
Abstract
We examined associations between adverse childhood experiences (ACEs) and shorter telomere length (TL) in 83 older women, including 42 women with less than secondary education and 41 with secondary or more education in a city of Northeast Brazil, a region with substantial socioeconomic inequalities. The low education sample was selected from a representative survey at local neighborhood health centers, while the high education group consisted of a convenience sample recruited by advertising in community centers and centers affiliated with the local university. Relative leukocyte TL was measured by quantitative polymerase chain reaction from blood samples. ACEs were self-reported. Spline linear regression was fitted to assess the strength of the associations between ACEs and TL. Among women with low education, median TL was 1.02 compared with 0.64 in the high education group (p = 0.0001). Natural log-transformed T/S ratio as the dependent variable was used in analysis. Women with low education had been exposed to more ACEs, and among them those experiencing two or more ACEs had longer TL than women exposed to ≤1 ACEs (p = 0.03); among women with high education, this difference was not significant (p = 0.49). In analyses adjusted by age, education, and parental abuse of alcohol, the linear trend of higher TL with increasing ACEs was confirmed (p = 0.02), and the mean difference in TL between groups remained significant (p = 0.002). The unexpected positive relationship between low education and ACEs with TL suggests that older adults who have survived harsh conditions prevailing in Northeast Brazil have the longest TL of their birth cohort.
Introduction
L
About two-thirds of older adults in the world live in middle and low income countries, but most research on aging has been carried out in high income countries. 7,8 Population aging in middle income countries is fast. In particular, during the second part of the 20th century, Brazil went through a sharp sociodemographic transition in industrialization and important economic growth, and with a remarkable increase in life expectancy from 45.5 years in 1940 to 73.4 in 2010. 9 This increase in life expectancy is mostly due to improvements in Public Health interventions, such as childhood vaccination and technological advances in medicine. 10 Nonetheless, widespread poverty and undernutrition have coexisted with economic growth during this period: the Gini coefficient, normally used to measure economic inequalities, has a value of 0.53 in Brazil in 2013 11 demonstrating the unequal distribution of wealth. Within Brazil, the northeast region has the highest poverty rates 9 and the highest gender inequality. 12 In this context, where poverty and violence have been widespread, we would expect that chronic exposure to ACEs and low education completion would be associated with shorter telomeres in old age, in addition to the poor health and functional status as reviewed above.
In this research we will examine older Brazilian women because they have a consistent disadvantage in life expectancy, 13 health, and function. 14 Due to the intersection of class and gender inequalities, women with low socioeconomic status (SES) have the worst health compared with high SES women and men of their birth cohort. 15,16 It is expected that women who were exposed to ACEs and attained little education will be more likely to be pregnant in adolescence and to be exposed to domestic violence and poverty during adulthood. As a consequence, these women would be expected to be at higher risk of chronic conditions and poor physical function in old age. 17,18 Recent studies in Northeast Brazil provide evidence to support these hypotheses. Studies conducted in this region of Brazil have reported a high exposure of women to domestic violence during their lifecourse, 19 adolescent childbirth and multiparity, which were associated with chronic diseases and poor physical performance in older age. 20
Based on the above literature, we compared exposure to ACEs in older women with high and low education and we examined associations between ACEs and telomere length (TL) in both education groups of women from Northeast Brazil, a probably population of survivors. Our original hypotheses were as follows: (1) Women with low education would have shorter TL compared with women with high education; (2) Women with low education would be exposed to more ACEs than women with high education; and (3) Shorter TL in low education women would be explained by their higher exposure to ACEs.
Materials and Methods
The study protocol received ethics approval from the Ethics and Research Committee of the Onofre Lopes University Hospital (approval no. 623/11). All the participants gave their written informed consent.
Study population
A cross-sectional study was performed. The study population was composed of community-dwelling women aged 65 to 74 who were residents in the city of Natal, Rio Grande do Norte, Brazil. Two samples were drawn for this study, to represent low and higher education groups. The first one was a random sample of women recruited from women registered for medical care at five neighborhood primary care centers in Natal; this sample is part of the International Mobility in Aging Study (IMIAS) in Natal. 21 Selected neighborhoods were located in middle and low socioeconomic areas where most of the Natalense population resides. Participants were directly approached by our interviewers and invited to participate in the study, which took place between April and June 2014.
Almost all of the women in the IMIAS sample in Natal (92%) had less than secondary education. According to the 2010 census for that city, only 7.6% of women aged 60 years or more had completed high school. 9 As the IMIAS in Natal provided insufficient sample size to constitute the two education strata, a convenience sample of women with secondary or higher education was required to implement our study design and complete the comparison group of women who had completed high school education. For the high education group, potential participants were approached directly at senior citizen social groups and at the association of retired employees of the Universidade Federal do Rio Grande do Norte at Natal, between July and December 2014. A flow chart of the recruitment process of the IMIAS sample and the convenience sample can be found in Figure 1.
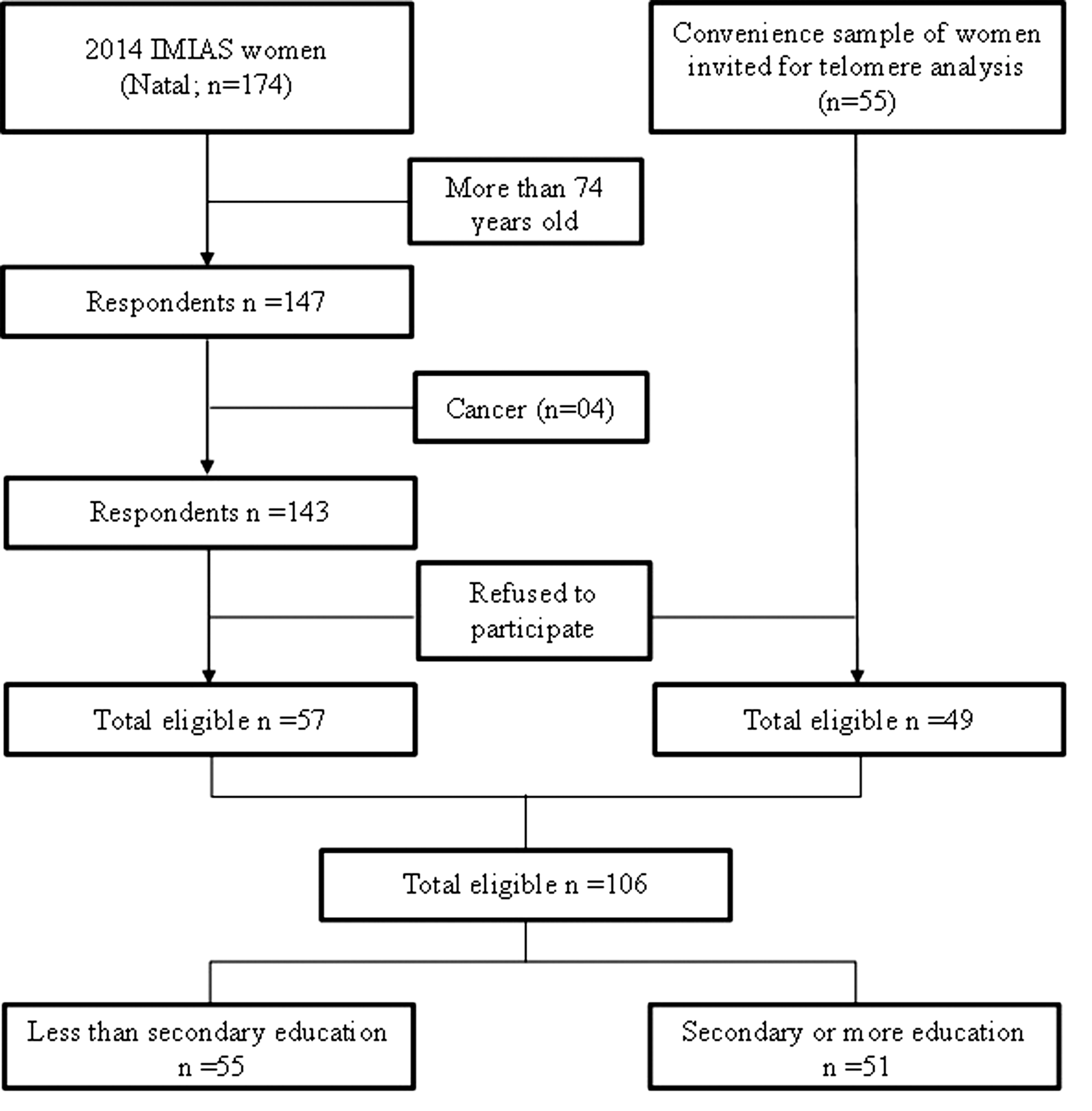
Flowchart of the study recruitment.
Eligibility criteria
Inclusion criteria included being aged between 65 and 74 years. Participants who had cancer (n = 4) were excluded. One hundred six (106) women met these criteria and were interviewed at home. In the analysis stage, 17 women were excluded because of insufficient DNA, and 6 additional women were excluded due to high coefficient variance or outlier values of TL measurements. This gave a final sample size of n = 83. There were no missing data on any of the variables in the final 83 women with valid TL assessments.
There were no statistically significant differences between the groups of included and excluded participants due to age (p = 0.27), years of education (p = 0.51), and number of childhood adversity experiences (p = 0.44).
Data collection
Interviewers were trained based on protocol instructions. Data were collected during two home visits. Each participant was visited by a single interviewer, who was responsible for all data collection from that participant. In the second visit, a laboratory professional was responsible for collecting venous blood.
Measurements
Education
Subjects completed a questionnaire detailing their educational level (years of schooling) and were categorized into two groups: less than secondary education (less than 11 years), and secondary or more (11 years or more).
Exposure to ACEs
We used a battery of eight questions on ACEs during the first 15 years of life. 5 These questions included the following: having witnessed physical family violence, experienced physical abuse by a close relative, hunger, poor economic status, prolonged parental unemployment, parental death, divorce of parents, and parental abuse of alcohol. The response was dichotomous (yes/no) and one “point” given for each category of self-reported adverse experience. As the effects of ACEs on health are known to be cumulative, 22 a categorical adversity variable was created by counting the frequency of experiences and the number of childhood adversities was classified as 0, 1, 2, 3, or 4+ exposures.
Parental abuse of alcohol was not included in the cumulative index of ACEs because abuse of alcohol at the time of conception or intrauterine exposure to alcohol is linked with DNA methylation programs. Though few studies have examined this relationship, there are associations between maternal alcohol consumption and cord blood methylation in the fetus that may cause epigenetic changes in specific locus of parental and newborn genomes, 23 and in vitro studies in fertilization show that the quality of sperm DNA is lower in men who abuse alcohol. Thus, as there are associations between DNA methylation and TL, 24 children born to parents who abused alcohol at the time of conception or mothers who abused alcohol during pregnancy may have shorter telomeres than children without these exposures. This direct effect of parental alcohol abuse on infant's TL would confound the possible social (neglect, physical abuse, and divorce) and economic (poverty, hunger, and prolonged parent's unemployment) consequences of parental abuse of alcohol during the first 15 years of life. Therefore, we included parental abuse of alcohol as a potential confounder in the statistical analyses.
Telomere length
Genomic DNA was extracted from peripheral blood leukocytes using QiAmp® DNA blood isolation kits (Qiagen) genomic DNA according to the manufacturer's instructions and stored frozen in aliquots until experimentation. TL was estimated in all samples by quantitative polymerase chain reaction (qPCR) 25 with modifications as described below.
DNA concentration of each sample was estimated by a UV spectrophotometric method and all samples were diluted in TE buffer to maintain a final concentration of 5 ng/μL. DNA quality was evaluated by UV spectrophotometry at 260/280 and 260/230 nm. Low DNA yield or poor quality DNA (based on nano drop thresholds) was excluded from the analysis.
The final telomere primer concentration was 900 nM, and the final β-globin primer concentration was 1000 nM. All qPCR were performed on the StepOne Real Time PCR machine (Applied Biosystems—Thermo Fisher Scientific, MA, USA) with 46 wells. The reaction constituted 5 μL SYBR Green PCR Master Mix, 3 μL DNA, and 1 μL of each primer. The equipment's thermal cycling conditions for telomere measurement were as follows: 1 cycle 95°C for 10 minutes followed by 26 cycles of 95°C for 15 seconds, 57°C for 30 seconds, and 60°C for 2 minutes. The β-globin qPCR conditions were 1 cycle of 95°C for 10 minutes followed by 40 cycles of 95°C for 15 seconds, 56°C for 45 seconds, and 60°C for 1 minute. Four serial dilutions of human DNA (10-fold) at an initial concentration of 50 ng/μL (50–0.05) (reference DNA) were included as a positive control and standard curve in each reaction batch for assay validation. Sterile deionized water was used as a negative control for each reaction batch. All samples were analyzed in duplicate and outlier samples were reanalyzed using a second fresh DNA aliquot.
The standard curves for qPCR assays had R 2 = 0.99 for both amplification targets (β-globin gene and telomere). The PCR efficiency ranges for β-globin amplifications were 82% to 88% and for telomere were 84% to 108%. The inter- and intra-experimental coefficient of variation was 1.67% and 2.7% for beta-globin gene, respectively. For telomere, inter- and intra-experimental coefficient of variation was 5.8% and 4.5%, respectively. No primer dimer formation or nonspecific amplification in the negative control was observed. Quantitative values were obtained from the cycle threshold value. The exponentiated T/S ratio for each sample was calculated, and was examined as a continuous variable.
Potential confounders
In addition to parental abuse of alcohol, we adjusted for age, which is a potent confounder since it is associated to both TL and education. Our final models did not adjust by health behaviors or chronic conditions because they are consequences of ACEs and education; however, we included this information for descriptive purposes of the study sample. Additionally, an exploratory follow-up analysis including these variables was performed to examine the robustness of our results. Height and weight were assessed. Body mass index (BMI) was calculated by dividing weight in kilograms by height in meters squared. Participants were asked if they had ever smoked (yes vs. no). 26 Chronic conditions, including high blood pressure, diabetes mellitus, chronic obstructive pulmonary disease or asthma, coronary heart disease, cerebrovascular accident, rheumatoid arthritis, and/or osteoporosis were self-reported as answers to the question: Has a doctor ever told you that you have…? A count of diagnosed chronic conditions was constructed for each woman with a maximum of seven for those conditions.
Statistical analysis
We used the Statistical Package for Social Sciences for data analysis considering a p-value of <0.05. The Kolmogorov–Smirnov test was used to check data normality. Since T/S ratio measures were highly skewed, the log transformed values (ln T/S ratio) were used to compare means across levels of education and ACEs.
To test our first hypothesis that women with low education have shorter TL compared with women with high education, we used a t-test in bivariate analyses and multiple linear regression to control for age and parental alcohol consumption. To test our second hypothesis that women with low education would be exposed to more ACEs than women with high education, we used Chi-squared tests of associations between each ACE and education level. Lastly, to test our third hypothesis, independent-sample t-tests were used to compare means of ln T/S ratio by the presence or absence of each childhood adverse experience and comparisons of means of ln T/S by number of childhood adversities was carried out by one-way ANOVA. To test whether shorter TL in low education women would be explained by their higher exposure to ACEs, we used spline multiple linear regression using a spline function for ACEs. Although the rationale of analyses between adversities and TL was based on previous studies demonstrating a linear relationship, 6 in our study we conducted exploratory analyses testing for a linear and quadratic trend in the association between adversity and TL in each level of education. Lastly, a fitted spline regression analysis was performed because the effect of ACEs on TL was nonlinear and could be better characterized by spline regression. Age and parental abuse of alcohol were adjusted for in the final multiple linear regression.
Results
The analytical sample included 83 women born between 1940 and 1950. The average ln T/S ratio in the low education group was 2.79 ± 0.9 compared with 2.03 ± 0.9 in the high education group (p = 0.001) (Table 1).
IQR, interquartile range; SD, standard deviation.
Women in the low education group were significantly older, had lower income, and more often reported that their income was insufficient to cover their basic needs (p = 0.001).
Women with less than secondary education were more likely to have ACEs (Table 2). Having experienced hunger and prolonged parental unemployment in childhood was significantly more frequent in the low education group than in the high education group.
ACEs: witnessing physical family violence, physically abused, death of parents, divorce of parents, hunger, poor economic status, and prolonged parental unemployment.
ACE, adverse childhood experience.
Parental alcohol abuse was reported by 21.4% of women in the low education group, whereas only five (12.2%) women with secondary or more education reported having experienced parental abuse of alcohol (p = 0.26).
Mean scores of ln T/S ratio on the adversity indicators are shown in Table 3 separately by education. The mean TL across number of childhood adversities (0, 1, 2, 3, 4, or more) by education group is illustrated in Figure 2. Unexpectedly, increasing TL was observed with increasing number of ACEs among women with less than secondary education. Among women with higher education, the same phenomenon is observed, but the minimum TL was observed for women with two adverse experiences, and mean TL increased for those with three or four adverse events.
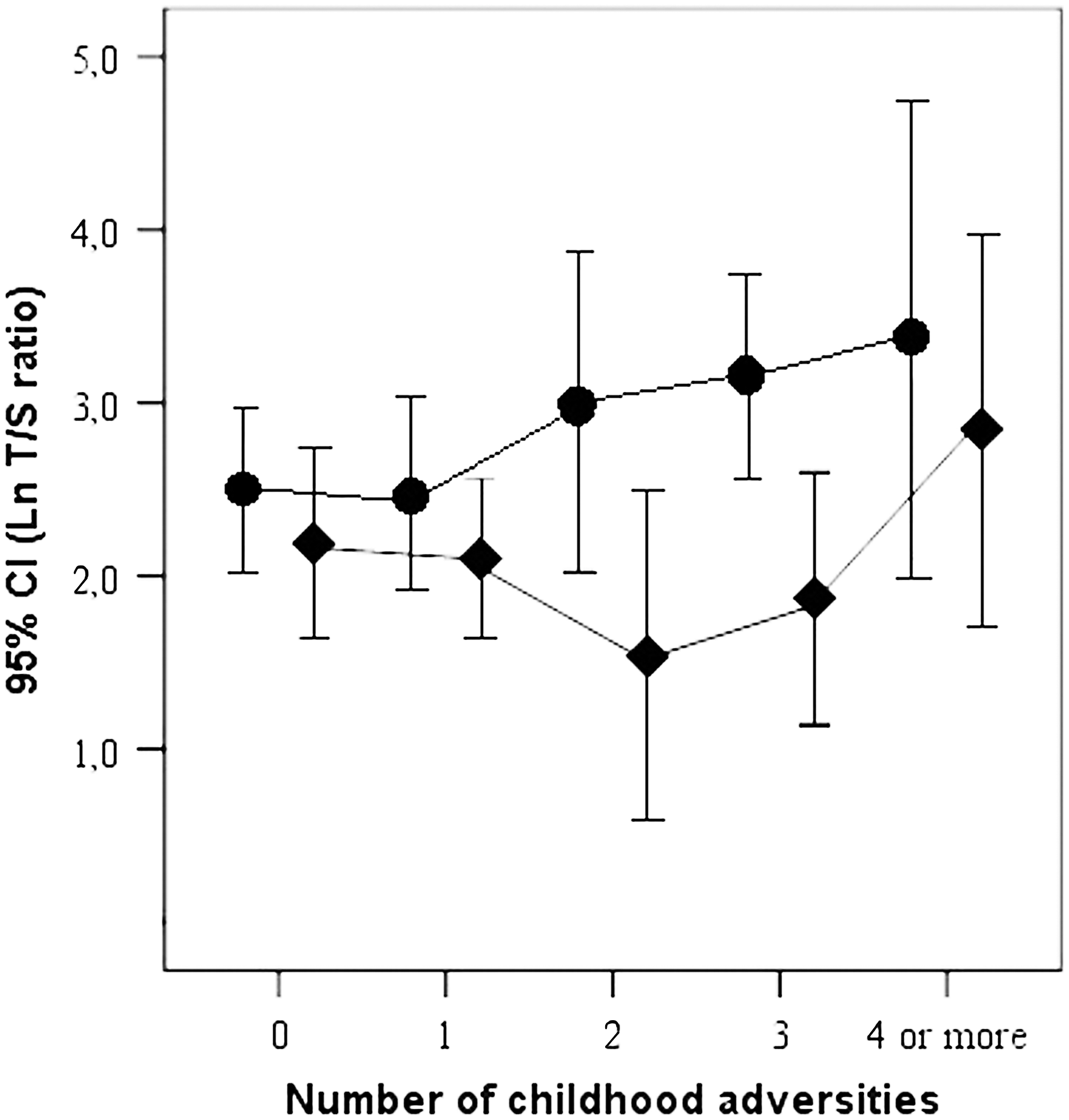
Mean ln T/S ratio for adverse childhood experiences (0, 1, 2, 3, 4 or more) by education group. Circles, low education group; Diamonds, high education group. CI, confidential interval.
ACEs: witnessing physical family violence, physically abused, death of parents, divorce of parents, hunger, and early economic situation.
We first conducted exploratory analyses of variance for each education group adjusting quadratic terms. A significant linear trend was detected (p = 0.03) in the low education group, but in the high education group, neither the linear or quadratic terms reached significance (results available upon request). Next, a spline regression was fitted with a knot at one adversity for the low education group and a knot at two adversities for the high education group using pooled data. Including age did not change results. Remarkably, age was positively and significantly associated with TL in bivariate analyses, but the significance of this association disappeared after controlling for education.
Two spline regression models are shown in Table 4. Model I included the intercept, the slope of ACEs for less than two adversities, the slope of ACEs for more than two adversities, and parental alcohol abuse. We added education in model II. The difference between the low and high education groups remained significant (p = 0.002) and the linear trend of higher TL with increasing childhood adversity was confirmed (p = 0.02). Parental alcohol abuse was significantly associated with shorter telomeres independent of ACEs and education. Exploratory analysis including chronic disease (0–1 or 2+) or self-reported health (very good/good or fair/poor/very poor) did not change the results (data not shown).
ACEs: witnessing physical family violence, physically abused, death of parents, divorce of parents, hunger, and early economic situation; Intercept: the intercept for two ACEs.
SE, standard error.
Discussion
This study examined whether ACEs were associated with TL comparing women with different educational levels. We found that women with lower education had longer TL on average; women with lower education experienced higher childhood adversity than women with higher education but for each level of ACEs, women with lower education had longer TL. In addition, TL was longest among those with the highest number of ACEs for both educational groups.
Before discussing these unexpected results, which contradict our hypotheses, some historical information on the state of Rio Grande do Norte (RGN) in Northeast Brazil (where this study was conducted) is needed. In 1940/1950, overall life expectancy was 45.9 years in Brazil, 49.9 years in the state of Sao Paulo, 33.9 years in RGN, 27 and infant mortality was 145/1000 with large geographical variations, being 128/1000 in Sao Paulo and 199/1000 in RGN. Social conditions vary in the same direction. In 1950, the proportion of women with high school education was 4.6/1000 in Sao Paulo and 2/1000 in RGN. 28 Given the lack of national statistics on life expectancy by education in Brazil, and for the sake of this argument, we consider that the life expectancy of Sao Paulo birth cohorts could be indicative of the life expectancy of those with higher education in Natal. These figures show that life expectancy in Brazil has increased steeply in recent decades. Life tables by sex are available at the IBGE website since 1980. In 1980, it can be seen that the life expectancy of women in RGN was 61.0 years and the probability of reaching age 65–69 for women born in 1980 was 63%, and of reaching age 70–74 was 56%, indicating that even in 1980 mortality was high at all ages. Thus, we conclude that we were analyzing two samples of survivors who reached 65–74 and they come from birth cohorts that were expected to live up to 34 or 50 years, according to their education.
In this cohort of survivors, although women with higher education were less exposed to ACEs, they had on average shorter TL than women with lower education. The impact of education on TL can be observed at every level of ACEs, suggesting that the survival advantage associated with TL is manifesting among those with both multiple ACEs and among those with low education during the lifecourse.
In this study, mean TL had a positive linear relationship with number of ACEs; the positive trend was significant for one or more adverse experiences in the low education group and for two or more adverse events in the high education group. This linear relationship maintained statistical significance adjusting for age, education, and parental abuse of alcohol. There is no previous research that simultaneously considers ACEs and education effects on TL that allows us to compare our results. We propose that the women with the lowest education and highest ACEs had greater TL because longer telomeres could be markers for survival (greater potential for life). This survival potential has allowed them to overcome life challenges that they would have not been able to overcome had they not had long telomeres at birth or a mechanism to maintain long telomeres. Selection of those with long telomeres at birth and mechanisms to maintain long telomeres have been proposed as “selection hypothesis” and “elongation hypothesis,” and have been tested as competing hypotheses in animal models of hatchlings and adult storm petrels with the evidence favoring the selection hypothesis. 29
One possible explanation to the associations observed in our study, is that TL might act as a sorting machine enhancing survival among those who, had they had short telomeres would not have survived their first years of life; or, if they had survived childhood, they would not have reached their 65th birthday. At the extreme end of this reasoning, reaching their 65 birthday or being part of the “club of survivors” happens under two conditions: either having long telomeres at birth or having experienced little adversity during childhood and during their lifetime. These two criteria required to reach old age would explain why we observe women over the age of 65 with little ACEs and high education to have shorter telomeres.
Recent findings by the IMIAS on five international older populations provide evidence to support this survival hypothesis. 20,30 The effect of early maternal age at first birth on physical function was stronger in the Canadian and Albanian sites than the Latin American sites, 20 suggesting a higher mortality in women with an adolescent pregnancy in Latin America. Authors reported that ACEs in older participants from Brazil and Colombia were not significantly associated with high inflammation, while significant associations were found in Canadian participants. 30 Furthermore, those Latin American participants who were exposed to childhood social adversity tended to have lower levels of inflammation than those without this early exposure. 30 Survival bias in studies of population aging has been well described by Willson et al. 31 and better survival of the more educated has been observed in the Natal IMIAS sample, where 31 deaths occurred during the 2012 and 2106 four years follow-up with a retention of 91%; all deaths occurred in the low education group (n = 333) for whom mortality reached 9.3% and no deaths were observed among those with high education (n = 33) (Fisher p-value = 0.047).
Authors reported that the distribution of TL has less variability in older populations than in younger populations, 32 suggesting that individuals with long telomeres survive longer or keep the mean average length of their telomeres. In concordance, it is argued that older individuals have superior characteristics of genetic stability reflected by longer and/or more stable telomeres, 33 and evidence suggests that survival bias could lead to discrepant results in older survivors with relatively longer telomeres than expected for the general population. 34 –36
Due to social and gender inequalities, women had little access to education before 1980 in Brazil. 37 Thus, an alternative hypothesis that could explain the results would be that those women with higher education in our study sample broke away from social norms and as a result they were exposed to more social stress, cultural and gender discrimination, and consequently their rate of TL shortening would be more rapid. However, the lower exposure to hunger and parental unemployment in our group of high education women indicates that these women had early origins in more affluent families than the low education women and as a consequence, they should have a more advantageous life on average.
Women with parental abuse of alcohol had shorter TL on average, and this effect was strong and independent of ACEs and education. Parental consumption of alcohol could be an important confounder in the association of ACEs and TL, since parental alcohol abuse is strongly associated with ACEs and exposure to alcohol abuse may have occurred at the time of conception or during uterine life with potential effects on TL.
Our results have implication for international studies of aging populations since they suggest that survival bias may seriously affect the magnitude of associations between risk factors for health and health and functional status across populations with different life expectancy. Strong associations observed in high income countries may not be detected in low and middle income countries due to survival of the fittest under harsh living conditions in early life and adulthood.
The modest sample size limits the power to examine the associations of TL with ACEs by type of adverse event or to examine the possible mediating pathways between low education and adversity, and TL through smoking, physical activity, or chronic conditions. However, associations between these health behaviors and chronic conditions with TL have been shown to be weak or nonsignificant. 38,39 Inclusion of chronic sources of stress during adult life, such as violence and poverty, would allow for more in-depth lifecourse analyses. If our proposed survival hypothesis were true, these sources of chronic stress would further increase mortality in the study population, sorting out those with longer TL. Birth cohort studies are needed to examine these hypotheses. Concerning race, the population of Natal is very mixed. Official 2010 census figures, based on self-reported skin color, for Natal women were as follows: 43.2% white, 50.7% brown (pardo), 4.8% black, and 1.3% other (yellow or indigenous). Although health inequalities in Brazilian society are mostly based on poverty and lack of education, 40 future studies should examine the effect of race with ACEs and TL because studies reported mixed associations for the interaction of racial/ethnic category with education in the prediction of TL. 41,42
Although our study was limited by using the relative qPCR method, this method has been used in valid clinical and epidemiological studies. 22,43 –46 Additionally, studies comparing TL derived from the gold standard method (Southern blots) versus those derived from the qPCR method show significant correlations. 25,47,48
Conclusion
The unexpected results linking ACEs and low education with the longest telomeres in this highly selected sample of older women who are survivors of their birth cohorts may be due to their higher longevity marked by their longer telomeres. Questions on TL maintenance or stability need to be examined in longitudinal designs that would allow for examining the rates of change in TL and the intra-individual and inter-individual associated factors.
Footnotes
Acknowledgment
This work was supported by funding from the National Council for Scientific and Technological Development (480322/2012-0).
Author Disclosure Statement
No competing financial interests exist.