
Abstract
Dehydroepiandrosterone (DHEA) and its sulfate ester are the most abundant steroids in humans. DHEA levels fall with age in men and women, reaching values sometimes as low as 10%–20% of those encountered in young individuals. This age-related decrease suggests an “adrenopause” phenomenon. Studies point toward several potential roles of DHEA, mainly through its hormonal end products, making this decline clinically relevant. Unfortunately, even if positive effects of DHEA on muscle, bone, cardiovascular disease, and sexual function seem rather robust, extremely few studies are large enough and/or long enough for conclusions regarding its effects on aging. Moreover, because it has been publically presented as a “fountain of youth” equivalent, over-the-counter preparations lacking pharmacokinetic and pharmacodynamic data are widely used worldwide. Conceptually, supplementing a pre-hormone is extremely interesting, because it would permit the human organism to adequately use it throughout long periods, increasing or decreasing end products according to his needs. Nevertheless, data on the safety profile of long-term DHEA supplementation are still lacking. In this article, we examine the potential relation between low DHEA levels and well-known age-related diseases, such as sarcopenia, osteoporosis, dementia, sexual disorders, and cardiovascular disease. We also review risks and benefits of existing protocols of DHEA supplementation.
Introduction
DHEA is produced by fetal adrenal glands, and DHEAS levels are high at birth. Following the involution of the adrenal fetal zone, DHEA decreases to almost undetectable levels during the first year of life. 6 The production of DHEA starts again at ages 6–8, a phenomenon called “adrenarche.” 1 DHEA levels peak during the third decade of life. In premenopausal women, daily production of DHEA is 6–8 mg. A total of 50% is secreted by the adrenals, 1–2 mg by the ovaries, and the rest by peripheral tissues. 1 In post-menopausal women, production of estrogens and DHEA from the ovaries is near zero, 1 making adrenals the main source of estrogens and testosterone through DHEA. 2 DHEA levels range between 1.12 ng/mL and 7.43 ng/mL before and between 0.6 ng/mL and 5.7 ng/mL after menopause with median concentrations of 3 ng/mL and 1.67 ng/mL, respectively. 7 In men, DHEA is produced mainly by the adrenals (10% of DHEA is secreted by the testis). 8 Median DHEA concentrations are around 2 ng/mL. 7
Age-related decrease of DHEA levels suggests an “adrenopause” phenomenon characterized by low DHEA and maintained cortisol levels. 9 Indeed, DHEA levels range between 1.33 ng/mL and 7.78 ng/mL between 18 and 40 years, and between 0.63 ng/mL and 4.7 ng/mL after 40 years, for both men and women. 7 By the age of 70–80 years, levels may be as low as 10%–20% of those encountered in young adults, even if inter-individual differences are very important. 6 Lower concentrations are observed in women compared to men. 10 The underlying mechanism is not fully understood, but seems related to a decrease in adrenal production rather than a modification in DHEA metabolism. 5 Other conditions related to low DHEA levels are acute stress, severe systemic illness, anorexia nervosa, and adrenal failure. Conversely, levels may be high in patients with hyperprolactinemia. 1
Studies point toward several potential roles of DHEA, making its age-related decline clinically relevant. In this article, we will review data on the physiological role of DHEA, as well as the relations between adrenopause and well-known geriatric syndromes.
Physiological Role of DHEA
Activity of DHEA through its end products
DHEA and DHEAS are pre-hormones. DHEAS is hydrophilic and constitutes a circulating stock. Only lipophilic DHEA can be transformed in peripheral tissues to more potent androgens and estrogens. 6 Steroid production at a tissue level permits an auto-regulation of the local hormonal environment according to local needs, with less systemic effects. 1,2 This phenomenon is called intracrinology. In women before menopause, 50%–75% of estrogens and the majority of androgens are produced through intracrine mechanisms from DHEA. After menopause, practically all androgens and estrogens are synthesized at a tissue level. In men, whose testes continue to secrete androgens throughout life, local hormone production also occurs but is more difficult to assess. 4,6
Studies in humans have shown different intracrine patterns in men and women after DHEA administration. Thus, DHEA increases mostly circulating androgens in women and estrogens in men. 11 –14 Nevertheless, it is practically impossible to measure precisely the hormonal end products of DHEA administration. First, peripheral hormone levels do not always correspond to the tissue hormone levels produced through intracrine mechanisms. Second, other products of steroid metabolism deriving from DHEA may also have estrogenic or androgenic properties, not taken into account when peripheral steroids are measured (Fig. 1).
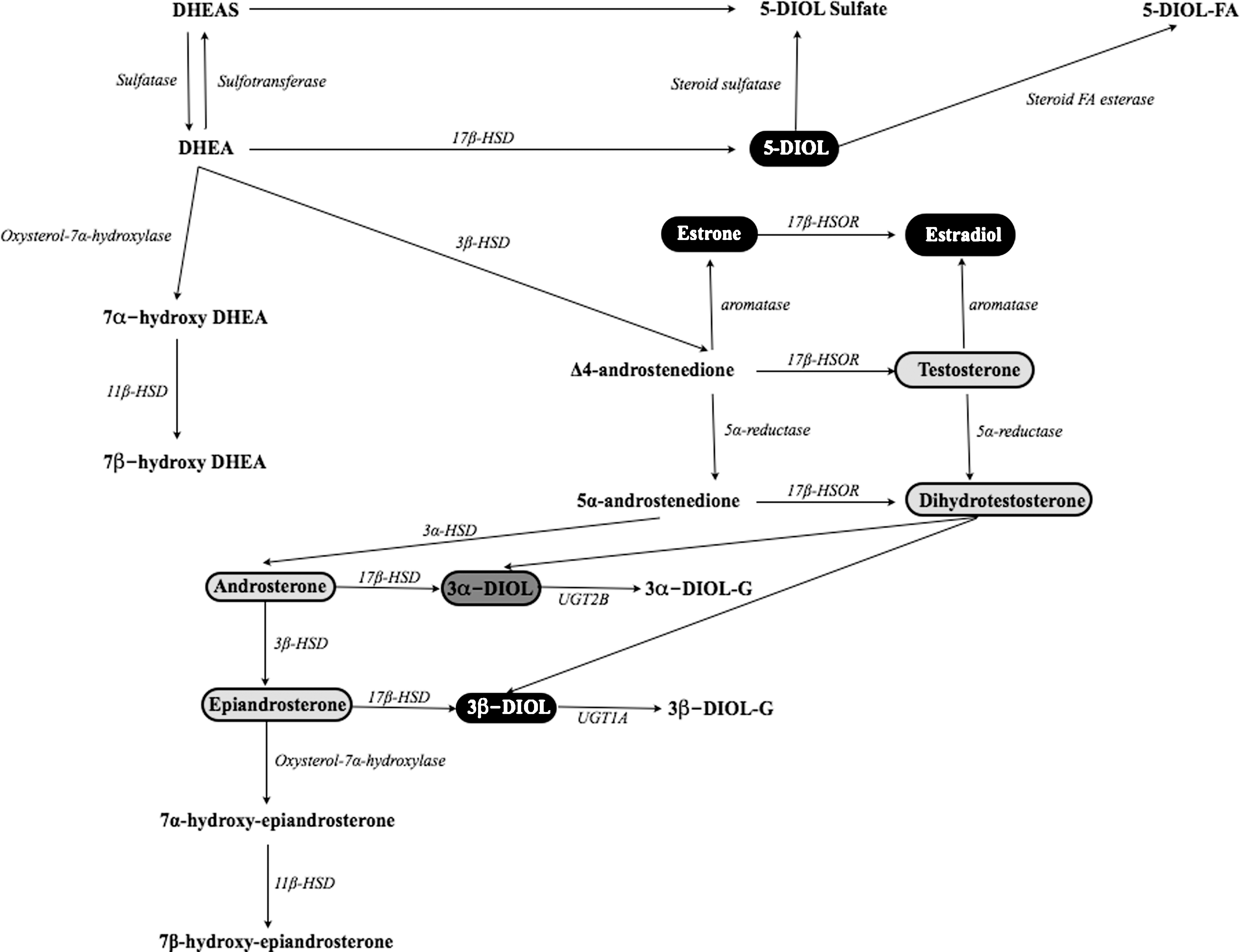
Dehydroepiandrosterone (DHEA) and its hormonal end products. Those with intrinsic estrogenic activity are noted in black, those with androgenic activity in light gray, and those with both in dark gray. DHEAS, DHEA sulfate; HSD, hydroxysteroid dehydrogenase; HSOR, hydroxysteroid oxydoreductase; UGT, uridine glucuronosyl transferase; 5-DIOL-S, androst-5-ene-3α,17β-diol sulfate; 5-DIOL, androst-5-ene-3α,17β-diol; 3α-DIOL-G : androstane-3α,17β-diol glucuronide; 3α-DIOL-G, androstane-3α,17β-diol glucuronide; 5-DIOL-FA, androst-5-ene-3α,17β-diol fatty acid. FA, fatty acid.
Potential activity of DHEA through specific receptors
No specific intra-nuclear receptors of DHEA have been identified yet. 5 However, recent evidence supports the existence of membrane receptors interacting with high specificity and affinity with DHEA. 15 –17 Such receptors have been found in the endothelium, heart, kidney, and liver. 18 Studies show that DHEA increases nitric oxide (NO) production from intact endothelial cells in vitro (both animal and human), probably through a G-protein–dependent activation of endothelial NO synthetase (eNOS). This effect was independent from androgens, estrogens, and progesterone, as well as intracellular calcium. Conversely, it seemed influenced by tyrosine and mitogen-activated protein kinases (MAPKs). 15 –17 A concomitant increase of eNOS activity and intracellular cyclic guanosine monophosphate (cGMP) suggests that DHEA might act partly through the eNOS/cGMP pathway. 18 Finally, 7α- and 7β-hydroxylated derivatives of DHEA seem to have a direct effect on nuclear receptors, but their physiological function is not clear yet 18 (Fig.1).
DHEA's physiological role is only partly understood. Its role as a steroid hormone stock is crucial because intracrine mechanisms produce a large part of estrogens and androgens. Recent data support also direct actions of DHEA through specific receptors.
Low DHEA and Geriatric Syndromes
Musculoskeletal disorders
One-third of patients over 65 and half of those in nursing homes fall at least once per year. 19 The lifetime risk for a fracture after 50 years is 51% for women and 20% for men. 20 One of the major risk factors for falls in the elderly is muscle weakness. 21 Muscle mass decreases with age at a rate of 6% per decade, beginning around age 45. 22 No specific DHEA receptor has been identified in the muscle tissue. Potential effects could be mediated by a DHEA-related increase of insulin-like growth factor-1 (IGF-1) levels 11,14 and bioavailability (decrease of insulin growth factor binding protein-1 [IGFBP-1] 14 ) in men and women and an increase of androgen levels mostly in women. 11,14,23 Studies in elderly individuals support a positive relation between DHEA blood levels and muscle mass, 24 strength, 24,25 mobility, 26 and a lower risk for falls. 27 A positive effect of DHEA administration on body composition, 11,28 –30 muscle strength, 11,31 and physical performance 31 has also been reported. Nevertheless, others failed to confirm such an effect. 32 –36 Disparities between studies could be related to the rather moderate effect of DHEA, but mostly due to great differences between study designs, short durations of treatment, and small population samples. So to date, even if the link between DHEA and musculoskeletal disorders seems clear, the usefulness as well as the modalities of DHEA use in rehabilitation protocols for older patients is not well known.
The risk for fractures depends on the combination of the propensity for falling and bone frailty, today best reflected by the quantitative assessment of bone mineral density (BMD). 37 In an in vitro analysis, primary human osteoblasts showed aromatase activity converting DHEA to estrone. 38 Another in vitro study showed that DHEA inhibits apoptosis and promotes proliferation of rat osteoblasts through MAPK signaling pathways, independently from androgens and estrogens. 39 These findings support a positive effect of DHEA on bone through conversion to estrogens, but also independently from its hormonal end products. In a group of 120 post-menopausal women aged 51–99 years, lumbar spine BMD was related to DHEAS but not to estradiol plasma levels. 38 DHEA levels have been positively related to BMD in men 40 and post-menopausal women. 38
In post-menopausal women, several studies have reported positive effects of DHEA administration on BMD of both the lumbar spine 28,41 –45 and the hip. 9,43,44 Positive effects of DHEA administration on BMD have also been reported in men, for both the lumbar spine 28,43,46 and the hip. 28,43,44,46,47
To conclude, DHEA has positive effects on BMD in both men and women, even if it is weaker than other treatments of osteoporosis. 1 Further studies could help to better define the role of DHEA in osteoporosis prevention and treatment.
Cognitive disorders
Dementia and specifically Alzheimer disease prevalence after the age of 65 are around 6%–8%, and 4.4%, respectively. 48,49 Actual estimations put the number of patients suffering from dementia worldwide around 34 million. Numbers could rise three-fold in 2050 if no efficient prevention strategies are implemented. 50,51 The related personal, social, and economic burdens are extremely high.
In vitro studies on human neural cells supported neurotrophic and neuroprotective effects of DHEA and its metabolites, mainly through DHEA-dependent neural stem cell stimulation, genomic activity modulation, and up-regulation of androgen receptor levels. 52,53 Furthermore, DHEA inhibits the production of pro-inflammatory proteins such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6). 18 High levels of cytokines found in aging individuals may affect the metabolism of amyloid precursor protein and increase the production of αβ-40 and αβ-42 peptides forming the amyloid plaques, a hallmark of Alzheimer disease. 54 However, to our knowledge, no specific data exist on the role of the immunoregulatory effects of DHEA in prevention of dementia.
In clinical studies, DHEAS levels have been related to better executive function 55 and higher scores on the Mini Mental State Examination. 56 Surprisingly, an inverse relation between DHEA levels and cognitive performance has also been described. 57 Barrett-Connor et al. 58 found no relation between DHEA levels and incident dementia 15–20 years later. Concordantly, most studies addressing the effect of DHEA supplementation on cognitive function showed no 59 –63 or only a small effect on specific cognitive domains such as verbal fluency. 64 However, most studies available were very short (2 weeks to 1 year) and included only small groups of patients. Thus, in our opinion, current data do not appropriately address the potential role of DHEA in dementia prevention and treatment.
Mood disorders
The prevalence of depression increases with age. 65 It is related to cognitive and functional decline as well as high morbidity and mortality. 66 Animal studies showed that DHEA increased the activity of 5-hydroxytryptamine (5-HT) neurons, offering a physiological basis for a potential anti-depressant effect. 67 Other neurotransmitters probably affected by DHEA are dopamine, glutamate, and γ-amino butyric acid. 18 Clinical studies have suggested a relation between higher DHEA and psychological well-being in older individuals. 1 Low levels of DHEA have been related to the presence of depressive symptoms 68,69 and DHEA supplementation improved such symptoms, 70 –74 even if studies are not unanimous. 59 Overall, DHEA treatment has mostly positive effects on mood disorders. Further studies are warranted to better define indications and treatment modalities.
Cardiovascular disease
Cardiovascular disease prevalence increases with age. Thirty percent of all acute myocardial infarctions affect patients over 75 years. More than 60% of patients hospitalized for unstable angina are over 65, and 80% of deaths from coronary disease occur in patients over 60. 75
DHEA administration has been related to a decrease in high-density lipoprotein (HDL) levels. 47,76,77 This was mostly observed in women, probably due to the more prominent androgenic effects of DHEA compared to male patients. 11,14,76,78 –80 Conversely, one study reported significantly higher HDL, lower low-density lipoprotein (LDL), and lower triglycerides levels after a daily administration of 25 mg of DHEA for 12 months to 20 post-menopausal women. 81 Overall, most studies report no association between DHEA plasma levels 82,83 or DHEA administration 11,32 61,84,85 and the lipid profile.
Animal studies support a beneficial effect of DHEA administration on obesity and insulin sensitivity. 86 –88 In humans, actual data are rather inconsistent. Low DHEA levels have been related to higher fasting glucose but not diabetes in post-menopausal women. 89 On the contrary, Barrett-Connor et al. 90 found a direct relation between higher DHEA levels, higher waist-to-hip ratio, impaired glucose tolerance, and diabetes mellitus in post-menopausal women. A positive effect of DHEA administration on insulin sensitivity has been described in a group of middle-aged hypo-adrenal women 91 as well as in groups of elderly men 30 and women. 30,79,81 Nevertheless, most interventional studies found no effect of DHEA replacement therapy on glucose tolerance and diabetes mellitus. 11,14,33,36,47,78,85,92
Animal studies have suggested a protective effect of DHEA against atherosclerosis. 93 –96 Current opinion consensus supports a lipid profile independent mechanism mediating the anti-atherosclerotic effects of DHEA, 18,93 –95 partly through transformation to estrogens and testosterone. 97 The previously described anti-inflammatory effects of DHEA, 18,95 as well as direct stimulation of eNOS could also participate. 17,18 Indeed, low DHEAS predicted incident ischemic heart disease in a group of men in a 9-year follow-up study, independently from classic cardiovascular risk factors. 98 Others found a significant inverse relation between DHEAS levels and common carotid artery intima media thickness in men and a direct relation with common carotid artery blood flow in women. 99 Low DHEA levels were also associated with more severe coronary atherosclerosis on coronary angiography in 206 middle-aged patients. 100 In heart transplant patients, cardiac allograft vasculopathy developed more frequently and earlier in patients with low DHEA. 101 Finally, actual data support a relation between heart failure and low DHEA levels. In fact, the heart produces DHEA in an autocrine way, which decreases as the disease progresses. 102 Low DHEA has been related to a worse prognosis in male patients with chronic heart failure. DHEAS levels were also positively associated with left ventricular ejection fraction, and negatively with amino-terminal pro-brain natriuretic peptide levels. 103
Cardiovascular and overall mortality were higher in post-menopausal women with low levels of DHEAS and coronary disease, after a mean follow-up of 6 years. 83 Others found no relation between DHEA levels and cardiovascular mortality in post-menopausal women. 104 In men, low DHEA has been associated with higher overall and cardiovascular mortality. 105 In the same study, an increase of DHEAS levels by 100 μg/dL was associated with a reduction of all cause and cardiovascular mortality by, respectively, 36% and 48%. 105
The evidence for an inverse relation between DHEA levels and cardiovascular risk are rather robust. Nevertheless, the effects of DHEA administration have been studied insufficiently.
Sexual function/menopause symptoms
Sexual disorders are most prevalent in aging men. In a group of male patients aged between 75 and 95 years, sexual problems were present in 72% of cases (49% erectile problems, 48% lack of interest, 39% unable to climax, 20% sexual performance-related anxiety). 106 Low DHEA levels have been related to a higher risk for erectile dysfunction, 107 –109 even in people younger than 60. 110 DHEA supplementation has been related to an improvement of erectile function, but also of desire, sexual interest, sexual activity, arousal, and fantasy, 70,111 even if negative studies also exist. 59,112 Positive effects on erectile function were mostly achieved in the absence of any underlying organic pathology. 111,113 Indeed, there was no benefit in patients with diabetes or neurological disorders. 113
In women, androgens and estrogens are produced from DHEA in the vagina tissue. Androgens are well known for their effects on arousability, pleasure, and intensity of orgasm in women. They are particularly implicated in the neurovascular smooth muscle response of swelling and lubrication, whereas estrogens contribute to vulval and vaginal congestive response and affect mood and sexual responses. 6 Pre- and post-menopausal women with lower sexual responsiveness have lower levels of serum DHEAS. 1,4,114 However, given the extremely large interval of normal values in women, a threshold for a higher risk of sexual disorders is difficult to define. 1
Most studies on DHEA supplementation in post-menopausal women report benefits in various sexual domains such as increased desire, fantasies, lubrication, arousal, activity, interest, sexual drive, satisfaction, and orgasm. 9,70,115 –117 Intra-vaginal administration of DHEA improved arousability, sensation, lubrication, orgasm, and pain during sexual activity, without increasing serum steroids. 118 The positive effects of DHEA on sexual function in post-menopausal women may be related to the concomitant increase of estrogens and androgens and their effects on the central nervous system and the genital tract. 115 Nevertheless, others reported no positive effects. 14,59,119 Differences in pre-treatment DHEA and testosterone levels could be partly responsible for the discrepancies in results between these studies. 18
An improvement in symptoms of menopause in peri-menopausal and early post-menopausal women has also been reported with DHEA. 115,120 Intra-vaginal administration of DHEA was effective for reversing vaginal atrophy in post-menopausal women. 121 DHEA supplementation in early post-menopausal women is interesting. First, no increase of endometrial thickness has been reported with DHEA, probably because endometrial tissue does not have the necessary enzymes to transform it into estrogens, or because estrogen and progesterone are both its derivatives. Finally, the risk for breast cancer does not seem to increase with DHEA. 122
Treatment
Treatment modalities
DHEA is considered as a dietary supplement in the United States but as a hormone in Europe. This difference has no scientific foundation and is mostly a matter of declaration. At present, questionable over-the-counter DHEA preparations lacking pharmacokinetic and pharmacodynamic data are widely used in the United States.
Treatment indications and modalities of DHEA supplementation are not well defined. In one study, after administration of 25–50 mg of DHEA, half-life varied from 18.7±5.5 to 25.1±10.7 hr in men, and from 23.6±8.5 to 26.6±8.6 hr in women. 5 Long half-life allows a single take of 25–50 mg/day. Target levels of DHEA are around the middle of normal range for healthy young subjects, controlled by a blood sample 24 hr after the last take. 123
End products of DHEA supplementation depend on the patient's sex, with a non-symmetrical transformation of DHEA favoring androgens in women and estrogens in men. 2 DHEA administration for 23 months to elderly healthy individuals resulted in higher estradiol and testosterone in women and higher estradiol in men. 47 End products may also vary according to the way of administration. Daily oral intake of 50 mg of DHEA for 12 months in post-menopausal women was associated with an increase of estrone, estradiol, androst-5-ene-3α,17β-diol (5-diol), testosterone, dihydrotestosterone, and androstenedione. There was also a four- to five-fold increase of androstane-3α,l7β-diol-3-glucuronide (3α-diol 3G), androstane-3α,17β-diol-17-glucuronide (3α-diol 17G), and androsterone glucuronide. 119 In another study, a 12-month transdermal DHEA administration provoked similar increases in estrone, estradiol, and 5-diol, but the sum of androsterone glucuronide, 3α-diol,3G, and 3α-diol,17G increased by only 71%. 124 First hepatic pass effect, through hepatic 5α-reductase, could contribute to the difference between oral and transdermal administration 1 (Fig. 1). Consequently, depending on the desired effect, less important conversion of DHEA to androgens should be considered when transdermal formulations are used. Moreover, DHEA transformation to DHEAS in the liver after ingestion seems responsible for the longer half-life and better pharmacokinetic profile observed with oral compared to intravenous or transdermal formulations. 5,124,125
Adverse effects
DHEA has been very well tolerated in studies using oral or percutaneous administration, with daily doses ranging from 25 mg to 1,600 mg. In women, only minimal adverse effects have been reported such as mild acne, seborrhea, facial hair growth, and ankle swelling. 5,18 No adverse effects were observed on endometrium or breast tissue. 1 In men, concerns have been expressed about DHEA transformation to androgens and their effects on the prostate tissue. After local transformation, DHEA may be responsible for one-sixth of dihydrotestosterone present in the prostate. 126 However, no increases in prostate volume or PSA were noted after 2 years of treatment with 50 mg of DHEA in a group of older men. 47
An important metabolite of DHEA is 5-diol (Fig. 1), which appears to bind weakly to the estrogen receptor. The estrogenic effect of 5-diol was supported by a study in breast cancer patients who progressed under aromatase inhibitor treatment but improved with a sulfatase inhibitor. Sulfatase inhibition results in lower levels of DHEAS being transformed to DHEA, and thus to lower or even insignificant levels of 5-diol. 127 Nevertheless, studies have reported no increase in cancer risk after DHEA treatment. On the contrary, animal models demonstrated that DHEA administration inhibited experimentally induced tumors of the lymphatic tissue, lung, colon, breast, liver, and skin. 128,129 The underlying mechanism is not fully known, but seems to include the inhibition of glucose-6-phosphate dehydrogenase and the pentose phosphate pathways, which are a source of nicotinamide adenosine dinucleotide phosphate hydrogen (NADPH). This results to a decrease of NADPH-dependent reactions generating free radicals, and a decreased oxidative stress. 11,81,128,129 Further studies are warranted to better understand the underlying mechanism of DHEA anti-cancer effect and its potential applications in humans.
In general the safety profile of DHEA administration is satisfying. Unfortunately most studies available are too short to assess long-term safety of DHEA supplementation.
Conclusion
Conceptually, supplementing a pre-hormone is extremely interesting, but is very different from supplementing a hormonal end product. The human organism needs the time to adequately use it throughout long periods, increasing or decreasing end products according to his needs that may fluctuate over time. Therefore, DHEA administration is closer to “hormonal optimization” than “hormonal supplementation.” Unfortunately, extremely few studies are large and/or long enough to conclude on the effects of DHEA on aging and age-related diseases, even if positive effects of DHEA on muscle, bone, cardiovascular disease, and sexual function seem rather robust. The safety profile of long-term DHEA supplementation also needs to be better studied.
Author Disclosure Statement
No competing financial interests exist.