
Abstract
Infectious diseases remain a significant cause of morbi-mortality in adults aged over 60 years, and many of these diseases are vaccine-preventable (VPDs). There is a pressing need to promote a lifelong vaccine schedule to increase vaccination against VPDs during the different stages of life. We outline the impact of vaccines on the burden of common infectious diseases and consider the negative clinical impact of VPDs in the unvaccinated population. We further illustrate that vaccine uptake is associated with a reduction in the burden of VPDs at any age of life, due to herd immunity. Disability-free and healthy aging is closely linked to childhood health and medical conditions in young adulthood. The midlife vaccine gap drastically impacts health in later life, especially in unvaccinated and older populations. These arguments underline the need for a preventive lifelong health perspective from childhood through old age.
Introduction
Disability-free and healthy aging are closely linked to childhood health, as well as events and medical conditions in young adulthood, underlining the need for a preventive life-course health perspective.
5
Currently, infectious diseases remain a significant cause of morbidity and mortality in the adult population over 60 years of age, and many of these diseases are vaccine preventable. In the United States, in 2006, it was estimated that approximately 200 children died from vaccine-preventable infectious diseases (VPDs), compared to more than 70,000 adults—a stunning 350-fold difference.
6
Vaccine coverage rates in adults for the most common VPDs are still lower than recommended, even in high-risk groups. For example, influenza vaccine coverage in adults aged 65 and over is far from that recommended by the World Health Organization (WHO)
7
and the European Commission (EC).
8
Regardless of age, coverage rates are worst in high-risk adult populations.
9
This just goes to show what a short memory the populations in developed countries have, because they seem to have forgotten the outstanding benefits of childhood vaccine programs, only to focus their current beliefs and attitudes on incomplete or biased knowledge.
Evidently, there is a pressing need to promote a lifelong vaccine schedule with a view to increasing vaccination against preventable infectious diseases during the different stages of life. To support this argument, we propose to: (1) testify to the historical impact of vaccines on the burden of common infectious diseases, such as seasonal influenza and invasive pneumococcal disease, measles, diphtheria, and pertussis; (2) consider the negative clinical impact of VPDs in the unvaccinated population; and (3) demonstrate that vaccine uptake is associated with a reduction in the burden of VPDs at any age of life. Finally, increasing the vaccine uptake among older and aging adults would also reduce both antibiotic prescribing and/or misuse, hospitalization rates, and probably nosocomial infections, without increasing lifelong cost of care. 10
Epidemiological Changes in Infectious Diseases According to Whether or Not the Existing Childhood Vaccination Schedule Was Applied
Throughout the developed world, childhood vaccine programs are consistent, precise, well accepted, and effective. In the countries of the European Union, the European Economic Area, and the European Free Trade Association (hereafter, collectively termed “Europe”), the majority of childhood vaccination schemes were set up in the 1980s, but their implementation has progressively increased since, despite an active antivaccine movement. 6
Measles
In the 1980s, the number of notified cases of measles in Europe was above 4 million, with a vaccine coverage rate lower than 30% (Fig. 1). 11 In 1999, the number of notified cases in the same geographic area had dropped to 56,319 cases, and was further reduced to only 6,840 cases in 2008. This impressive fall (an 80% reduction in less than two decades) has to be attributed to the uptake of the measles vaccine, which has increased constantly over the same period, and is currently around 80%. This picture shows encouraging progress. However, the situation still remains unsatisfactory for several reasons.
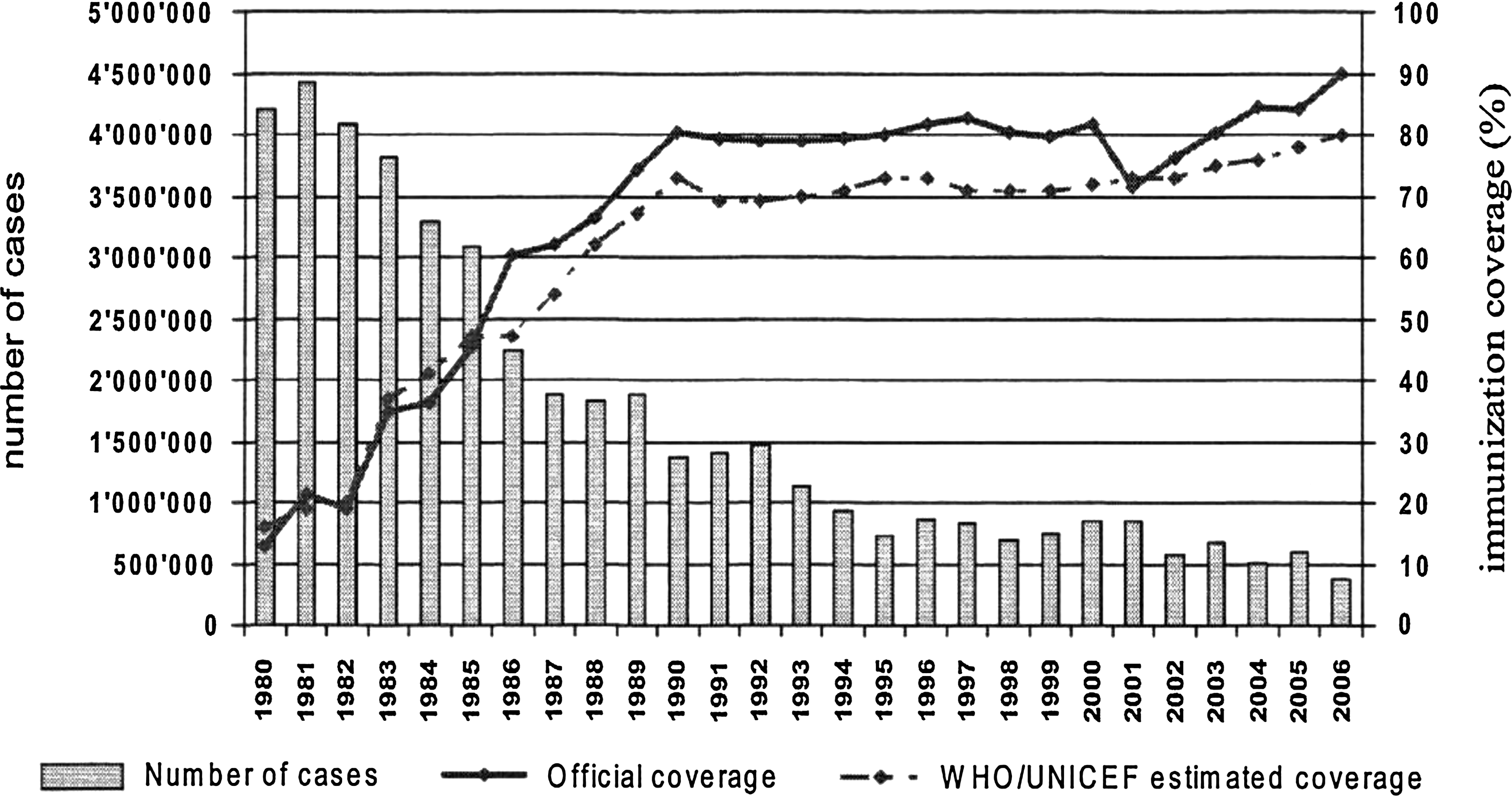
Measles global annual reported incidence and MCV coverage, 1980–2006 in the European Union, the European Economic Area, and the European Free Trade Association. Data from WHO Vaccine Preventable Diseases, Global Summary, Geneva, 2007.
First, in Europe, over the last decade (1999–2008), the total number of notified measles cases was 301,635; many of these were notified in Turkey (91,670 cases), Ukraine (72,484 cases), France (39,312 cases), and Italy (36,700 cases). 12 More importantly, many children born in the 1980s who did not receive the measles vaccine have gone on to develop more severe clinical forms of this disease during their third to fourth decade, such as serious diarrhea, pneumonia, or encephalitis (subacute sclerosing panencephalitis).
Therefore, measles, which is a VPD in childhood, is increasingly considered instead as a severe adulthood disease in the nonvaccinated population. This reinforces the importance of obtaining maximum measles vaccination coverage in newborns and infants.
Pertussis (whooping cough)
The same epidemiological figure can be drawn for pertussis. In 1999, the number of notified cases of pertussis in Europe was 55,166, decreasing to 21,061 in 2008. This reduction (almost 30% in less than one decade) can be attributed to the increase in the uptake of the pertussis vaccine in children and teenagers. Coverage has been progressively increasing, although it still remains below 90%. Over the last decade (1999–2008), the total number of notified pertussis cases in Europe was 292,806, occurring mainly in The Netherlands (59,915 cases), Norway (36,889 cases), and Switzerland (34,400 cases). 12 Among children born in the 1980s who did not receive the pertussis vaccine, there have been many cases of more atypical forms of the disease developing after the third decade of life. Moreover, herd immunity is particularly important in the case of pertussis, because the two populations at highest risk from this pathogen are children and older adults (generally the children's own grandparents). Thus, as for measles, pertussis is another childhood VPD that must be taken into consideration in the young and older nonvaccinated population.
Indeed, a recent epidemiological study comparing the incidence of pertussis in The Netherlands between two time periods (1998–2001 and 2002–2005) showed a 68% increase in pertussis in the population of subjects aged over 65. 13 Hospitalization rates are highest in infants aged below 6 months (86%) and in persons aged 85 or older (80%). 14 As morbidity from pertussis in older adults can be substantial (7.2% have prolonged cough), 15 with a high risk of disease interference with childhood infections, it would be advisable to try to reduce the burden of pertussis by vaccinating aging and old adults with diphtheria, tetanus, and pertussis (DTaP). 16 –19 The severity of disease after the age of 75 is comparable to that observed in young children, and hospitalization rates reach 80% in octogenarians. 15 More than 20% of unexplained chronic cough in old adults is linked to pertussis. 20 This demonstrates once again the importance of optimizing pertussis vaccination in children and teenagers with booster doses during adulthood.
Diphtheria
In 1980, the number of notified cases of diphtheria in Europe was just below 100,000. 11 In concrete terms, this means that in the 1980s the diphtheria vaccine coverage rate was below 30%, whereas currently it reaches 80%–90% (Fig. 2). However, between 1999 and 2008, the total number of diphtheria cases within Europe was dramatically high, reaching a total of 8,470, mainly occurring in the Russian federation (5,148 cases), the United Kingdom (1,790 cases), and Latvia (625 cases). The main populations infected were unvaccinated adolescents, middle-aged adults, and over 65s. Again, it can be seen that diphtheria is a classic childhood VPD that has become an adult disease in the nonvaccinated population. These data demonstrate the importance of a high vaccine coverage rate in newborns and infants, and the necessity to increase administration of booster doses in adults.

Diphtheria global annual reported incidence and MCV coverage, 1980–2006 in the European Union, the European Economic Area, and the European Free Trade Association. Data from WHO Vaccine Preventable Diseases, Global Summary, Geneva, 2007.
Tetanus
Unfortunately, the annual number of tetanus cases did not change significantly between 1999 and 2008, with nearly 200 cases notified each year. The total number of cases over the last decade (1999–2008) was 2,039, mainly notified in Turkey (420 cases), the Russian Federation (285 cases), France (173 cases), and Italy (with 139 cases per year in both 2002 and 2003). 11 Most of these cases affected adults over the age of 65, whereas, over the same 10-year period, neonatal tetanus has completely disappeared in Europe. These figures highlight the need for renewed, complete tetanus vaccination or a tetanus booster dose in the sixth decade of life, after assessment of vaccine history and clinical status.
This brief review of the epidemiological changes occurring in common VPDs over the last few decades clearly shows the need for scrupulous respect of the standard childhood vaccination schedule. This then needs to be consolidated by a vaccine program dedicated to older and aging adults. Bridging the vaccine gap that exists in the midlife period would contribute to healthier aging among the population.
Burden of Preventable Respiratory Tract Infectious Diseases in the Geriatric Population
Respiratory tract infections (seasonal influenza and pneumococcal diseases) are preventable infectious diseases (IDs) that remain a significant cause of morbidity and mortality. Together, they represent the fourth most frequent cause of death in developed countries, and mainly affect adults over 60 years of age. These data are particularly alarming when one considers the considerable increase in the proportion of adults who will be aged over 60 by the year 2050. 21
However, the implementation of guidelines for vaccination would be difficult in view of the conflicting evidence about the usefulness of vaccines, the widely held belief that previous or repeated exposures provides protection, the fact of feeling healthy, and the almost universal certitude that vaccines have more adverse side effects than benefits. 22 On the other hand, the onset of immunosenescence means that there is a likelihood of being less well protected when vaccinated at an older, rather than younger age with currently available vaccines. 23 Nonetheless, these arguments do not appear to discourage vaccination completely, as demonstrated for seasonal influenza and invasive pneumococcal disease, where it has been shown in Europe that influenza vaccination uptake is greater among subjects aged >65 than among high-risk subjects aged under 65. 24
Seasonal influenza
The majority (∼90%) of influenza-related deaths occur in older adults. In addition, catastrophic disability resulting from influenza-related hospitalization represents a significant burden in this vulnerable population. 25 Since May, 2003, recommendations for the use of influenza vaccines are mainly targeted at the older population and at-risk individuals, i.e., those with underlying diseases. 26 However, there are considerable discrepancies in the definitions of “at-risk” and “older,” with the result that vaccination coverage differs significantly between countries. Certain countries recommend yearly influenza vaccination after the age of 60 years (i.e., Austria, Belgium Denmark, Finland, France, Germany, Greece, Iceland, Ireland, Italy, Luxembourg, and Spain), whereas others recommend vaccination after the age of 65 (e.g., The Netherlands, Norway, Portugal, Sweden, Switzerland, and United Kingdom). 3 These different regulations, as well as the various existing incentives promoted by a few countries (especially the United Kingdom) explain the wide differences in influenza vaccine coverage rates observed in the population over 65 years of age in Europe. In 2008, nearly all European member states had coverage lower than the WHO goal of 75% to be achieved in 2010/2011 in the aged population and in individuals aged <65 with chronic conditions. 8 The vaccine uptake across EU target groups differs widely, ranging from 55% in Germany to 2% in Lithuania. 27 Moreover, it has been estimated than 60% of the whole EU population was noninfluenza-immunized. 28 Only two countries (The Netherlands and the United Kingdom) reached the 2010 WHO and EC goals for influenza vaccine coverage in subjects aged over 65 (Fig. 3). The observed vaccine coverage rate in at-risk adult groups aged below 65 is much lower than in the 65+ population, and even lower in the health-care worker (HCW) population. These data underline the need to target HCWs, including ancillary staff, to encourage influenza vaccine uptake. The low uptake is probably related to the fact that the influenza is not generally considered to be a disabling or life-threatening disease. However, it is a fact that in Europe 40,000–220,000 excess winter deaths are linked to seasonal influenza, mainly influenza by the virulence of the seasonal strain.
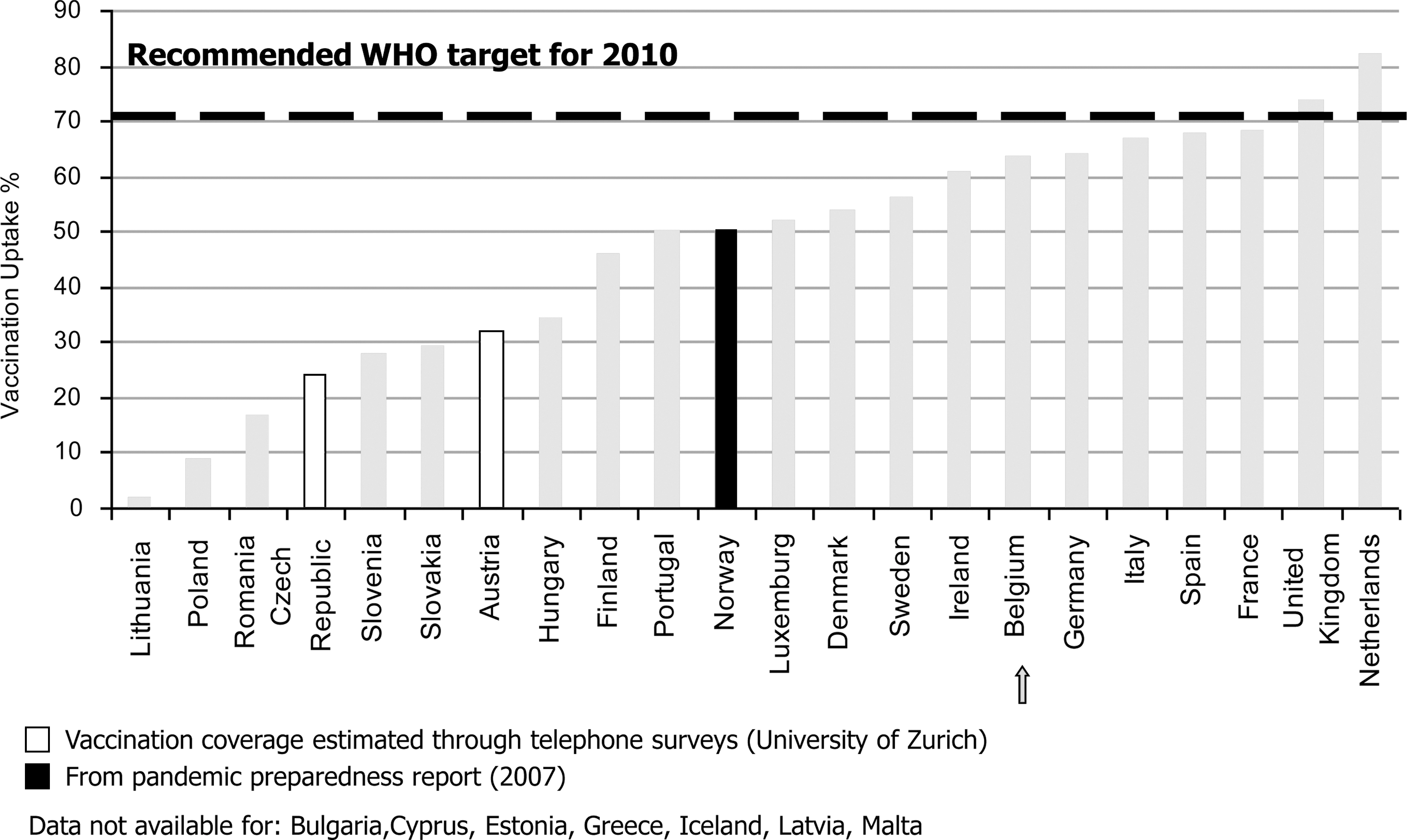
Vaccination coverate for seasonal influenza vaccine in 65+-year-old adults in European Union and European Economic Area countries (latest seasonal data available in spring 2008). Data from VENICE Survey and other sources, 2008, version 18 March 2008.
Influenza epidemics have also been associated with excess mortality from causes other than respiratory diseases. Cardiovascular mortality abruptly increases during influenza epidemics. Several studies have focused on the preventive effect of influenza vaccine in cardiovascular outcomes. In one population based-study among 342 cases versus 549 controls, influenza vaccine was associated with reduced risk of out-of-hospital primary cardiac arrest (odds ratio [OR] = 0.51; 95% confidence interval [CI], 0.33–0.79) after adjustment for demographic, clinical, and behavioral risk factors. 29 A significant benefit has also been observed in patients admitted for acute coronary syndromes. Gurfinkel et al. showed that the risk of death and ischemic events was significantly reduced during the first year following vaccination, and that this benefit was maintained during the second year if the patient was revaccinated. 30,31 Similarly, Ciszewski et al. in a randomized controlled trial conducted in 658 optimally treated patients with coronary artery disease (mean age 60 years) demonstrated that influenza vaccine improved the clinical course of the disease. The rate of 1-year coronary ischemic events was significantly reduced (OR = 0.54, 95% CI, 0.29–0.99). 32 Not only does vaccination prevent morbidity and mortality due to influenza-related complications and pneumococcal disease, but it also reduces costly hospitalizations and admissions to long-term care facilities. 33 Older adults who receive influenza vaccination are less likely to be admitted to hospital during the influenza season, and those who are admitted tend to have shorter hospital stays. Use of the pneumococcal vaccine also reduces hospital admissions. 34
Two further concerns deserve to be stressed. First, influenza infection is known to favor secondary bacterial respiratory tract infections. A recent reanalysis of autopsy pulmonary sections from patients who died during the 1918 influenza pandemic has raised numerous difficult questions concerning the respective roles of the viral strain virulence and bacterial reinfections. 35 In fact, the majority of deaths in the 1918 influenza pandemic were linked to pneumococcal (group A) and Staphylococcus aureus infections, as shown by the retrospective clinical analysis of 8,000 influenza cases diagnosed during the 1918 pandemic. 35,36
The second issue of major concern is the lower incidence of cardiovascular and neurovascular adverse events in influenza-vaccinated adults. 29 There are numerous randomized studies attesting to these facts. 30 –32 Indeed, these data led the American Heart Association to recommend influenza vaccination for secondary prevention of acute vascular events in all atherosclerotic patients. 37
The large body of evidence in favor of a beneficial effect of seasonal influenza vaccine emphasizes once again the importance of herd immunity. In a large Japanese retrospective analysis, it was shown that the mandatory vaccination program initiated in 1962 to vaccinate school children with the inactivated influenza vaccine significantly decreased excess mortality from seasonal influenza and invasive pneumococcal disease in adults and older adults. 38 Cessation of this mandatory school vaccine program in 1987 was followed by a new increase in community deaths from influenza and invasive pneumococcal disease. 38 This quasi-experimental demonstration of the efficacy of the child vaccine program on the health of community-dwelling adults underscores the major role of herd immunity. This concerns also HCWs, in whom low influenza vaccine uptake is truly nonunderstandable behavior. 39
Invasive pneumococcal disease (IVP)
Streptococcus pneumoniae vaccine recommendations vary from one European country to another. In most countries, vaccination is recommended in adults over the age of 65 and in populations at risk. However, in Poland for example, the recommendations are not age related, but rather disease related. Moreover, recommendations regarding boosters are not always consensual: for the over 65s, booster shots are recommended every 5 years in Finland and France, but every 6 years in certain counties of Sweden. They are only recommended every 5 years in Ireland, Switzerland, and the United Kingdom for at-risk populations (e.g., cigarette smokers; patients with chronic cardiovascular, pulmonary, liver, or renal diseases; patients suffering from diabetes, alcoholism, functional or asplenia, or from any immunocompromising conditions).
A recent appraisal study performed in three different European countries showed that even these inhomogeneous recommendations are not respected. 40 Pneumococcal vaccine coverage in the community is highest in the United Kingdom (21%) and lowest in Switzerland (9%). As recently demonstrated by a metaanalysis of 22 trials involving 101,507 participants, the currently available anti-pneumococcal vaccine does not appear to be effective in preventing presumptive pneumococcal pneumonia. 41 The pneumococcal vaccine is less effective in the oldest old as well as in the immune-compromised older adults. 42 –44 Moreover the duration of the protection decreases with the progression of the immune-senescence process. For these reasons pneumococcal vaccine has to be administrated in the early 60s.
Nonetheless, the nonrespect of pneumococcal vaccine recommendations explains the tremendous burden of invasive pneumococcal diseases in the Europe. Partial data collected in a few European countries mentioned the existence of 77,778 cases of IVP over the last 8 years. For example, 18,204 cases were notified in the United Kingdom over a period of only 3 years (2004, 2005, and 2006), 9,305 cases in Belgium between 1999 and 2005, 7,618 cases in Norway for the period 1999–2006, but no cases were notified in Italy, for reasons that remain unclear. 12 Thus, it can be seen that the burden of preventable infectious diseases remains very high at the beginning of this new century, despite the fact that vaccines exist to fight this disease, which concerns principally children and adults over the age of 65. 45,46 The importance of herd immunity is again evident in this situation. A recent large study from the United States showed that over the period 1998–2003, the introduction of a new 7-valent-conjugate pneumococcal vaccine for children not only significantly decreased the incidence of invasive pneumococcal disease in the young vaccinated population, but also in the old population, without any intervention. 47
Toward a Lifelong Vaccination Program to Limit the Burden of Vaccine-Preventable Infectious Diseases
Clearly, the under-use or total absence of diphtheria or measles vaccination in children is responsible for the onset of more severe forms of these diseases in young adults. 48,49 In addition, there is strong evidence that infant influenza vaccine 38 as well as the 7-valent pneumococcal vaccination in children beyond 5 years 47 significantly reduce the incidence of morbidity and mortality from seasonal influenza and invasive pneumococcal disease in adults over 65. Furthermore, it has been observed that influenza vaccination in HCWs reduced the incidence of the disease in hospitalized patients, and increasing rates of vaccination among family caregivers also reduced the incidence of influenza among the adults and children for whom they provide care. 50 Again, herd immunity is important in this situation to limit the spread of influenza. In this context, several arguments plead in favor of a “life course vaccination program.” 4 For these reasons, the EUGMS and IAGG-ER, the two main geriatric and gerontology societies in Europe, advocate the implementation of a lifelong vaccination program, 3,22 with a view to maintaining adequate vaccination status into adulthood and to achieve better vaccine coverage rates for a variety of VPDs.
In addition, because the effectiveness of vaccines is not only based on the vaccine match and circulating pathogens, but also on individual characteristics, it is currently acknowledged that the most crucial age at which to receive and better react to vaccines is the fifth to sixth decade of life, i.e., before the onset of immunosenescence. 51,23 For these reasons, the EUGMS and IAGG-ER propose to fill the adult vaccine gap by a new, adult-specific vaccine schedule starting at retirement age. Life expectancy at retirement is more than 2 decades in the majority of European countries, and can even exceed 4 to 5 decades in some individuals. In view of the burden of VPIDs in this population, it is evident that there is a need to harmonize vaccination programs in adults over 60 years to bridge the existing vaccine gap in this population. Application of the recent vaccination recommendations issued by the EUGMS and the IAGG-ER 2,3 would be a considerable step in the right direction.
Footnotes
Author Disclosure Statement
The authors have no conflict of interest to declare.