnervation and the mean muscle power was significantly higher in the PBM group. No adverse effects resulted from the administration of PBM.
Conclusions:
PBM is a treatment modality that can improve nerve regeneration after neurotization with the Oberlin Procedure.
Introduction
Traumatic brachial plexus injury is a devastating injury that significantly affects a patient's quality of life and productivity. 1 Young men aged between 15 and 25 years are most commonly affected, and these injuries severely impact these patients in the most productive years of their lives. 2 Brachial plexus injury may result from high energy trauma to the upper extremity and the neck. Majority of traumatic brachial plexus injuries are caused by motor vehicle accidents and ∼70% of them involve the use of motorcycles. 3 Advances in microsurgical techniques and technology have led to better surgical outcomes in recent years. There are four major surgical techniques used to treat brachial plexus injury namely direct repair in clean nerve transections, neurolysis, nerve grafting, and neurotization. 4
Neurotization of 10% of the bulk of ulnar nerve to the motor nerve of the biceps to restore elbow flexion was first described by Oberlin in 1994, hence the name Oberlin Procedure. 5 Subsequently the technique was adopted with great success by other surgeons to treat upper brachial plexus injury. 6 –8 The timing of surgery is crucial as the neuromuscular junctions will degenerate in 20–24 months. 4 Regeneration of nerves is time consuming as the rate of axonal regeneration is estimated to be ∼1 mm/day. 9 The Oberlin Procedure has the advantage of having a short distance from the site of nerve transfer to the motor end plates. 10 Any treatment modality that can potentially accelerate nerve regeneration would be extremely beneficial for patients who have undergone neurotization.
Low level laser therapy that is now known as photobiomodulation (PBM) has been studied extensively in animal experiments and is proven to be effective in enhancing nerve regeneration after nerve repair. 11 –13 PBM has been shown to increase the functional activity of the injured nerve; 14,15 decrease scar tissue formation at site of nerve injury; 16 improve the rate of axonal growth and myelinization; 17 and increase the diameter of nerve fibers, axon diameter, and myelin sheath thickness of nerve tissue. 12,18,19 This positive effect on nerve regeneration is thought to be caused by an increase in neurotrophic factors and suppression of inflammatory process by PBM. 20 –23 PBM in the near infrared wavelength of 780–830 nm is reported to have the maximum depth of penetration through tissues with a peak penetration at 808 nm. 24 Therefore, numerous studies have demonstrated the effectiveness of PBM within this 780–830 nm range in enhancing nerve regeneration in peripheral nerve injuries in experimental animal models. 12,25 –30
However, few clinical studies are available that demonstrate the effectiveness of PBM in improving nerve regeneration in humans. 31 –33 This may explain why PBM has not been incorporated in the standard rehabilitation protocol after nerve repair and peripheral nerve procedures. Therefore, this is a very promising area of research with great potential in improving outcomes after peripheral nerve surgery with no reported side effects from PBM in any of the studies conducted.
This study aims to study the effect of PBM on nerve regeneration after neurotization with the Oberlin Procedure in patients with brachial plexus injury.
Materials and Methods
This study is a prospective randomized controlled trial that was approved by the Medical Research Ethics Committee of the University of Malaya Medical Centre (MREC ID No: 2017101-5609). The study was carried out from January 2018 to May 2019 in two tertiary hospitals that provided subspecialized hand and microsurgery treatment, which are the University of Malaya Medical Centre and Kuala Lumpur General Hospital. Sample size calculation was performed using a power and sample size calculator (G Power 3.1) and a total of 14 patients with 7 patients in each arm would give the study a power of 80%.
All patients aged between 18 and 60 years old diagnosed with upper brachial plexus injury (C5, C6) and planned for neurotization with the Oberlin Procedure to restore elbow flexion were eligible to participate in this trial. Exclusion criteria were brachial plexus injury not suitable for the Oberlin Procedure, pre-existing hand deformities or congenital abnormalities, neurological disorders, and other musculoskeletal diseases.
A total of 14 patients were recruited and they were randomized into two equal groups of equal number (seven patients per group): PBM and control groups. The randomization was performed using sealed envelopes drawn by the patients. The PBM group received PBM therapy postoperatively in addition to the standard rehabilitation protocol after the Oberlin Procedure. The control group underwent only the standard rehabilitation after operation and did not receive any PBM therapy.
The surgical technique for the Oberlin Procedure was the same for all the patients from the study and was performed by qualified senior hand surgeons. An incision was made on the medial surface of the arm, measuring ∼10 cm. The space between the biceps brachii and coracobrachialis muscles was explored to identify the motor branch to the biceps that originates from the musculocutaneous nerve. Subsequently the ulnar nerve was identified posterior to the medial intermuscular septum and an incision was made in its epineurium. The motor fascicle supplying the flexor carpi ulnaris was identified using a nerve stimulator. This one fascicle of the ulnar nerve was separated and transferred to the motor nerve to the biceps through end-to-end neurorrhaphy using monofilament Nylon 8/0 sutures reinforced with fibrin glue. The exact site of neurotization was marked with Silk sutures on the skin to facilitate pinpoint administration of PBM therapy.
In this study, the laser equipment used to administer PBM therapy was a class 1 Gallium–Arsenide (Ga-As) laser device (LaserCat500-Med Solution, Germany). The laser was directed at the site of neurotization by applying the laser beam on the overlying skin marked with a Silk suture (Fig. 1). To standardize the timing of PBM therapy for patients from both centers, PBM therapy was started on the following Monday after the surgery and it was given in 10 daily consecutive sessions, with an interval of 2 days (weekends) using 808 nm wave length, 50 mW power, and 4 J/cm2 energy density (fluence). With an irradiation area of 1 cm2 and irradiation time of 30 sec, 4 J of energy was delivered to that single point daily (Table 1). After completion of the initial PBM therapy, no additional intervention was given to the PBM group during the follow-up period.

Application of laser beam on the site of neurotization marked with Silk suture.
Parameters of the Laser Used for Photobiomodulation
Muscle power of elbow flexion and finger flexors (testing ulnar nerve function) was assessed using the Medical Research Council (MRC) muscle strength grading system. 34 The outcome was assessed at baseline (before operation) and postoperatively at 1, 2, 3, and 6 months. Muscle power of elbow flexion is the main outcome measured that indicated the recovery of elbow flexion after the Oberlin Procedure. This parameter is indirectly a measure of nerve regeneration after neurotization as nerve regeneration must reach the motor endplate from the site of neurotization to activate muscular contraction of the biceps.
Sensation in the distribution of ulnar nerve will be recorded using Medical Research Council Scale of sensory nerve dysfunction. 35 Any deterioration from baseline may indicate ulnar nerve impairment, which will be considered a morbidity after the Oberlin Procedure.
Data were collected, tabulated, and analyzed using SPSS Version 21. During statistical analysis, normality test was carried out. Subsequently, the nonparametric Mann–Whitney U-test and chi-square test were utilized to analyze the difference between the two groups (PBM and control) with a p-value of <0.05 being considered statistically significant.
Results
Fourteen patients were included in the study and there were no dropouts. The baseline characteristics of the study population are presented in Table 2. There is no significant difference between the two groups in terms of age, gender, mechanism and duration of injury, and habit of smoking. There was no significant difference in preoperative baseline clinical parameters between both groups in terms of ulnar nerve motor function (p = 0.317) and sensory function (p = 0.611). All patients were men and sustained the brachial plexus injury in motor vehicle accident. Preoperatively, all patients had an elbow flexion muscle power of MRC grade 0.
Demographic and Clinical Parameters of Control and Photobiomodulation Groups
PBM, photobiomodulation; SD, standard deviation.
There was no recovery of elbow flexion muscle power at 1 month postoperation for both groups of patients as all patients recorded MRC grade 0 for elbow flexion. No difference existed between PBM group and control group. Patients who achieved elbow flexion power of at least MRC grade 1 were considered to have demonstrated signs of reinnervation of the biceps muscle and this sign was only detected in patients after 2 months postoperation. The difference in number of patients who had signs of reinnervation between both groups was analyzed using the chi-square test. At 2 months postoperation, more patients in the PBM group showed signs of reinnervation compared with control group (Fig. 2), but the difference was not significant (p = 0.094). The mean muscle power of elbow flexion was higher in the PBM group (Table 3); however, the difference calculated using the Mann–Whitney U test was also not statistically significant (p = 0.165).

Comparison of signs of reinnervation at 2 months.
Comparison of Mean Elbow Flexion Power with Time Between Control and Photobiomodulation Groups
Mann–Whitney U test.
At 3 months postoperation, the mean muscle power of elbow flexion was significantly higher in the PBM group (p = 0.026). All patients in the PBM group demonstrated signs of reinnervation (Fig. 3) and this percentage was significantly higher than the control group (p = 0.005).
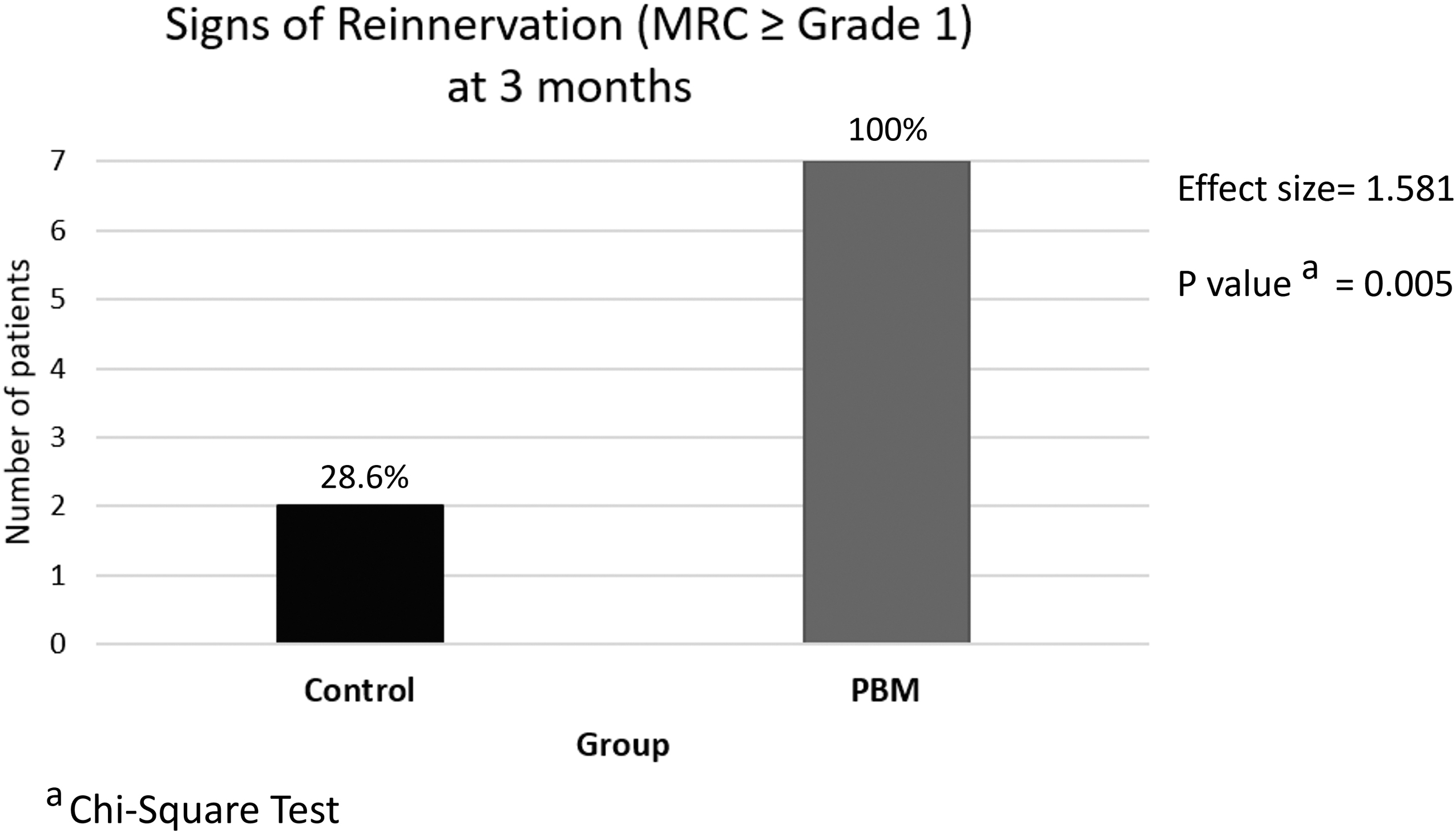
Comparison of signs of reinnervation at 3 months.
At 6 months postoperation, the mean muscle power of elbow flexion was higher in the PBM group; however, the difference was not statistically significant (p = 0.097). At that point of time, all patients in both groups had already demonstrated signs of reinnervation.
There was no change in muscle power and sensory function of the ulnar nerve (donor nerve) after the Oberlin Procedure compared with preoperative baseline in all patients. No adverse effects such as discomfort, pain, burns, or skin reactions were reported during or after administration of PBM.
Discussion
The demographic profile of the study population is similar to the findings reported by previous studies on patients with upper brachial plexus injury. 5 –8,10 All the patients in this study were men and sustained the injury in motor vehicle accidents. The average age of patients was 25 years, ranging between 18 and 34 years. The average interval between time of injury and surgery was ∼7 months.
The positive effects of PBM on nerve regeneration have been confirmed by extensive research in animal models. Rochkind's pioneering studies in the 1980s on the effect of PBM irradiation on injured peripheral nerves of rats found that PBM significantly increased the functional activity of the injured nerve over time, decreased scar tissue formation at the site of nerve injury, and improved the rate of axonal growth and myelinization. 14 –17 His study laid the foundation for further research in this field of interest. In a study using rat injury model of sciatic nerve-crushed rats, Wang et al. found sciatic-injured rats that were irradiated with 808 nm PBM had significantly improved sciatic functional index as well as increased myelin sheath thickness and growth-associated protein 43 expression levels compared with the control group. 27 This improvement in sciatic nerve function induced by PBM was also confirmed in other studies. 19,29,36 In addition, PBM therapy led to improved quantitative (myelin and blood capillary densities) and morphometric parameters (diameters of nerve fibers, axon diameter, and myelin sheath thickness) of nerve tissue. 12,18,19 The exact mechanism that brings about this improvement in nerve regeneration remains unknown, but it is widely attributed to the increase in neurotrophic factors and suppression of inflammatory process by PBM. 20 –23 This theory is supported by the study that showed that PBM increased the mRNA expression of neurotrophic factors (brain-derived neurotrophic factor and nerve growth factor) and reduced the expression of inflammatory marker (induced nitric oxide synthase) in an axonotmesis experimental model of nerve injury. 22
The wavelength of PBM is a key factor that regulates the depth and penetration of the laser irradiance in the tissue. 23 Andreo et al. reviewed studies published from 2007 to 2016 that investigated the effects of PBM on the treatment of peripheral nerve injury and found that there is a significant variability in the wavelengths used for PBM for nerve regeneration in the current literature (ranging from 632.8 to 980 nm). 36 Majority of the studies using PBM in the red spectrum utilized 660 nm, whereas studies of PBM in the infrared spectrum largely focused on the wavelength between 780 and 830 nm. The infrared irradiation is easily absorbed by tissues and loss of intensity is minimal, which allows it to exert its effect of PBM. 23,37 Byrnes et al. found that the depth of PBM penetration through Sprague–Dawley rat tissue is maximal at the near infrared region between 770 and 850 nm as compared with penetration of red light or longer infrared wavelengths up to 1200 nm. 24 In their experiment on spinal cord injury, 808 nm was chosen because it was the peak penetrating wavelength in their study. Hudson also found that 808 nm light penetrated bovine tissue samples significantly deeper than 980 nm. 38 The 808 nm was the chosen as the wavelength in this study as a maximum depth of penetration is desirable to ensure an adequate dose is achieved at the site of neurotization.
Fluences ranging from 3 to 10 J/cm2 have been reported to achieve the desired stimulation effect for peripheral nerve recovery. 23,36,37 Wang et al. compared the effects of different fluences of 3, 8, and 15 J/cm2 and noted that PBM at 3 and 8 J/cm2 accelerated recovery of nerve lesion. 27 Ziago et al. in their study that compared PBM at 4, 10, and 50 J/cm2 found that the fluence of 10 J/cm2 produced the best results for nerve regeneration. 18 Other authors have reported improved nerve regeneration at 4 J/cm2 39–41 as well as at 6 J/cm2. 20,25,26 Currently there is no conclusive evidence to show which fluence is the best for nerve regeneration. Many authors agree that future studies need to be done to determine the best treatment protocol to enhance regeneration of peripheral nerve injury. 11,23,36
The experimental model designed in this trial is established to propose a therapeutic modality that can accelerate the functional recovery of patients subjected to the Oberlin Procedure to restore elbow flexion. A thorough search of medical literature failed to find any trial that investigated the efficacy of PBM after neurotization. Therefore, the unprecedented nature of this novel trial precludes any direct comparison of our results. The clinical effect of the Oberlin Procedure in restoring elbow flexion is dependent on nerve regeneration of the motor branch to biceps brachii from the site of nerve coaptation (neurotization) to the motor end plate of the biceps brachii muscle. The Oberlin Procedure, a neurotization commonly performed in upper plexus injury with fairly predictable results, 5 –8 was chosen to test the effect of PBM on the regeneration of a pure motor nerve, thereby eliminating other confounding factors that might occur in the regeneration of a mixed motor and sensory nerve such as the median nerve that is commonly studied in other clinical studies. 31,32,42 In addition, the relatively superficial site of nerve coaptation in the Oberlin Procedure enabled to pinpoint transcutaneous irradiation with PBM.
All patients (100%) treated with PBM achieved elbow flexion of MRC grade 1 or better at 3 months postoperatively compared with 28.6% (2/7) of patients in the control group (p < 0.05). The mean muscle power of elbow flexion was also significantly higher in the PBM group (p < 0.05). This finding supports the hypothesis of the study that theorizes that PBM improves nerve regeneration after neurotization. In a randomized controlled trial conducted by Seyed Forootan et al., PBM significantly improved muscular strength of thumb abduction and opposition after median nerve repair in patients who suffered traumatic rupture of the median nerve in the distal third of the forearm. This clinical improvement was also supported by electromyography and nerve conduction studies. 31 In another study of patients with carpal tunnel syndrome subjected to surgical carpal tunnel release, PBM was shown to improve median nerve recovery evidenced by better functional results and improvement in electroneuromyographic examination. 32 This study adds to the growing body of evidence supporting PBM as a treatment modality that improves nerve recovery in the clinical setting.
At 6 months postoperation, all patients in both groups had demonstrated signs of reinnervation (at least MRC grade 1). The mean muscle power was higher in patients treated with PBM but the difference was not statistically significant. This phenomenon may be attributed to the possibility that, given an adequate amount of time, nerve regeneration in the control group has caught up with the PBM group. As long as the neuromuscular junction is not yet degenerated, reinnervation of the muscle will still be able to restore muscle contraction.
There were no side effects reported as a result of administration of PBM in this study and this finding is consistent with all previous clinical studies using PBM. 21,31 –33,42,43 Therefore, it can be concluded that PBM is a noninvasive treatment modality that can be safely administered to patients after nerve transfer or peripheral nerve repair.
The limitation of this study is the small sample size and short duration of study. Considering the fact that complete nerve healing takes at least 2 years, future studies with more patients and longer periods of follow-up can better demonstrate the effects of PBM on nerve recovery. Based on the results of this study, we recommend PBM in all patients after neurotization and microsurgical repair of peripheral nerves.
Conclusions
Based on this study, it can be concluded that PBM improves nerve regeneration after neurotization with the Oberlin Procedure to restore elbow flexion in patients with brachial plexus injury.
Footnotes
Acknowledgments
Special thanks to the staff of Rehabilitation Medicine Department of University of Malaya Medical Centre for their assistance in administration of PBM and to the Hand Unit in Kuala Lumpur General Hospital for their collaboration in this study. The authors also thank the patients who participated in this trial, without whom this study would not have been possible.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.