
Abstract
Objective:
This study aimed to evaluate the efficacy of laser-activated irrigation using photon-induced photoacoustic streaming (PIPS®) and photoactivated disinfection (PAD) techniques and their combination to improve penetration and activation of toluidine blue in the endodontic space of teeth experimentally infected with Enterococcus faecalis.
Materials and methods:
Twenty-seven extracted single-root teeth were instrumented, sterilized, and infected with E. faecalis and divided into seven groups of three teeth each: Group A [sodium hypochlorite (NaClO) 5% hand irrigation], Group B [NaClO 5% hand irrigation+ethylenediaminetetraacetic acid (EDTA)+NaClO 5% activated by PIPS], Group C (EDTA+NaClO 5% activated by PIPS), Group D (toluidine blue activated by PAD), Group E (toluidine blue activated by PIPS and PAD), Group F (NaClO 5% hand irrigation+toluidine blue activated by PAD), and Group G (NaClO 5% hand irrigation+toluidine blue activated by PIPS and PAD). Finally, positive and negative group controls were prepared. The presence of biofilms after the treatments was assessed by the BioTimer assay. PIPS was performed with an Er:YAG laser (2940 nm, LightWalker, Fotona® d.o.o., Slovenia) at 20 mJ, 15 Hz, 0.3 W, and 50-μs pulse duration. PAD was performed with a 635 nm diode laser (Smart M, Lasotronix®, Poland) at 400 mW in continuous wave (CW).
Results:
When NaClO was used, significant decontamination (p ≤ 0.05) was obtained in all experimental groups with respect to the positive control, other than Group G. Irrigation with EDTA+NaClO activated by PIPS produced a higher level of decontamination than Group A (p ≤ 0.05). Significant results in reducing biofilm load compared with the control and Group A were observed when NaClO was coupled with toluidine blue activated by PAD (p ≤ 0.05).
Conclusions:
Disinfection of root canals can be obtained using a combination of different irrigants, photosensitizers, and activation protocols. EDTA+NaClO using the PIPS protocol and toluidine blue activated by PAD (both preceded by NaClO irrigation) can be considered effective tools. The possibility of replacing NaClO with toluidine blue, whatever the method of activation, should be further investigated.
Introduction
The endodontic treatment consists of shaping and cleaning the root canals, removing organic and inorganic tissues, reducing the microbial load, and preventing reinfection by a tridimensional root canal filling. Nevertheless, endodontic treatment can fail 1 because of anatomical difficulties in achieving full decontamination of the endodontic space and the irrigant limitation of the ability to deeply penetrate the dentinal walls. Indeed, endodontic irrigants are the most important weapons to kill microorganisms that are organized in both planktonic form and biofilms adherent to walls of dentinal tubules. 2 –4
However, complete sterilization of the root canal is a difficult goal to be achieved by conventional procedures 5 because of three main factors: the complex anatomical structure of the endodontium, the biofilm lifestyle of colonizing bacteria, and the difficulty for irrigating solutions to penetrate deep into dentinal tubules up to the apical portion of root canals. 6
Endodontic pathogens can penetrate the dentinal tubules even up to 1 mm, while irrigating solutions reach a depth of about 130 μm (Refs. 7,8 ). Moreover, the small size of lateral canals and of the apical terminus and the high surface tension of endodontic irrigants make it difficult to achieve deep decontamination of this area.
Laser technology has been proposed in endodontics to improve root canal disinfection procedures. Many wavelengths could be used as additional devices in root canal disinfection. 9 –12
Specifically, diode and Nd:YAG lasers have bactericidal properties related to the photothermal effect and to their capability to deeply penetrate into dentinal tubules due to prevalent diffusion of these wavelengths. 9,11,13 –16 However, the fiber of the laser is often not flexible enough to reach the apex of a slightly curved root canal, therefore these techniques can be often used only in large and straight canals with huge preparation to permit insertion of the fiber of 200 μm up to 1 mm from the apex. When more flexible fibers are used, a mechanical preparation is still necessary, with diode and Nd:YAG lasers, for insertion until the apical space. Moreover, when lasers are used in dry canals and touch the dentin surface, near-infrared wavelengths could burn the dentinal walls causing morphological damages, the smear layer is only partially removed, and dentinal tubules are primarily closed through melting of inorganic dentinal structures. 17 –20 Mid-infrared lasers could not only completely vaporize the smear layer but they could also produce a superficial thermal phenomenon on the dentin in a straight canal because of the movement of the optical fiber that collides with the dentinal walls. 21 –25 When medium infrared wavelengths are used in curved and/or narrow root canals, they could cause ablation spots along dentin walls, perforation, and apical transportation in the apical area. 26,27
Hence, several studies investigated nonthermal laser methods for root canal decontamination, such as photoactivated disinfection (PAD) or photon-induced photoacoustic streaming (PIPS®). Both the methods do not consider direct irradiation of the root canal, but rather low-power irradiation/activation of the irrigant solutions used, without having a direct thermal impact on dentin walls.
The PIPS technique activates commonly used endodontic irrigant solutions, such as NaOCl, distilled water, and ethylenediaminetetraacetic acid (EDTA), with a specific Er:YAG laser, a conical and stripped tip, and subablative parameters. The activation occurs suddenly due to high absorption of the Er:YAG laser in water. The Er:YAG laser emits an infrared light with a wavelength of 2940 nm. The wavelength of the Er:YAG laser is more strongly absorbed by water than those of the diode, potassium titanyl phosphate (KTP), and Nd:YAG lasers due to the atomic resonance. Further, the Er:YAG laser is a solid-state laser whose lasing medium is an erbium crystal doped with yttrium aluminum garnet. The Er:YAG laser light can effectively cut soft and hard tissues, so it can be used in all fields of dentistry. When subablative energy (20 mJ at 15 Hz) is delivered with supershort pulses (SSPs; of 50-μs duration), photoacoustic and photomechanical effects are produced, creating a shock wave phenomenon leading to formation of powerful streaming of fluids inside the root canal. 28
The concept of PAD is the use of a specific nontoxic photosensitizer and its selective activation by specific laser wavelength irradiation. The photosensitizer solution, previously inoculated in the canal through a syringe, will color the substrate and will attach to bacterial cell membranes; the selective laser wavelength irradiation will activate the photosensitizer, leading to production of reactive oxygen species, such as singlet oxygen, which causes the rupture and lysis of bacterial cells and their death. 29,30
In this pilot study, two different lasers have been used: an Er:YAG laser (2940 nm) and a diode laser (635 nm). Considering the relevance of the nontoxicity of the photosensitizer, the purpose was to compare an established technique such as PIPS with PAD and try to improve the efficacy of PAD by combining the two techniques.
Objective
The aim of this in vitro study was to evaluate the efficacy of laser techniques such as PIPS and PAD protocols and the combination of these two technologies. In the combined protocol, toluidine blue was used as photosensitizer and activated by PIPS technology to push and stream it in the endodontic space.
Materials and Methods
A total of 27 single-root, single-canal, and not-decayed teeth, with curvatures of <10° such as mature roots, the absence of root filling materials, calcium metamorphosis, and root resorption, extracted for periodontal or orthodontic reasons, were selected. Patients were informed about the experiments carried out using their teeth and they signed their consent. All interventions were performed by the same specialist and conducted according to and by passing the online examination for the Certificate in Essential Good Clinical Practice (GCP; Certificate number: EGCP19/3015) and following the guidelines of the World Medical Association Declaration of Helsinki according to the local Ethics Committee. All decontamination protocols were performed in a private office and all the specimens were transported in ice immediately after to the department of microbiological science.
During the transfer, samples were placed in containers suitable for transport of biological material.
Preliminary preparation of teeth
All specimens were preliminarily prepared, up to apical constriction, with rotary Ni-Ti instruments up to ISO 0.20/0.07 v (F1, ProTaper Gold®; Dentsply Sirona) using hand irrigation with NaOCl 5%, saline solution, and EDTA 17% between each instrumentation step. The anatomic apex was sealed using an adhesive procedure and composite resin, and then all the specimens were sterilized in the autoclave (121°C/15 min).
Experimental infection of prepared teeth
Enterococcus faecalis (ATCC 29212) was streaked onto a Columbia agar (sheep blood 5%) plate (Oxoid Thermo Fisher Scientific, USA) to check strain purity. To prepare the inoculum for tooth contamination, ten colonies of E. faecalis were cultured in 5 mL of brain–heart infusion (BHI) broth with added glucose (Oxoid Thermo Fisher Scientific) for 2 h at 37°C to reach the logarithmic phase of growth. The bacterial suspension obtained was adjusted to the optical density (OD) equal to 0.5 on the McFarland scale, containing ∼107 colony forming units (CFUs)/mL. The teeth were placed in 1.5-mL volume Eppendorf vials and 10 μL of a 1:10 dilution of the bacterial suspension was used to inoculate each root canal through sterile syringes. Inoculated teeth were incubated for 48 h at 37°C in the upright position to avoid contamination of the external surfaces of the teeth. As reported, in these experimental conditions, E. faecalis formed biofilms on the root walls. 31
Treatments of experimentally infected teeth
After incubation, teeth infected with E. faecalis biofilms were randomly divided into seven groups, each consisting of three teeth: Group A: teeth were irrigated with sodium hypochlorite (NaClO) hand irrigation; Group B: teeth were first irrigated with NaClO hand irrigation, followed by irrigation with EDTA+NaClO activated by PIPS; Group C: teeth were irrigated with EDTA+NaClO activated by PIPS; Group D: teeth were irrigated with toluidine blue activated by PAD; Group E: teeth were irrigated with toluidine blue activated by PIPS and PAD; Group F: teeth were first irrigated with NaClO hand irrigation, followed by irrigation with toluidine blue activated by PAD; Group G: teeth were irrigated with both NaClO hand irrigation+toluidine blue activated by PIPS and PAD.
In addition to the above-described seven groups, positive and negative group controls were prepared as follows:
Positive control group: three teeth, inoculated with the E. faecalis suspension, were untreated.
Negative control group: three teeth were inoculated with 10 μL of sterile BHI.
The PIPS protocol was performed with the Er:YAG laser (2940 nm, LightWalker, Fotona d.o.o., Slovenia) using a PIPS tip (12 mm long, 400 μm diameter). Er:YAG laser parameters were 20 mJ, 15 Hz, 0.30 W, and 50-μs pulse duration (SSP), with air/water spray off (Figs. 1 and 2).

Position of the PIPS® tip in the access cavity. PIPS, photon-induced photoacoustic streaming.

Laser parameters during the PIPS protocol; 15 Hz–0.30 W SSP 50 μsec. No water, no air. SSP, super short pulse.
The PAD protocol was performed with a diode laser (635 nm, Smart M; Lasotronix, Poland) using a special, transparent, plastic endodontic tip. The parameter was 400 mW emitted in continuous wave (CW). The toluidine blue solution used was the PAD SMART SOLUTION Endo Liquid (Denfotex Research Ltd., London, UK; Figs. 3 and 4).

Experimental PAD protocol. PAD, photoactivated disinfection.

Laser parameters during the PAD protocol.
The treatments of the groups were as follows:
Group A: the samples were treated with hand irrigation of 5 mL NaClO 5% for 30 sec; after irrigation, the liquid was immediately removed with distilled water (3 mL).
Group B: the samples were first treated with hand irrigation of 5 mL NaClO 5% for 30 sec; after irrigation, the liquid was immediately removed with distilled water (3 mL). Then, the teeth were first treated with two cycles of 17% EDTA (3 mL; EDTA Ogna, Italy) irrigation, delivered with a hand syringe, and simultaneously activated by Er:YAG laser for 30 sec each. Another 30 sec of resting time followed each activation cycle of the irrigant. A 30-sec irrigation cycle with distilled water (3 mL) activated by the Er:YAG laser was performed after EDTA irrigation to wash out the solution and avoid any chemical reaction with the following irrigant solution used. Then, 3 cycles of 5% NaClO (3 mL; Niclor 5, Ogna, Italy) irrigation were delivered with a hand syringe and simultaneously activated by the Er:YAG laser for 30 sec each, followed by 30 sec of resting time. A final 30-sec irrigation cycle with distilled water (3 mL) activated by the Er:YAG laser (2940 nm) was performed to wash out the solution from the canal.
Group C: teeth were treated as in Group B, without the preliminary hand irrigation of 5 mL NaClO.
Group D: a total of 1 mL of toluidine blue solution (PAD SMART SOLUTION Endo Liquid; Denfotex Research Ltd.) was introduced into the canal with a syringe. After 5 min, excess dye was removed through a suction cannula and the toluidine blue solution was activated by two cycles of diode laser (635 nm) irradiation for 30 sec each, followed by 30 sec of resting time. A final 30-sec hand irrigation with distilled water (5 mL) to wash out the dye was performed.
Group E: the treatment consists of 1 cycle of irrigation with toluidine blue solution activated by the Er:YAG laser for 30 sec. After 5 min, excess dye was removed through a suction cannula and then toluidine blue was activated by two cycles of diode laser (635 nm) irradiation for 30 sec each, followed by 30 sec of resting time. A final 30-sec hand irrigation with distilled water (5 mL) was performed to wash out the dye.
Group F: teeth were first treated with hand irrigation of 5 mL NaClO 5% for 30 sec, immediately removed with distilled water (3 mL), and then treated in the same way as Group D.
Group G: samples were first treated with hand irrigation of 5 mL NaClO 5% for 30 sec, immediately removed with distilled water (3 mL), and then treated in the same way as Group E.
Evaluation of biofilms on the inner walls of experimentally infected teeth
To quantitatively evaluate the biofilm present on the walls of root canals, the BioTimer assay (BTA) was employed. BTA measures bacterial metabolism and employs the Phenol Red-BTA (PR-BTA) reagent whose color shifts from red to yellow due to bacterial metabolic acidification. 6,32 –34 The time (in hours) required for the reagent shift was inversely related to the E. faecalis planktonic concentration. 6 To correlate the time for the reagent shift and the bacterial concentration, serial dilutions (from 108 to 102 CFUs/mL) of E. faecalis planktonic suspensions in PR-BTA were performed in a 96-well polystyrene microplate (Corning Incorporated, New York, NY). The time required for the color switch was measured by detection of color change at wavelengths of 450 nm and 630 nm in a microplate reader (EL808; BioTek Instruments, Winooski, VT). Absorbance values were recorded every 15 min for a 24-h period. To draw the correlation line linking the time for color shifts and bacterial concentrations, the Δ-OD values (450–630 nm) were considered and plotted versus the log10 of CFUs of the initial bacterial concentration at time 0. The equation and linear correlation coefficient describing the correlation line were calculated on the whole data set: y = −0.1816x + 5.4529, R 2 = 0.948.
To evaluate the biofilm on root canal walls, at the end of the treatment, each tooth was placed in a 1.5-mL Eppendorf vial containing 1 mL of the PR-BTA reagent and vigorously vortexed for 60 sec. After that three 100-μL aliquots of BTA reagent for each tooth were placed in a sterile, 96-well polystyrene microplate (Corning Incorporated) and incubated in the microplate reader at 37°C for 24 h (Fig. 5). The bacterial load was calculated evaluating the time required to obtain a Δ-OD (450–630 nm) of −0.05 from that of time 0 and the above reported equation. As the equation correlates the time required to shift the BTA reagent color and planktonic bacteria, the number of biofilms of E. faecalis was reported as planktonic-equivalent CFUs. 32
Ninety-six-well microplate after 24 h of incubation in the microplate reader at 37°C. The yellow wells are those in which the color shift of the BioTimer assay reagent occurred, and red wells are those in which the color shift did not occur.
Statistics
The correlation line and linear correlation coefficient were obtained as previously reported. 6,32 –34 Results are reported as mean values ± standard deviations obtained from at least three independent experiments. Statistical analysis was performed using Student's t-test, and p-values <0.05 (p ≤ 0.05) were considered significant.
Results
The conventional use of NaClO by hand irrigation significantly reduced the bacterial load in Group A with respect to the positive control. Of course, NaOCl has a well-known decontamination rate, so Group A was considered as a control group to evaluate the efficacy of different disinfection protocols. The important aspect that we found was that some analyzed techniques showed better results than only NaOCl hand irrigation. The results are shown in Fig. 6.
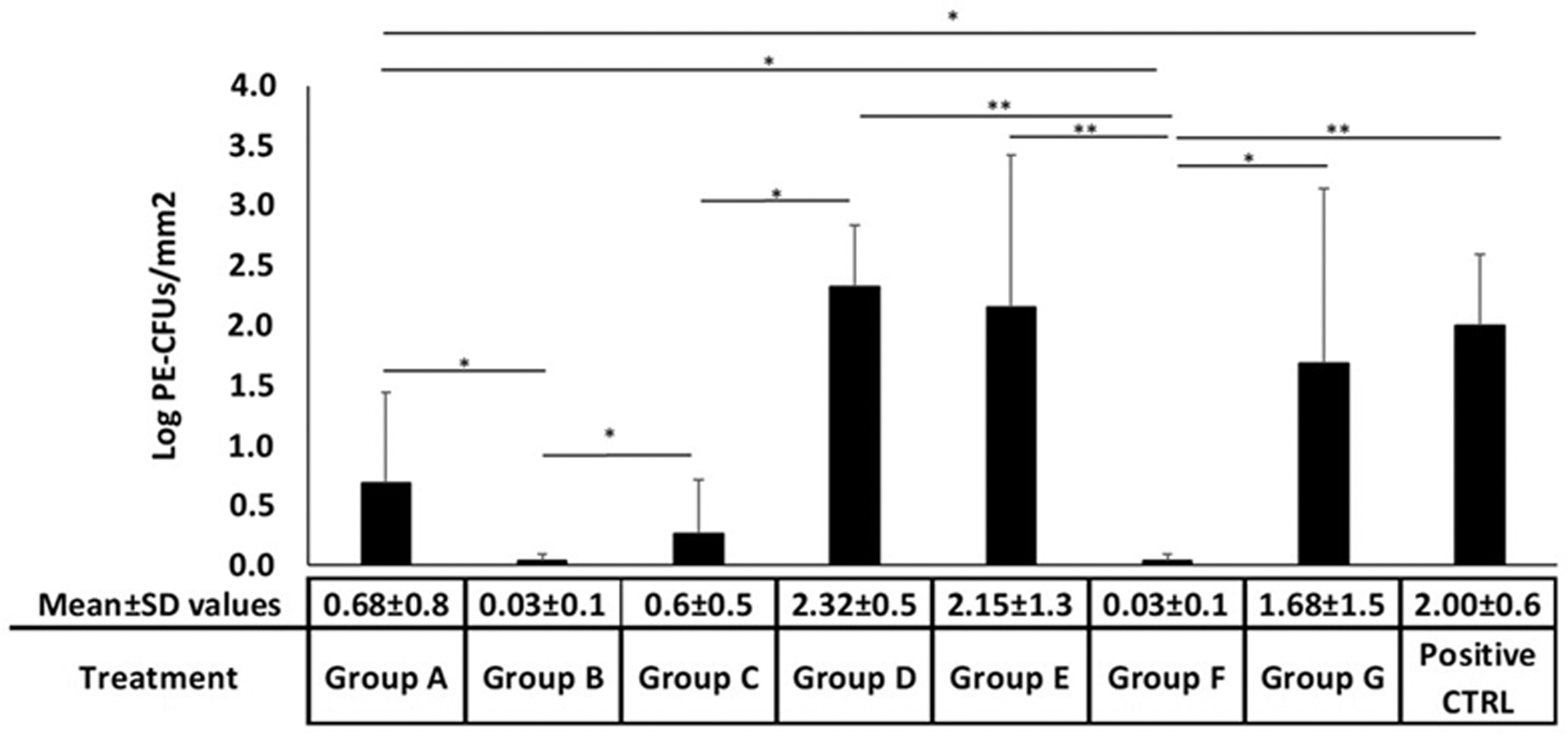
Counts of Enterococcus faecalis ATCC 29212 biofilms in experimentally infected single-root teeth. The experimentally infected teeth were treated as follows: Group A, NaClO hand irrigation; Group B: NaClO hand irrigation+EDTA+NaClO activated by PIPS; Group C: EDTA+NaClO activated by PIPS; Group D: toluidine blue activated by PAD; Group E: toluidine blue activated by PAD and PIPS; Group F: NaClO hand irrigation+toluidine blue activated by PAD; and Group G: NaClO hand irrigation+toluidine blue activated by PIPS and PAD. CTRL POS: positive control: no treatment. CTRL, control; EDTA, ethylenediaminetetraacetic acid; NaClO, sodium hypochlorite; POS, positive.
Moreover, in Table 1, the percentage reduction of E. faecalis biofilms with respect to control is reported. When NaClO was used in combination with EDTA+NaClO activated by PIPS (Group B), the effect of hand irrigation with NaClO (Group A) was increased and a significant decrease in bacterial load (>90% reduction) was recorded (p ≤ 0.05).
Treatment Efficacy in Reducing the Enterococcus faecalis ATCC 29212 Biofilm Population in Experimentally Infected Single-Root Teeth
CTRL, control.
Irrigation with EDTA+NaClO activated by PIPS (Group C) produced better decontamination than the conventional PAD protocol using toluidine blue (Group D; p ≤ 0.05) and a reduction of about 85% of bacterial biofilms was observed.
On the contrary, when PAD technology, both with and without PIPS (Groups E and D, respectively), was used to activate the photosensitizer, no bacterial reduction in comparison with controls was obtained. When a preliminary hand irrigation of NaOCl was performed, the PAD technique with toluidine blue as a photosensitizer (Group F) determined the highest reduction of bacterial load (98%) and significant values were recorded also in comparison with the positive control and Group A. The use of PAD and PIPS with toluidine blue as a photosensitizer after NaClO disinfection (Group G) showed weak antibacterial activity.
Discussion
The long-term success of a root canal therapy depends on effective cleaning and decontamination of the endodontic space in addition to a hermetic canal obturation. Since a bacterial-free endodontium is still unlikely to be obtained, 5 the risk of bacterial regrowth exists. 1
According to many studies, the use of laser techniques can help operators to achieve better decontamination. 6 Since thermal effects of diode and Nd:YAG lasers adversely affect the canal walls, other laser techniques such as laser-activated irrigation (LAI)-PIPS and PAD were proposed.
Accordingly, medium-infrared lasers with the LAI technique allow to overcome the difficult access of irrigants in the three-dimensional endodontic space, improving the decontamination effectiveness of commonly used irrigant solutions. 35,36
Golob et al. 37 determined the effectiveness of LAI by PIPS in reduction of E. faecalis in root canal disinfection and concluded that LAI using the 5% NaClO and PIPS protocol resulted in effective eradication of the bacterial biofilm and removal of the smear layer.
Azim et al., 38 comparing the efficiency of 4 irrigation systems to reduce the bacterial load in root canals, concluded that PIPS appears to be most effective in killing bacteria deep in the dentinal tubules.
Galler et al. 39 also investigated 4 irrigation methods and found that greater penetration depth occurred in the apical thirds with the PIPS technique.
In addition, PAD techniques were investigated by many authors for root canal disinfection.
Mohan et al., 29 comparing the efficacy of PAD with the conventional endodontic treatment and also a combination of conventional endodontic treatment along with PAD in infected root canals with E. faecalis, concluded that PAD used after chemomechanical preparation reduced the bacterial load of E. faecalis by 98.89% at 2 min and 99.5% at 4 min.
Similar results were obtained by Zorita-García et al. 30 who showed that PAD as an adjunct to conventional endodontic treatment produces a significant reduction in E. faecalis bacterial load and it should be considered for successful treatment.
By contrast, a recent review by Trindade et al. 40 suggested that most studies in endodontics do not confirm the ability of PAD to substitute conventional techniques. Although PAD may be an excellent adjunct to conventional endodontic therapy, data suggest the need for protocol adjustments, or new photosensitizer formulations, to improve PAD predictability in root canal disinfection.
In our study, when the PIPS protocol was used with EDTA and NaClO, significant decontamination in comparison with the control was achieved; when a preliminary NaClO irrigation was performed, a further reduction of about 98% in the bacterial load was observed (Group B).
The conventional PAD protocol showed minor antimicrobial activity compared with the PIPS protocol; however, its combination with preliminary NaClO irrigation enhanced bacterial reduction (Group F), reaching a rate of disinfection similar (98%) to that of the PIPS protocol (Group B), indicating the main role of NaClO irrigation in root canal disinfection.
However, NaClO hand irrigation alone (Group A) achieved worse disinfection (about 66%) results than Group C (about 87%) when the Er:YAG laser was used for irrigant activation and streaming in accordance with many studies that demonstrated that hand irrigation alone is not able to deeply penetrate the dentinal tubules, especially in the apical area. 6 –8,35 –37,39
The results of our preliminary study indicated that when hand irrigation is followed by PIPS activating EDTA and NaOCl and/or the PAD protocol using toluidine blue, superior results can be reached.
In this pilot study, no favorable results were obtained when PAD was preceded by Er:YAG laser irradiation to push the photosensitizer into the three-dimensional endodontic space, as in the PIPS protocol, but using toluidine blue instead of NaClO and EDTA.
The reasons for these unexpected results could be related to a possible chemical change of toluidine blue after irradiation with the Er:YAG laser, with different reactivity of free radicals produced and consequent possible minor effects of the radicals on bacterial cells with inadequate results. In addition, the number of samples is limited and a wider investigation is required to better evaluate these preliminary results and hypothesis.
By contrast, NaClO is a potentially toxic agent for periapical tissue, 41 so this innovative combined protocol and the possibility of replacing NaClO with toluidine blue, whatever the method of activation, should be further investigated.
Clinically, our preliminary results could suggest that the use of these disinfection techniques to improve root canal decontamination can be useful in daily activities to reduce postoperative endodontic pain and prevent some complicated endodontic infections supported by E. faecalis. 42
Conclusions
NaClO remains the best irrigant in endodontics, and primary NaClO hand irrigation enhances the results obtained with PIPS, PAD, and the combined technique. Without the preliminary irrigation of NaClO, the PIPS protocol using EDTA and NaClO is more effective than the conventional PAD protocol with toluidine blue in reducing the E. faecalis bacterial load in experimentally infected root canals. The possibility of replacing NaClO with toluidine blue, using a combined protocol of streaming and activation of the solution using both 2940 and 635 nm lasers, should be further investigated.
Footnotes
Acknowledgments
The authors wish to thank the laser companies, Fotona d.o.o. and Lasotronix, for the technical materials provided during the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding received for this study.