
Abstract
Data on the relationship between aging, chemotherapy, and risk for venous thromboembolism (VTE) are controversial. We sought to evaluate the risk of chemotherapy-associated VTE in young to middle-aged (YMA) and elderly cancer patients and to analyze the VTE-free survival time in both groups. Patients with histologically confirmed diagnosis of solid malignancy receiving any type of systemic chemotherapy, no clinical diagnosis of VTE before chemotherapy initiation, and Eastern Cooperative Oncology Group (ECOG) performance status (PS) ≤2 were enrolled in this study. Of the 486 consecutive patients included in the study, 380 (78%) were classified as YMA (≤70 years of age) and 106 (22%) as elderly (>70 years of age). At a median follow-up of 1 year, the incidence of VTE events was almost two-fold greater in elderly than in YMA (11% vs. 6%). Age (≤70 years vs. >70 years (hazard ratio [HR], 2.42; 95% confidence interval [CI] 1.15–5.06; p=0.020), ECOG-PS (HR, 6.54; 95% CI 3.10–13.8; p<0.0001), and platinum-based chemotherapy (HR, 2.46; 95% CI 1.06–5.69; p=0.035) were independent risk factors for VTE. In the elderly subset, a trend toward an increased risk of VTE in patients receiving a platinum-based chemotherapy when compared with a non-platinum-containing regimen was observed (15% vs. 9.1%). The Kaplan–Meier analysis showed that elderly patients had a significantly shorter VTE-free survival time compared with younger cancer patients (log-rank test=2.0; p=0.045). Our study reports an increase incidence of VTE in elderly cancer patients treated with chemotherapy compared with the younger group, suggesting that aging is one of the most important risk factors for VTE. On the basis of the results of this study, we believe that a validated predictive model including age, ECOG-PS, and type of chemotherapy (platinum- vs. non-platinum containing regimen) would enable clinicians to target thromboprophylaxis to those patients considered to be at greatest risk.
Introduction
To date, the biological and clinical interactions between cancer and age are not fully understood and may provide some clues to future preventive strategies of cancer-related complications, such as VTE. The increased risk for VTE in patients with cancer treated with chemotherapy has been explained, at least in part, with an activation of hemostasis, occurring via induction of pro-coagulant activity, which may increase the risk for pro-thrombotic state. 8 These mechanisms may be exacerbated in the elderly who have laboratory signs of clotting activation per se, possibly related to various co-morbidities. 9 Thus, the management of thrombosis in elderly cancer patients is a relevant and common clinical problem, but studies specifically addressing this are nearly completely lacking and controversial. Khorana et al. 10 recently developed and validated a model for predicting chemotherapy-associated VTE using baseline clinical and laboratory variables. In contrast to previous reports, 11,12 in this analysis older age (>65 years old) and stage of disease were not associated with VTE.
Better understanding of the relationship between chemotherapy, aging, and risk for VTE may help us in developing new anti-thrombotic preventive strategies in elderly patients with cancer. In a previous study, we investigated the potential role of anti-oxidant supplementation options as a possible strategy to reduce the cardiovascular toxicity effects of a platinum-based chemotherapy in the elderly. 13 In the present study, we sought to evaluate the risk of chemotherapy-associated VTE in young to middle-aged (YMA) (≤70 years of age) and elderly (>70 years of age) cancer patients. Secondary end points included an analysis of the VTE-free survival time in both YMA and elderly groups and an assessment of the potential predictive and/or risk factors leading to a VTE event during chemotherapy.
Patients and Methods
Study population
A single-center, retrospective cohort study on the risk of chemotherapy-associated VTE in elderly cancer patients (>70 years of age) was conducted on patients admitted to the Medical Oncology Unit of the Tor Vergata Clinical Center, University of Rome “Tor Vergata,” from October, 2006, to February, 2012. Adult patients (age ≥18 years) with histologically confirmed diagnosis of solid malignancy receiving any type of systemic chemotherapy in the neo-adjuvant, adjuvant, or metastatic setting were eligible. Patients were required to have no clinical diagnosis of VTE including DVT and PE before the start of chemotherapy. Other inclusion criteria were: Eastern Cooperative Oncology Group (ECOG) performance status (PS) ≤2 14 ; presence of routine blood work in our database providing bilirubin, creatinine, platelets, white blood cells, hemoglobin, and D-dimer blood levels; and adequate follow-up for at least 1 year. Exclusion criteria were: Impaired liver (bilirubin level >1.5 mg/dL) or renal (creatinine level >1.5 mg/dL) function; evidence of brain metastases, including leptomeningeal involvement at diagnosis; major surgery or significant traumatic injuries within 4 weeks prior to enrollment; therapeutic doses of any heparin before enrollment; or concomitant treatment with anti-coagulant or anti-platelet drugs. No patient received prophylactic treatment with any anti-coagulant drug after chemotherapy start. No patient underwent surgery during follow-up, nor was admitted to clinic for acute medical illness requiring thromboprophylaxis. By searching in our electronic clinical database, a total of 549 consecutive patients were identified and analyzed retrospectively. After a case-by-case non-blinded review, 63 patients (49 assigned to the YMA group and 14 to the elderly group) did not meet the inclusion criteria and were deemed ineligible (20 patients received concomitant or prophylactic treatments with anti-coagulant or anti-platelet drugs, 13 patients underwent surgery during follow-up, 11 patients had inadequate follow-up, 8 patients had impaired liver or renal function, 5 patients had clinical diagnosis of VTE before chemotherapy initiation, 5 patients had brain metastases, and 1 patient had a traumatic injuries within 4 weeks prior to enrollment). We report here the outcome among 486 consecutive patients. The study was approved by the University of Tor Vergata Institutional Review Boards. Written informed consent was obtained from each subject, and the study was performed in accordance with the principles embodied in the Declaration of Helsinki.
Data collection
An electronic medical record review was performed for all patients included in this study for 1 year from chemotherapy initiation. Data collection included demographic data, body mass index (BMI), cancer type, stage, ECOG-PS, chemotherapy setting, use of bevacizumab or anti-tyrosine kinase inhibitors (anti-TKI), erythropoietin, prophylactic granulocyte colony-stimulating factor (G-CSF), corticosteroids, pre-treatment hematology, chemistry and coagulation studies (bilirubin, serum creatinine, platelets, white blood cells, hemoglobin, and D-dimer blood levels), Khorana score, 10 type and duration of chemotherapy, date of diagnosis and localization of VTE events, and date and cause of death. VTE was defined as any upper or lower extremity DVT or PE, radiologically diagnosed by Doppler ultrasonography (USG) or computerized tomography (CT). 1 Both symptomatic and/or asymptomatic VTE events were considered in our analysis. The time to VTE was measured from the date of chemotherapy initiation to the date of diagnosis of VTE.
Statistical analysis
Differences in baseline characteristics between YMA and elderly patients were tested for statistical significance using the two-tailed Fisher exact test for categorical data and the Student-t test or the Mann–Whitney U-test for continuous variables. A Cox proportional hazard model was used to estimate hazard ratios (HR) for VTE. The HRs were adjusted for gender, age, site of primary tumor, metastasis, ECOG-PS, Khorana score, use of bevacizumab or anti-TKI, prophylactic G-CSF, and corticosteroids. A Kaplan–Meier analysis of VTE-free survival time in solid cancer patients undergoing chemotherapy and categorized on the basis of age was also performed, and the groups were compared for statistical differences with the log-rank test. Patients were censored at time of event, at time of death, or after 1 year of follow-up, whichever came first. Calculations were performed using a computer software package (Statistica 8.0, StatSoft Inc., Tulsa, OK) or free web-based applications (
Results
Patients' characteristics
Of the 486 patients included in the study, 380 (78%) were classified as YMA (≤70 years of age) and 106 (22%) as elderly (>70 years of age). Mean ages for YMA and elderly patients were 57±9 years and 75±3 years, respectively. In the YMA group, there were significantly more female patients than males (60% vs. 33%, p<0.0001, respectively). All patient characteristics with VTE are summarized in Table 1. No differences between the two groups were found in performance status, BMI, time to event, and in the use of additional drugs (such as erythropoietin, bevacizumab, and G-CSF). At a median follow-up of 1 year, the incidence of VTE events was almost two-fold greater in elderly than in YMA (11% vs. 6%). Interestingly, a significant higher intermediate, but not high, Khorana class of risk was observed in the older patients (56% vs. 36%). Blood levels of bilirubin, creatinine, platelets, white blood cells, hemoglobin, and D-dimer were also evaluated before the start of chemotherapy. The results are summarized in Table 1. No differences were observed between YMA and elderly patients except for higher creatinine levels in patients older than 70 years (0.90 mg/dL vs. 0.78 mg/dL, p=0.0001). A summary list of anti-cancer agents administered in the whole population and in the elderly is reported in Table 2.
For Laboratory parameters all values are expressed as median and interquartile ranges (IQR); p values calculated by the Mann–Whitney U-test.
Student t-test.
Mann–Whitney U-test; two-tailed Fisher exact test for categorical variables.
YMA, Young to middle aged; SD, standard deviation; NSCLC, non-small cell lung cancer; ECOG, Oncology Group; BMI, body mass index; EPO, erythropoietin; G-CSF, granulocyte colony-stimulating factor.
VTE–free survival time analysis
A multivariate analysis was performed using the Cox proportional hazards model to assess a potential association between different individual variables and VTE development (Table 3). The results showed that age (≤70 years vs. >70 years; HR, 2.43; 95% confidence interval [CI] 1.16–5.09; p=0.019), ECOG-PS (HR, 6.63; 95% CI 3.13–14.0; p<0.0001), and platinum-based chemotherapy (HR, 2.51; 95% CI 1.08–5.83; p=0.033) were independent risk factors for VTE. On the other hand, gender (male vs. female), site of primary tumor (colorectal, gastric, pancreas, non-small cell lung cancer [NSCLC], kidney, breast, and prostate), presence of metastatic disease, D-dimer levels, class of risk according to Khorana, use of gemcitabine, use of bevacizumab or anti-TKI, prophylactic G-CSF, or corticosteroids did not correlate with an increased risk of VTE. During 1 year of follow-up, VTE was diagnosed in a total of 33 patients (6.8%). The median time to event (mTE) from chemotherapy initiation to the diagnosis of VTE was 163 days for the entire cohort. According to age groups, VTE was observed in 21 patients (6%) in the YMA and 12 patients (11%) in the elderly, with a mTE of 203 days and 87 days, respectively. In the YMA group, 8 patients (38%) had PE, 6 patients (29%) lower-extremity DVT, 2 patients (9%) superior vena cava thrombosis, 2 patients (9%) subclavian vein thrombosis, 1 patient (5%) upper-extremity DVT, 1 patient (5%) common iliac vein thrombosis, and 1 patient (5%) renal vein thrombosis. In the group of elderly patients, 3 (25%) developed PE, 7 (58%) lower-extremity DVT, and 2 patients (17%) subclavian vein thrombosis. Among the YMA patients with a VTE event, 11 (52%) had a diagnosis of colorectal cancer, 5 (24%) NSCLC, 3 (14%) breast cancer, 1 (5%) kidney cancer, and 1 (5%) stomach cancer. In the elderly, colorectal cancer accounted for 42% (5 patients), NSCLC for 25% (3 patients), prostate cancer for 17% (2 patients), pancreatic cancer for 8% (1 patient), and stomach cancer for 8% (1 patient) of VTE events. Metastatic disease was present in 15 patients (71%) in the YMA patients and in 8 patients (67%) in the elderly. Two patients (10%) and none received neo-adjuvant chemotherapy regimen in YMA and elderly arms, whereas 4 patients (19%) and 4 patients (33%) had adjuvant chemotherapy in both groups, respectively. The Kaplan–Meier analysis (Fig. 1) showed that patients older than 70 years had a significantly shorter VTE-free survival time compared with younger cancer patients (log-rank test=2.0; p=0.045). Moreover, an analysis by chemotherapy treatment was performed among elderly patients: 40 out of 106 subjects received a platinum-based (i.e., cisplatin, oxaliplatin, or carboplatin) chemotherapy, whereas a non-platinum-based chemotherapy was administered in the remaining 66 patients. Six VTE events occurred in each group during the observational period, 15.0% in the platinum-based chemotherapy group vs. 9.1% in the non-platinum-based chemotherapy, respectively (HR, 2.42; 95% CI 0.71–8.31; p=0.159).
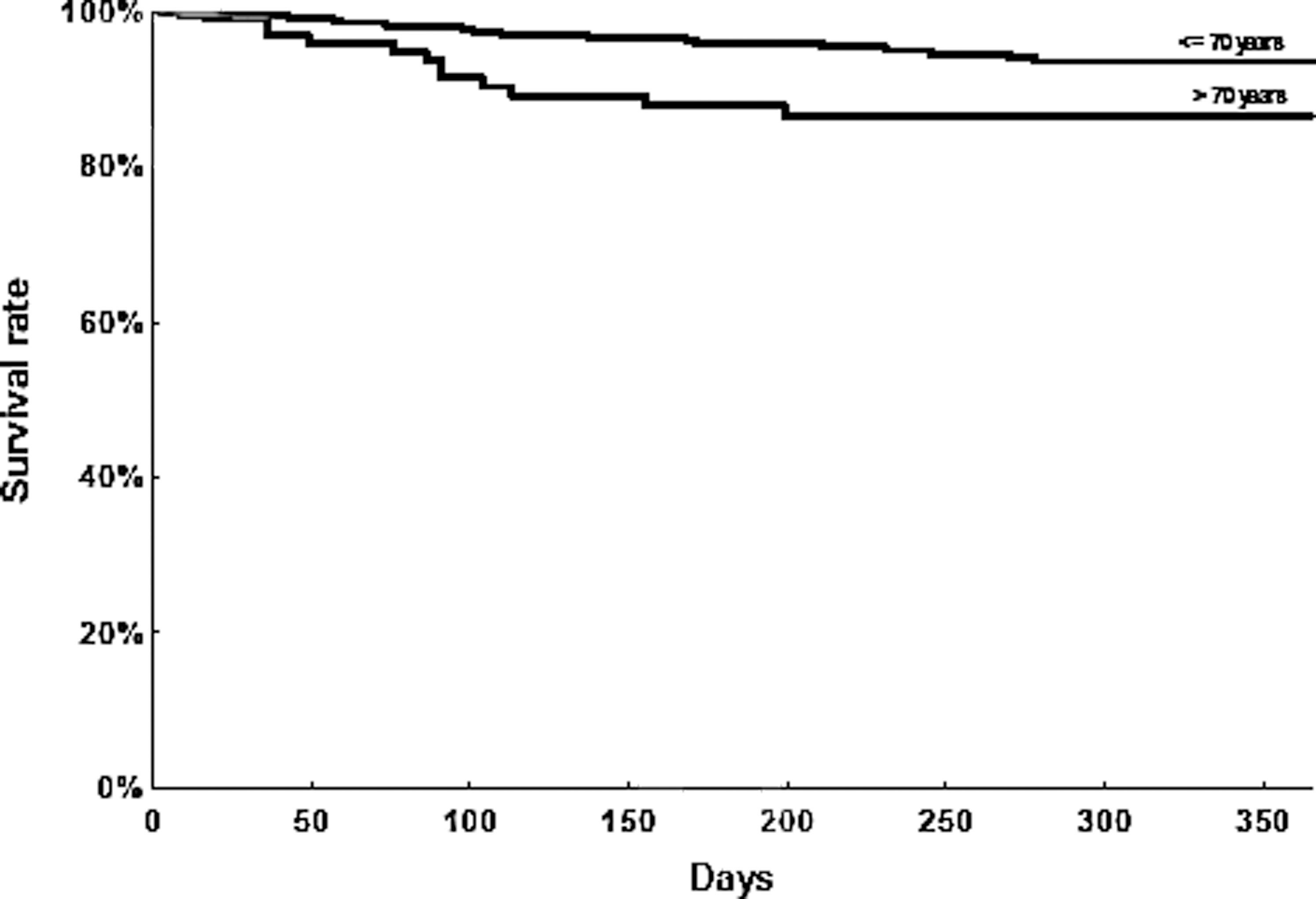
Kaplan–Meier Analysis of venous thromboembolism (VTE)-free survival time in solid cancer patients undergoing chemotherapy and categorized on the basis of age. Log rank test=2.0; p=0.045.
Categorized on a diagnostic cutoff of 280 ng/mL. Numbers in parentheses represent percentages.
VTE, venous thromboembolism; HR, hazard ratio; CI, confidence interval; NSCLC, non-small cell lung cancer; ECOG-PS, Eastern Cooperative Oncology Group performance status; anti-TKI, anti-tyrosine kinase inhibitors; G-CSF, granulocyte colony-stimulating factor.
Discussion
In a cohort population of a total of 486 patients with different types of solid cancer, treated with any type of systemic chemotherapy, we found a greater incidence of VTE in the elderly cancer patients. Age was an independent risk factor for VTE, and similar results were found for a high ECOG-PS score and the use of a platinum-based chemotherapy. Moreover, during 1 year of follow-up, we found that elderly patients had a significantly shorter VTE-free survival time compared with younger cancer patients.
Our results are in agreement with previous data that demonstrated an interaction between cancer and older age as risk factors for VTE. The MEDENOX (Prophylaxis in Medical Patients with Enoxaparin) study, conducted in 1,102 acutely ill, immobilized general medical patients, showed how age older than 75 years, cancer, and a history of VTE were statistically significantly associated with an increased VTE risk. 15 The Medicare Provider Analysis and Review Record (MEDPAR) database was used to analyze the association of malignancy and non-malignant disease with an initial episode of VTE, recurrent VTE, and related mortality in 7,238 cancer patients older than 65 years. 16 The mTE for VTE was 183 days, close to the mTE reported in our dataset (163 days), and the percentage of patients with VTE at the initial hospitalization was higher for those with cancer compared with those with non-malignant disease. Moreover, among those patients with VTE and cancer, the probability of death during the follow-up was greater than among those with VTE and no cancer. In this study, tumors of the ovary, pancreas, and central nervous system were most commonly associated with VTE. In our analysis, the type of tumors occurring most commonly in the elderly groups were colorectal and NSCLC. This discrepancy may be easily explained with the heterogeneity typical of the general cancer population comprising newly diagnosed patients, those receiving active therapy, hospitalized patients, and those receiving end-of-life care.
The role played by chemotherapy in increasing the risk of VTE has been previously investigated. 17 We further explored this role by evaluating the impact of age on the risk for VTE in patients treated with chemotherapy. The results here reported are in agreement with those found in a prospective, multicenter observational study from Awareness of Neutropenia in Cancer (ANC) Study Group Registry, showing an increased incidence of VTE among 3,003 patients with an average age of 60 years and treated with at least one cycle of chemotherapy. 18 This incidence varied significantly by site of cancer, with highest rates in gastrointestinal and lung cancer, similar to our results. Moreover, in that study, in accord with our findings, patients with ECOG-PS of 2 or greater had a trend toward an increased frequency of VTE. A geriatric oncology study tried to validate a Comprehensive Geriatric Assessment with the scope to revise the ECOG-PS for better adherence of elderly cancer patients. 19 However, in our analysis, we used the original definition of ECOG-PS and applied it in the two arms of the study.
In previous studies, an increase in mortality VTE-related in the elderly has been shown. In 644 elderly patients from the prospective SWIss Venous ThromboEmbolism Registry (SWIVTER), the overall in-hospital mortality rate for VTE was 6.6% in the elderly versus 3.2% in the younger patients (p=0.033), suggesting that the elderly had more serious VTE than younger patients. 20 Recently, a retrospective study using Surveillance, Epidemiology and End Results (SEER) Medicare data demonstrated how diagnosis of VTE significantly reduced survival rates for elderly patients with stage III colon cancer and further reduced survival rates for patients treated with chemotherapy. 21
Aging is a natural process leading to a decline in physical and possible mental functions. These changes predispose elderly subjects to develop diseases such as cancer. Therefore, the senescence per se may, at least in part, explain the greater incidence of VTE accidents in patients treated with chemotherapy and the increase in VTE-related mortality. The decline in drug metabolism and changes in disposition in elderly compared with younger people is well established. 22 The doses of chemotherapy are usually adjusted for age; however, aging may impact with an increase in the side effects of the therapy, as can be demonstrated by the significant difference in creatinine between YMA and elderly patients that we found in our analysis.
Current guidelines do not recommend VTE prophylaxis for cancer patients, 23 because the majority of these patients do not develop VTE, and because the use of anti-coagulants in cancer patients has been associated with an increased risk of bleeding complications. 24 The ability of the clinician would be to stratify and identify risk that will allow an appropriate use of VTE prophylaxis only in patients at highest risk. On the basis of our findings, we suggest that age, for its characteristic, is one of the most important risk factors to evaluate VTE prophylaxis in patients treated with chemotherapy. However, this is an open debate in the scientific community. Indeed, although the concept of thromboprophylaxis has been supported by early reports of the successful use of low-molecular-weight heparin (LMWH), in combination with chemotherapy to reduce VTE incidence in patients with advanced pancreatic carcinoma 25 or breast cancer, 26 with the exception of the PROTECHT study, 27 there are no data yet that define clearly the indication for LMWH for at-risk patients.
In this context, a validated predictive model, such as that validated by Khorana et al., 10 would enable clinicians to target thromboprophylaxis to patients considered to be at greatest risk. On the other hand, studies have been performed to identify novel candidate biomarkers. 28,29 Recently, Verso et al. designed a modified Khorana risk assessment score (Protecht score) by adding platinum or gemcitabine-based chemotherapy to the predictive variables already taken into account in the Khorana score. 30 In the present study, a higher rate of VTE was found in patients receiving platinum-based chemotherapy, whereas no differences were found in patients treated with gemcitabine. In agreement with previous observations, 31 in the elderly subset, a trend toward an increased risk of VTE in patients receiving a platinum-based chemotherapy was observed. Despite the small number of this subgroup sample, these data could be useful for stratifying the VTE risk in an elderly cancer population in planning future clinical trials.
In a cohort population of 208 cancer patients with a mean age of 60±11 years, we recently demonstrated how early changes of activated protein C (APC)-dependent thrombin generation assay during chemotherapy improve VTE risk stratification and help identify a population of cancer patients at high risk for VTE. 32 Moreover, using a subgroup of the same population study, we also showed how using a high-sensitivity (HS) assay for D-dimer determination prior to chemotherapy might allow for VTE risk stratification of intermediate-risk cancer patients, helping in identifying those individuals who could benefit from thromboprophylaxis. 33
In the analysis reported here, we did not find any significant difference between elderly and YMA groups in the Khorana model for risk of chemotherapy-associated thrombosis. The Khorana model is a clinical risk model for predicting rates of VTE in cancer outpatients receiving chemotherapy that includes five clinical and laboratory parameters: Primary site of cancer, pre-chemotherapy platelet count of 350×109/L or more, hemoglobin level less than 100 g/L (10 g/dL), use of erythropoiesis-stimulating agents (ESAs), leukocyte count more than 11×109/L, and BMI of 35 kg/m2 or more. 10 In this study, age was not significantly associated with VTE either when the population was dichotomized at 65 years or categorized as younger than 40 years, 40 years to younger than 65 years, and 65 years or older. Authors explained this unexpected result with the characteristics of the cohort population study that presented an excellent performance status of most of the enrolled patients. 10 On the basis of the results of the present study and previously discussed findings, we believe that age, ECOG-PS, and type of chemotherapy should be always taken in account in the identification of cancer patients at highest risk for VTE that would benefit from thromboprophylaxis.
In conclusion, our study reports an increased incidence of VTE in elderly cancer patients treated with chemotherapy, suggesting age as one of the most important risk factors for VTE in this type of patient. In the cancer population, especially in the elderly that are the most affected population, identification of patients most at risk for VTE followed by effective prophylaxis could improve morbidity, mortality, delivery of cancer therapy, related outcomes, quality of life, and use of health care resources. The limitations of our study include its relatively small population size and the retrospective design. The lack of an association between VTE and the class of risk according to Khorana score or the presence of metastatic disease may indeed be the consequence of lack of power of the current study. For these reasons, we firmly believe that further prospective studies are imperative to better understand this phenomenon.
Footnotes
Acknowledgments
This work was carried out within the PhD program in Physiopathology (XXVI cycle, Medical Oncology Course), University of Rome Tor Vergata. This work was partially supported by the Italian Ministry of Health Grant MERIT RBNE08NKH7.
Author Disclosure Statement
No competing financial interests exist.