
Abstract
Objectives:
Older adults complain of sleep disturbances more often than younger adults do. It is not clear whether the age-related rise in sleep problems is related to aging itself or to health-related quality of life. The aim of this study was to explore the presence of self-reported sleep problems in healthy elderly individuals and to evaluate whether changes occurred over a 3-year follow-up.
Methods:
A total of 314 older community-dwelling volunteers, aged 71.6±1.0 years old, were examined and followed for 3 years. All of the subjects completed questionnaires evaluating anxiety, depression, and sleepiness and the Pittsburgh Sleep Quality Index (PSQI) at the first and second evaluations. On the basis of the PSQI items, the subjects were classified as good or bad sleepers and as short, normal, or long sleepers.
Results:
At baseline, 53% of the subjects reported good sleep, with 61% reporting a sleep duration of approximately 7 hr. The total sleep time and the numbers of short, normal, and long sleepers were similar at baseline and at 3 years later. Over time, there was a slight increase (p<0.001) in bad sleepers (53%) and a rise in the occasional hypnotic intake (p<0.001). Considering individual variation, the majority of subjects remained stable at follow-up for sleep duration (65%), sleep quality (75%), and medication (83%).
Conclusions:
In a healthy older population, the majority of the subjects did not report bad and short sleep at baseline and did not have significant changes in self-perceived sleep 3 years later. These findings suggest that the reported sleep disturbances described in the elderly are more dependent on physical, environmental, and health factors rather than on age-dependent sleep changes. Clinical trial registration: NCT 00759304 and NCT 00766584.
Introduction
S
Moreover, longitudinal studies have demonstrated a strong link between poor and short sleep, and mortality, 5,6 as well as vascular 7 –10 and metabolic morbidity.
Physiological studies on sleep have described subjective and objective changes within the sleep–wake cycle and circadian rhythms in the older population. As we age, total sleep time is slightly reduced compared to younger adults, with decreased amounts of slow-wave sleep, increased sleep latency, and increased nocturnal sleep fragmentation. 11 –15 These changes in sleep structure can be explained by age-related changes in sleep homeostasis and the circadian regulation of sleep, inducing a reduction in the diurnal sleep propensity and in deep sleep. 16 –18 Therefore, these physiological sleep changes in the elderly and the increases in health problems and sleep disorders with aging could explain the rise in sleep complaints commonly found in community-based studies. More than 50% of adults older than 65 years old have at least one chronic sleep-related problem, 17,18 such as sleep-related breathing disorders, which are estimated to be present in 10%–20% of the population, and insomnia and restless leg syndrome, both of which frequently increase in people older than 65 years old. 19,20 Moreover, changes in circadian rhythms have also been demonstrated with advancing age, with a decline in the cortisol and melatonin rhythms that entail alterations in day–night activity patterns. 18,21 Indeed, we can say that in the elderly, physiological sleep changes and associated medical and sleep diseases play key roles in insomnia complaints and hypnotic intake. However, as suggested by some studies, 16,22 there is with aging reduced sleep ability related to environmental factors, life changes, and associated illnesses more than real reductions in sleep time. If so, the inability to sleep and to sleep well could be considered more a consequence of poor health and environmental factors than related to aging per se. In a cohort of 9000 adults aged >65 years old, 17 42% of the participants reported difficulties in falling asleep and maintaining sleep at the first examination. In the 3-year follow-up assessment, 15% of subjects not reporting sleep disturbances at baseline had disturbed sleep, suggesting an annual increase in incidence of 5%. In contrast, in another epidemiological study of 6800 elderly people 23 complaining of insomnia and followed for 3 years, the authors found that 50% of sleep disturbances and insomnia symptoms were related to poor health, and 50% of the population reported an improvement in sleep disturbances related to improvements in general health. As recently proposed by the multi-country INDEPTH WHO-SAGE study, examining more than 40,000 older adults, 24 aging in itself did not induce sleep disturbances, and the reduced sleep ability in the older population was related to other factors, such as low income, medical illness, and medication, as well as retirement and changes in lifestyle. 25 –27
The aims of the current study were two-fold. First, using a validated questionnaire, i.e., the Pittsburgh Sleep Quality Index (PSQI), we sought to determine whether, in a group of healthy elderly people without medical and psychiatric diseases, as assessed by an extended clinical and instrumental assessment, a real reduction in sleep duration and sleep quality would occur and thereby explain the reported increased prevalence in insomnia with age. Second, we re-examined the population 3 years later to assess whether perceived sleep duration and sleep quality physiologically deteriorated during the follow-up. In performing these analyses, we might better understand the role of physiological sleep changes or associated factors in age-related sleep perception.
Materials and Methods
Participants
The participants consisted of a subset of individuals enrolled in the PROgnostic indicator OF cardiovascular and cerebrovascular events (PROOF) study, 28 which was performed to investigate the influence of autonomic nervous system activity on cardio- and cerebrovascular morbidity. This population consisted of 1011 subjects recruited from 2001 to 2003 from the inhabitants of the city of Saint-Étienne, France, and who were aged 65 years old at inclusion. The exclusion criteria were the following: Previous myocardial infarction, arrhythmia, cardiac pacemaker, stroke, neurological or psychiatric disease, insulin-dependent diabetes, magnetic resonance evaluation suggesting neurological diseases or dementia, and currently living in institutions. At the third and fourth clinical assessments, performed between 2006 and 2009 and between 2009 and 2011, respectively, the participants underwent clinical re-evaluations and they completed several questionnaires, including evaluation of sleep perception, daytime sleepiness, and the presence of anxiety and depression. Respiratory ambulatory recording during sleep was performed at the study entry and at the third evaluation to establish changes in respiratory sleep disturbances. The general practitioner was informed about the results of the study and the need to treat subjects. The decision to start or not to start continuous positive airway pressure treatment (CPAP) for obstructive sleep apnea (OSA) syndrome was done by him/her.
Subjects were excluded according to the following criteria: A non-complete PSQI questionnaire being returned; initiation of CPAP for OSA; a diagnosis of a new medical or neurological disease; being non-French speaking; and moving from Saint-Étienne. Figure 1 is a flowchart of the study. The final study population, for which we had all of the data, including polygraphy, at the third assessment, consisted of 314 subjects, aged 71.6±1.0 years old at the time of inclusion. This study sample did not differ from the total sample at the third assessment in terms of age, sex, or Epworth Sleepiness Scale (ESS) and PSQI scores.
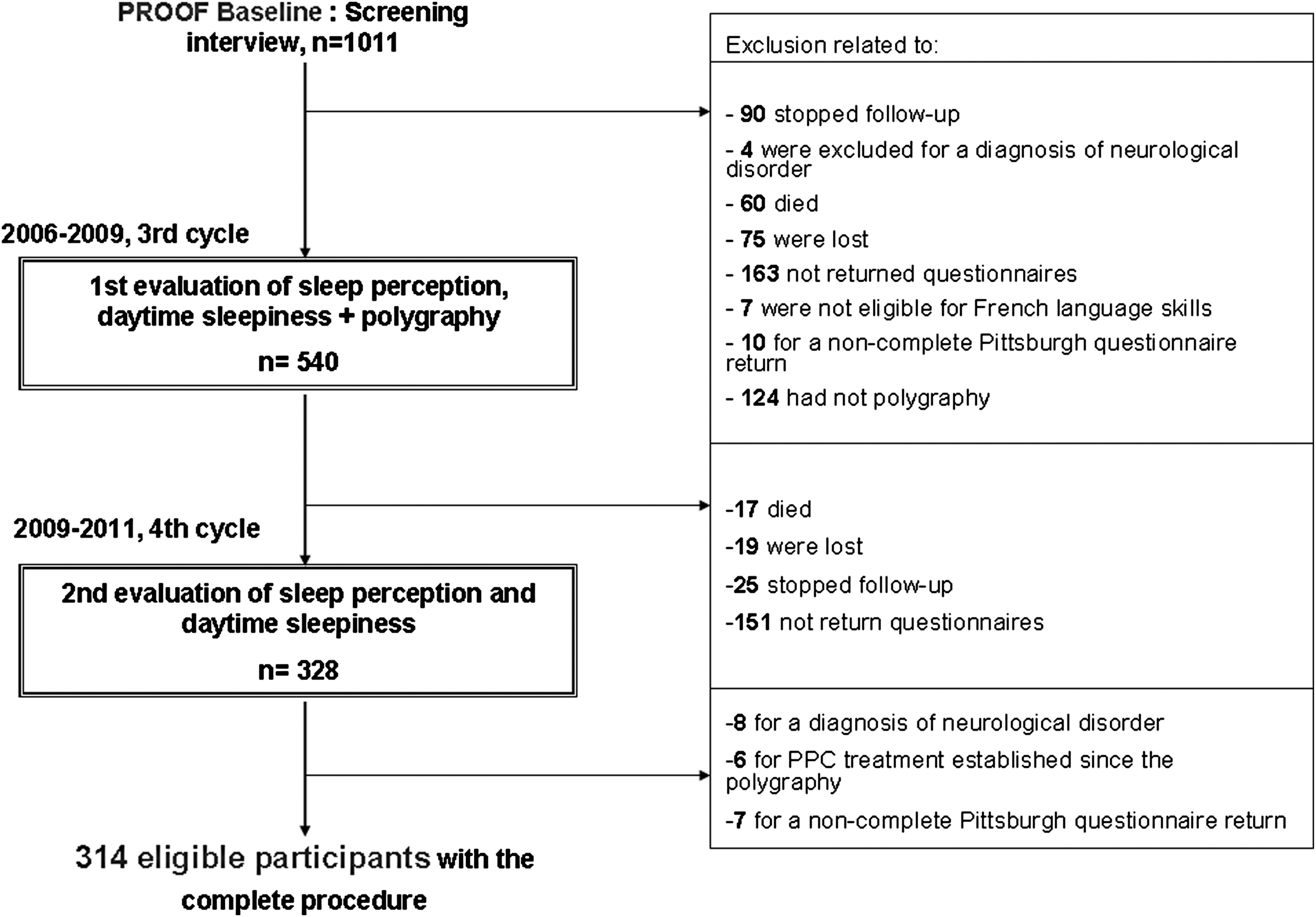
Flow chart of the participants' inclusion procedure.
The PROOF study was approved by the University Hospital and the IRB-IEC (CCPRB Rhône-Alpes Loire). The National Committee for Information and Liberty (CNIL) approved the data collection. All of the subjects provided written consent for study participation.
Methods
Self-assessment of sleep
Sleep quality and duration were assessed by the PSQI, which has been proved to have an excellent sensitivity and reliability in middle-aged subjects (see ref. 34) and in the elderly. 29,30 The questionnaire assesses subjective sleep quality and quantitative sleep–wake parameters, i.e., sleep latency, sleep duration, and sleep efficiency over the preceding month, as well as hypnotic use. A global PSQI score ranging from 0 to 21 is calculated, with higher scores indicating worse sleep. The responses to the 19 questions on the questionnaire are scaled into seven component scores (subjective sleep quality [C1], sleep onset latency in minutes [C2], sleep duration in hours [C3], percentage sleep efficiency [time spent asleep divided by the time spent in bed] [C4], sleep disturbances [such as awakenings from sleep due to discomfort or bad dreams] [C5], use of sleep medication [C6], and daytime dysfunction [C7]). These seven components are weighted equally on an ordinal scale of 0–3. The participants were divided into two groups on the basis of their total PSQI score: Good sleepers (GS), with scores of less than 5, and poor sleepers (PS), with scores of 5 or more. This threshold was established according to previously published data. 31 Sleep duration was analyzed as a categorical variable, and on the basis of the reported sleep duration, three groups were defined: Short sleepers, who slept <6 hr; normal sleepers, who slept between 6 and 8 hr; and long sleepers, who slept ≥8 h. The cutoff values for sleep duration were chosen on the basis of previous studies showing that a sleep duration less than 6 hr 32 indicated short sleep and a sleep duration of approximately 7 hr conferred a low risk for cardiovascular consequences. 33 –35
The frequencies of sleep disturbances, daytime consequences, and the use of hypnotics were quantified on the basis of the four possibilities for answers on items C5, C6, and C7. The subjects were defined as having sleep disturbances and/or daytime consequences if the frequency of these complaints was greater than two times per week. Frequents hypnotic users were defined as those using sedatives or hypnotics more than two times per week.
To obtain a more detailed picture of possible longitudinal individual differences in sleep duration, sleep quality, and hypnotic intake, the subjects were stratified into three groups according to the direction of the changes: (1) Stable condition, if the PSQI and/or the type of sleep duration or the type of hypnotic intake were stable between evaluations; (2) worsened condition, if the PSQI and/or the hypnotic intake increased and/or sleep duration became shorter; and (3) improved condition, if the PSQI and/or the hypnotic intake decreased and/or if the sleep duration became longer.
Other measurements
Clinical assessment
The clinical evaluation was undertaken with a structured interview, which included history of cardiac and cerebrovascular disease, hypertension, diabetes, and respiratory, neurological, and psychiatric disorders. Current medication was analyzed, focusing on anti-hypertensive, anti-diabetic, hypnotic, anxiolytic, and/or anti-depressant therapy. Body mass index (BMI), calculated as weight (kg)/height squared (kg/m2), and neck circumference (NC), calculated at the mid-point of the neck between the mid-cervical spine and the anterior neck 0.5 cm below the laryngeal prominence, were measured. The weight and the height were, respectively, measured using a digital medical scale and a height rod.
Anxiety and depression measurements
Depressive symptomatology was measured using the Pichot (QD2A) questionnaire, 36 consisting of 13 questions. QD2A scores ranged from 0 to 13 points, and subjects with a score >7 were considered to have depressive symptoms. Anxiety was assessed using the French version of the Goldberg scale, 37 a nine-item scale with scores ranging from 0 to 9. Individuals with scores >4 were considered to be suffering from anxiety.
Sleepiness
The impact of sleepiness during the day was evaluated using the ESS, 38 a four-grade scale ranging from 0 (no chance of napping) to 3 (high chance of napping) in eight different situations, yielding a maximum score of 24. The presence of excessive daytime sleepiness was identified with a score >10.
At-home respiratory polygraphic
An unattended ambulatory respiratory recording during sleep for OSA screening (HypnoPTT, Tyco Healthcare, Puritan Bennett, CA) was performed in all of the subjects, including sound, electrocardiogram, pulse transit time (PTT), R-R timing, nasal pressure, respiratory effort, body position, and oxygen saturation (SpO2). 39 The sleep period was defined by the individual report of the time elapsing between lights-out and lights-on in the morning following the nocturnal study. Hypopnea was defined as a 50% or greater reduction in airflow from baseline, lasting at least 10 sec and associated with at least 3% oxygen desaturation. Apnea was defined as the absence of airflow in the nasal cannula lasting at least 10 sec. The apnea plus hypopnea index (AHI) was established as the ratio of the number of apneas to hypopneas per recorded hour. An AHI >15 with at least 85% of events scored as obstructive was considered diagnostic of a sleep breathing disorder (SBD). 40 Cases were classified as mild (AHI between 15 and 30) and moderate to severe (AHI >30). 41 The oxygen desaturation index (ODI) was also established as the number of episodes of oxygen desaturation per hour of recording time during which SpO2 fell by 3% or more.
Statistical analyses
The study population characteristics are reported as the means±standard deviations (SDs) for continuous variables and as totals and percentages for categorical variables. Differences between the groups were examined with the chi-squared test for categorical variables and with the Student paired t-test for continuous variables. Pearson correlation coefficients were calculated to assess the relationships between sleep duration and quality and the various clinical and polygraphic parameters. Multiple logistic regression analysis was performed, and the dependent variable was the type of evolution of sleep duration, sleep quality, and hypnotic intake and the independent variables were sex, age, educational level, anxiety, depression, and body mass index (BMI), AHI, and ODI at inclusion.
All of the statistical analyses were undertaken using the SPSS statistical software package (SPSS for Windows, version 17.0, SPSS, Chicago, IL). After correction for multiple comparisons, two-tailed p values<0.05 were considered to indicate statistical significance.
Results
Clinical and behavioral characteristics
The characteristics of the entire study population at baseline and follow-up are shown in Table 1. At study entry, the mean age of the study population as was 71.6±1.1 years old, and 57.7% were women. The mean depression score was 2.5±2.6, the mean anxiety score was 3.8±3, and the mean ESS was 5.2±4. Thirty-two percent had anxiety, and 7% had depression. No differences were found between evaluations for the overall clinical data.
BMI, body mass index; NC, neck circumference; p, paired Student t-test or chi-squared; NS, not significant.
Concerning polygraphic data obtained at the first evaluation, the mean AHI was 15.8±12.9, the mean ODI was 8.8±8.7, and the mean SpO2 was 95.3±1.7%. None of the participants started treatment for obstructive sleep apnea during the follow-up period.
Self-reported sleep data
The data relative to perceived sleep duration and quality at baseline and follow-up are reported in Table 2. At study entry, 53% of the subjects reported good sleep, with 61% reporting a sleep duration of approximately 7 hr. At the follow-up, the total sleep time and the sleep efficiency did not change over time, with the Δ values being, respectively, −0.10±1.4 and −0.87±13.8. Moreover, 3 years later, no changes were found for the numbers of short, normal, and long sleepers. The most significant overtime change was a rise in sleep latency of approximately 3 min (p<0.001), with the values, however, still lower than that of the pathological threshold value of >30 min commonly used to define insomnia. There was a significant increase in sleep medication at follow-up (p<0.001), which was related to a rise only in occasional intake (10% vs. 15%). The percentage of subjects taking regularly hypnotics did not change between the first (13%) and second evaluations (12%).
p, paired Student t-test or chi-squared; PSQI, Pittsburgh Sleep Quality Index; NS, not significant.
The most important 3-year change was the significant increase in the mean PSQI from the baseline value of 5.9±3 to 6.4±3 (p=0.002). The PSQI changes were related to the increase in BS (p<0.001) and the consequent reduction in GS (p=0.004). Despite the significant decrease in sleep quality over time, approximately 47% of the participants still reported good sleep.
To assess the degree of longitudinal changes, we examined the individual variations in sleep quality, duration and hypnotic intake. As illustrated in Fig. 2, the majority of the subjects remained stable at follow-up for sleep duration (65%), sleep quality (75%), and medication (83%), with a small percentage of subjects showing deterioration in sleep duration and quality and/or an increase in occasional medication intake.
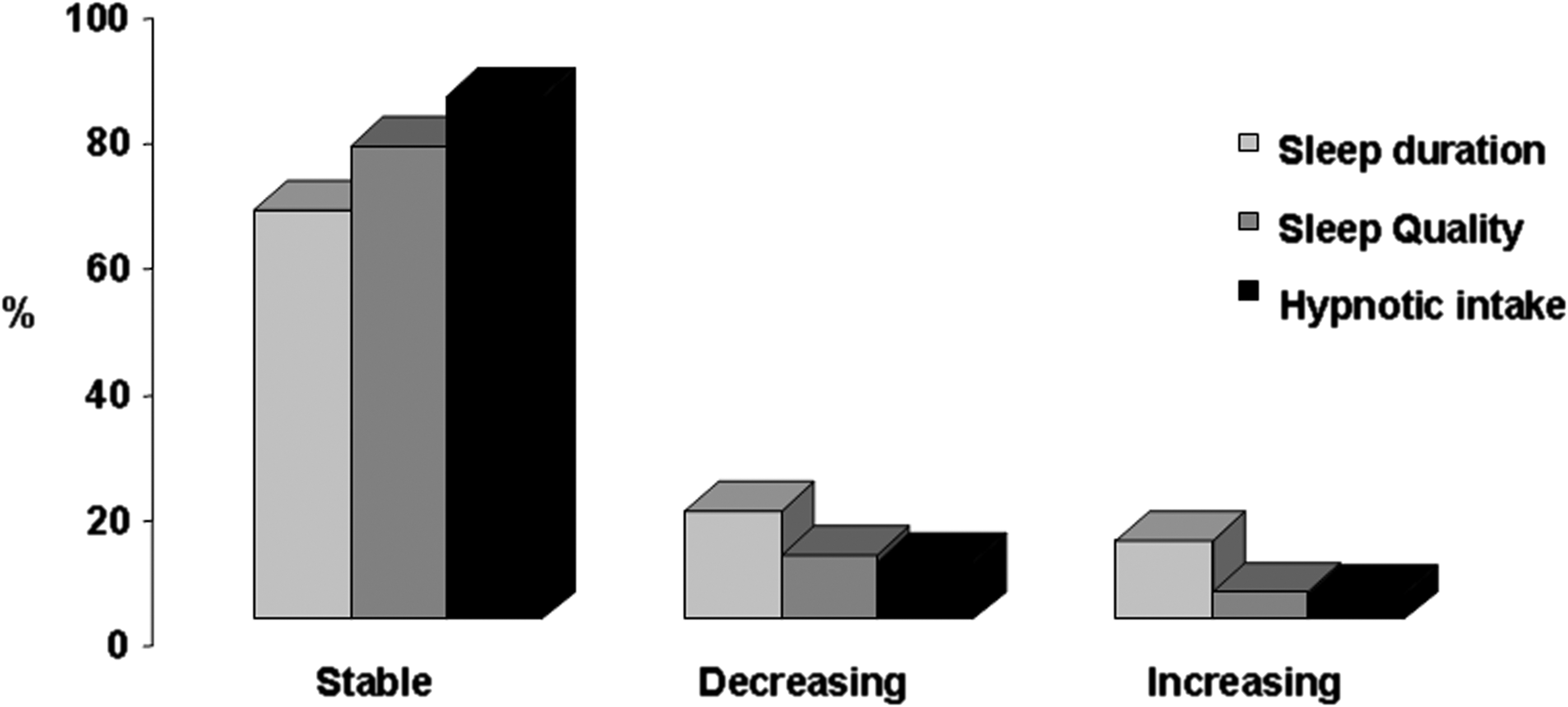
Sleep duration, sleep quality, and the use of hypnotics according to the longitudinal direction of changes.
Figure 3 demonstrates the changes in sleep disturbances, daytime functioning, and type of hypnotic intake, as derived from items C5, C6, and C7 of the PSQI. There was a slight but significant increase in sleep disturbances and in occasional hypnotic intake, without any effects on daytime functioning.

Longitudinal changes in the use of hypnotics, sleep disturbances, and daytime consequences. The p value=chi-squared test; (*) p<0.001.
To determine whether some clinical and polygraphic data at baseline might have affected the degree of changes in sleep duration and quality, multiple logistic regression was performed between the degree of sleep changes and sex, AHI, ODI, BMI, hypnotic intake, and the presence of anxiety and depression (Table 3). None of these variables at baseline significantly affected the evolution of perceived sleep quality or duration at follow-up; the anxiety and depression scores showed a trend toward being higher in the worsened group, however without statistical significance.
Expressed in kg/m2 and centered at the mean value.
Oxygen desaturation Index >15.
Apnea plus hypopnea Index >15.
Based on the Goldberg scale with a score above 4 points.
Based on the Pichot QD2A questionnaire with a score above 6 points.
Based on the Epworth Sleepiness Score questionnaire with a score above 10 points.
OR, Odds ratio; CI, confidence interval; odds ratios significant at p<0.05.
Discussion
This study was novel research examining the changes over time in self-reported sleep, hypnotic intake, and diurnal consequences in a healthy elderly population without complaints of insomnia. The first interesting finding was that approximately 53% of our population reported good sleep at the first examination, suggesting that elderly subjects without health problems are unlikely to report sleep problems and insomnia. Second, despite a slight but significant deterioration in sleep quality at follow-up, the size of the reported decrease was relatively small, with 65% or more of the subjects reporting stability in sleep duration, sleep quality, and hypnotic medication, as well as in daytime functioning. Last, the changes in sleep perception were independent of factors that might have affected sleep, such as the presence of SBD, anxiety or depression, and sex. This finding in our healthy elderly suggests that the variation in sleep perception and the reported rise in insomnia complaints in the elderly population are more modulated by external or lifestyle factors affecting perceived health than by age-related changes in sleep.
Several studies have shown that sleep-related complaints are common among older subjects compared to younger people, with approximately 65% of adults older than 65 years old reporting insomnia symptoms. 42 These disturbances have been explained by age-related changes in sleep need and structure, 16 including more sleep fragmentation, earlier awakening, less slow-wave sleep, and circadian advancement. 43 –45 However, in a large study including more than 30,000 adults, 46 the authors found that participants aged older than 65 years old reported similar rates of poor sleep quality and a poor sense of well-being, compared to subjects younger than 65 years old. In addition, Buysse and colleagues 47 found that 68% of healthy older adults rated their subjective sleep as “good.” Similarly, Vitiello and co-workers 48 reported that elderly people without medical or psychiatric diseases did not complain of sleep problems. A study comparing sleep satisfaction among young and elderly subjects reported that elderly subjects reported greater satisfaction with their sleep, compared to young adults. 49 More recently, Grandner and co-workers, 27 examining a large population of 155,877 participants, found that advancing age was not associated with increased self-reported sleep disturbances and fatigue or lack of energy, confirming that sleep problems and the course of sleep quality in the elderly are mediated by other factors beyond physiological sleep changes. 50
In agreement with these data, the first finding of our study was that 53% of our subjects defined themselves as good sleepers and 61% had normal sleep durations at the first evaluation. Interestingly, the self-perception of sleep affected neither the ESS nor the presence of daytime dysfunction, stressing again the role of medical and environmental factors affecting health status and well-being in the reported fatigue, tiredness, and sleepiness of the elderly. 47
Second, although an increase in subjects reporting bad sleep was found in our sample 3 years later, the degree of the changes was slight, indicating a lack of significant and worse sleep deterioration with aging.
An interesting point raised from this study is that the self-evaluation of sleep by some questionnaires, such as the PSQI, yields information about several measurements of sleep, including sleep latency, total sleep time, and sleep quality or satisfaction, which reflect a subjective global appraisal of several nights of sleep. Moreover, the consistency of the sleep perception in our elderly population across evaluations stresses the validity of the PSQI in the longitudinal assessment of sleep perception, as well as the application of this tool in epidemiological studies on aging.
Strengths and limitations of the study
The first strength of our study was that our participants were recruited from a community-dwelling population, and strict exclusion criteria were applied, ensuring a homogeneous age (>65 years) and educational level (11 years), with the exclusion of subjects with neurodegenerative diseases, as confirmed by magnetic resonance imaging (MRI) evaluation, and the lack of treatment for sleep disorders, such as restless leg syndrome and sleep apnea, at baseline and follow-up. These exclusion criteria were chosen to obtain a sample of participants who were physically functional and without other medical problems that could affect sleep.
This study, alternatively, suffered from limitations inherent to longitudinal design. First, compared to the population at study entry, the sample completing the PSQI questionnaire at baseline and follow-up was smaller, not allowing us to draw stronger conclusions. Second, we used a questionnaire to assess sleep duration and quality that did not allow for the estimation of sleep structure and that did not differentiate time asleep from time in bed or estimate the number and duration of naps. Although actigraphy might be considered a simple method to assess sleep structure better, 51 researchers agree that self-estimation of sleep by specific questionnaires, such as sleep diaries 52 or the PSQI, 30 are useful methods for assessing subjective sleep and sleep disturbances in large samples.
In conclusion, our data demonstrate that, in a healthy elderly population, self-reported sleep estimations did not reveal a large number of sleep complaints, suggesting that older adults are likely to have poor and short sleep when medical disease, environmental, and lifestyle factors occur. Moreover, advancing age was not associated with an increase in sleep disturbances, with the majority of our elderly not reporting significant changes in sleep duration, sleep quality, hypnotic intake, or daytime functioning over the long term. Further research directly comparing elderly good sleepers to elderly insomniacs is necessary to elucidate the mechanisms implicated in the sleep changes observed with increasing age.
Footnotes
Acknowledgments
This study was supported by a grant from the French Ministry of Health (Cellule Projet Hospitalier de Recherche Clinique National, Direction de la Recherche Clinique, CHU Saint-Etienne; Appel d'Offre 1998 and Appel d'Offre 2002) and by a grant from the “L'Association de Recherche SYNAPSE” (President, Michel Segura).
Author Disclosure Statement
This was not an industry-supported study. None of the authors declares any financial conflicts of interest.