
Abstract
The global population is aging, and although age remains the primary risk factor for all major causes of death, no priorities for aging research exist. After reviewing the literature on mortality modeling, we found that different chronic processes underlie mortality before and after reproductive age. To identify priorities in aging research, we propose a simple ranking method that uses the percentage of deaths attributable to each disease for the over 60 population on the basis that, rather than being the result of individual risk factors, these deaths are largely due to underlying senescent processes. Our ranking suggests that vascular aging, led by ischemic heart disease and stroke, is the most important focus for aging research. The availability of funding, however, is not currently aligned with health priorities, and we believe that rectifying this disconnect may improve societal health outcomes.
Introduction
L
We support the view that aging results from the accumulation of damage due to normal metabolism. 1 With this in mind, it would be ideal to prioritize the various types of damage that lead to aging. Unfortunately however, biomarkers of aging damage are not standardized, and there has been no large-scale collection of these data. Instead, we propose to prioritize causes of death (COD)—primarily diseases—for which high-quality data are available as collected by national governments and consolidated by the World Health Organization (WHO). Disease priorities will be calculated using burden of disease data from Australia. 2
An obvious benchmark for prioritizing diseases would be to rank them by the percentage of deaths or disabilities they cause over all age groups. Given that age is the strongest predictor of mortality, it would be logical to expect that this ranking approach is reasonably accurate. However, there are some diseases that do not increase with age, for example pregnancy-related deaths. Others, like falls, are more ambiguous, with early-life deaths generally associated with accidents, whereas late-life deaths are associated with a frail musculoskeletal system. Diseases such as lung cancer increase strongly with age throughout adult life, but a large proportion of these deaths can be attributed to risk factors such as smoking. We conducted a literature review of mortality modeling research with the goal of identifying algorithmic tools that would highlight the proportion of mortality driven by the aging process.
Literature Review
In 1825, Gompertz showed that the age-specific mortality rate grows exponentially throughout adult life at a relatively constant rate. 3 Simply put, an adult's chance of dying increases by around 11% per annum. However, looking at mortality curves for specific diseases, we find that they have widely varying growth rates and many are not exponential. Research by Simms 4 and Kohn 5 analyzed and categorized specific disease mortality curves in an effort to understand the underlying causes of mortality.
Horiuchi et al. drilled down further into the data and found that there are significant changes in the rate of growth of mortality for specific diseases over the human life span. 6 They hypothesized that, on the basis of evolutionary theory, different causes of death would exhibit different growth rates before and after reproductive age, thus reflecting the characteristics of underlying chronic processes. The following is a high-level summary of those diseases that showed a significant change in the growth rate of mortality between middle age (30–54) and old age (65–89). Diseases that accelerate in old age include: Dementias, e.g., Alzheimer disease; infectious diseases, e.g., influenza; frail musculoskeletal system, e.g., falls; digestive system, e.g., bowel obstruction; genitourinary system, e.g., kidney. Diseases that decelerate in old age include: Lifestyle diseases, e.g., liver damage caused by heavy drinking, lung cancer caused by smoking, type 2 diabetes caused by obesity; disease history, e.g., hepatitis, rheumatic heart disease; genetic frailty, e.g., multiple sclerosis, some cancers. Horiuchi et al.'s interpretation of the results suggested that diseases accelerating in old age are dominated by underlying senescent processes and those that decelerate in old age are dominated by individual risk factors.
Prioritization method
While Horiuchi et al. did not have disease prioritization in mind, we felt that their analysis might be used to identify those diseases that are largely age related. In terms of ranking, we rejected using the disease-specific mortality growth rate in old age, because this would overweight those diseases whose mortality rises dramatically in old age but from a very low starting level, e.g., bowel obstructions. Adjusting the mortality data to allow for risk factor-associated deaths was also rejected; the Australian mortality dataset includes statistics on the deaths associated with 14 risk factors, but this is still limited and does not include data for disease history and genetic frailty.
Two simple ranking methods were chosen; diseases are ranked by the percentage of deaths they cause for those aged: (1) 60 years and over, post-reproductive age; (2) 85 years and over, the oldest old. The first ranking method, based on the work of Horiuchi et al. 6 assumes that deaths in post-reproductive age largely result from underlying senescent processes and excludes reproductive age deaths that are more closely associated with individual risk factors and accidents. The second method is based on further work by Horiuchi, which demonstrated that there are significant differences between the COD for the old (65–84 years) and the oldest old (85+ years). 7 We believe that the deaths of those aged over 85 years are more representative of underlying senescent processes. However, it should be noted that less theoretical support exists for the assumptions behind this second measure.
The background research used to develop our ranking method is based on mortality data and not disability data. However, we have assumed that our method will also apply to disability-adjusted life years (DALYs) data, which provides a measure of the disability and life expectancy lost to diseases rather than just mortality.
Results and Discussion
The ranking methods described above were applied to all 155 COD given in the Australian burden of disease data for both mortality and DALYs.
2
The complete results may be downloaded from our website (
Figure 1 shows a high-level visual summary, and the key findings are presented in brief below: • In general, the diseases found to accelerate in old age increase in ranking both for deaths over the age of 60, and those over the age of 85. • Diseases found to decelerate in old age reduce in ranking. Although cancer remains the second highest ranked category, there is a dramatic reduction in the percentage of deaths attributed to cancer for those aged over 85. • Cardiovascular disease is the highest ranked category for all rankings and increases to over 50% of deaths for those over the age of 85. The major cardiovascular diseases have a high mortality growth rate throughout the duration of the human life span, rather than accelerating in late life. • Just two vascular diseases, ischemic heart disease (IHD) and stroke, exceed the old age rankings for cancer and all other disease categories, which together include 146 COD.
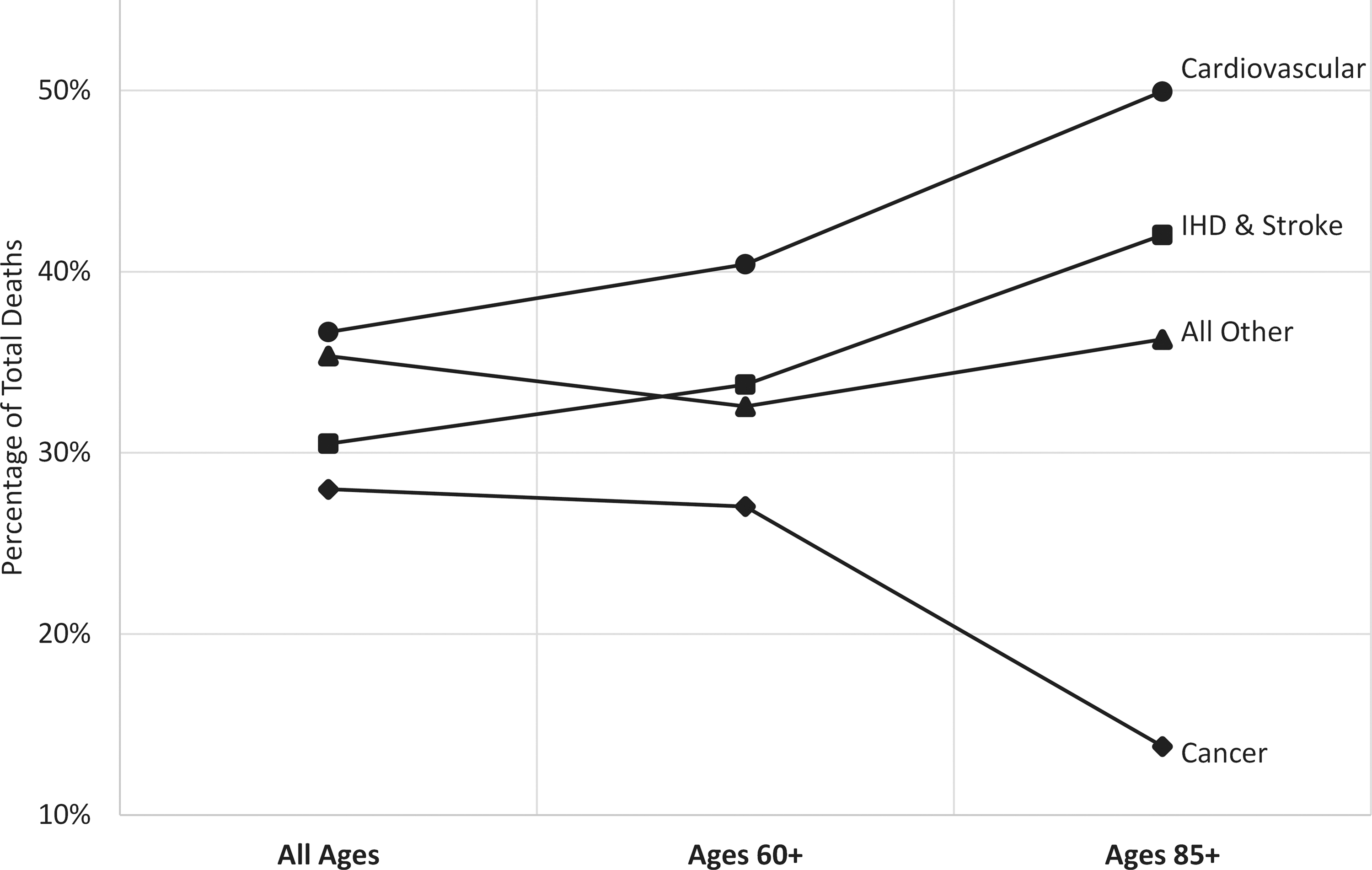
Percentage of total deaths represented by major disease categories for: (1) All ages, (2) population over the age of 60, and (3) population over the age of 85. Ischemic heart disease (IHD) and stroke, predominantly resulting from vascular aging, are highlighted as a subcategory of cardiovascular disease.
The rankings using DALYs rather than mortality are largely aligned, although there are a few interesting differences: • After cardiovascular disease and cancer, the third largest category of DALYs for all ages is mental illness at 13%, with anxiety and depression representing the major disabilities. However, as with suicide in the mortality statistics, we see that the ranking for mental illness for those over the age of 60 drops dramatically to just over 1%. This suggests that mental illness is not driven by senescence. • Another category that is prominent when measured using DALYs is sense organ disorders, including blindness and hearing loss. This category has a ranking of around 5% through the three rankings, with genetic factors being important in early life, and age-related factors, for example macular degeneration, important in old age.
We were surprised that there was a reduced ranking for cancer in the oldest old; however, it was found that much work has gone into confirming this relative decline and the possible reasons for it. 8 It appears that individual risk factors play a part in the middle age rise in mortality, but this is also the case with cardiovascular disease. It also appears that the virulence of cancer in old age is impacted by general senescence, which limits the proliferative potential of cells and the angiogenesis required for tumor growth.
The clear dominance of the two highest ranked age-related diseases, IHD and stroke, has led us to focus our research and investments exclusively on vascular aging. Dementia is the third-placed disease for those over the age of 85 and, while not fully understood, appears to have a major vascular component. Several other blood barrier and filter diseases are also highly ranked.
From the outset, we assumed that medical research funding would be largely aligned with those priorities implied by the burden of disease reports that have been produced by WHO for over a century. However, Gillym et al. in 1996, found that only 39% of National Institutes of Health (NIH) funding variance was explained by DALYs in the United States. 9 Even after demands from the US Congress in 1998 for this disparity were corrected, a decade later the rate had further dropped to just 33%. This disparity is highlighted in the case of IHD and stroke, which together represent 33% of mortality, but received only 6% of NIH funding in 2006. These disappointing findings showed that, for whatever reason, politicians and scientists are unwilling or unable to align research funding with the burden of disease on society. Nevertheless, they also highlight the opportunity to improve research outcomes in future.
Footnotes
Author Disclosure Statement
The author is an owner of an investment company, Leading Technology Group, which intends to make investments in this field.