
Abstract
Urinary incontinence (UI) is very common in the elderly and has personal and social implications. Many authors have pointed out the necessity to analyze UI in correlation with the overall quality of aging, to better understand this syndrome and define measures for its prevention and treatment. In the present study, we addressed this problem by analyzing the UI correlation with frailty, which has emerged in the last decade as the geriatric syndrome correlated with individual homeostatic capacity and then as the basis of the age-related physical decline. In addition, the monitoring of our sample for a long period allowed us to estimate the prognostic significance of UI by analyzing the correlation between UI and mortality. The analysis was performed in a large sample that included numerous ultra-nonagenarians, a population segment that is still poorly known for UI and other geriatric parameters. We found a strict correlation between UI and frailty, suggesting that UI is correlated to the homeostatic and physiological decline leading to frailty. In addition, we found that UI is an independent mortality risk factor in ultra-nonagenarians, suggesting that the neurological sensitivity needed to be continent is lost very soon when the frailty associated physiological decline begins. On the whole, our study suggests that UI is a marker of frailty and that UI patients should be monitored and, in case, treated in a timely manner to avoid, or to limit, the effects of frailty such as malnutrition, falls, and the consequent accumulation of disabilities.
Introduction
Frailty corresponds to a combination of deficits or conditions that arise with increasing age and contributes to making the elderly person more vulnerable to changes in surroundings and to stress (see refs. 11 and 12 and references therein). The definition of frailty has evolved rapidly in the last decade, and, if it was previously thought to overlap (or even being identical to) disability, it is now emerging as a specific physiological state indicating a loss of homeostatic capacity, or resilience, which exposes the elderly to a number of negative outcomes, such as falls, disability, diseases, and death. 13 –15 Thus, frailty is not disability but the cause of disability. A certain number of clinical conditions have been shown to be associated with frailty, such as nutritional problems, restricted mobility, history of falls, cognitive impairment, and decreased bone mineral density. 16 –18 The identification of new parameters significantly associated with frailty is essential to recognize persons at risk for the application of adequate programs of prevention. The present study aimed at evaluating the correlation between incontinence and frailty, and availed of a previous study that allowed classification of elderly subjects according to their frailty phenotype. 19,20 In addition, a follow-up study allowed us to estimate the correlation between UI and mortality and then to evaluate the prognostic significance of UI. Special attention was dedicated to understanding the correlation of UI with frailty and mortality in ultra-nonagenarians and centenarians. In fact, very little is known regarding UI, as well as many other health issues regarding this rapidly growing population, in western countries, and this is posing unprecedented questions about social and medical care.
Materials and Methods
The study was carried out on two samples. Sample 1 (S1) comprised 270 subjects (154 females and 116 males, age range 65–89 years, median age 73 years). Sample 2 (S2) comprised 300 subjects (169 females and 131 males, age range 90–107 years, median age 92 years). All subjects were born and living in Calabria and were recruited from 2000 to 2010 during different recruitment campaigns. Details on the campaigns and on different aspects of the Calabrian population are given in De Rango et al. 21
The subjects were classified with respect to frailty by using a cluster analysis that availed of specific geriatric parameters,
20
including Activities of Daily Living (ADL), Mini-Mental State Examination (MMSE), Hand Grip Strength (HG), and Self-Reported Health Status (SRHS). The frequency distributions of these parameters and common diseases, as well as the output of the clustering algorithm in both samples, are reported in Supplementary Material (Tables S1 and S2; and Fig. S1). (Supplementary Data are available at
To choose the optimal number of clusters, in the classification algorithm adopted in the previously mentioned work, the increase in the total within-cluster sum of squares was plotted against the number of groups. The optimal number of clusters was determined in correspondence of the largest drop in the total within-cluster sum of squares. In the case of the S1 sample (subjects 65–89 years old), the largest drop in the total within-cluster sum of squares was observed when three clusters were obtained. We defined these clusters as “non-frail” (the cluster with subjects showing the best scores for the classification variables), frail (the cluster with subjects showing the worst scores for the classification variables), and pre-frail (the cluster with subjects showing intermediate scores for the classification variables). In the case of the S2 sample (subjects older than 90 years), the largest drop was observed when two clusters were obtained. Similar to the first classification, we defined these clusters as frail (the cluster with subjects showing the best scores for the classification variables) and very frail (the cluster with subjects showing the worst scores for the same variables). Follow-up for about 7 years for sample 1 and about 3 years for sample 2 have been carried out to establish survival of the participating subjects.
UI was assessed by a questionnaire that evaluated any incontinence, including stress incontinence and urge incontinence. Patients were carefully informed about the nature of the questions and about the importance of providing accurate information. The questions were the following. Question 1: “In the past 12 months, about on how many days have you lost any urine, even a small amount, beyond your control?” Question 2: “Since urine loss is the main interest in our study, I want to be sure that you have understood that we need to identify all occasions where urine loss occurred during the last 12 months.”22 Then the interviewer asked if urine leakages were occasional or if these leakages had been so frequent to request the use of diapers or catheter. Thus, we classified as incontinent all the subjects who reported leakage or dribbling of urine in the 12 months prior to the interview. The subjects for whom repeated occurrence of incontinence had led to the use of diapers or catheter were classified as “severe incontinence” patients.
Statistical analysis
Testing for independence in contingency tables was carried out by using the Fisher exact test. Logistic regression analyses were performed to assess the association between frailty and incontinence. In particular, in sample S1 a multinomial logistic regression model was employed using age and sex as co-variates and nonfrail group as reference category. In sample S2 a binary logistic regression model was employed using age and sex as co-variates and the frail group as reference category. In both logistic regression models, incontinence data were coded as a binary independent variable (1 for subjects showing moderate or severe incontinence problems, 0 otherwise).
Kaplan–Meier estimates were used to obtain the survival curves with respect to the incontinence status in both samples. To evaluate the effect of the incontinence on the mortality risk, the obtained survival curves were then compared by log-rank test.
In both samples, Cox proportional hazard models 23 were used to assess the independent contribution of the incontinence on the mortality risk. Sex, age, and frailty status were used as adjunctive co-variates. Schoenfeld 24 residuals were used to assess the proportional hazard assumption. Statistical analyses were performed with the R statistics package. 25 In particular, the survival package was used for survival analyses. 26 A significance level of 0.05 was chosen in all the tests.
Results
Table 1 reports the general characteristics and post-survey mortality of the analyzed samples. In sample S1, 60 (22.2%) and 11 (4.1%) subjects showed moderate and severe incontinence problems, respectively. Incontinence was significantly higher in females than in males (35.1% vs. 13.8%; p<0.001). A multinomial logistic regression model (including covariates as age and sex as possible confounding factors) allowed us to evaluate the effect of incontinence (odd ratios [OR]) on the probability to belong to frailty groups. We found that an incontinent subject was 6.5 times more likely to fall in the “frail” group (OR=6.638, p=0.004) and 2.3 times more likely to fall in the “pre-frail” group (OR=2.312, p=0.021) with respect to a continent subject (Table 2).
The reference category is the nonfrail group.
SE, Standard Error; OR, odds ratio; CI, confidence interval.
Consistently, we found that the average survival time in males was 59.6 months for incontinent and 86.3 months for continent subjects (p=0.002). In females, average survival was 91.6 months for continent and 83.2 months for incontinent subjects (p=0.140). However, a Cox regression model that controlled for confounding factors (age, sex, and frailty status) showed that incontinence does not influence mortality independently from such factors. Also, when stratifying for degree of incontinence (moderate and severe), no significant association was obtained. In sample S2 (subjects older than 90 years), 41 (13.7%) and 71 (23.7%) subjects showed moderate and severe incontinence problems, respectively. Incontinence was higher in females than in males (40.8% vs. 32.8%, p=0.039). A binary logistic regression model allowed us to evaluate that incontinent subjects were about eight times more likely to fall in the “very frail” group with respect to continent subjects (OR=7.856, p<0.001; Table 3).
The reference category is the frail group.
SE, Standard error; OR, odds ratio; CI, confidence interval.
Consistently, we found that the average survival time in males was 29.8 months for incontinent and 37.1 months for continent subjects (p=0.121); in females, average survival was 51.3 months for subjects without incontinence problems and 30.6 months for incontinent subjects (p<0.001). A Cox regression model that controlled for confounding factors (age, sex, and frailty status) showed that incontinence does not influence mortality independently from other factors. However, stratifying the previous analysis for degree of incontinence (moderate and severe), we found that subjects with severe incontinence problems exhibit a significance difference in terms of survival than subjects with no incontinence problems (Hazard Ratio=1.475, p=0.028; Table 4, Fig. 1).
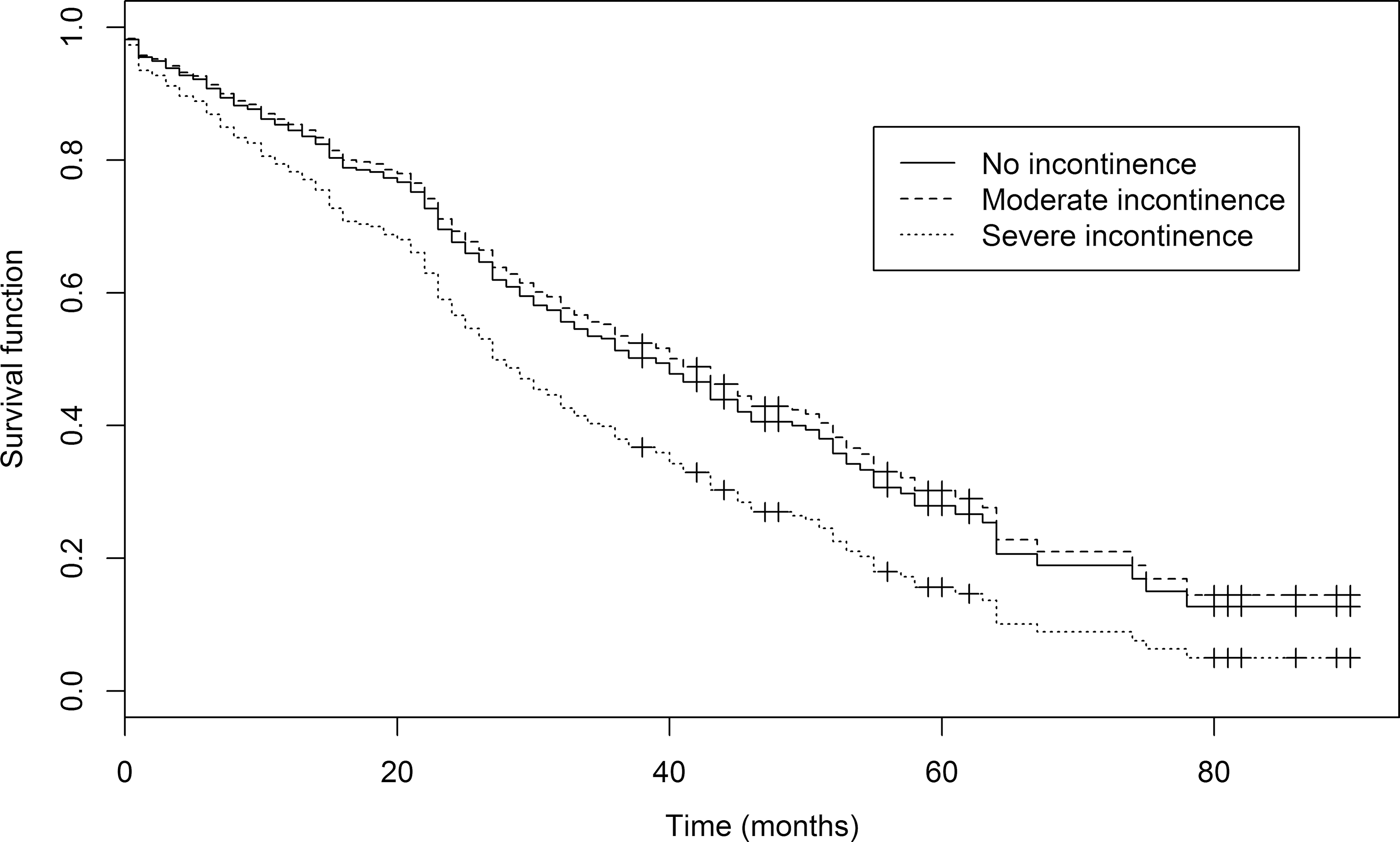
Survival functions in the S2 sample stratified for incontinence status after adjustment for confounding factors (age, sex, and frailty status).
SE, standard error; HR, hazard ratio; CI, confidence interval.
Discussion
UI is one of the most disturbing problems for the elderly and greatly affects quality of life by hindering social and emotional relationships and causing anxiety and depression. 27 The management of UI patients can be quite difficult and can lead to the placement in nursing homes. 28 –30 It has been reported that UI does not affect mortality, but it is certainly correlated to frailty, which, in turn, is emerging as the main factor to understand in elderly subjects in need of help. 7,9,31 In fact, the presence of frailty indicates a diminished physiological homeostatic capacity that is strictly correlated to a diminished capacity to use energy and leads to sarcopoenia and to a cognitive decline. 14,20,32 –34 Our study was aimed at better understanding the correlation of UI with frailty and mortality in the elderly population of Calabria. It is of note that for the first time we analyzed this problem in ultra-nonagenarians and centenarians. Our data clearly show that UI is highly correlated with frailty, and it can then be considered as a marker of frailty, which may suggest a closer monitoring to understand if the subject is, or is becoming, frail.
The most important finding emerging from our study is the association between UI and mortality in nonagenarians. Indeed, as previously reported, UI is not to be considered an independent mortality risk factor in elderly subjects in the age range 65–89 years. 9,22,35 In fact, although UI is correlated with mortality, this is due to the correlation of UI with frailty. However, in ultra-nonagenarians, we found that severe UI is correlated with mortality also after adjustment for frailty and other confounding factors. This might suggest that being continent after 90 years of age implies the conservation of a neurological sensitivity that is beyond what is measured by geriatric tests used to evaluate cognitive impairment and frailty. In turn, this might then suggest that UI is a marker of frailty also in ultra-nonagenarians, and it can be considered also as a precursor of frailty and an independent mortality risk factor. Indeed, it is possible that the neurological sensitivity needed to be continent is lost very soon when the physiological decline due to the frailty begins.
As to the limitations of this study, we need to highlight that incontinence was self-reported by the patients or by the caregiver in the cases of impaired cognition. Additionally, our study may lack precision in estimating the observed association owing to its limited statistical power. Finally, findings from our single-center study may not necessarily apply to oldest old populations coming from different Italian regions or other countries. As for the strengths of our study, the 5-year follow-up period allowed us an almost optimal exploration of the prognostic impact of UI in a population including nonagenarians and centenarians.
In conclusion, strict correlation between frailty and UI provides some important hints on how to deal with this symptom in the elderly. Indeed, as most of the symptoms in the elderly and in the oldest old, UI should be treated as part of the declining homeostatic capacity. In particular, as suggested by Coll Planas et al., 36 this finding calls for an early intervention to avoid, or to limit, some of the effects of frailty, such as malnutrition, falls, and the consequent accumulation of disabilities. On the other hand, UI has a negative prognostic impact, which for oldest old can even be independent of frailty syndrome. Further efforts are then required for the prevention of UI in older people. In consideration of its negative prognostic impact, UI should be recognized in a timely manner, and the patient eventually should be properly treated, even the oldest old.
Footnotes
Acknowledgments
The research leading to these results has received funding from the European Union's Seventh Framework Programme (FP7/2007-2011) under grant agreement no. 259679 and from “Fondi di Ateneo” of the University of Calabria.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.