
Abstract
Objective:
The aim of this study was to investigate and compare the acute effects of red and infrared photobiomodulation (PBM) using a cluster device on biceps brachii muscle fatigue in young and healthy males.
Background:
Vigorous physical activity could lead to muscle fatigue, which compromises motor control and muscle strength and consequently impairs performance. The positive effects of PBM in reducing fatigue onset have been highlighted. However, the better wavelength with cluster devices is not yet established.
Methods:
A randomized double-blind session was used. Thirty-two young and healthy males were randomized into the control group (CG), red PBM group (RPG), and infrared PBM group (IPG). A PBM cluster device [7 visible diodes (630 nm), 7 infrared diodes (850 nm), 100 mW/diode, 2 W/cm2 power density, 91 J/cm2 energy density, 4 J per point, 28 J total energy, and 40 sec] was applied after muscle fatigue. Muscle fatigue was analyzed by surface electromyography (EMG) recorded from the long head of biceps brachii, blood lactate concentration, and evaluation of the rate of perceived exertion (RPE) using the Borg Scale. The fatigue protocol consisted of a maximum voluntary isotonic contraction of elbow flexion–extension with 75% of one-repetition maximum until exhaustion. The Borg Scale was applied before and at the end of the experiment to measure the RPE. The electromyography fatigue index (EMGFI) was calculated by windows of median frequency from EMG data.
Results:
EMGFI, blood lactate concentration, and RPE showed no intergroup statistical difference, except the EMGFI delta value that showed a difference between IPG and CG, with a greater value in the CG. However, intragroup comparisons showed that EMGFI decreased in the CG and RPE and lactate concentration increased significantly in all groups.
Conclusions:
There was no difference between red and infrared PBM in reduction of biceps brachii fatigue. However, the EMGFI delta value was greater in the IPG compared with the CG, suggesting that infrared can be more effective in reducing biceps brachii fatigue.
Introduction
Muscle fatigue is characterized by decline in the ability that a muscle has to generate force during prolonged or repeated muscle activity. 1 It can occur by decrease in the nerve capability of generating a sustained neural signal (neural fatigue), by reduction in the ability of muscle fiber contraction (metabolic fatigue), and by decrease in blood perfusion and available energy. 2,3 This leads to a decrease in muscle strength, which influences execution of movements, training performance, motor control impairment, muscle pain, and musculoskeletal disorders. 3 –7 Biceps brachii is an important muscle in elbow flexion and it has a high impact on sports performance and activities of daily living. Thus, to prevent fatigue in biceps brachii, it is important to enhance muscle performance during exercise or athletic performance.
Due to the effects that low-level laser therapy (LLLT) and light-emitting diode therapy (LEDT) have in reducing fatigue markers during physical exercise, 8 –16 photobiomodulation (PBM) is suggested to maintain the ability that a muscle has to generate force during exercise or other physical activity by recovering muscle fatigue. From a practical standpoint, PBM shows positive effects in delayed fatigue onset 17 by reducing levels of inflammatory markers, such as creatine kinase (CK) and lactate dehydrogenase, and by reducing levels of blood lactate. 16,18 Then, electromyography (EMG) has been pointed out as an efficient tool to elucidate the effects of PBM on muscle recovery. 18,19
PBM seems to induce photochemical and photophysical effects in cells through absorption of light by mitochondrial photoreceptors, 20 increasing the cellular synthesis of adenosine triphosphate, RNA, proteins, and enzymes. 21,22 The magnitude of these events could be influenced by the choice of wavelength, fluency, power density, and absorption spectrum of the photoreceptor. 23,24 In the case of wavelengths, it is known that infrared radiation penetrates better than red radiation into the human skin. 25 However, de Almeida et al. 13 observed similar effects of both wavelengths in delaying musculoskeletal fatigue. PBM could be delivered by pen or cluster devices. To date, there is no consensus about which device and which parameters are better to improve muscle performance by reducing muscle fatigue.
The cluster device covers a greater muscle area when compared with pen device radiation. 26 Additionally, the cluster device seems to be more effective in clinical settings for reducing muscle fatigue. 19,27 However, there are few studies related to the upper extremity compared with the lower extremity. 18 In this context, we designed this research to assist in the understanding of using PBM for reducing fatigue in the upper extremity muscle.
Based on the importance of investigating different PBM wavelengths in upper extremity muscles associated with the fact that PBM would have an optimized effect when tissues present oxidative stress, 28 we designed this study. The aim of this study was to investigate and compare the effects of red and infrared PBM on delaying biceps brachii fatigue in young healthy males. We expected that the red wavelength would be more effective in reducing muscle fatigue and for having more interactions with superficial and vascularized tissues. 24 Thus, results of this study would assist in identifying a wavelength that could lead to greater improvement of muscle performance by delaying muscle fatigue.
Methods
Subjects
Procedures were approved by the Ethics Committee of the Federal University of São Paulo (Approval Number 188.666). All subjects were informed of the purpose and procedures of the study and signed an informed consent form before their participation in the experiment.
Inclusion criteria
Subjects included were male, aged 18 to 25 years, clinically healthy, and classified as active (who performed a physical activity with a frequency of at least five times a week, totaling a minimum of 150 min/week according to criteria), established by The American College of Sports Medicine and measured by the International Physical Activity Questionnaire–Short Version (IPAQ). In this questionnaire, the subject needs to describe how many days/week and hours/day he spends in walking or moderate- and vigorous-intensity activities. 29
Exclusion criteria
Those with previous musculoskeletal injury or recent pain complaints in the dominant upper limb and shoulder girdle and positive tests for shoulder, elbow, wrist, and finger injuries were excluded.
Experimental procedures
The experimental procedures comprised two sessions. The first session included anamneses, physical evaluation, IPAQ, and the one-repetition maximum (1-RM) test.
Forty-eight hours after 1-RM determination, the second session procedures were performed before and after the fatigue protocol. Before the fatigue protocol, a baseline blood sample was collected, followed by the first surface EMG data acquisition. Then, the Borg Scale was applied and shortly after, muscle fatigue was assessed until subject's exhaustion. Immediately after the fatigue protocol, PBM was applied to the biceps brachii during a period of 40s, according to randomization. In the sequence, EMG data were collected again, followed by the second blood sample collection. Three more blood samples were collected after 3, 6, and 9 min. At the end of the procedures, the Borg Scale was applied again. Details of experimental procedures are described in the Methods section.
Proper attention was paid to ensure the standardization of procedures. Subjects performed all sessions in the standard position on a Scott bench and for the same period in the day. Additionally, each subject performed the muscle fatigue protocol with load defined in 75% of his 1-RM test. Sessions are detailed in Fig. 1.

Experimental procedures.
Design
This study is a double-blinded, randomized controlled trial. Subjects were randomized into groups to compare the outcomes of red or infrared PBM on delaying muscle fatigue onset. Sample size calculation was performed using the GPower 3.0.10 program with the following parameters: effect size of 0.25, power observed of 0.80, and α = 5%, considering the analysis of variance (ANOVA) model for three groups. Sample size obtained was 36 subjects randomly allocated into control, red, or infrared PBM groups by simple drawing of lots, which determined whether they should receive PBM or not, as follows:
Control group (CG): participants who did not receive PBM.
Red PBM group (RPG): participants who received PBM, red LED (630 nm), after the fatigue protocol.
Infrared PBM group (IPG): participants who received PBM, infrared LASER (850 nm), after the fatigue protocol.
Randomization
Randomization was performed through a computer program that created a random table of numbers that allocated participants in the CG, RPG, or IPG. Researcher (1) was responsible for sealing the envelopes and for setting the PBM before procedure. She was instructed to not communicate with subjects and any other researcher about group allocation. Researcher (2) was responsible for data analysis. Moreover, subjects and researcher (2) wore opaque goggles during PBM, which helped to blind the PBM wavelength.
Determination of 1-RM
The 1-RM was obtained with the participant seated on the Scott bench, and weights were used to find the participant's maximum load lifted in just one repetition, used to determine the participant's maximum strength. Before the 1-RM test, all participants were familiarized with procedures. The 1-RM test was determined by a maximum of five sets of one repitition until the participants were unable to perform a proper lift and complete range of motion. An integral with 3–5 min of rest between attempts was oriented. If 1-RM was not determined between the five sets, the test was rescheduled to avoid muscle fatigue influence. All procedures were based on the American College of Sports Medicine Guidelines. 30
Fatigue protocol
The fatigue protocol followed the design by Leal et al., 25 which evaluates the individual's ability to perform voluntary isotonic contractions of elbow flexion–extension with a load of 75% of 1-RM until exhaustion. The protocol was performed with the participant on the Scott bench and with both upper extremities. The load of exercise was individualized for each participant and all subjects were oriented to perform elbow flexion–extension, with movement starting from full elbow extension to full elbow flexion, not too abruptly or too slowly.
PBM protocol
The cluster device (DMC™ Equipment Ltda, São Carlos, Brazil) comprised 14 diodes, seven light-emitting diodes (LEDs) with visible wavelengths of 660 nm and 7 diodes (LLLT) with infrared wavelengths of 808 nm. It is important to highlight that the equipment allows the use of only one isolated wavelength or both wavelengths concomitantly. PBM was performed immediately after the fatigue protocol. Only cables of the electrode were removed to deliver PBM. We decided not to remove the electrode because it could cause detrimental delay in applying PBM over the muscle. The cluster device was positioned 2 cm above the elbow joint line guided by the skin marked before the beginning of the experiment, covering the biceps brachii surface of the dominant upper limb (Fig. 2). Forty seconds of PBM was necessary to deliver PBM according to selected parameters (Table 1).

PBM application on the biceps brachii surface. PBM, photobiomodulation.
Irradiation Parameters
LEDs, light-emitting diodes; LLLT, low-level laser therapy.
Electromyography
The surface EMG signal was sampled using a 16-bit A/D converter board, with a 2 kHz frequency (Miotec™, Brazil). For capturing the surface myoelectric signal, a disposable bipolar electrode (Ag/AgCl, 20 mm interelectrode distance) connected to a sensor with input impedance of 10 GΩ, common mode rejection ratio of 130 dB, and gain of 20 times (Miotec) was used. A circular disposable electrode was attached to the sternal notch for reducing acquisition noise.
The skin at the electrode's site was shaved and cleaned with alcohol before attachment of the electrode to reduce skin impedance and to achieve good fixation. The electrode was placed on the line between the medial acromion and the fossa cubit at one-third the distance from the fossa cubit. All procedures were realized according to Surface Electromyography for Non-Invasive Assessment of Muscles–SENIAM. 31
The electrode was placed only on the dominant arm (reported by the participant) as described above. Then, each participant performed 30 sec of biceps brachii maximum isometric contractions (MICs) on the Scott bench before the fatigue protocol and another 30 sec of biceps brachii MICs immediately after PBM application. Participants performed MICs with both arms in the neutral position for rotation, 90° of elbow flexion, and forearms in supination. Researcher (2) ensured that participants were applying maximal and constant effort while performing MICs and with no compensation. If the participant did not follow the requirements mentioned above, the protocol would be suspended and a new protocol would start after 30 min. However, participants presented no compensation.
Blood sample collection
Lactate was collected from the region of the earlobe using a disposable lancet as follows: at baseline, immediately after second EMG data collection, and 3, 6, and 9 min after second EMG data collection. The first drop of blood was discarded to avoid contamination and then 25 μL of blood was collected using a calibrated, heparinized glass capillary tube. Blood samples were placed in tubes containing 50 μL of 1% sodium fluoride to prevent continued glycolysis and stored in a freezer at −10°C for further analysis. 32
Evaluation of the rate of perceived exertion
The Borg Scale has a 0–10 score and is a simple method to evaluate the rate of perceived exertion (RPE), for instance, in a session of exercise, fatigue protocol, estimation of exercise load, and in submaximal or maximal efforts. 7 Thus, we used this tool in our study since fatigue is an important issue in our protocol. Before the fatigue protocol, the subject was asked to look at the scale and point out his RPE. At the end of the session, the subject was again asked to point out the scale.
Data analyses
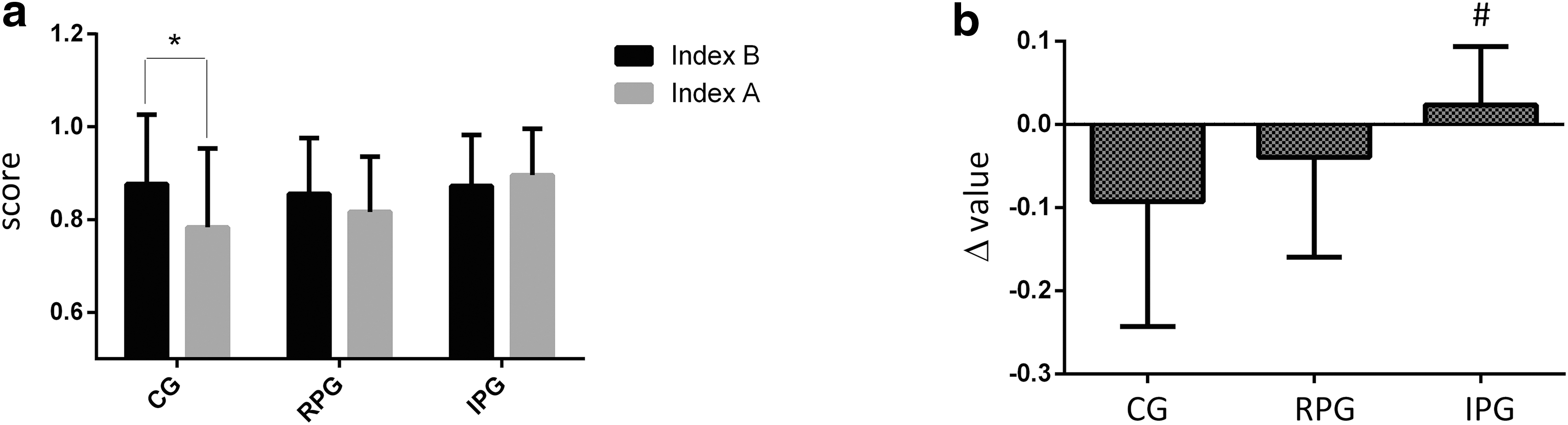
EMG digital signal processing was done using Myograph software (Miotec). Raw EMG was digitally filtered at a frequency bandwidth of 20–1000 Hz, and the median frequency (MDF) of the signal was used for data analysis. EMG signals sampled during 30-sec MCIVs in the second session were used to analyze electromyographic fatigue of biceps brachii before and after the fatigue protocol. Electromyographic fatigue was determined by the electromyography fatigue index (EMGFI). To determine EMGFI, 30-sec MICs were divided into three windows of 10 sec each, but only the initial and final windows were used to calculate the index. The first window (window i) corresponds to the value obtained from the beginning of the signal (0–10 sec) and the final window (window f) corresponds to the ending of the signal (20–30 sec). For ease of interpretation, initial and final windows obtained before (B) the fatigue protocol were named as Bi and Bf and after (A) the fatigue protocol as Ai and Af, respectively.
To obtain EMGFI before the fatigue protocol (named Index B), window Bf was divided by window Bi, and to obtain EMGFI after the fatigue protocol (named Index A), window Af was divided by window Ai. Thus, normalization of signals was done through this division. Index B and Index A were used in posterior intra- and intergroup comparisons.
The analyses of blood samples were performed using a YSI 1500 Sport Lactate Analyzer (YSI, Inc., USA), which was calibrated according to the manufacturer's instructions. 32
Values of RPE were compared between inter- and intragroups. 7 Intragroup comparison was done among values obtained before and after the procedure. Intergroup comparisons were done to analyze the possible differences among groups before and after procedures.
Statistical analysis
To evaluate intra- and intergroup comparisons of EMGFI (Index A and Index B), RPE, and lactate concentration variables, the two-way ANOVA model was used, followed by the Duncan post hoc test. To evaluate the intergroup effect of the magnitude of intervention, delta values (Δ) were used for statistical analysis. Delta values (Δ) were obtained for variables through the calculation [Δ = (after value – before value)] to make sure that follow-up differences, if any, truly result from the protocol intervention. The significance level was set at 5%.
Results
Thirty-six subjects were selected according to our inclusion criteria. Four subjects were excluded because they did not finish procedures. Thus, the final sample size was 32 subjects. Similar values were found between the groups for the variables, age, height, body mass, and body–mass index (Table 2).
Means and Standard Deviations of Anthropometric Characteristic Values
Values are mean ± SD.
BMI, body–mass index; CG, control group; IPG, infrared PBM group; RPG, red PBM group; SD, standard deviation.
Results showed greater values of Index B compared with Index A in the CG (p = 0.024), indicating that subjects showed more EMG fatigue after the procedure (Fig. 3a). Additionally, delta values were greater in the CG compared with the IPG (p = 0.04) (Fig. 3b).
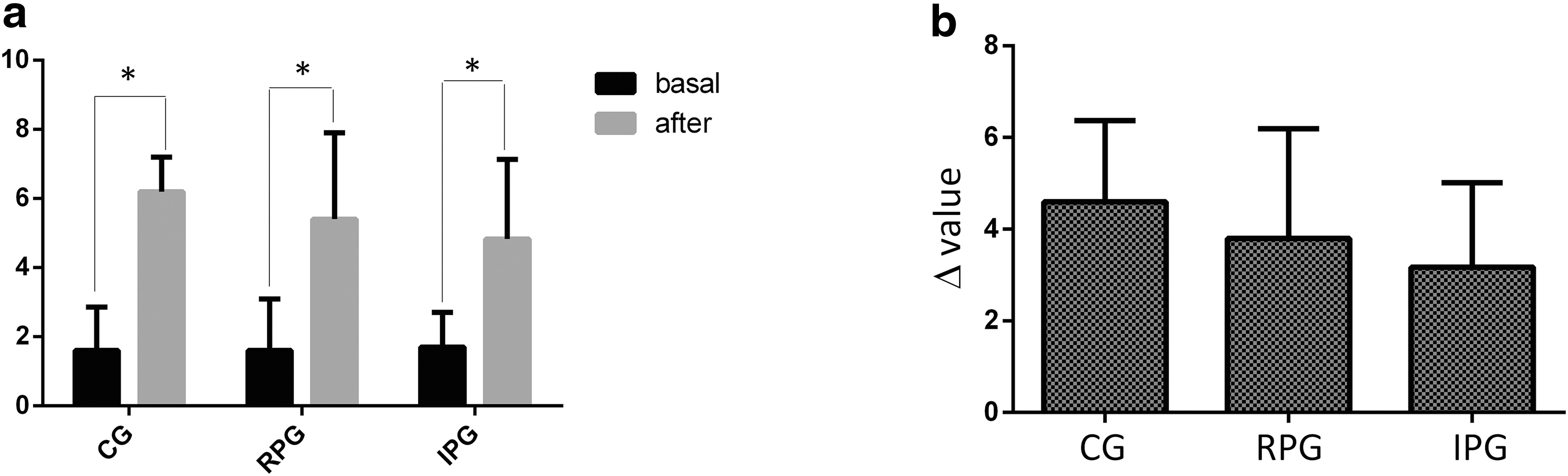
There were significant differences in the intragroup comparisons for all measurements of lactate (p ≤ 0.05) (Fig. 4). Additionally, results showed greater values of RPE after the procedure in all intragroup comparisons (CG p = 0.00002; RGP p = 0.00005; and IPG p = 0.0001), and RPE (p > 0.05) and delta (p > 0.05) values did not show significant differences in intergroup comparisons (Fig. 5a, b).
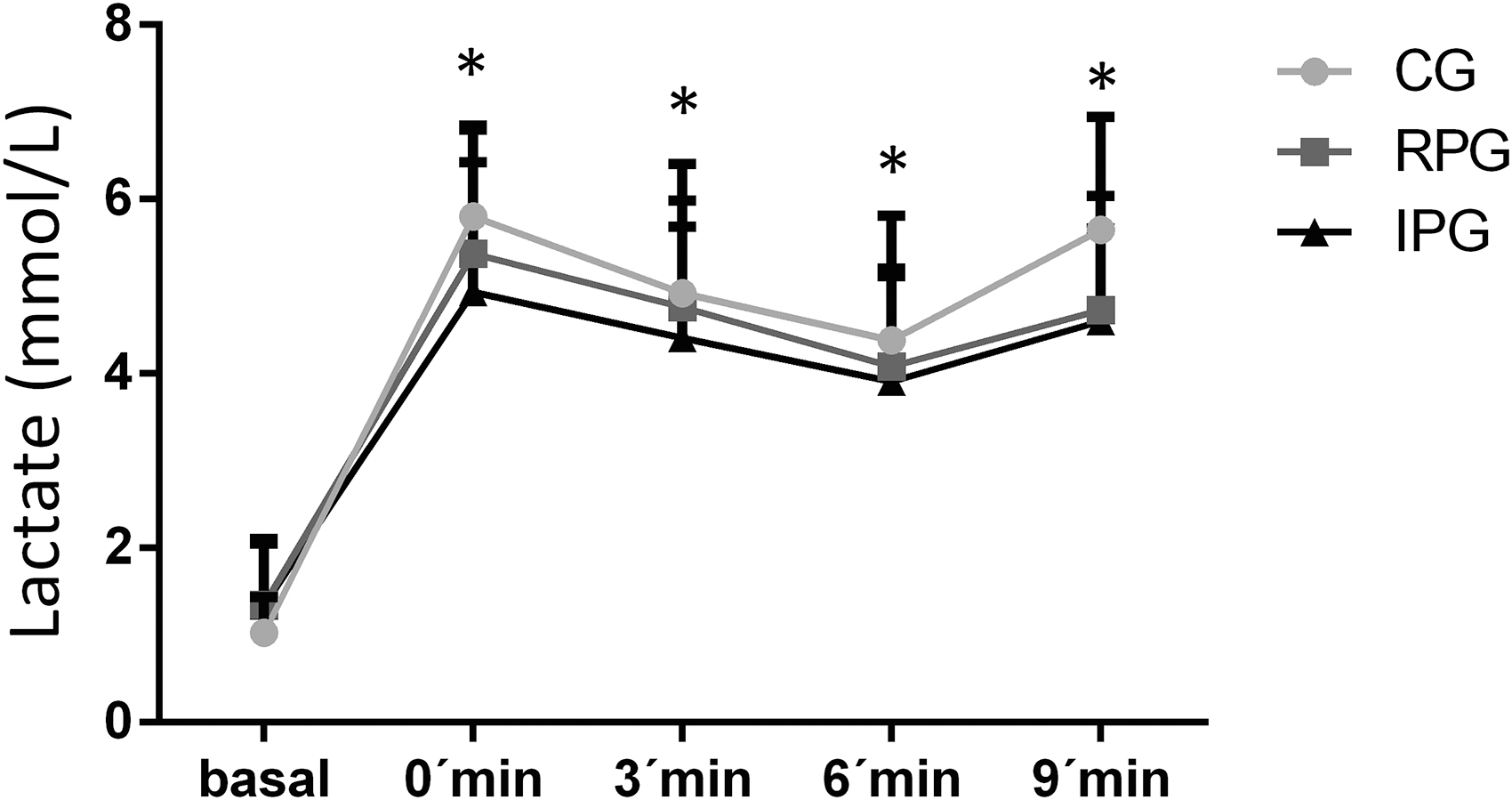
Means and standard deviations of lactate concentration. *Statistical difference of basal condition for the same group.
Discussion
This study investigated and compared the effects of red and infrared PBM on delaying biceps brachii fatigue. The hypothesis of this study was not confirmed since the results showed no significant differences when variables were compared between RPG and IPG. However, the delta value of EMGFI was higher in the IPG compared with the CG.
In our study, all groups showed greater values of the lactate concentration compared with the baseline. Additionally, all groups showed significantly greater values of RPE after the fatigue protocol. These findings demonstrate that the protocol was effective in inducing muscle fatigue. However, PBM groups showed no difference in lactate concentration compared with the CG, not corroborating with researchers who observed increased lactate removal due to microcirculation improvement caused by PBM. 11,13,16,32
PBM delivered by cluster devices has shown effectiveness in reducing muscle fatigue and inflammatory markers and improving muscle performance. 17 Blood lactate concentration reduced when PBM was delivered to the biceps brachii of volleyball players using the cluster device with combined wavelengths (red and infrared) 9 and cluster device only with the infrared wavelength. 25 However, those studies delivered PBM before the fatigue protocol, while we delivered PBM after the protocol. Thus, differences in procedures could justify differences between results. Considering irradiation using a pen device, our results agree with the research that observed no reduction in the level of lactate between PBM and placebo groups. 9,25,33,34 It is important to note that the PBM cluster device has been effective in studies involving other muscles. 15
Besides, the CG showed no increases in lactate concentration after the fatigue protocol compared with RPG and IPG, only the CG showed a significantly greater Index B compared with Index A of EMGFI. The increase in lactate concentration causes intracellular acidification after muscle fatigue, which could alter the speed of action potential propagation along the sarcolemma, 35 an alteration in the cellular environment that has a direct influence on electromyographic fatigue. Thus, a possible justification for the lack of agreement in fatigue indexes between studies is that PBM parameters chosen in this research could not be effective in reducing muscle fatigue. Moreover, selected muscles and fatigue protocols, as well as the time of PBM application (most studies were performed before muscle fatigue), 9,18,25 are important issues to be considered as justification for the absence of agreement between studies.
Nevertheless, considering the EMG results, the PBM delivered after biceps brachii fatigue showed an increase in MDF, while Rossato et al. showed no changes in MDF when PBM is delivered before biceps brachii fatigue. Thus, in this study, the EMGFI delta value was significantly greater in the IPG compared with CG, suggesting that the infrared wavelength can be effective in reducing biceps brachii fatigue. It is known that the infrared radiation is more absorbed by deeper tissues, while the red wavelength has more interaction with superficial and vascularized tissues. 24 This result corroborates with a study in the literature that applied PBM (780 nm, 30 mW, and 0.81 J/point) before an exhaustion protocol using isotonic contractions of the tibialis anterior muscle and observed a decrease in muscle fatigue using EMG. 15 It can be supposed that infrared PBM may have modulated the mitochondrial activity, increasing cellular synthesis of adenosine triphosphate and improving sodium, potassium, and calcium channels of muscle. 11 This finding indicates that infrared PBM could be more effective compared with the red wavelength, although it is relevant to note that there was no significant difference in the delta value between RPG and IPG. Thus, these data need to be further explored in future studies.
PBM is capable of reducing the level of inflammatory markers in subjects submitted to fatigue of biceps brachii. De Marchi et al. 12 observed lower concentrations of biochemical markers and CK in the PBM group compared with the placebo group. Felismino et al. 36 observed that infrared PBM attenuated CK concentration after the biceps brachii fatigue protocol. Moreover, studies suggested that infrared PBM and red PBM were able to increase the peak of torque and muscle performance. 16,19
This study has strengths. There is no consensus yet about which wavelength is more effective in reducing muscle fatigue. Moreover, clusters are attaining visibility in clinics since they deliver many outputs for PBM simultaneously. Thus, our results help in understanding which wavelength is more effective in this field of research. Additionally, we delivered PBM just in one muscle, which helped us to observe better fatigue since we did not combine different anatomical or physiological aspects of muscle structure.
However, this study has limitations. The major limitation refers to the lack of a placebo group. Additionally, we did not measure force or torque. Last, collecting inflammatory markers and more blood samples over time is desirable to understand how long PBM effects last in the muscle tissue, improving knowledge about muscle fatigue and muscle performance improvement.
Conclusions
There was no difference between red and infrared PBM in reduction of biceps brachii fatigue. However, the EMGFI delta value was greater in the IPG compared with the CG, suggesting that infrared PBM can be more effective in reducing biceps brachii fatigue.
Footnotes
Acknowledgment
The authors thank Prof. Hanna Karen Moreira Antunes from the Biosciences Department, Federal University of São Paulo, Brazil.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding received for this study.