
Abstract
The aims of this study were to analyze the effects of two different training protocols—vibratory platform and multi-component training—and to determine what kind of training creates greater adaptations on bone density and isokinetic strength of the knee extensors and the stabilizer muscles of the ankle joint in post-menopausal women. Thirty-eight women (59.8 ± 6.2 years) were randomly assigned to whole-body vibration group (WBVG), multi-component training group (MTG), or a control group (CG). The experimental groups performed incremental training for 12 weeks, three sessions/week. Significant differences were found in total fat mass and total lean mass in the training groups. In addition, both WBVG and MTG showed significant increases in isokinetic strength for knee extensors at 60°·s−1 and at 270°·s−1. With respect to the ankle joint, a significant increase for eversion at 60°·s−1 and inversion at 60°·s−1 was found in both training groups, and eversion at 120°·s−1 only in WBVG (p = 0.012). There were no significant differences between WBVG and MTG in knee and ankle strength tests. Therefore, we found significant adaptations to whole-body vibration and multi-component training in the present study. However, the improvements were similar for both groups and we cannot claim that WBVG is better than MTG, or vice versa.
Introduction
O
The deficit in lower body strength is considered the most relevant factor in the elderly, with post-menopausal women being the most affected. 5 For example, muscular strength reduces by 15% per decade after 50 years old and by 30% after 70 years. The strength loss is one of the main symptoms of sarcopenia,6–8 with a major incidence in old women. Another disease associated with age and women is osteoporosis, and one of its symptoms is the decrease of bone mass, intensifying the risk for fall fractures. 9 Estrogen deficiency in menopause induces instability between resorption and bone formation in such a way that the amount of bone removed during the remodeling cycle is slightly higher than what is renewed. 10 Women present less bone mineral density (BMD) than men in all age groups and suffer an accelerated loss during the 5 years after menopause as a result of hormonal changes that happen during this stage.11,12
In this regard, neither body weight nor physical activity is independent of muscle mass, but it is true that muscle forces place greater loads on bones than do gravitational forces associated with weight. The formation and development of skeletal tissue is a continuous and dynamic process that involves the participation of hormonal, nutritional, behavioral, and environmental factors. The central piece of bone regulation is the feedback loop between bone deformation (tissue strain) and bone strength. During growth, this homeostatic system is continually forced to adapt to external challenges. The theoretical background for this approach is provided by the mechanostat theory, which proposes that bones adapt their strength to keep the strain caused by physiological loads close to a set point. Because the largest physiological loads are caused by muscle contractions, there should be a close relationship between bone strength and muscle force or size. 13
Many strategies have been used against bone reduction, however, as reflected by Schoenau. 13 Physical activity, which produces muscle adaptations, is the most effective tool to prevent the effects of aging. 14 With practice, both physical condition and quality of life improve 15 without adversities from medicines and their lack of effectiveness. Strength training in older adults is the most efficient procedure for improvement of muscle mass and therefore bone mass, because the mechanical load that is produced on bone structure contributes to the osteogenesis process.16–23
In this sense, between different methods for improving the strength, whole-body vibration (WBV) training contributes to an increase in BMD.24–27 It has been shown that vibration is an appropriate stimulus to generate bone formation. Tanaka et al. 28 and Kaspar et al. 29 studied its effect on bone and concluded that vibratory stimuli favor the proliferation of osteoblasts, producing improvements in BMD. On the other hand, the effects of WBV training programs are determined by neural adaptation and possible hormonal and biochemical changes. WBV exercises cause excitation of the primary endings of muscle spindles (whose afferent feedback stimulates increased discharge of α-motor neurons) as well as activation of Golgi tendon organs (GTO), which are sensitive to force development and whose activation results in inhibition of muscle action. 30 In addition, different studies provide improvements on the strength of the knee extensors.31,32 However, there is no agreement in the literature defining the program that determines the optimum vibration, such as a greater effectiveness when compared to traditional protocols. Thus, there is a need to continue research into this type of training and the effects it has on the different types of population.
Despite the fact that vibratory training may be an appropriate strategy for improvement of BMD with shortened working time, in the last years, training programs combining different exercise modalities (multi-component training) appear to be an effective training system to avoid loss of BMD,33–39 decrease body fat, 36 and improve strength levels. 40 In previous studies addressing multi-component training, the authors suggest that high-impact activities (such as jumps, climbing stairs, jogging, and hopping exercises) combined with dynamic maximum strength, balance, agility, or aerobic training is an effective way to maintain or increase muscle strength and to prevent bone fragility in post-menopausal women.4,41
The effects of vibration and multi-component training on strength and body composition have been studied separately among different age groups, including post-menopausal women. However, there are no studies that have compared the effects of the vibration versus combined training on these variables. Thus, in view of the great methodological differences in relation with the ideal program as a natural therapy to prevent the loss of strength and BMD, the aims of this study were to: (1) Analyze the effects of two different training protocols (vibratory platform and multi-component training) and (2) determine what type of training creates greater adaptations on bone density and the isokinetic strength of the knee extensors and the stabilizer muscles of the ankle joint in post-menopausal women.
Methods
Experimental design
A quasi-experimental intra- and inter-subjects design with pre- and post-test, 12 weeks, with a control group, was conducted. Participants were matched by BMD and were randomly allocated to three groups: Whole body vibration group (WBVG) (n = 28), multi-component training group (MTG) (n = 23), and control group (CG) (n = 13).
Body composition measurements were performed, and later, isokinetic concentric strength of the knee extensors was measured and ankle function tests were executed. All tests were administered by the same investigator. All participants were instructed to maintain their normal daily routines and dietary intake.
Subjects
Sixty-four post-menopausal women (considering post-menopausal as the period comprising the years following the year after the cessation of menstruation) were recruited by non-probability convenience sampling. Exclusion criteria included: Presenting a high level of osteoporosis (BMD <70 grams/cm2), being treated for a disease that can affect bone structure or neuromuscular system, having orthopedic prosthetic implants in the lower limbs and/or spine, having herniated discs, suffering ocular diseases that affect the retina, suffering severe cardiovascular diseases, suffering from epilepsy, having a pacemaker or osteosynthesis material, practicing some type of physical activity regularly, and frequency of participation in the stipulated program lower than 90% (participants who missed more than 10% of the training sessions were excluded). Before the onset of the study, all subjects signed an informed consent document about how training and assessments would be developed. The study design was approved by the Human Subjects Ethics Committee of the Local University.
Bone mass density
Initially, the height and weight of the participants were obtained. Later, subjects were placed in the supine position on a table and bone mass density was measured by dual-energy X-ray absorpiometry (DEXA; XR-46, Norland Corp., Fort Atkinson, WI). The DEXA scanner was calibrated using a lumbar spine phantom. Participants had to maintain a static position for 8 min (duration of the test). Total bone, fat and lean (body mass − [fat mass + bone mass]) masses were assessed from the whole body scan. Areal BMD (BMD = grams · cm−2) was calculated using the formula BMD = BMC × area−1. In addition, body mass index (BMI = height/weight2) was calculated.
Isokinetic strength
For isokinetic strength measurement, a Biodex System 3 Pro isokinetic dynamometer (Biodex Medical System, NY) was used. Concentric isokinetic strength was evaluated in the right knee and ankle joints. The dynamometer was calibrated prior to testing according to recommendations outlined by the manufacturer, and gravity correction was performed as described in the Biodex test manual. The axis of rotation of the dynamometer lever arm was aligned with the anatomical axis of the knee and ankle.
A specific warm-up was performed prior to tests (8 min on a cycle ergometer at moderate intensity, active and passive stretching, and joint mobility of the lower limbs). Each subject performed a familiarization at the test velocity to become accustomed to the movement. Participants were instructed to generate maximum force as fast and as hard as possible.
For isokinetic strength measurement in knee extension, the joint range was 90°, where 0° was up to the full extension. Participants sat on the seat and were held in with straps around distal trunk and thigh, to avoid movement of the body. The check consisted of one set of five maximal concentric knee flexion and extension repetitions at 60°·s−1 and 270°·s−1.
In addition, isokinetic strength in eversion and inversion was evaluated. For this, subjects remained seated at 90° for hip and knee joints. The thigh and foot were secured and supported so that the ankle was placed at 90° with regard to the leg (tibia perpendicular to the sole of the foot). Once the limits of the joint were marked, the ankle was placed from a neutral position, and an inversion movement followed by eversion was performed. The test consisted of one set of five maximal concentric ankle eversion and inversion repetitions at 60°·s−1 and 120°·s−1.
Between trials, a 2-min rest period was imposed. Verbal encouragement was given during the test. The peak concentric torque obtained for each test. Isokinetic strength was normalized relative to body mass (kgf · N · m−1) (in newton-meters per kilogram).
Training
The total duration of the intervention phase was 12 weeks. The experimental groups were exposed to a training stimulus with a frequency of three sessions per week and a total volume of 36 sessions. Rest period between each training day was at least 24 hr and a maximum of 72 hr. Before training sessions, participants performed a specific warm-up consisting in 8 min on a cycle ergometer at moderate intensity followed by stretching and joint mobility of the lower limbs.
WBV training
The WBVG exercised on a sinusoidal vertical vibration platform (Power Plate Next Generation; Power Plate North America, Northbrook, IL). During sessions, subjects stood on the platform holding a half-squat (knee and hip angle 120°). The arms remained crossed and parallel to the floor with a shoulder flexion of 90°, without using the handholds of the platform during the training. Then, participants performed ankle plantar and dorsal flexion with the following work sequence (establishing a rhythm of 100 beats per minute [bpm]: 1 bpm for the concentric phase and 5 bpm for the eccentric phase). The amplitude (4 mm), working time (60 sec), and recovery time (60 sec) parameters remained constant for the 12 weeks of training. The training intensity was 35 Hz. 42 Familiarization lasted for the first 2 weeks, being the working time of 45 sec. The training volume was increased by increasing the number of series per session (five sets at the beginning and increasing by eight sets the last weeks).
Multi-component training
After the warm-up and prior to aerobic activity, MTG participants performed a progressive program of vertical jumps. During the first month, small reactive vertical jumps (without knee and ankle flexion) were executed. Later, subjects performed drop jumps progressively starting at a height of 5 cm and finishing at 10 cm at the end of the program (increases of 5 cm each month). The sets increased from 4 × 10 drop jumps to 6 × 10 each week. The drop jumps were the same each month, but the load progression (imposed by height) was undulatory (the load increased during 3 weeks and decreased during 1 week).
After drop jumps, the aerobic exercise took place. 43 The load increased progressively over the 12 weeks. Subjects walked at an intensity range between 50% and 60% of reserve heart rate (maximum heart rate − resting heart rate) and the volume ranged between 30 and 45 min. The training intensity was established through the gait speed after an initial test with training computer/heart rate monitor prior to training.
Statistical analyses
Statistical analysis of data was performed with SPSS 15.0 (Chicago, IL) in the MS Windows environment. A descriptive analysis was performed to detail and analyze the characteristics of the sample participating in the study.
For the inferential analysis, a Kolmogorov–Smirnov test was performed to establish the normality of sampling distribution and analysis of runs to observe the independence of observations. To determine the effect of independent variables on the dependent variable, repeated analysis of variance (ANOVA) measurements (general linear model) were carried out for the entire sample. If there were statistically significant differences (p ≤ 0.05) for the time factor, an ANOVA test was performed to assess repeated measures of each group to differentiate between pre-test and post-test. If there were statistically significant differences (p ≤ 0.05) for time × , a group factor ANOVA and Tukey post hoc test were performed to see if there were significant differences between groups. Power (1−β) was determined for all variables and effect sizes were calculated using eta square (d).
Results
A total of 38 women completed training programs and all of the assessments. The distribution of the sample was homogeneous in terms of number of participants. Twenty-six subjects dropped out during the training period for personal reasons or health problems (Fig. 1). None of the drop outs left the program as a result of injuries or adverse responses to the treatment. The characteristics of the final subjects at baseline are represented in Table 1.
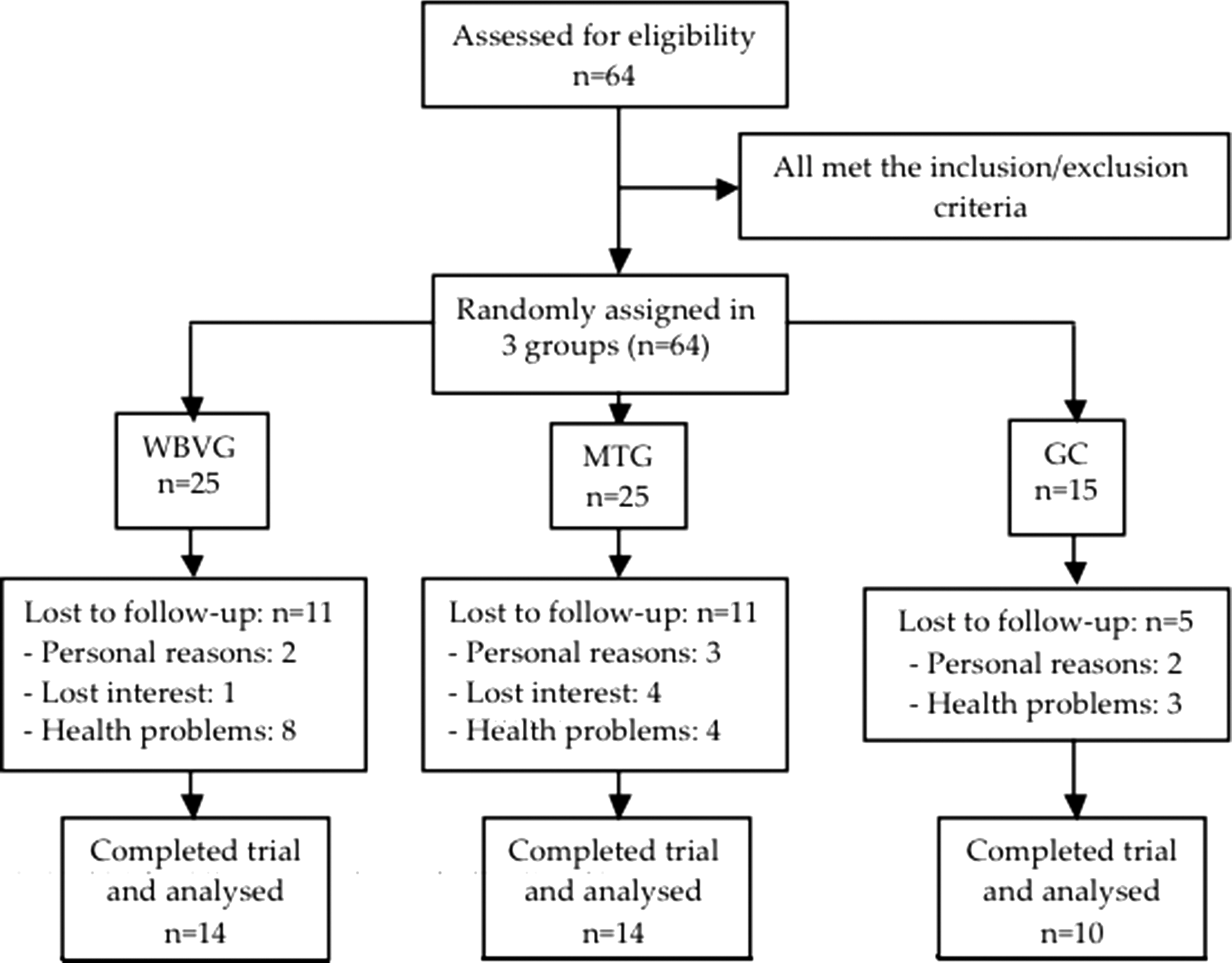
Trial profile.
Values are given as mean (standard deviation [SD]).
BMI, body mass index; WBVG, whole-body vibration group; MTG, multi-component training group; CG, control group.
Bone mass density
There were no changes in total BMD in either group (Table 2). Significant differences were found in total fat mass (WBVG, p = 0.001, d = 0.58, 1−β = 0.98; MTG, p = 0.026, d = 0.04, −β = 0.11) and total lean mass (WBVG, p = 0.001, d = 0.60; −β = 0.98; MTG, p = 0.013, d = 0.34, −β = 0.67) between pre- to post-test in the training groups. There was a significant decrease in body fat (%) only in the WBVG (p = 0.001, d = 0.78, −β = 1.0). There were significant differences between the WBVG and CG in total fat mass (p = 0.001) and lean mass (p = 0.016).
Values are given as mean (standard deviation [SD]).
Significant difference from pre- to post-training (p ≤ 0.05).
Significant difference from pre- to post-training (p ≤ 0.01).
Significant difference from WBV (p < 0.05).
WBVG, whole-body vibration group; MTG, multi-component training group; CG, control group; BMD, bone mineral density; Δ, change.
Isokinetic strength
Knee
Concentric isokinetic strength for knee extensor is presented in Table 3. In the training groups, an increase was found in the peak torque in extension at 60°·s−1(WBVG, p = 0.021, d = 0.25, 1−β = 0.49; MTG, p = 0.011, d = 0.34, 1−β = 0.67) and extension at 270°·s−1 (WBVG, p = 0.002, d = 0.46, 1−β = 0.87; MTG, p = 0.001, d = 0.62, 1−β = 0.99). With respect to peak torque per body weight, there was an increase in extension at 270°·s−1 in the experimental groups (WBVG, p = 0.006, d = 0.41, 1−β = 0.80; MTG, p = 0.001, d = 0.64, 1−β = 0.99). Figure 2 presents relative gains in the peak torque between the pre-test and post-test for each group.
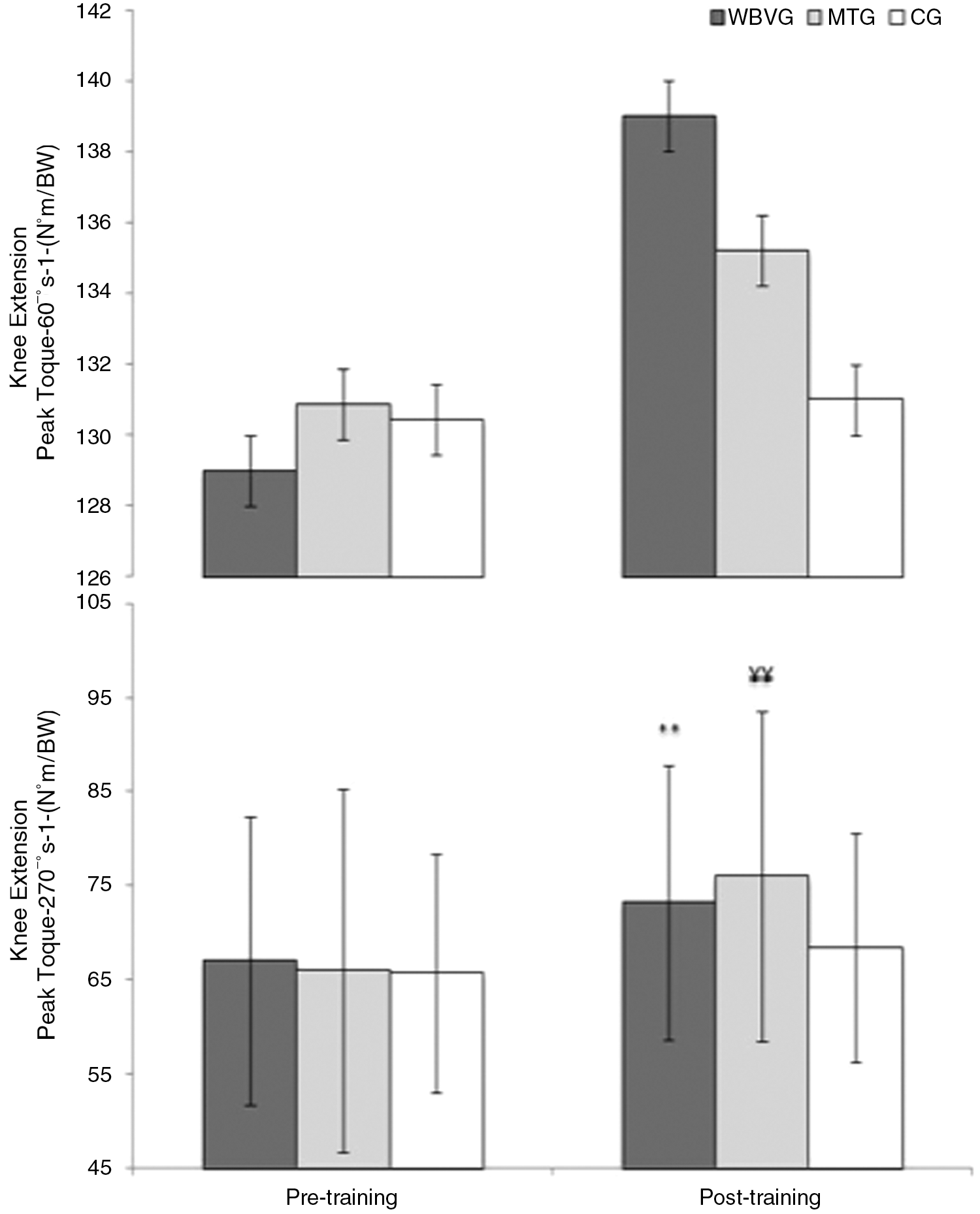
Changes in isokinetic peak torque for knee extension at angular velocities of 60°·s−1 and 270°·s−1 for each group. (*) Significant difference from pre- to post-training (p ≤ 0.05) in the whole-body vibration group (WBVG); (**) significant difference from pre- to post-training (p ≤ 0.01) in the WBVG; (¥) significant difference from pre- to post-training (p ≤ 0.05) in the multi-component training group (MTG); (¥¥) significant difference from pre- to post-training (p ≤ 0.01) in the MTG.
Values are given as mean (standard deviation [SD]).
Significant difference from pre- to post-training (p ≤ 0.05).
Significant difference from pre- to post-training (p ≤ 0.01).
WBVG, whole-body vibration group; MTG, multi-component training group; CG, control group; Δ, change.
Ankle
Table 3 presents gains in peak torque for eversion and inversion for the experimental between the pre-test and post-test. In the training groups was found a significant increase for eversion at 60°·s−1 (WBVG, p = 0.001, d = 0.64, 1−β = 0.99; MTG, p = 0.003, d = 0.36, 1−β = 0.71), inversion at 60°·s−1 (WBVG, p = 0.015, d = 0.42, 1−β = 0.78; MTG, p = 0.044, d = 0.20, 1−β = 0.39), eversion at 120°·s−1 only in WBVG (p = 0.012, d = 0.42, 1−β = 0.76). In relation to relative gains in the peak torque, there were differences between pre- to post-test in the training groups during the concentric contraction of eversion at 60°·s−1 (WBVG, p = 0.001, d = 0.18, 1 − β = 0.33; MTG, p = 0.003, d = 0.50, 1−β = 0.12), inversion at 60°·s−1 only in WBVG (p = 0.021, d = 0.45, 1−β = 0.82) and eversion at 120° · s−1 only in WBVG (p = 0.027, d = 0.38, 1−β = 0.70). Figure 3 presents relative gains in the peak torque between the pre-test and post-test for each group.

Changes in isokinetic peak torque for eversion and inversion at angular velocities of 60°·s−1 and 120°·s−1 1 for each group. (*) Significant difference from pre- to post-training (p ≤ 0.05) in the whole-body vibration group (WBVG); (**) significant difference from pre- to post-training (p ≤ 0.01) in the WBVG; (¥) significant difference from pre- to post-training (p ≤ 0.05) in the multi-component training group (MTG); (¥¥) significant difference from pre- to post-training (p ≤ 0.01) in the MTG.
There were no significant differences between the WBVG and MTG in knee and ankle strength tests. No significant differences were found in the CG between pre- and post-test in any of the strength measurements.
Discussion
The aims of the present study were to analyze the effects of two training protocols, WBV and MT, during 12 weeks on bone density, and isokinetic strength of the knee extensors and stabilizer muscles of the ankle joint, and to determine which training protocols produce greater adaptations of these variables in post-menopausal women.
Regarding the BMD variables, there were no significant changes in any of the experimental groups after training. No differences were found between groups. Some studies have proved that WBV is useful in bone tissue, which may represent an effective method for preventing the loss of BMD. Ruan et al. 44 studied the effect of 6 months of WBV in 66 post-menopausal women (five sessions per week). After vibration therapy, there were significant increases in BMD at the lumbar spine (4.3%) and femoral neck (3.2%) when compared with baseline. In contrast, Russo et al. 45 showed no changes in bone characteristics following 6 months of WBV training in older women. These findings suggest that the training protocols should be more long lasting and that an analysis of BMD should be performed in specific areas to try to determine more precisely the effect of vibratory training on BMD.
However, Tanaka et al. 28 evaluated the effects of broad frequency vibration on cultured osteoblasts. The results suggested that osteoblasts are more sensitive to low-amplitude, broad-frequency strain, and this kind of strain could sensitize osteoblasts to high-amplitude, low-frequency strain. This suggestion implies a potential contribution of stochastic resonance to the mechanical sensitivity of osteoblasts and modulating mechanical adaptation responses in bone. Kaspar et al. 29 investigated whether bone formation by human osteoblasts in vitro is stimulated at low strain levels. Furthermore, they identified those bone cell activities that are dependent on mechanical strain and responsible for an increased bone formation in reaction to mechanical loading. The results demonstrated that cyclic strain at physiologic magnitude leads to an increase of osteoblast activities related to matrix production, whereas those activities that are characteristic for the differentiated osteoblast and relevant for matrix mineralization are decreased.
On the other hand, multi-component training appears to be a useful tool in the prevention of osteoporosis because such programs cause an anabolic effect on bone mass. In this sense, Vainionpaa et al. 46 reported that a 12-month exercise program with walking and jumping training was able to improve bone parameters in women. Nevertheless, another study carried out by Binder et al. 47 showed that combined flexibility–coordination–movement speed-strength training of 6 months duration was not enough to enhance bone mass. The broad differences of data found between studies may be because most of research used a time of exposure to exercise and weekly frequency was greater than in current study. The large methodological differences in relation to multi-component training, with no uniformity between programs, hinder a real comparison between studies.
With regard to lean mass, there were statistically significant changes between pre- and post-training in the two experimental groups. There were also significant differences between the vibratory and control groups after 12 weeks. In this connection, Roghani et al. 48 also obtained significant increases in lean mass after 6 weeks of multi-component training that included walking and resistance exercises. In exchange, Yoo et al., 49 who assessed the body composition of 112 students after 12 weeks of vibration exposure three times per week, obtained no significant increase in lean mass compared to the control group. Bosco et al. 50 found that exposure to vibration produces a sharp increase in blood levels of hormones such as testosterone and growth hormone. These endocrine changes would explain the increase in lean mass after vibration training. The practice of intense physical exercise long term causes changes in hormonal response, 51 but WBV will produce a similar result with less practice time. As we grow older, a loss of muscle mass associated with attenuation of these anabolic hormones (especially in older women) occurs. 52 The skeleton is a dynamic tissue associated with the muscular system. Therefore, an increase on muscle mass generates changes on bone mass. Along these lines, Calendo et al. 53 evaluated whether muscle activation and muscle strengthening caused by WBV has an effect on bone density. The study showed a positive correlation between muscle and bone mass. There was a significant increase on muscle activity that resulted in an improved bone density in the lumbar spine and the hip in post-menopausal women.
After 12 weeks of training, the experimental groups showed a significant decrease in total fat mass (WBVG = −2.2%; MTG = −0.7%), whereas it did not change (1.7%) in the CG. Furthermore, there were significant differences between WBVG and CG. Comparing our study with that by Milanese et al. (2012), similar results can be observed. Those authors assessed the body composition of 44 young women after 8 weeks of vibration training, obtaining a significant decrease in total body fat between pre- and post-test and without changes in body weight. 54 Nevertheless, other studies have not obtained favorable results for WBVT in decrease in fat mass, like Roelants et al., 32 who did not observe changes in body fat with a 24-week of vibration program, three times/week, in women. Despite the existence of conflicting results, in a more recent review about the effects of WBV training on weight loss, Cristi-Montero et al. 55 described as a possible explanation three pathways involved in weight loss—inhibition of adipogenesis and reduction of fat mass, increased energy expenditure, and an increase in muscle mass. An increase in muscle volume raises resting energy expenditure, which could help in reducing body weight and in fatty acid oxidation.
Another important finding was that the two training groups showed significant increases in isokinetic strength of the knee extensors muscles at 60° · s−1(WBVG = 7.9%; MTG = 8.8%) and 270° · s−1 (WBVG = 4.9%; MTG = 7.3%) after 12 weeks. In addition, the experimental groups showed significant improvement for eversion and inversion movements at 60° · s−1, and only WBVG for eversion at 120° · s−1 in ankle joint between pre- and post-test. However, there were no differences between groups. These results are in line with those published by other authors who support that WBV increases the dynamic strength of the muscles of the lower extremities.32,56–58 Machado et al. 57 studied the effect of 10 weeks of WBV on strength (measured by maximal voluntary isometric contraction [MVIC]) in older women (age = 65–90 years). The strength of the knee extensors and hip improved significantly when compared with baseline values. 57
Similar results were obtained by Roelants et al., 32 who proposed a training protocol of 24 weeks in post-menopausal women (n = 69) in which three groups were established, one exposed to vibration, another to resistance training, and a third to control. The vibration group performed high squat, deep squat, wide-stance squat, and lunge exercises. On the other hand, the resistance group combined 20 min of cardiovascular exercises and 40 min strength training for knee extensors. Mid-tests were performed after 12 weeks of training. The isometric strength (MVIC) and dynamic strength of knee extensors were measured. Women in the two experimental groups improved isometric and isokinetic strength, whereas power showed a greater gain in the WBV group. With respect to gain strength through multi-component training programs, Cadore et al. 59 studied the effect of combined training protocol of 12 weeks duration in nonagenarians (n = 24), two sessions per week. Each session encompassed resistance training with progressive loads, balance, and walking exercises. As in our research, the final evaluations showed beneficial results on the strength of the knee extensors. Similarly, in another study they found that a program of MT of 12 months, integrating weight-bearing exercises and aerobic activity, increased levels both maximal isometric force of the knee extensor muscles, and balance in older adults. 40
There are studies in the literature that evaluate the effects of long-term WBV training on reflex activity of the ankle stabilizer muscles. In recent research, a 6-week intervention, three sessions/week, in 44 healthy and physically active volunteers was performed. After training, there were no significant differences in reflex activity of muscles analyzed (peroneus longus, peroneus brevis, and anterior tibialis). 60 Similarly, Melnyk et al. 61 studied the effect of 4 weeks of vibration training on the stabilizing muscles of the ankle joint. Despite using amplitude and stimulus frequency parameters similar to those of the present study, they found no significant results after treatment. In our study, the participants performed a program including dynamic vibration action that renders plantar flexion of ankle, raising the heels on vibration platform to take the position of dorsiflexion again later, keeping in both cases periarticular ankle muscle contraction.
In the current study, improvements were found in the isokinetic strength of the muscles involved in the movements of ankle inversion and eversion. The instability that adopts the ankle to make a dynamic pattern on the vibratory platform could justify this strength gain. The literature shows that the vibratory stimulus generates greater adaptation training in the muscle group closer to the vibration platform. 62 Increases in the strength of the knee extensors were associated with increased joint mobility. 63 The improvement in the strength deficit of the inversion muscles can be of great importance as a system of long-term prevention of sprains, falls, and induced injuries by these in older people. 64
No study has been found relative to the isokinetic strength gains of the ankle inversion and eversion musculature through multi-component exercise programs. In our training protocol, participants combined the aerobic exercise of walking with drop jumps. During the landing, the ankle adopts a dorsiflexion position to cushion the impact. Thus, this could justify the improvement on the strength evertors and invertors of the ankle because their passive activation is necessary during the fall or imbalance occurs. 65 In this regard, Lin et al. 66 suggest the work of proprioception and strength of ankle stabilizers muscles by co-activation of agonist–antagonists such as preventive training with the aim of stabilizing the complex periarticular.
In summary, the present research shows that 12 weeks of WBV and MT significantly improve the strength of the knee and stabilizer muscles of the ankle joint. Furthermore, CG values remained constant throughout the study. The increased muscular strength of lower limbs decreases the likelihood of a fall, sprain, or fracture. 67 In this sense, these results are considered very important because falls are a major cause of morbidity and mortality in actual society, especially in post-menopausal women. In addition, adaptations occurred in body composition (decreased fat mass and increased muscle mass). Thus, obesity and sarcopenia risks, diseases that commonly occur in older adults, would be reduced. Even though one of the aims of this study was to determine which training protocol produces greater adaptations in body composition and strength, there were no significant differences between WBV and MT. The improvements were similar for both groups and the claim cannot be made that vibration is better than multi-component training. However, taking into account that training on a vibratory platform brings benefits with shortened session time and perceived exertion, this may be a good alternative to use in the elderly.
With the objective to find differences in the variables of strength and body composition between the training groups, more investigations are needed. The main limitations of the present study were: (1) High experimental drop-out over the 12-week study; (2) shortened duration of the treatment period that can explain why no results were obtained on BMD; (3) more specific measurement of BMD (lumbar spine and femoral neck); and (4) lack of assessments that have transferred to activities of daily life.
Footnotes
Acknowledgments
The authors thank the Universidad Católica de Murcia, located in Spain, for financing this research (grant no. pmafi/05/12). The authors also express gratitude to all the subjects who volunteered to participate in this study and made this project possible.
Author Disclosure Statement
No competing financial interests exist.