
Abstract
Fractional bipolar radiofrequency (FRF) has been well established for facial rejuvenation, but there is no report showing its efficacy for the treatment of suborbital wrinkles. The aim of this study was to investigate and objectively evaluate the clinical efficacy and side effects of FRF for the treatment of suborbital wrinkles, including observation of histological changes of the suborbital skin along the therapy. Thirty-two female patients with suborbital wrinkles underwent three sessions of FRF at 3-week intervals with a follow-up period of 6 months after treatment. Two independent dermatologists with standardized photographs evaluated improvement grade. Most patients improved according to photographic assessments and the differences between results at 1 and 6 months were not statistically significant (p > 0.05). The median score of pain rated by patients using a visual analog scale (0–10 points) was 4.4 ± 1.2. Most patients rated themselves as satisfied (68.8%) and very satisfied (9.4%). Ten subjects (31.3%) experienced hyperpigmentation in 24 of all together 96 treatments (25.0%). Skin biopsies of three patients were routinely obtained, processed, and stained, and the histological changes had shown that 1-month after the end of the treatment, both the collagen and normal elastic fibers increased in accordance with the clinical efficacy. The study suggested that FRF is a safe and effective method to treat suborbital wrinkles.
Introduction
S
Current therapies for sub- and periorbital wrinkles require intensive research and improvement. Due to specific anatomic structures, fragility, and sensitivity of the area, the vulnerability for adverse events during surgery, injections, or ablative laser therapy is much higher. 10 –12 Surgical approaches, such as lower blepharoplasty, are quite effective, but associated with a greater number of side effects, such as long recovery, ectropion, or scarring. 10 Botox injection for suborbital wrinkles lead to a limited improvement because it has little effect on static wrinkles, and very precise injection skills of the operator are required. 11,12 Local syringe-based fillers, such as hyaluronic acid, calcium hydroxyapatite, or collagen, restore the volume loss of the periocular region, but have a very limited effect on fine lines and skin texture. Moreover, skin fillers might cause early and late adverse effects, which range from bruising to necrosis. 12,13
In recent years, patients turned to photoelectric therapy, which offers fewer traumas, minimal risk, and rapid recovery. 14,15 Fractional resurfacing thermally ablates microscopic columns of epidermal and dermal tissue, accompanied by residual heating. The following new collagen formation leads to skin tightening. 16,17
The fractional model of bipolar radiofrequency (RF) is a rapidly developing technology, with a reported efficacy in rejuvenation and treatment of acne scars in Europe and the United States of America. 18 –21 Asian studies are still limited, especially for treatment of suborbital wrinkles. In our prospective study, we evaluated the efficacy and safety of fractional bipolar radiofrequency (FRF) in the treatment of suborbital wrinkles, reporting both subjective and objective clinical effect, finally also objectivizing the visible effects with histological changes of the suborbital skin.
Materials and Methods
Subject selection
Thirty-two healthy females were enrolled in the study (n = 32, aged 30–60, 45 ± 0.43 years, skin types III–V). All female subjects were postmenopausal or used an acceptable form of birth control for at least 3 months before the study commenced. The exclusion criteria included immunosuppression, sun exposure within 3 weeks before the enrollment, infections with herpes simplex virus or bacteria, a history of hypertrophic scarring or keloid formation, pigment metabolism disorders, endocrine disorders, adrenal cortex dysfunction, use of drug causing photosensitivity 6 months before enrollment, injections of fillers or botulinum toxin in the treatment area up to 1 year until the enrollment, pregnancy, and breastfeeding. All subjects provided signed informed consents. Photography was standardized for all patients.
Treatment device and study design
We used eMatrix™ (Syneron & Candela, Irvine, CA), which delivers fractionated bipolar RF and contains a disposable single-use treatment tip, consisting of rows of 44 gold-coated electrode pins in a 3 × 11 mm area. A total of 200 pulses are available on each of the single-use tips. Pins are arranged in alternating rows of positive and negative electrode pins. These electrode pins form a closed circuit through the irradiated skin, delivering 1 MHz of conducted RF current to the skin. In this prospective study, subjects received three treatments in the suborbital wrinkles area every 3 weeks. Target areas were first washed with mild soap and water. One hour before FRF treatment, 1% Lidocaine cream was placed in the areas as topical anesthesia, and eye protection was installed. The skin was then cleaned, sterilized, and treated with FRF. Treatment was delivered in a single nonoverlapping pass over the treatment area at 30–60 mJ/pin. Postinterventionally, patients were advised to avoid water contact with the face for 5 days, to pay attention to moisture and to avoid sun exposure for 6 months.
Evaluation of efficacy and adverse reactions
Efficacy and adverse effects were assessed by two independent, double-blinded dermatologists at 1- and 6-month follow-up visits. Patients were photographed with a standard camera and settings (Nikon D90, Tokyo, Japan) to record the clinical effect. To assure the objective character of the assessment, we used five evaluation criteria for a final wrinkle improvement rate: grade 1 (no improvement or worsening), grade 2 (1%–25% improvement), grade 3 (26%–50% improvement), grade 4 (51%–75% improvement), and grade 5 (76%–100% improvement). Patient satisfaction was rated as follows: 0 (not satisfied), 1 (relatively satisfied), 2 (satisfied), and 3 (very satisfied). Pain assessment was conducted on the visual analogue scale (VAS) 0–10 (0 no pain, 10 unbearable pain). Side effects were documented at each control: every patient was asked to report edema, crusting, duration of postinflammatory erythema, and incidence of hyperpigmentation and scars.
Statistical methods
Statistical analyses were performed using SPSS 19.0. Data are expressed as mean ± standard deviation, with paired t-test to compare the degree of improvement between 1-month follow-up and 6-month follow-up. p-Value <0.05 was considered statistically significant.
Histological examination
To obtain a fully objective picture on the in vivo processes in the area of suborbital wrinkles along the FRF treatment, three volunteers agreed to provide histological samples. One side (left or right, chosen randomly) of the lower eyelid was selected as an “experimental group,” the respective other side as a “blank control group.” The three volunteers were treated with FRF on one (randomly assigned) side of the lower eyelid skin, and the other side was a blank control (no treatment). Biopsy time points and parts were as follows: a. Immediately after the first treatment, a round skin tissue with a diameter of 3 mm was taken near the midline of the pupil, at the treated side of the lower eyelid skin. b. One month after the end of three treatments, a round skin tissue with a diameter of 3 mm was taken near the midline of the pupil, at the blank side of the lower eyelid skin. c. One month after the end of three treatments, a round skin tissue with a diameter of 3 mm was taken at 3 mm from the biopsy side described in point a.
Hematoxylin–eosin (HE) staining allowed to analyze the range of heat gasification and the thermal coagulation zones in a. Masson trichrome was used to observe changes in the active region of dermal collagen fibers, and Van Gieson staining was used to observe changes in elastic fibers in b and c. However, all of the staining could not give quantitative objective evaluation.
Results
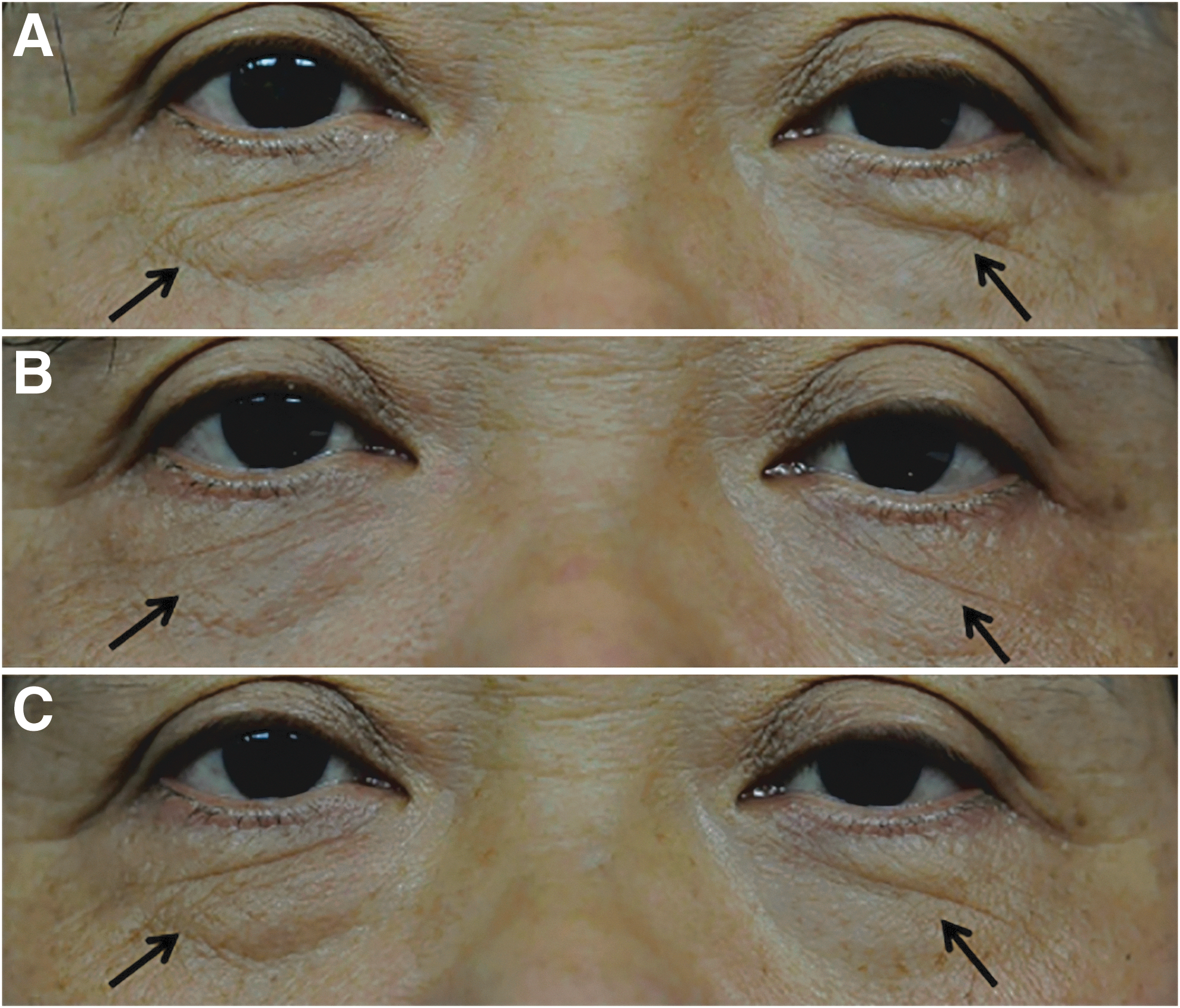
Thirty-two patients (skin type III–IV) were included in this prospective trial. All patients were subjected to a standardized photography. Results from two representative patients are presented in Figures 1A–C and 2A–C.

Physicians' assessment
At 1 month, we observed improvement grade 5 in 5 cases (15.6%), grade 4 in 7 cases (21.9%), grade 3 in 10 cases (31.3%), grade 2 in 6 cases (18.8%), and grade 1 in 4 patients (12.5%). The average grade of improvement was 3.1 ± 1.3. At 6 months, we documented improvement grade 5 in 3 patients (9.4%), grade 4 in 9 cases (28.1%), grade 3 in 6 patients (18.8%), grade 2 in 10 cases (31.3%), and grade 1 in 4 patients (12.5%), with an average of 2.9 ± 1.2 (Fig. 3). Independent assessment of the physicians was evaluated using GraphPad Prism software. In paired t test, p > 0.05, no statistical significance was seen.
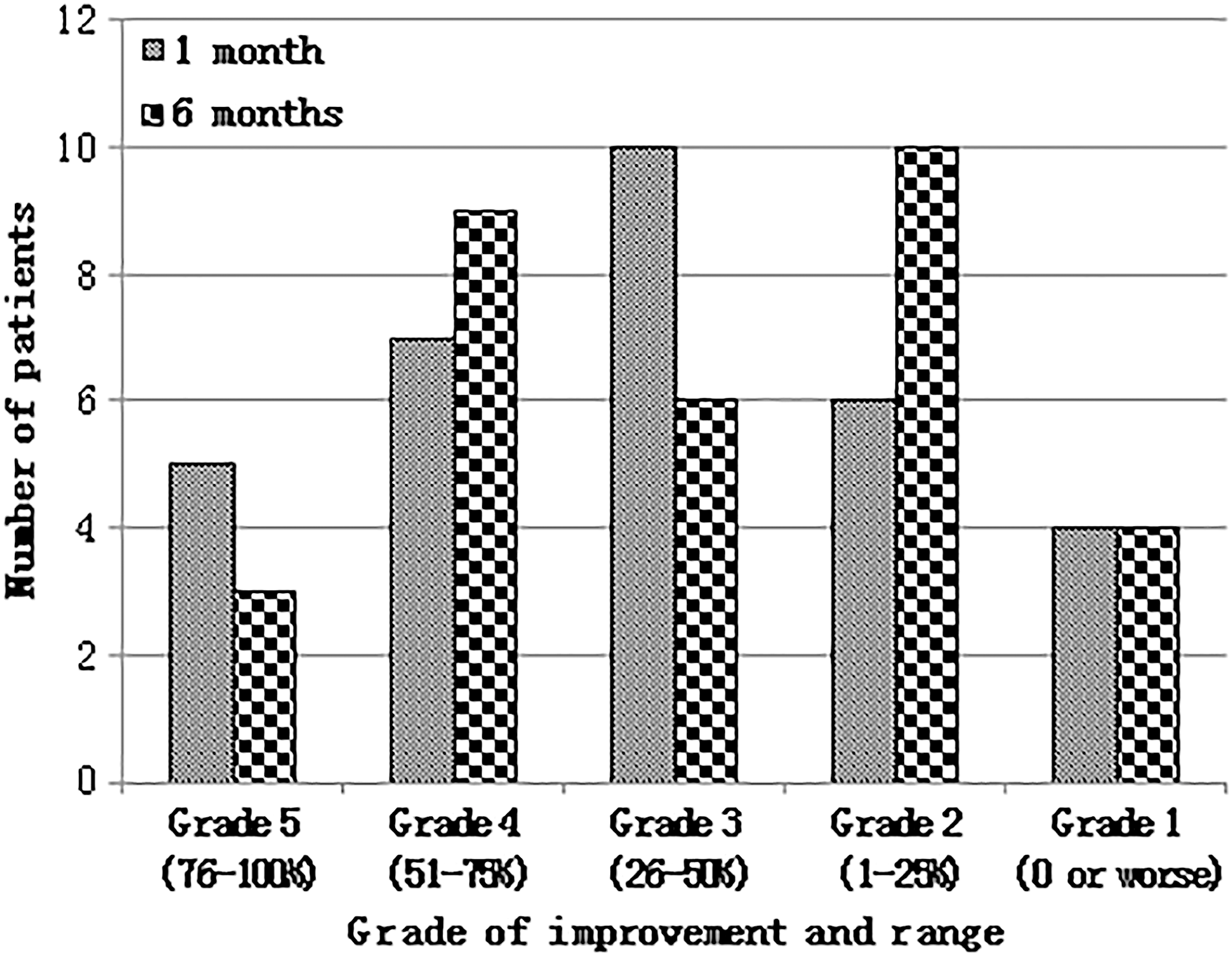
Results of the improvement per two blinded, standardized physicians' assessment.
Patients' satisfaction per self-assessment
Patients' subjective satisfaction was reported regularly with a standardized grading. Overall, 2 cases (6.2%) were not satisfied, 5 cases (15.6%) relatively satisfied, 22 cases (68.8%) satisfied, and 3 cases (9.4%) very satisfied.
Adverse reactions and pain
Pain assessed by the patients at the VAS was continuously documented. The median VAS pain score was 4.4 ± 1.2. Median edema duration was 2.9 ± 0.5 days. Median scab persistence was 5.9 ± 1.0 days. Postinflammatory erythema duration was 3.4 ± 1.1 days. In a total of 96 treatments, pigmentation was reported 24 times (25.0%) and disappeared within 3 months. All cases had no scars (Table 1).
Duration, days.
No. of occurrences/total treatment session (%).
Visual analog scales.
Histological examination
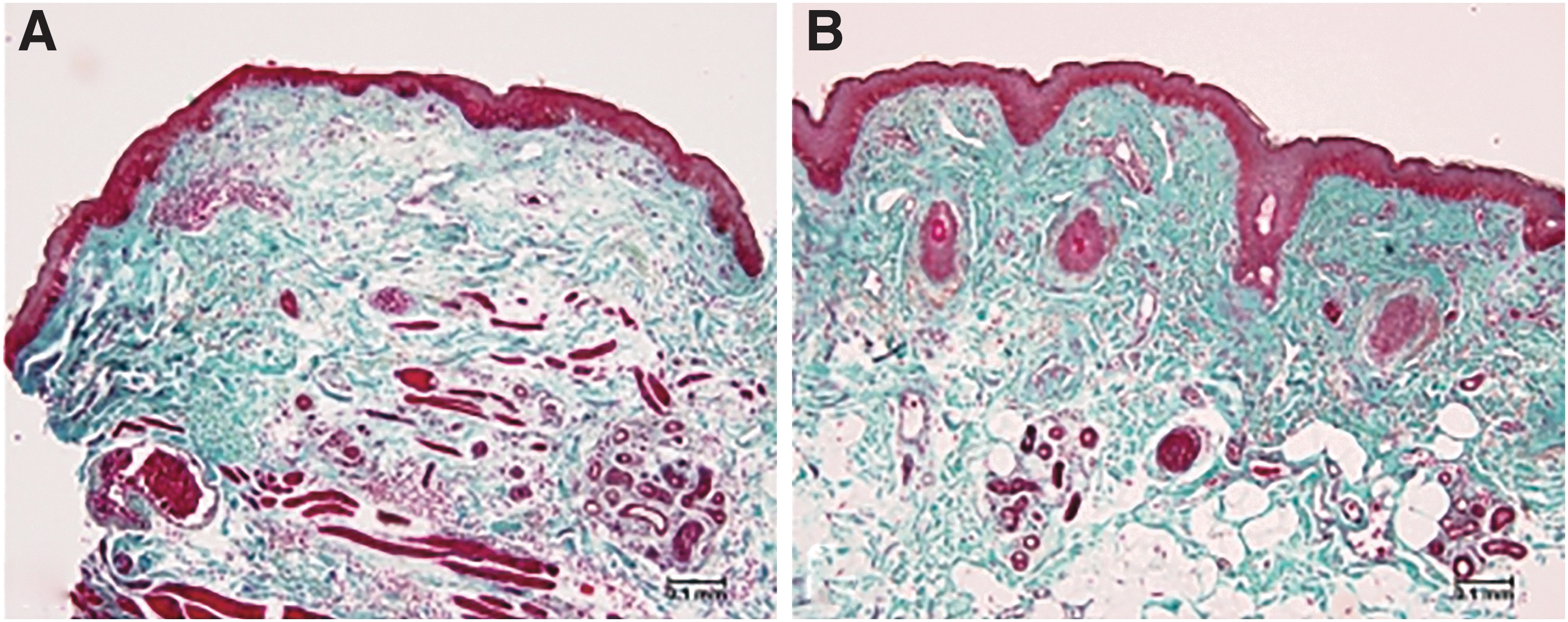
Tissues treated with FRF treatment were subjected to a series of staining. In the HE staining (Fig. 4), the treated areas showed large microexfoliation with shallow depth immediately after the first treatment. One month after the end of three treatments, Masson trichrome staining of tissues (Fig. 5) showed denser collagen fiber areas in FRF treatment areas than in the (untreated) controls, Van Gieson staining (Fig. 6) showed many abnormal elastic fibers in nontreated skin because of solar elastosis, and abnormal elastic fibers decreased after treatment with appearance of some newly formed normal elastic fibers in treated group.
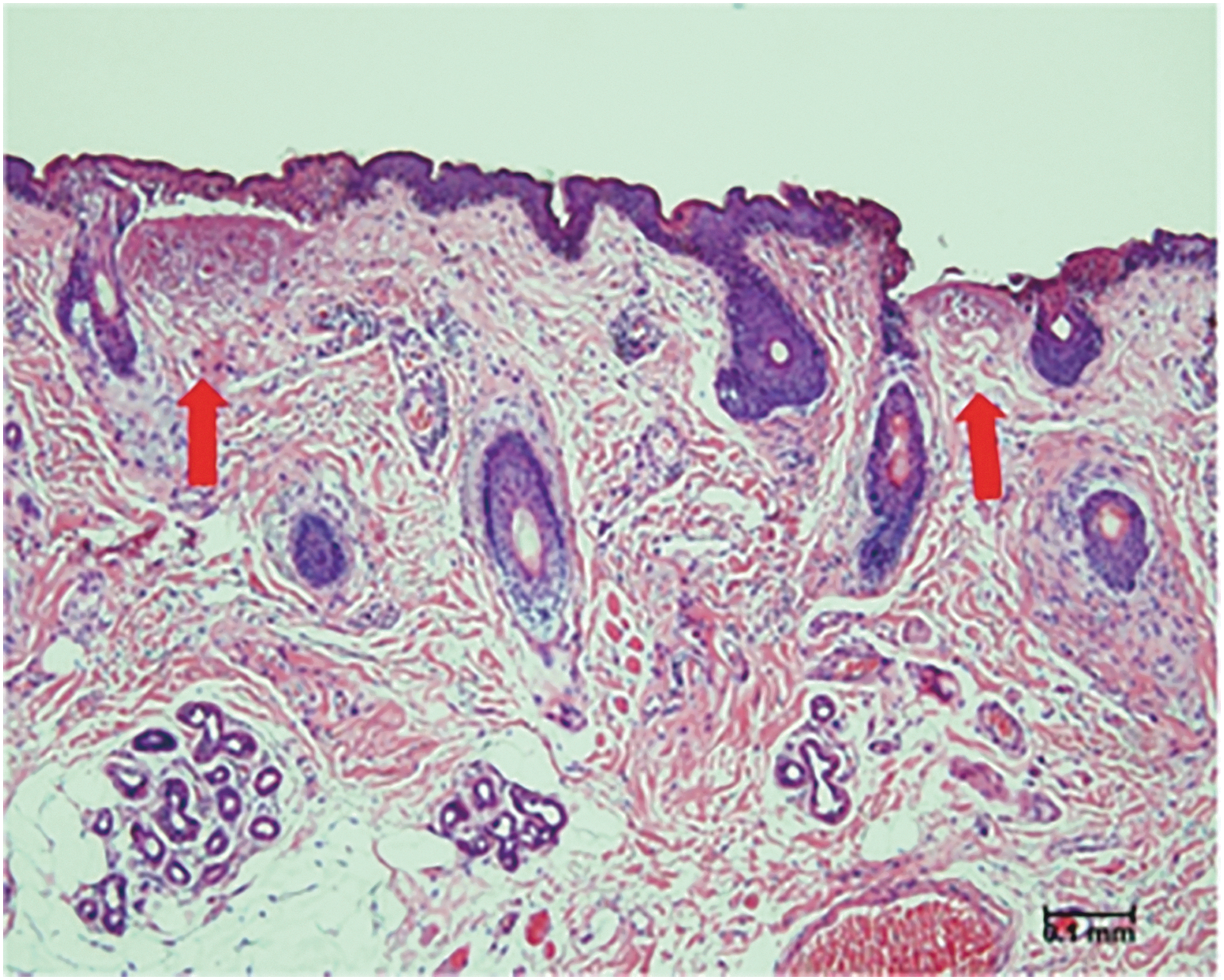
HE staining immediately after the first treatment. The gasification zone is wide and shallow, diameter 120–250 μm, depth range 80–100 μm. The thermal coagulation necrosis around the area ranges from 40 to 55 μm. HE, hematoxylin–eosin.
Masson trichrome staining.

Van Gieson staining.
Discussion
Skin rejuvenation has been well developed over the past two decades, from ablative methods to nonablative, as well as recently fractional ablative, methods. 22 The ablative methods, such as CO2 and Er:YAG lasers, have been described as effective for facial wrinkle treatment, including periorbital areas, but these methods sometimes are difficult for patients to accept their significant time-out related to prolonged erythema, swelling, and even dyspigmentation. 23,24 The advantages of nonablative interventions are obvious (less scaring, less pain, less adverse events, better patients' compliance, etc.), but multiple sessions are required to achieve the desired effect. 16,25,26
Fractional photothermolysis (FP) was introduced and revolutionized laser resurfacing recently. It applies an array of microscopic treatment zones of thermal damage and it spares tissue surrounding each wound serving as a reservoir of cells to heal rapidly. The area of contact with the skin was being exfoliated with electrodes in the form of a dot-like array. With help of adjustable energy control, thermal damage reached up to the reticular dermis, but spots between the damaged areas still retained a large number of intact areas for collagen and elastic fibers to remodel. The technique is so-called “sublative rejuvenation” for it has a deep dermal effect but relatively low-impact epidermal effect, so it overcomes the deficiencies of both ablative and nonablative treatments. 22,27 –29
RF is an electromagnetic wave. Passing through the skin, RF passes through resistances to radio waves, causing instant fast oscillations of water molecules and leading to production of heat in the target tissue. Heat effect acts therapeutically in facial rejuvenation. With the concept of FP, a novel FRF system has been recently developed for wrinkle treatment. 30 –32
We present in this study for the first time, as to our knowledge, objective efficacy of suborbital wrinkles treated with FRF, including histological correlates along with the subjective evaluations of both patients and blinded physicians.
In our study, we observed a significant clinical improvement at 1 month and at 6 months after the treatment (Figs. 1 and 2). The median grade of improvement at 1 month was 3.09 ± 1.25 and 2.90 ± 1.22 at 6 months. In paired t test, p > 0.05, the improvement at 6 months was only slightly lower than at 1 month (no statistical significance), indicating that suborbital wrinkle treatment with the FRF is effective and the visible improvements durable. As to patients' satisfaction, most patients rated themselves as satisfied (68.8%) and very satisfied (9.4%). This is mainly due to the treatment effect and the mild side effects, limited only to short-lasting erythema, crusting, edema, and pigmentation. The pain was assessed as low and fully tolerable; no subjects dropped out of the study.
In our histological analysis we could confirm that immediately after the FRF treatment, the FRF treated region is wide and shallow, with a diameter of 120–250 μm, depth range 80–100 μm, and is surrounded by a zone of thermal denaturation and coagulation (40–55 μm) (Fig. 4). In Masson trichrome (Fig. 5) and Van Gieson staining (Fig. 6), we saw in FRF treated areas a significant increase of collagen fibers' number and compaction, resulting in a denser and thicker epidermis. These findings are consistent with the visual improvement of the wrinkles and thus the clinical efficacy. 33
Our clinical and histological results have proven FRF to be a safe and effective method for treatment of suborbital wrinkles. However, the fine setting of the energy and density parameters to achieve the best results with minimal side effects needs further studies. At the moment, the choice of parameters shall differ for each individual and be personalized.
Conclusion
This study demonstrated that the use of FRF for suborbital wrinkle treatment is efficient, with a minimal occurrence of side effects and a short time needed to achieve visible long-lasting results. To our knowledge, it is the first study investigating FRF role in vivo on the suborbital skin, including histological findings. Our data imply that FRF is safe and tolerable, with a high satisfaction rate of the patients.
Footnotes
Acknowledgments
The authors are thankful to the staff and faculty of the Department of Dermatology and the Laser and Cosmetic Medicine, Ninth People's Hospital, School of Medicine, Shanghai Jiao Tong University.
Author Disclosure Statement
No competing financial interests exist.