
Abstract
If controllable, stem cell activation following injury has the therapeutic potential for supporting regeneration in acute or chronic wounds. Human dermally-derived stem cells (FmSCs) were exposed to the cytokines interleukin-6 (IL-6), IL-1β, and tumor necrosis factor-α (TNF-α) in the presence of erythropoietin (EPO). Cells were cultured under ischemic conditions and phenotypically characterized using flow cytometry. Topical EPO application was performed in three independent clinical wound healing attempts. The FmSCs expressed the receptor for EPO. EPO had a strong inhibitory effect on FmSC growth in the absence of IL-6 and TNF-α. With IL-6, the EPO effects were reversed to that of growth stimulation. TNF-α had the strongest stimulatory effect. In contrast, IL-1β had an inhibitory effect. Topically applied EPO considerably enhanced wound healing and improved wound conditions of acute and chronic wounds. Site specificity of stem cell activation is mediated by IL-6 and TNF-α. In trauma, EPO ceases its inhibitory role and reverts to a clinically relevant boosting function. EPO may be an important therapeutic tool for the topical treatment of acute and chronic wounds.
Introduction
In an effort to identify new sources of MSCs, dermal rodent fibroblast cell lines were examined for their mesenchymal potential. 9 –11 Publications by Toma et al. 9 and Crigler et al. 10 suggest that the adult mammalian dermis contains tissue-derived stem cells and that these fibroblastic MSCs are more plastic than previously appreciated. Dermis-derived fibroblastic MSCs have been used for therapeutic applications such as transplantation to support bone formation. 12 –14 Toma et al. 9 demonstrated the mesenchymal plasticity of primary human dermal fibroblasts in vitro with different approaches regarding characterization and applications. 15 –18 Zuk et al. analyzed the phenotypic characteristics of these fibroblasts 19 and noted that their phenotype seems to be similar to that of adult-derived stem cells (ADSCs). 5,16,18
To continue these studies, we examined whether unselected human dermis fibroblastic mesenchymal cells possess stem cell-like characteristics and are phenotypically similar to ADSCs. 20 Bone marrow-derived MSCs (bmMSCs) have been shown to support the wound healing of chronic skin wounds. Badiavas and Falanga have demonstrated that chronic skin ulcers of patients with arterial and venous insufficiency were healed with complete wound closure and less scar formation when treated with bmMSC-seeded grafts. 21
To characterize dermally-derived stem cells (FmSCs) relative to ADSCs, we analyzed the cytoskeletons and compositions of the extracellular matrix as well as the mesenchymal phenotypes and differentiation properties of both. The data obtained show for the first time that primary human dermal fibroblasts in vitro share common characteristics with ADSCs, such as phenotype and differentiation potential. Our results demonstrated that FmSCs fulfill the three main characteristics of MSCs: They express all MSC-related surface antigens homogeneously; their cytoskeleton and matrix compositions are quite similar to that of MSCs; and they differentiate along the adipogenic and osteogenic cell lineages. 20
These conditions, however, do not sufficiently explain the mechanism of endogenous stem cell activation in the case of injury alone. Therefore, we developed an in vitro model of trauma conditions by investigating the role of IL-6, IL-1β, and TNF-α on human skin stem cells, identified a receptor for erythropoietin (EPO) in these cells, and investigated the role of EPO with and without the presence of the trauma cytokines. The knowledge obtained from these studies was then transferred to three independent and specific clinical cases: EPO was topically applied to a split-thickness skin graft donor site, a pressure ulcer, and a vascular ulcer.
EPO has been used in clinical practice for a wide range of diseases, 22 obtaining systemic application via a subcutaneous, intramuscular, or intravenous route. 23 –28 A topical administration to stem cells at the site of the wound injury would allow a more direct stimulatory response and would work only if an appropriate interference with site-specific mechanistic responses occurred. The elucidation of such mechanisms and the development of a therapeutic potential are the scope and success of this study.
Methods
Cell isolation
Human juvenile foreskin samples were obtained from 4-year-old patients undergoing circumcision after written consent was obtained. This study was approved by the ethics commission of Leipzig University and was conducted in accordance with the Declaration of Helsinki protocols.
Epidermal and dermal tissue were isolated by mechanical and enzymatic digestion, as previously described by Ponec et al. 29 After removing the epidermis from the dermis, the tissue was cut into small pieces and washed three times with sterile phosphate-buffered saline (PBS) at room temperature. The pieces were then incubated with 0.075% collagenase type A (Roche Diagnostics, Mannheim, Germany) for 12 h at 37°C with gentle agitation.
For FmSC suspensions, the enzymatic reaction was inactivated with Dulbecco modified Eagle medium (DMEM)/10% fetal bovine serum (FBS; Gibco/Invitrogen, Karlsruhe, Germany) and filtered through a 70-μm mesh. This cell suspension was centrifuged at 600 × g for 5 min. The cell pellet was then gently resuspended in DMEM/10% FBS, filtered through a 70-μm mesh, and plated in conventional T75 tissue culture flasks (BD Falcon, Heidelberg, Germany). Cells were cultured in DMEM supplemented with 10% FBS, GlutaMAX-I, 4.5 g/L glucose, and pyruvate (Gibco/Invitrogen).
Cell proliferation
FmSCs were seeded in six-well plates at passage 4. After 1 day of cultivation in DMEM/10% FBS, the cells attached and adapted to start proliferation. On the following day, the cells were cultured with the same medium but without FBS to minimize serum-induced effects. The next day, cytokine stimulation of the cells was initiated with cultivation in DMEM/10% FBS supplemented with or without 10 ng/mL EPO in combination with 10 ng/mL IL-6, 10 ng/mL IL-1β, or 10 ng/mL TNF-α. Controls were also performed with each cytokine alone. At days 3, 5, 7, and 11, cells were trypsinized, and viable cell numbers were counted in a hemocytometer by Trypan Blue staining. All experiments were done in triplicate, with three independent sets of patient materials.
Cell immunophenotyping
Immunophenotyping of FmSCs was performed as described previously by Lorenz et al. 19 The following labeling reagents were used: Fluorescein isothiocyanate (FITC)- or phycoerythrin (PE)-conjugated mouse antibodies, anti-human CD31 (Biozol Diagnostica, Munich, Germany), anti-human CD45 (Sigma-Aldrich, Seelze, Germany), anti-human CD90 and anti-human CD105 (BD Biosciences, Heidelberg, Germany), and anti-human CD166 (Acris Antibodies, Hiddenhausen, Germany). The monoclonal antibody mouse anti-human CD73 (BD Biosience) was unlabeled and combined with a secondary PE-labeled goat anti-mouse antibody (Sigma-Aldrich). Incubation and flow cytometry analyses were performed according to conventional techniques. 29 Isotype controls were equally concentrated, labeled or unlabeled. The stained cells were analyzed on a FACSCalibur (BD Bioscience) using CellQuest Pro (BD Bioscience). Fluorescence intensities were determined by flow cytometry in a minimum of 1 × 104 cells.
Growth curves
To record a growth curve, three individual tests were performed, each in triplicate. Cell counting was performed at day 0, 1, 3, 5, and 7 by trypsinization and Trypan Blue staining using a Neubauer chamber. The cells were seeded at passage 6 with a density of 20,000 cells/well (9.6 cm2) in a six-well plate (Falcon) 2 days before stimulation (day 0). The exchange of medium 1 day before stimulation from 10% FBS-containing DMEM to serum-free DMEM ensured the attachment of the cells during the last 24 h and a minimal protein background from the FBS. The stimulation was made with or without the presence of IL-6, IL-1β, and TNF-α by adding EPO (NeoRecormon, Roche) and/or the cytokines (all RELIAtech) to the medium and performing a full medium exchange. At days 3 and 5, half the volume of the medium was changed with medium containing the initial concentrations of EPO and/or cytokine. The cell scores of each sample and the average of all nine samples were calculated, including the standard deviation. To compare the different growth curves, a Student t-test was used to test the significance of the differences between the breakpoints.
For stimulation with cytokines, a concentration-dependent pretest was performed to identify the minimum concentration needed for successful stimulation; this was determined to be 10 ng/mL.
Clinical cases
In three highly different clinical situations, topical EPO application was used to support wound healing. All patients provided informed consent according to the guidelines of the local ethical committee and the national legal requirements in Germany. Topical treatment was performed using a mixture of 3,000 IE erythropoietin-β (NeoRecormon®, F. Hoffmann-La Roche AG, Basel, Schweiz) and 20 g of hydrogel (Varihesive®, ConvaTec, NJ). In patient A, the mixture was topically applied to a 0.3-mm deep split-thickness skin graft donor sites measuring 8 × 24 cm directly after skin harvesting. The donor site at the thigh was subsequently closed with a polyurethane dressing (OpSite®, Smith&Nephew, London, UK). After 3 and 6 days, the mixture was again applied by puncturing the polyurethane film, which remained on the wound. At day 7, the film dressing was removed to evaluate the reepithelialization. Another donor site of equal depth and dimension at the contralateral leg of patient A was treated similarly, but the mixture was replaced by hydrogel alone, without EPO. Again the dressing rested in place for 7 days followed by dressing removal and wound assessment. The standardized wound management provided an ideal comparability of both similar wounds.
Patient B had a nonhealing pressure sore at the heel following urosepsis, and patient C had a nonhealing vascular ulcer. In both patients, the wounds were surgically debrided and treated in the same manner, using the same mixture of EPO and hydrogel. Moist wound management was provided by covering both wounds with Varihesive® (Convatec, Skillman, NJ). A total of five dressing changes with new EPO applications were performed in both patients to prepare the wound for skin grafting. The poor general condition of patients B and C did not allow extensive reconstructional procedures. Therefore, the aim of local EPO application was to prepare the wound bed in a manner that would enable subsequent successful skin grafting and avoid lower leg amputation by a minor surgical procedure.
Results
Sequencing the EPO receptor in human FmSCs
Cells were characterized for their expression of CD31, CD45, CD73, CD90, CD105, and CD166. The expression of CD34, CD71, and CD133 was also examined. Fig. 1a shows the mRNA expression profile of the EPO receptor in FmSCs. Sequencing of the PCR product for the mRNA of the EPO receptor showed 90–98% sequence homology.

Cells were cultured from human biopsies and grown to the 4th passage in vitro. (
Switch from inhibitory to stimulatory effects of EPO on stem cell proliferation
Cells were cultured from human biopsies and grown to passage 4 in vitro. Stimulation of EPO alone in the absence of any cytokines showed an inhibitory effect on stem cell growth (Fig. 1b). Cells under control conditions grew up to 0.515 million cells. In contrast, we observed a dramatic decrease in cell proliferation when the FmSCs were stimulated with EPO. Cell proliferation was minimized by 32%, to a total cell number of 0.351 million cells. IL-6 stimulation of FmSCs also resulted in decreased growth activity relative to the control cells, but this was reversed in the presence of EPO (Fig. 1c). This indicates both an inhibitory role of EPO (Fig. 1b) in the absence of cytokines or in the late phase of trauma and a supportive, boosting activity of EPO in the presence of IL-6 (Fig. 1c). TNF-α was a strong stimulator of FmSC proliferation, and the presence of EPO did not influence this. Cell proliferation was elevated most with TNF-α. IL-1β had an inhibitory effect on the proliferation of the stem cells compared to controls cells, both with and without EPO.
Effect of stimulation on the expression of stem cell markers
To characterize the FmSCs, surface antigens were analyzed by flow cytometry. FmSCs homogeneously expressed CD90, CD73, CD105, and CD166 (Figs. 2 and 3). In contrast, expression of endothelial cell-surface markers such as CD31 was not detected. In addition, hematopoietic cell subpopulations positive for surface antigens such as CD45, CD14, and CD133 were not observed. During cultivation and stimulation of FmSCs with inflammatory cytokines in combination with EPO, we did not detect any changes in the surface antigen expression of MSC markers. Except when cultivating FmSCs with IL-6 in combination with EPO, we found changes in the expression of CD90. This suggests that the unselected stem cell population was stimulated differently, and thus two different CD90-expressing cell populations were detected. (Fig. 3)
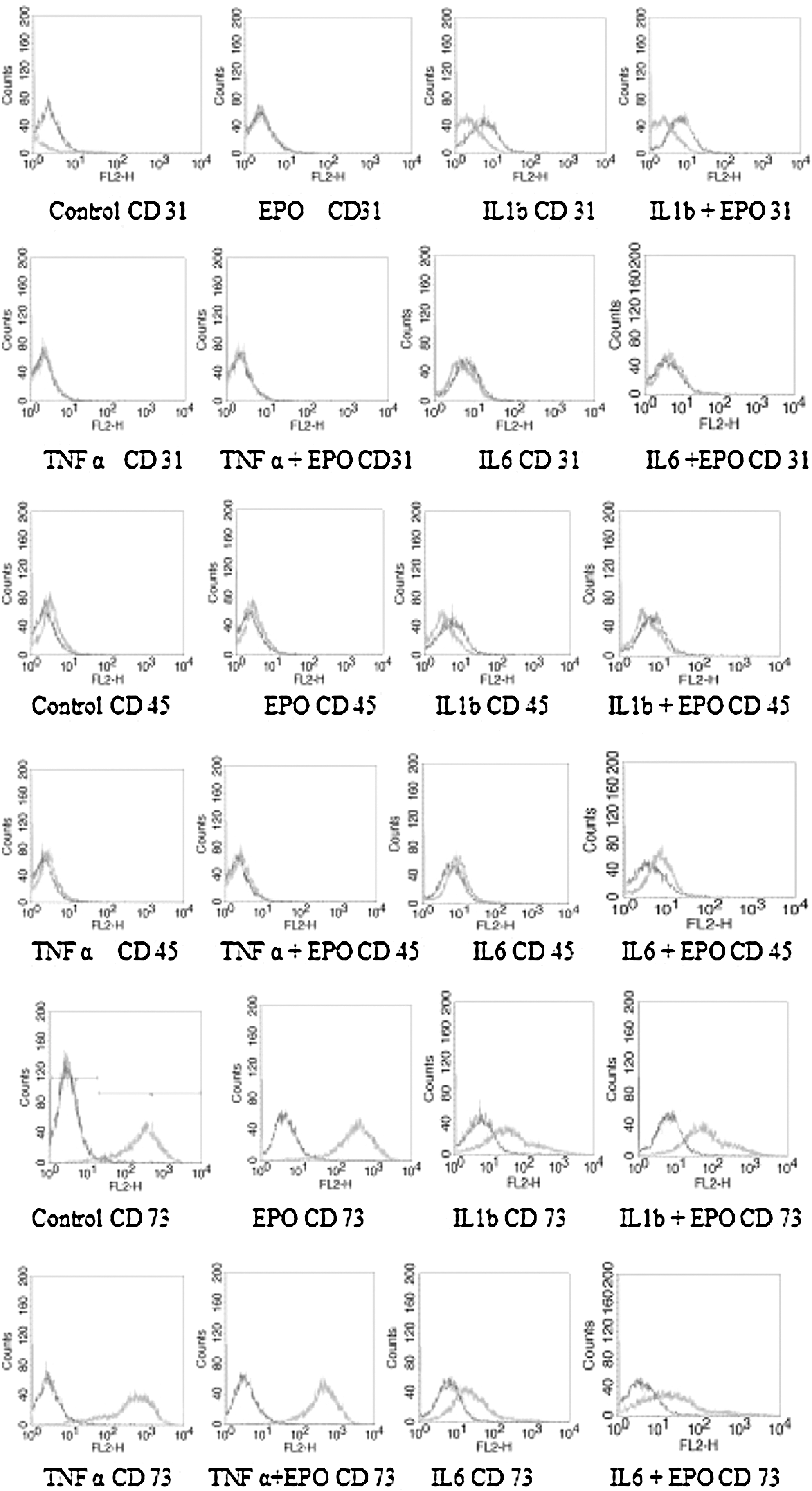
Phenotype of the dermally derived stem cells (FmSCs), determined using flow cytometry. Erythropoietin (EPO) triggering did not change the phenotype at all; CD31, CD45, and CD73 remained stable with or without the presence of trauma cytokines. There was no major population shift. IL1b, Interleukin-1β; TNF-α, tumor necrosis factor-α.
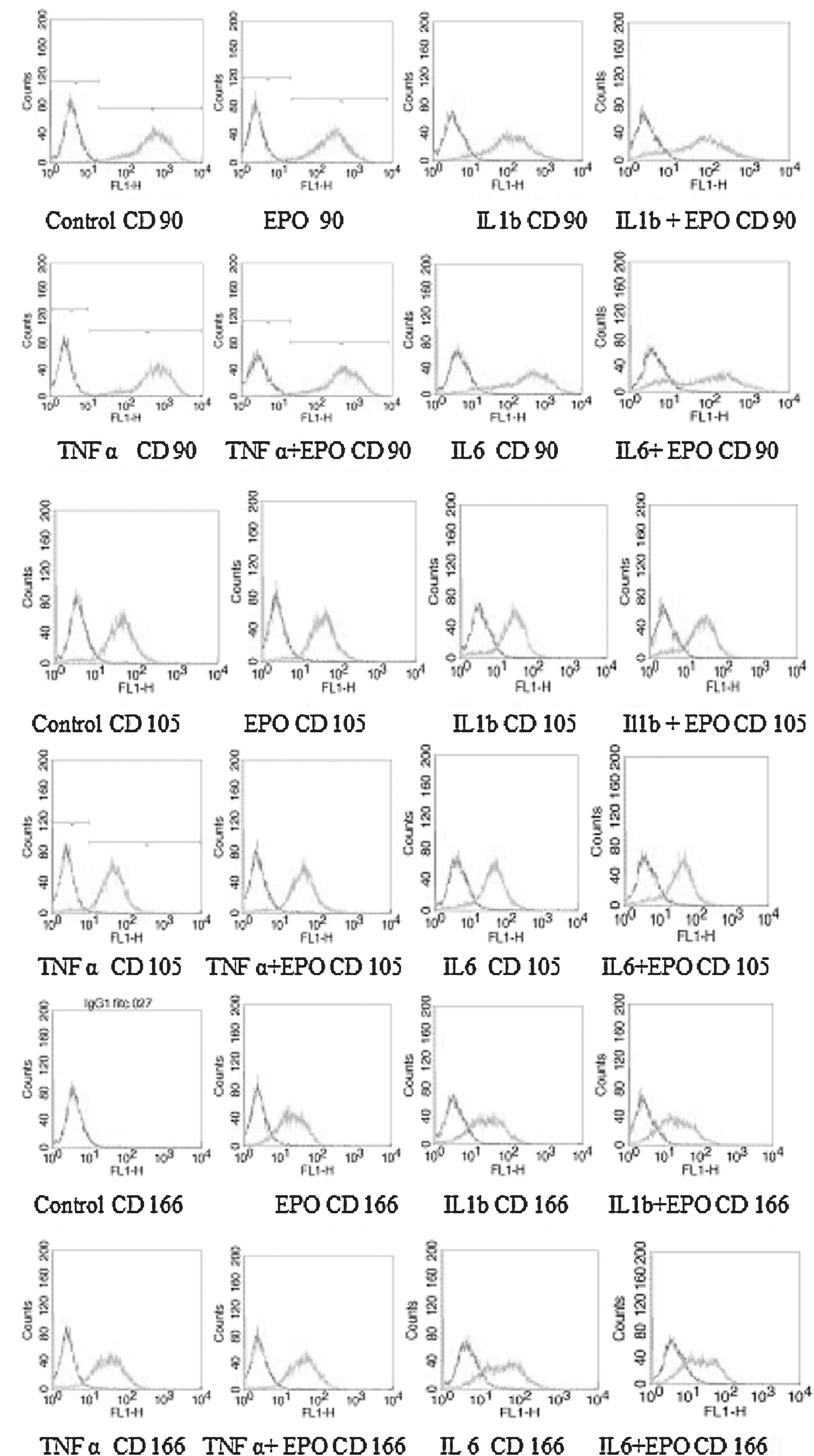
The phenotype of dermally derived stem cells (FmSCs) did not change with CD105, and CD166 remained stable with or without the presence of trauma cytokines. We did observe that cells expressing CD90 partially switched to a non-CD90-expressing subpopulation in the presence of interleukin-6 (IL-6). This “IL-6 effect” paralleled the growth curves in the presence of IL-6. No major population shift occurred except for this. (Control CD 166: EPO CD 166.) EPO, Erythropoietin; IL1b, interleukin-1β; TNF-α, tumor necrosis factor-α.
In vivo experiments
The more complex in vivo situation is characterized by an intricate interplay of cytokine profiles, consisting of mixtures and time-sequence variations with respect to availability. In patient A, complete and stable reepithelialization of the split-thickness skin graft donor site, topically treated with EPO, was achieved 7 days after the operation. The wound surface was closed, dry, and clearly looked pale. (Fig. 4a). In contrast, the donor site at the contralateral thigh that was treated without EPO showed incomplete reepithelialization at this time point, indicated by secretion and a dark-red wound surface. (Fig.4a)

In patient B, sufficient granulation tissue formation was obtained after five local treatment sessions with EPO, which provided an highly vascularized wound bed for sucessful split-thickness skin grafting. The ideal prepared wound bed enabled salvage of the limb without extensive reconstructive procedures (Fig. 4b). In patient C, improved healing and sufficient granulation tissue formation was achieved following five local applications of EPO. (Fig.4c) After subsequent skin grafting at days 21 and 56, the wound healed well and has remained stable for more than 12 months (Fig. 4c).
Discussion
EPO is a type I cytokine that was approved by the U.S. Food and Drug Administration (FDA) in 1989 for the treatment of the anemia of end-stage renal disease. Thereafter, EPO has been used for the treatment of a diverse range of diseases, including cancer, 28,31,32 heart care erythropoiesis, 33 –37 malaria, 38 ischemic and degenerative damage of neurons, 40 retinopathy, 40,41 and diabetic retinopathy. 42 –45 EPO plays a crucial role in the process of endochondral ossification in bone repair in mice via EPO-receptor (EPO-R) expression. 46 Gough 47 supported the concept that understanding the EPO receptors by which EPO signaling contributes to organ development provides information on the differentiation of erythrocytes. Interestingly, Foster et al. 48 found increased EPO-R protein levels in dynamically growing canine lungs after pneumonectomy, suggesting a paracrine role for EPO signaling in lung growth and remodeling. This hypothesis may be applicable to other types of organ repair because EPO and EPO-R are expressed in several organs (e.g., kidney, brain, heart, muscle, and endothelial cells). 49 However, it is now known that EPO and EPO-R are local products in a wide range of cells that specifically protect other cells from potentially cytotoxic events and metabolic stress.
Adding to the evidence of Bodo et al. 50 that normal human skin expresses EPO and functional EPO-R, our study showed that skin stem cells specifically are the responsive elements in normal skin containing the receptor for EPO and thus show a special readiness for action in the case of traumatic skin injuries. In the case of injury and ischemic trauma, cytokines IL-6, IL-1β, and TNF-α are alerted. We demonstrated that the trauma cytokine IL-6 and EPO synergistically upregulated stem cell growth in the case of hypoxic skin conditions. In contrast, without trauma, EPO exerted an inhibitory effect on in vitro skin stem cells. This effect reverted to stimulation in the presence of IL-6 and TNF-α. Only IL-1β maintained its inhibitory function with or without EPO. Neither the trauma cytokines nor EPO grossly changed the phenotype of the fibroblast precursor cells.
Our findings agree with the observations of Paus et al. 51 that the oxygen-sensing skin response is mediated by skin EPO. In situations of low oxygen, skin EPO and IL-6 are “alarmed” to react to the site-specific injury. This finding complements the relevance of our data as a physiological and potentially highly relevant therapeutic strategy for endogenous stem cell activation in the case of trauma.
In the human scalp, it was shown that hair follicles expressed EPO at the mRNA and protein levels, upregulated EPO transcription under hypoxic conditions, and expressed transcripts of EPO-R and the EPO stimulatory transcriptional cofactor hypoxia-inducible factor-1α. These findings are in line with recent research results showing that hair follicle-derived keratinocytes were a major cell source for reepithelialization during wound healing 52 and that the hair follicle connective tissue sheath was a source of granulation tissue formation. 53
Boutin et al. 54 revealed the EPO-connected oxygen-sensing functions of the skin and elucidated how mammalian cells adapt to low oxygen levels by recruiting the skin as a central coordinator of the systemic response to hypoxia. Hair follicles are able to detect insufficient oxygen levels, a crucial mechanism of the extremely fast renewing and proliferating cell population, to regulate its metabolic balance. Using transgenic mice studies, Köchling 55 revealed that the hypoxia response elements are located upstream (between 9.5 and 14 kb) of the EPO gene in the kidney and downstream (within 0.7 kb) of the EPO gene in the liver. It has been shown that the circulating levels of EPO may increase up to 1,000-fold in response to hypoxia in the kidney. 53
In the absence of trauma cytokines, EPO downregulates the proliferation of skin stem cells in vitro. In the case of traumatic skin hypoxia, IL-6 and TNF-α activate stem cells. Specifically, in the presence of IL-6, the inhibitory role of EPO is reversed to increase stem cell proliferation. This represents an adequate response to a pathophysiological need. The stimulatory effects of TNF-α are not diminished by the previously inhibitory role of EPO. Among the trauma cytokines studied here, only IL-1β also exhibited an inhibitory function that did not interfere with the original inhibitory role of EPO. In vivo, we observed the net effect of cytokine and EPO stimulation in acute and chronic wound types. In both cases, the regenerative response was boosted qualitatively and quantitatively. By these mechanisms, the skin trauma EPO system switches from its inhibitory function to a supportive role for boosting skin regeneration. The inflammatory activity of the wound itself represents a permissive situation for the boosting activity of EPO, which seems to reduce the healing time at split-skin graft donor sites from 10 to 7 days. In the previously nonhealing wounds, EPO assumes an enabling role that shifts the balance from nonhealing to healing and triggers the formation of granulation tissue. The expression of EPO-R on the stem cells suggests that this could be a normal role of EPO that permits the human body to recover from site-specific tissue damage or injury in any area of the human body. This mode of action has been demonstrated clinically by the clearly accelerated reepithelialization of the EPO-treated donor site in direct comparison to the non-EPO-treated donor site at the same patient.
Nonhealing chronic wounds are at the opposite end of the spectrum of acute wound-healing mechanisms, progressing toward healing at a different rate. In the case of diabetic patients, this represents a critical situation for surgical practice, because approximately 22 million diabetic patients suffer from chronic wounds, 57,58 with many of them suffering from nonhealing chronic wounds. 59 There are approximately 5.2 million pressure ulcers and 7.6 million venous ulcers in the world that require treatment every year.
Fibroblasts form granulation tissue via hyperproliferation. This leads to a normal process of not only cellular rebuilding of lost dermal tissue but also reconstitution of the physical barrier of the basal lamina and the scaffold for revascularization. Large-area wounds do not heal within a short time, so the risk of infection and dehydration rises dramatically. Our results suggest that we can completely alter the wound-healing landscape and have a major impact on the care of both acute and chronic wounds. This study provides mechanistic evidence to support the hypothesis that this novel treatment modality physically modifies the wound microenvironment and thereby promotes wound healing in clinical relevant manner.
In a few clinical applications, fibroblasts were used to treat diabetic or venous ulcers, 60 –62 but this methodology remains controversial. We report a mechanism explaining how endogenous stem cells can be activated locally at the site of a severe wound without necessitating the transplantation of exogenous cells. All clinical cases, although diverse in their pathophysiology, were dramatic successes with respect to their respective healing responses.
Brines and Cerami described 63 that EPO is locally produced in the immediate surrounding area of a tissue injury to counteract the destructive effects of cytokines such as TNF-α by preventing cell apoptosis, thus the development of secondary, proinflammatory cytokine-induced injury can be reduced. However, a delicate balance in tissue injury exists between EPO and proinflammatory cytokines such as TNF-α. Therefore, compensatory EPO production by nearby tissue balances the effects of inflammatory mediators and prevents the further spread of damage. 63 Hamed et al. reported that treatment with topical EPO improves the defect repair of excised wounds in diabetic rats. 64 They suggested that vascular vascular endothelial growth factor (VEGF)-induced angiogenesis, enhanced collagen deposition, and reduced apoptosis in the diabetic wound bed are among the mechanisms that underlie the effects of topical EPO. This work by Hamed et al. 64 was the first to investigate the use of topical EPO treatment for wound healing. However, we are the first of topical EPO treatment for acute and chronic wounds patients. Although other cytokines such as tumor growth factor-β, monocyte chemoattractant protein-1, and colony-stimulating factor-1 are released from the invading inflammatory cells to the wound bed upon skin injury and in chronic wounds, 65 we selected these cytokines (IL-6, TNF-α, and IL-1β) because these are leading cytokines that are associated with organ trauma injury, including chronic wounds. 66
Despite the beneficial effect on wound repair, one has to assume that doses of EPO are rather high within the defect wound and low systemically. Rezaeian et al. 67 demonstrated that a triplicate intraperitoneal dose of 500 IU EPO/kg body weight over 48 h did not influence red blood cell (RBC) count and hematocrit, whereas Galeano et al. 68 observed a significant increase in RBC count and hemoglobin after 12 days of daily subcutaneous administration of 400 IU EPO/kg body weight. In comparison to this, the EPO concentration of our present clinical study is 50 U (one time) by topical application of the hydrogel containing EPO in the patients. This concentration (50 U) is 75 times less than other existing dose of various other experimental or clinical models. Using this concentration, we are conducting multicenter clinical trials for actute and chronic wound pateints. Each time, fresh hydrogel is prepared; the half-life of EPO is 48 h and it is stable in gel up to 12 weeks. There is no systemic effect of treated patients, which is one of the main advantages of this topical application. We measured the RBC count and the hemoglobin, leukocyte, and platelet counts of the patients before and after EPO treatment, but there was not any difference.
Our present investigation may provide a standard supplemental therapy for reducing the mortality and morbidity associated with chronic wounds, especially in the elderly, the disabled, and those with diabetes. Large-area burn injuries, where the wound closure is a race against time, may especially benefit from the healing accelerating characteristics of EPO. The burned, debrided, and grafted areas and the skin graft donor sites have to heal in a limited time frame. Frequently, donor sites do not rejuvenate for reharvesting as fast as needed, resulting in graft deficiencies that may lead to further extensive complications with fatal outcomes. The targeted clinical areas will improve in the assistance toward accelerating regeneration of acute and chronic wounds, and endogenous stem cell activation may reduce the need for skin grafting of burns.