
Abstract
Cognitive reserve (CR), for which formal education represents a proxy index, has been claimed as a factor mitigating the clinical manifestations of Alzheimer disease (AD). The aim of this study was to assess the impact of formal education in modifying the relationship between cerebral grey matter (GM) damage and clinical manifestations in a large cohort of patients with AD or amnesic mild cognitive impairment (a-MCI).
We recruited 22 patients with AD and 23 with a-MCI, and we classified them in subjects with high (HEL) or low educational level (LEL). All patients underwent a neuropsychological assessment and magnetic resonance imaging (MRI) scanning at 3T. T1-weighted volumes were analyzed, using voxel-based morphometry, for GM investigation. A 1-year clinical follow-up was available for part of the a-MCI patients. There were no between-groups differences in clinical features, memory, and language functions. Conversely, HEL subjects performed better in all tests assessing visuo-spatial abilities. GM volumes of LEL compared with HEL patients were reduced in the supramarginal gyrus bilaterally and in the right posterior cingulate/precuneus and frontal opercular cortex. Conversely, HEL compared with LEL patients showed reduced GM volumes in the entorhinal cortices and temporal poles, regions typically affected by AD pathology. These results remained unchanged when including in the analysis of only patients with clinically proven AD (AD and a-MCI converters). This study suggests that CR produces selective GM changes that mitigate the clinical impact of AD. Moreover, it supports the idea that CR is based on several “brain reserves” rather than on a generalized increase of brain plasticity.
Introduction
Altogether these data suggest that at an individual level, there may be other factors that impact on different degrees of brain resilience to pathological damage. To account for these apparent inconsistencies between extent of brain damage and clinical manifestations, the concept of “reserves” has been introduced (for a review see ref. 1). So far, two different models of reserves have been proposed: (1) A passive model (brain reserve [BR]), which is based on quantifying brain size, neuronal amount, and number of synapses; and (2) an active model (cognitive reserve [CR]), which postulates the existence of brain mechanisms able to cope with cerebral damage. These mechanisms are believed to rely on pre-existing cognitive processes or to enlist compensatory processes. 1,7
It has been hypothesized that BR and/or CR may both modulate the clinical onset of AD. 1 Indeed, because AD results from a progressive accumulation of neuropathological lesions with a long period during which the clinical symptoms remain silent, 8,9 it is reasonable to hypothesize that a higher CR and/or BR may contribute to postponing the time point of inflection toward dementia. 1 In fact, subjects with a higher CR and/or BR require a more severe extent of AD pathology to manifest symptoms of cognitive decline. 1,10 –12
As clearly demonstrated in previous studies based on animal models, 13 –16 the development of BR and CR is highly correlated with the extent of environmental enrichment to which the animals are exposed. Although translating results from animal models to humans requires caution, and bearing in mind that education may also be interpreted as a proxy measure for inherited brain characteristics, it is reasonable to assume that education and lifestyle are the most important factors for developing CR and BR. 1,7 It has been consistently reported that although education does not prevent the onset of AD, it may provide protection against the expression of its clinical symptoms. 17 –19 When regional cerebral blood flow was compared in different groups of AD patients with the same degree of cognitive deterioration but different levels of education, it was observed that patients with a high level of education had a more severe deficit of parieto-temporal perfusion, indicating that AD pathology was more advanced in these subjects. 20 This observation supports the hypothesis that neurodegenerative signs associated with AD have fewer immediate repercussions in subjects with high educational levels. 21 –24 In fact, highly educated subjects become demented later than less educated subjects. 17 –19 Several studies support the contention that education has a protective effect against the clinical occurrence, or at least the detection, of AD. 22,23,25,26
It should be pointed out that the evolution of AD neuropathology is an independent process, and its impact on patients' clinical symptoms (AD syndrome) can be somehow modulated by external factors. Recently, neuroimaging studies have shown that the level of formal education is a relatively good estimate of CR in patients with dementia. 27,28 Using single-photon emission computerized tomography (SPECT), Borroni and co-workers identified an inverse correlation between educational level and rCBF in the medial and dorsolateral frontal cortex of patients with fronto-temporal dementia. 27 Consistently, Teipel and co-workers, using diffusion tensor magnetic resonance imaging (MRI), reported an association between microscopic measures of white matter integrity and BR capacity in both healthy individuals and patients with AD. 28
Voxel-based morphometry (VBM) is a spatially specific and unbiased method of analysis of MR images reflecting the regional gray matter (GM) volume at a voxel scale. 29,30 This is one of the most suitable techniques for assessing GM modifications in aging and dementia. 31 In patients with AD at different stages, VBM has shown patterns of GM abnormalities that fit well with both cognitive measures 31 and behavioral features. 32 –34 Due to its ability to assess not only group differences in regional GM volumes, but also associations between regional brain volumetrics and behavioral data, VBM seems to be a promising tool for assessing the potential role played by CR in patients with AD. Because formal education has been indicated as a positive predictor of age-associated cognitive decline, 21,23,24,35 we found it interesting to investigate the impact of formal education in modifying the relationship between GM tissue damage and clinical manifestations of dementia, by using VBM in a large cohort of patients with AD at different clinical stages. For this purpose we recruited either patients with AD or amnesic mild cognitive impairment (a-MCI) (a condition associated with an increased risk for developing AD), which is currently considered by most authors as a prodromal stage of AD. 36 Nevertheless, it should be mentioned that some a-MCI patients will not progress to dementia in a short time, and some of them will even revert to a cognitively normal profile.
Methods
Subjects
A cohort of 45 patients, 22 with a diagnosis of probable AD and 23 with single-domain a-MCI, were enrolled for this study. Patients were recruited consecutively from the specialist dementia clinics of Santa Lucia Foundation (Rome, Italy), “La Sapienza” University of Rome (Rome, Italy), and the Catholic University of Rome (Rome, Italy). The principal demographic and clinical characteristics of the studied subjects are summarized in Table 1.
One-way analysis of variance (ANOVA) or chi-squared; statistical threshold, p < 0.05.
a-MCI, Amnesic mild cognitive impairment; AD, Alzheimer disease; SD, standard deviation; N.S., not significant; HEL, group with high educational level; LEL, group with low educational level; MMSE, Mini- Mental State Examination; BPF, brain parenchymal fraction.
The diagnosis of probable AD was defined according to the clinical criteria established by the National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer's Disease and Related Disorders Association (NINCDS-ADRDA). 37
Patients with a-MCI were identified according to current criteria. 36,38,39 They had to report a subjective memory impairment corroborated by an assistant and confirmed by performances below the normality cutoff scores on at least one of the administered tests for episodic memory (see below), without fulfilling the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) 40 criteria for the diagnosis of dementia. They had to show a preservation of general cognitive functions, in the absence of impairment in cognitive domains other than memory. This criterion was confirmed by reporting normal scores at the Mini-Mental State Examination (MMSE) 41,42 (Italian normality cutoff score ≥23.8 42 and at all tests of the neuropsychological battery assessing cognitive functions other than episodic memory. Finally, the memory deficits observed in a-MCI patients had to result in no or in a very mild impact on their daily living activities, as confirmed by their total Clinical Dementia Rating score, 43 which could not exceed 0.5.
All recruited patients had to be right-handed, to reduce any potential source of variability due to hemispheric dominance. Major systemic, psychiatric, and other neurological illnesses were carefully investigated and excluded in all the studied subjects. Moreover, as explained below, subjects with signs of concomitant cerebral vascular disease (CVD) on conventional MRI scans were excluded because vascular pathology might be at least partially responsible for cognitive deficits and brain atrophy, making the diagnosis of MCI (on a neurodegenerative basis) or AD less plausible. As previously described, 44 subjects were excluded if they had either two or more hyperintense lesions with a diameter ≥10 mm or more than eight hyperintense lesions with a diameter between 5 and 9 mm on dual-echo MR images to minimize the risk of CVD.
The data presented here are part of a follow-up study, in which patients with a-MCI undergo a clinical and neuropsychological reassessment at 1-year intervals and are then reclassified as those who remain MCI and those who convert to dementia. So far, 12 out of 23 a-MCI patients completed their first follow-up. As explained below, the available follow-up data were used for additional VBM analyses based on the retrospective identification of a-MCI converters.
Local Ethical Committee approval and written informed consent (either from the subjects or from their responsible guardians if incapable) were obtained before study initiation.
Classification criteria to define the level of cognitive reserve
To evaluate the impact of CR on clinical manifestation of AD, we divided our patients' cohort on the basis of their level of formal education. Mean (μ) and standard deviation (σ) of years of formal education were first estimated across the sample. Then, for each subject, a z-score representative of the individual level of formal education was calculated as follows: z = (x − μ)/σ, where x is the raw score (years of formal education) to be standardized.
Within such a distribution, all individuals reporting a z-score ≤0 were considered as belonging to the group of patients with low educational level (LEL; n = 24). Conversely, individuals with a z-score >0 were considered as belonging to the group of patients with high educational level (HEL; n = 21). As reported in Table 1, the LEL group included 13 patients with AD and 11 with a-MCI, whereas the HEL group included 9 patients with AD and 12 with a-MCI.
Neuropsychological assessment
All recruited patients (AD and a-MCI) underwent an extensive neuropsychological battery (Table 2), including the following tests: Verbal episodic long-term memory, 15-Word List (Immediate and 15-min Delayed recall) 45 ; Short Story Test (Immediate and 20-min Delayed recall) 46 ; visuo-spatial episodic long-term memory, Complex Rey's Figure (Immediate and 20-min Delayed recall) 46 ; short-term memory, Digit span and the Corsi Block Tapping task 47 ; executive functions, Phonological Word Fluency 45 and Modified Card Sorting Test 48 ; language, Naming objects subtest of the BADA (“Batteria per l'Analisi dei Deficit Afasici”, Italian for “Battery for the analysis of aphasic deficits”) 49 ; Reasoning, Raven's Coloured Progressive Matrices 45 ; constructional praxis, copy of simple drawings with and without landmarks 45 and copy of Complex Rey's Figure 46 ; general cognitive efficiency, MMSE. 41,42
For each studied group, mean (SD) scores obtained in each administered test are reported. For the purposes of the current study, scores from all employed tests were not adjusted for age and education.
One-way analysis of variance (ANOVA); statistical threshold, p < 0.05.
HEL, Group with high educational level; LEL, group with low educational level; N.S., not significant.
Given the purposes of the current study, scores from all employed tests were not adjusted for age and education. One-way analysis of variance (ANOVA) was used to assess between groups differences (statistical threshold, p < 0.05).
MRI acquisition
All subjects underwent an MRI examination at 3T (Magnetom Allegra, Siemens, Erlangen, Germany), including the following acquisitions: (1) Dual-echo turbo spin echo (TSE) (repetition time [TR] = 6,190 msec, echo time [TE] = 12/109 msec); (2) fast-FLAIR (TR =8,170 msec, TE =96 msec, TI = 2,100 msec); (3) 3D Modified Driven Equilibrium Fourier Transform (MDEFT) scan (TR =1,338 msec, TE =2,4 msec, matrix = 256 × 224, n. slices = 176, thickness = 1 mm). According to the inclusion criteria, TSE and FLAIR scans were reviewed to exclude the presence of remarkable macroscopic brain abnormalities, as previously described. 44
VBM analysis and statistics
None of the T1-weighted (MDEFT) volumes were affected by macroscopic artifacts, as assessed by visual examination. T1-weighted volumes were preprocessed using the VBM protocol
50
implemented in SPM8 (
Statistical analysis was performed on smoothed GM maps within the framework of the general linear model. We used an ANOVA full factorial design, with a two-level factor to model the groups (HEL and LEL), and with diagnosis (AD or a-MCI), brain parenchymal fraction (BPF) (obtained by adding up WM volume + GM volume and then dividing the results by WM volume + GM volume + CSF volume), and MMSE as nuisance covariates to adjust for potential confounds. p values were considered significant if lower than 0.005. In regions of significant GM changes between LEL and HEL patients, we further investigated potential correlations between the mean GM density (extracted subject by subject) and those neuropsychological scores where the two groups performed differently. Correlations were estimated by the Pearson coefficient (p < 0.05).
According to current diagnostic criteria 36,38,39 and guidelines for the diagnosis of dementia, 51 well-selected patients with a-MCI should be considered as in a prodromal stage of AD. Nevertheless, it has also been reported that a proportion of a-MCI patients do not convert to dementia in a short time. 52,53 To exclude that the presence of a-MCI nonconverters might have biased our VBM results, thus making questionable any conclusion on AD, we repeated the analysis (ANOVA full factorial design, with same level factors [HEL and LEL] and covariates) by including only patients with AD and a-MCI converters, as assessed by clinical and neuropsychological follow up at 1-year interval. Again, p values were considered significant if lower than 0.005.
Results
When considering all patients according to their diagnosis of AD or a-MCI, as expected, the former group reported significantly lower MMSE scores than the latter (Table 1A). According to selection criteria, patients with a-MCI (single domain) reported abnormal scores only at tests for memory functions, whereas AD patients showed a widespread impairment in all cognitive domains (data not shown). Again, as expected, BPF, which is a measure of global brain volumetrics, was significantly lower in AD as compared with a-MCI patients (Table 1A). Moreover, since the beginning of this research project, 12 a-MCI patients were clinically reassessed at a 1-year interval. Seven out of 12 remained stable (58.3%) and 5 out of 12 had converted to dementia (41.6%).
In comparing LEL with HEL patients, their mean years of formal education were significantly different by definition. Conversely, the two groups were homogeneous with respect to proportion of diagnoses (AD or a-MCI), age, gender, MMSE score, and BPF (Table 1B).
Neuropsychological assessment
Neuropsychological data for each considered group of subjects (patients with HEL and patients with LEL) are summarized in Table 2. HEL and LEL patients did not show any significant difference in scores reported at tests exploring memory and language functions. Conversely, HEL patients performed significantly better than those with LEL in most visuo-spatial tests (executive functions, constructional praxis, and reasoning).
VBM analysis group comparisons
Between-group differences are summarized in Table 3 and illustrated in Fig. 1. Patients with HEL compared with patients with LEL showed lower GM volumes in the entorhinal cortex bilaterally and in the left temporal pole. Conversely, patients with LEL compared with those with HEL showed reduced GM volumes in the supramarginal gyrus bilaterally and in the right posterior cingulate gyrus, precuneus, and frontal operculum.
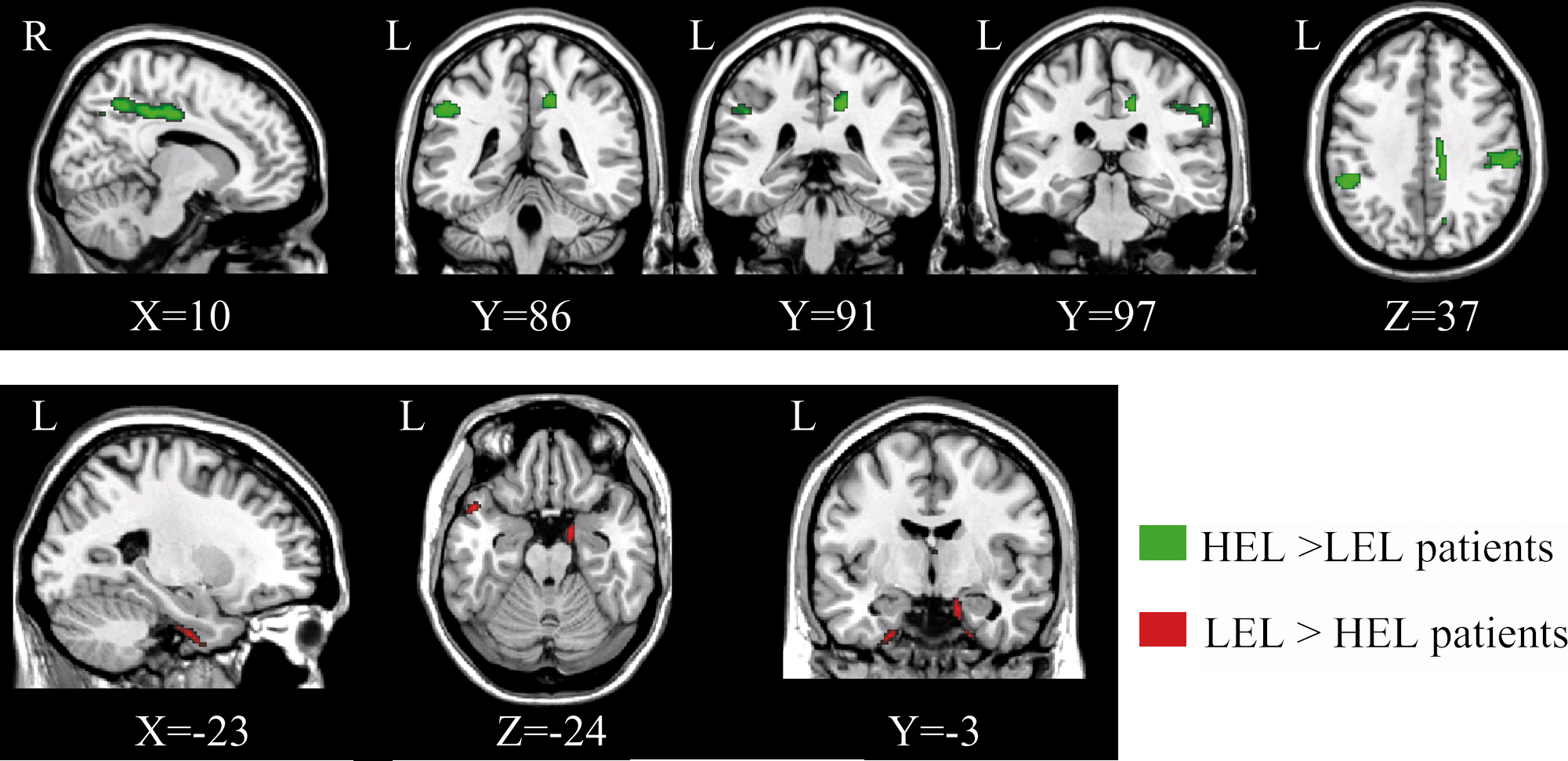
Regional changes in grey matter (GM) volumes between patients with Alzheimer disease (AD) at different clinical stages (amnesic mild cognitive impairment or fully developed dementia) divided in those with an higher (HEL) and those with a lower educational level (LEL). HEL patients compared with LEL patients showed increased GM volumes in the supramarginal gyrus bilaterally and in the right posterior cingulate/precuneus and frontal opercular cortex (areas shown in green, top panel). In contrast, HEL patients compared with LEL patients showed reduced GM volumes in the entorhinal cortex and in the temporal pole bilaterally (areas shown in red, bottom panel). The statistical images are overlaid onto a T1-weighted template image. For the purposes of illustration, the statistical threshold was set to an uncorrected p < 0.01. See text for further details.
The size of each region is expressed in number of voxels. This analysis includes all patients recruited at baseline. See text for further details.
GM, Grey matter; HEL, high educational level; LEL, low educational level; R, right; L, left.
Correlations between regional GM volumes and cognitive measures
Scores obtained by all patients at the Raven's Coloured Progressive Matrices were significantly correlated with the GM density in the right (r = 0.35, p = 0.02) and left supramarginal gyrus (r = 0.30, p = 0.05) (Fig. 2) and in the right precuneus (r = 0.43, p = 0.003).

Associations between grey matter (GM) density in the supramarginal gyri and scores obtained using the Raven's Coloured Progressive Matrices, in which patients with higher educational level (HEL) performed significantly better than those with lower educational level (LEL). See text for further details.
Further significant correlations were found between scores obtained at the “Copy of drawings with landmarks” test and GM density in the right supramarginal gyrus (r = 0.39, p = 0.02), and between scores obtained at the Modified Card Sorting Test and GM density in the right precuneus (r = 0.37, p = 0.05).
Comparison between subjects with HEL and LEL in the subgroup of patients with clinically proven AD
This group included all recruited patients with AD (9 with HEL and 13 with LEL) and 5 a-MCI converters (2 with HEL and 3 with LEL). Between-group differences are summarized in Table 4. Patients with LEL compared with those with HEL (Table 4A) showed lower GM volumes in the supramarginal and anterior cingulate gyri bilaterally, in the right posterior cingulate gyrus, and in the right middle and in the left inferior frontal gyri. Conversely, HEL patients showed lower GM volumes than those with LEL in the right entorhinal cortex and temporal pole, and in the left fusiform gyrus (Table 4B). These patterns of group differences are fully consistent with those found in the analysis including all recruited patients.
The size of each region is expressed in number of voxels. This analysis was performed considering only patients with clinically defined Alzheimer disease (AD). Only those amnesic mild cognitive impairment (a-MCI) patients who converted to AD at the 1-year follow up were included in the statistical model. See text for further details.
GM, Grey matter; HEL, patients with high educational level; LEL, patients with low educational level; R, right; L, left; B, bilateral; Inf, inferior; Mid, middle.
Discussion
The aim of the present work was to assess, by using VBM, the impact of formal education on the brain tissue of patients with AD. Formal education is indeed considered as a proxy for CR and is indicated as a positive predictor of cognitive decline on the clinical manifestations of AD. The recruited patients suffered from either a-MCI or fully developed AD. A-MCI is widely regarded as a prodromal AD state, 36,38,39,51 although, in some studies, a proportion of patients with a-MCI has been reported not to convert to AD in a short time. 52,53 Nevertheless, the conversion rate observed in our partial follow-up is consistent with that expected in MCI populations. In the current study, we decided to include patients with a-MCI to add faceting to our sample, in terms of cognitive performance as well as of brain tissue involvement.
The two groups of HEL and LEL patients were not significantly different in any demographic and clinical characteristic, as well as in global measures of cognitive decline. In the two groups of patients, the ratio of a-MCI/AD as well as the BPF, which is an index of global brain atrophy, was consistently similar. Moreover, the homogeneous distribution in BPF between HEL and LEL groups suggests that CR (at least that expressed by formal education) does not have a strong impact on gross brain anatomy. Conversely, CR appears to be significantly related to local structural changes of brain tissue. LEL and HEL patients exhibited a similar impairment in long- and short-term memory functions, as well as a similar preservation of verbal abilities. On one hand, memory deficits are consistent with the diagnosis of a-MCI or AD, although, LEL and HEL groups showed a different pattern of GM volumes in the entorhinal cortex. On the other hand, the preservation of basic verbal abilities (as assessed by tests exploring verbal production) is consistent with previous literature. In fact, language abilities are resilient against normal aging 54 and remain relatively preserved until the most advanced stages of AD. 55 The preservation of basic language abilities in both HEL and LEL groups is also corroborated by the absence of any significant group difference in GM volumes in cortical regions of the left hemisphere known to be implicated in language.
Interestingly, HEL patients had better preserved abilities than those with LEL in visuo-spatial abilities, such as logical deductive reasoning, constructional praxis, and executive functions. These differences in neuropsychological performances between groups fit well with VBM results, showing greater GM volumes in the bilateral supramarginal gyrus, right posterior cingulate gyrus, frontal operculum, and precuneus of patients with HEL as compared with those with LEL. Notably, just these associative brain regions are implicated in highly demanding cognitive functions, 56 which are in turn associated with hemispheric asymmetry. 57 Furthermore, the increased GM volumes observed in HEL compared with LEL patients had a prominent rightward distribution, and significant associations were found between GM density in these association cortices and patients' performances at tests for complex visuospatial abilities.
The main finding of the present study is that CR development is associated with specific and well-localized GM changes across the brain. In comparison with LEL patients, HEL patients exhibited significantly higher GM volumes in associative regions and more marked GM atrophy in the entorhinal cortices, which are considered the earliest target for AD pathology. 4,5 Using this perspective, we may advance that the higher volumes of associative cortices render the brains of HEL subjects more resilient to the early stages of AD pathology, thus requiring more severe damage to the medial temporal lobes for eliciting clinical manifestations of similar severity.
This interpretation is consistent with a previous pathological study, showing a delay of inflection toward dementia in patients with higher compared with those with lower CR. 6 Critically, the relationship between higher BR, of which the increased GM volumes in the associative brain areas may represent an index of occurrence, and higher CR, is supported by the significant correlations between GM densities in specific regions and neuropsychological performances in test tapping functions mediated by those specific circuits. We hypothesize that CR accumulated by patients with HEL during their educationally enriched life span resulted in local GM changes, probably reflecting the enhanced neuroplastic properties developed in conditions of cognitive enrichment. These mechanisms have already been demonstrated in animal models. 13 In fact, the exposure to an enriched environment induces an increased neurogenesis and brain volume in mice. 13,14 Furthermore, behavioral stimulation has been shown to increase neuroplasticity in the hippocampus of transgenic mice with AD. 15,16
When considering a-MCI patients as an early AD stage, it remains to be proven whether they will eventually convert to dementia in a short time. In principle, the presence of a-MCI nonconverters might preclude any general conclusion on AD. To reduce this potential bias, we repeated the VBM analysis by including only subjects with clinically proven AD (AD patients and MCI converters). Between-group contrasts (HEL vs. LEL) confirmed, in both directions, the results obtained using the original sample of patients. This suggests that our inference about the impact of CR on pathophysiological aspects of AD is plausible. More generally, VBM findings of the present study support, by anatomical definition of regional brain tissue damage/preservation, previous evidence that patients with brain damage and HEL cope significantly better than those with LEL in performing cognitive tasks. 1,7
A caveat of the current study is the use of statistical threshold at an uncorrected level for VBM analyses. However, our findings were obtained on a relatively small sample size of clinically homogeneous patients, without assuming any a priori hypothesis on the anatomical localization of GM changes. It is noteworthy that regional GM findings that we found in the present research were not only obtained by between-group comparisons, but were also supported by associations with neuropsychological measures in the same subjects. This investigation, although preliminary to further studies on larger populations, appears significant because it provides an interesting approach for correlating structural (regional GM volumes) and behavioral (neuropsychological measures) measures.
Footnotes
Acknowledgments
This project was supported by grants of the Italian Ministry of Health and of the Italian Ministry of University and Research.
Author Disclosure Statement
None of the authors has any actual or potential conflict of interest, including any financial, personal, or other relationship with other people or organizations within 3 years of beginning the work submitted that could inappropriately influence (bias) their work. The study was approved by the local ethics committee before initiation. All subjects gave written informed consent before taking part in the study.