
Abstract
Coenzyme Q10 (CoQ10) is a well-known antioxidant molecule which is used in the treatment of neurodegenerative disorders, but due to poor solubility it suffers with the drawback of low oral bioavailability. The aim of present study was to prepare and characterize CoQ10 loaded nanoemulsion to improve the oral bioavailability. Prepared formulation was studied for droplet size, polydispersity index (PDI), percentage transmittance, refractive index, viscosity, zeta potential, surface morphology by transmission electron microscopy, and in vitro release study. Optimized formulation (A10) showed spherical droplets with mean diameter of 60.00 ± 15 nm, PDI of 0.121 ± 0.053, and zeta potential values of −24.40 ± 0.16 mV. Prepared nanoemulsion exhibited good transmittance (100.50% ± 0.86%), refractive index (1.41 ± 0.02), and viscosity (30.54 ± 2.86 cP). Various behavioral tests like forced swimming test, locomotor activity test, catalepsy, muscle coordination test, and akinesia test performed in haloperidol challenged rats and treated with CoQ10 nanoemulsion significantly improved the behavioral activities in comparison to CoQ10 suspension by reducing nigrostriatal dopamine depletion and thereby helping in the treatment of Parkinson's disease. Biochemical estimation data showed that CoQ10 nanoemulsion was helpful in elevating the decreased content of glutathione and reducing the increased content of thiobarbituric acid reactive substances. Improved CoQ10 release was obtained with nanoemulsions. Pharmacokinetic study results revealed that nanoemulsion exhibited 1.81 times enhancement in bioavailability in comparison to CoQ10 suspension.
Introduction
P
Coenzyme Q10 (CoQ10; chemically 2,3-dimethoxy-5-methyl-6-decaprenyl benzoquinone) is a lipophilic, endogenous essential molecule of respiratory chain, found in eukaryotic cell membranes. One usually gets 3–5 mg of CoQ10 from daily supplements, although our body can synthesize it. With aging there is diminution in synthesis of CoQ10. 3 Several studies have reported that deficiency of CoQ10 is associated with neurodegenerative disorders, 4 cardiovascular diseases, 5 myopathy, 6 and cancer. 7 In mitochondrial respiratory mechanism, CoQ10 accepts electron for complex I and II and therefore assists in improving the adenosine triphosphate level. In Parkinson's disease patients, there is reduced complex I in the substantia nigra and this leads to destruction of dopaminergic neurons. CoQ10 helps in restoring the functions of dopaminergic neurons and prevents dopaminergic axons against excitotoxin-induced destruction. As age increases there is declination in ubiquinone and ubiquinol level in brain, which is one of the bases for neurodegenerative disease. The possible mechanisms of antioxidant activity of CoQ10 include activation of mitochondrial uncoupling protein expression. Actually such proteins are responsible for suppression of free radical production. 8 –10
A clinical trial involving 600 patients with early Parkinson's disease at 67 sites throughout North America tested the effectiveness of CoQ10 at 1200 and 2400 mg/day. The results showed that adjusted average changes in total Unified Parkinson's disease rating scale scores were 6.9 points (placebo), 7.5 points (1200 mg/day of CoQ10), and 8.0 points (2400 mg/day of CoQ10). The average plasma concentration of CoQ10 (patients receiving 1200 mg/day) was 5.80 μg/mL, whereas administration of 2400 mg/day produced an average level of 9.94 μg/mL. The level in the active treatment groups was elevated in comparison to placebo group. Investigators concluded that CoQ10 was safe and well tolerated. Although trial revealed no evidence of clinical benefits, failure to show clinical efficacy for CoQ10 in Parkinson's disease contrasts with expectations based on indication for oxidative stress and mitochondrial dysfunction in disease pathogenesis. 11 A phase II trial evaluating the efficacy of CoQ10 also reported similar disappointing results for amyotrophic lateral sclerosis (ALS). Kaufmann et al. designed and applied a multicenter trial. Their study results showed unsatisfactory evidence to explain Phase III trial of high dose CoQ10 for ALS treatment. 12
CoQ10 has demonstrated neuroprotective activity in multiple preclinical models of disease, including cell cultures and animal models of Parkinson's disease. It is very important to optimize administration because the oxidized form of CoQ10 achieves threefold less blood level in comparison to the reduced form of CoQ10 (ubiquinol). 13,14
Due to low solubility and high permeability, CoQ10 is categorized as a class-II drug according to the biopharmaceutical classification system and, therefore, its absorption is enhanced in presence of lipids. 15 That's why there is a need to develop a novel formulation of CoQ10 for overcoming the problem of poor aqueous solubility leading to improved oral bioavailability of CoQ10. For improving solubility and oral bioavailability of CoQ10 a number of approaches have been used starting from oil solutions, solid dispersions, complexation and nanoemulsions, and so on. 3 Most of the aforementioned techniques adopt lipid based delivery system, augmenting the absorption and bioavailability of lipophilic drug. 16,17 Main advantages of using lipids as a medium for drug delivery are that they enhance the solubility of water insoluble drug in the intestinal milieu, bypassing hepatic degradation by following intestinal lymphatic drug transport system and by altering enterocyte based drug transport. The aim of present study was to develop CoQ10 nanoemulsion using spontaneous emulsification method. Prepared nanoemulsion was characterized and evaluated to analyze the improvement in CoQ10 bioavailability.
Materials and Methods
Materials
CoQ10 was received as a gift sample from D.D Nutrition Pvt Ltd (Sonipat, Haryana). Labrafac lipophile WL 1349, Captex GTO, Capryol 90, Capmul MCM, and Transcutol P were obtained as a gift sample from Gattefosse (Saint Priest, Cedex, France). Solutol HS 15 as surfactant was obtained as a gift sample from Signet chemicals (Mumbai, India). Distilled water was obtained from Milli-Q water purification system (Millipore, MA). DPPH (2, 2-diphenyl-1-picrylhydrazyl) was obtained as a gift sample from Sigma-Aldrich (St. Louis, MO). High performance liquid chromatography (HPLC) grade of methanol and n-hexane were purchased from Loba Chemie Pvt Ltd (Mumbai, India) and Merck (Mumbai, India), respectively. HPLC grade of propan-2-ol and double distilled water were purchased from SD fine chemical Ltd (Mumbai, India). p-Benzoquinone was purchased from Alfa Aesar (England). All other remaining chemicals and solvents used in the study were of analytical grade.
Selection of excipients
Screening of oil phase
Higher CoQ10 solubility in oil is required to produce a stable nanoemulsion, as maximum solubility ensures high drug loading in nanoemulsion and prevents CoQ10 precipitation on longer period of storage. Solubility of CoQ10 in oils like vitamin E, Labrafac lipophile WL 1349, Captex GTO, Capryol 90, and Capmul MCM was determined by adding an excess amount of CoQ10 in 1 mL oil which was then allowed to mix using vortex shaker (Nirmal International, Delhi, India) for about 72 hours to reach to an equilibrium. Equilibrated samples were centrifuged at 3000 rpm for 15 minutes, supernatant was collected, and amount of CoQ10 dissolved was determined using UV spectrophotometer (Shimadzu, Kyoto, Japan) at 275 nm.
Screening of surfactants and cosurfactants
By reducing the interfacial tension existing at interface between two immiscible liquids (water and oil), surfactant plays an important role in production of stable nanoemulsion. Selection criteria used for surfactant were solubility of CoQ10 in surfactant along with its miscibility with the selected oil. Solubility of CoQ10 in various surfactants (Tween 20, Tween 80, Solutol HS 15, and Unitop FFT 40) was determined by adding an excess amount of CoQ10 in 1 mL of the selected surfactant and then allowed to mix using vortex shaker. Equilibrated samples were centrifuged at 3000 rpm for 15 minutes, supernatant was collected, and CoQ10 content was determined using UV spectrophotometer at 275 nm. Miscibility evaluation of surfactant with the selected oil was carried out by shaking 1:1 ratio of surfactant and oil. The mixture was visually observed for turbidity, opalescence, and phase separation. The mixture that remained clear was considered as miscible. In similar way selection of cosurfactant (Transcutol P, ethanol, propylene glycol, and polyethylene glycol 400) was done on the basis of miscibility with selected oil. 18
Pseudoternary phase diagram construction
For the preparation of phase diagram, oil exhibiting maximum drug solubility and specific ratio mixture of selected surfactant and cosurfactant (Smix) was mixed in different volume ratios from 1:9 to 9:1 making various combinations (1:9, 1:8, 1:7, 1:6, 1:5, 1:4, 1:3.5, 1:3, 3:7, 1:2, 4:6, 5:5, 6:4, 7:3, 8:2, and 9:1). Under moderate stirring, each mixture of oil and Smix was titrated with water. After each 5% addition of water to the volume ratio, visible observation was made. To attain equilibrium the system was left for 24 hours. Transparent easily flowable o/w emulsions were marked as nanoemulsion on a pseudo three component phase diagram with three axis representing aqueous phase, oil, and Smix at fixed weight ratio. 19,20
Selection of formulations from phase diagram
From each phase diagram, different formulations were selected having maximum nanoemulsion area that could incorporate the required amount of CoQ10 (100 mg) in oil without showing any sign of precipitation. Moreover, the composition composed of less Smix content, which could help in minimizing surfactant related adverse effects. In addition to this, the formulation was supposed to have more volume of water. Selected formulations were subjected to physical stability tests to reject unstable formulations.
Physical stability studies
Heating–cooling cycle test was performed to study the temperature dependent stability of nanoemulsions. In this test the formulation was stored at 25°C ± 2°C and 45°C ± 2°C for 24 hours. This storage at each temperature was carried out six times. Nanoemulsions exhibiting stability at these temperatures were further tested by freeze–thaw stress test. Freeze–thaw test was carried out by subjecting the selected formulations to six freeze–thaw cycles at temperatures between −20°C ± 2°C and +25°C ± 2°C with storage at each temperature for not less than 24 hours. Nanoemulsions that passed this test by exhibiting stability were considered stable and were subjected to centrifugation study. 18 Selected nanoemulsion was centrifuged at 5000 rpm for 20 minutes. Nanoemulsions which appeared clear were considered stable and were subjected to dispersibility test.
Dispersibility test
To evaluate the efficacy of nanoemulsion, dispersibility test was performed. The test was performed by mixing 2 mL of formulation with 250 mL of media (distilled water and 0.1 N HCl) in a beaker and stirred continuously by placing on magnetic stirrer. This test was carried out to verify the homogeneity of the formulation. As represented in Table 1, different grading was given to the formulation.
Drug loading
The physically stable placebo nanoemulsions were subjected to CoQ10 loading. For this purpose, 100 mg CoQ10 was dissolved in oil phase and mixed with required amount of Smix, followed by addition of water under constant vortexing. Drug loaded nanoemulsions were again subjected to physical stability tests to reject physically unstable formulations.
Characterization of Optimized Formulation
Droplet size and droplet size distribution of selected nanoemulsion formulation were determined using photon correlation spectrometer (PCS, Zetasizer 1000 HAS; Malvern Instruments, Worcestershire, UK). All the formulations were properly diluted to about 200 times with distilled water followed by vigorous shaking to minimize multiple light scattering effects before each measurement. Polydispersity index (PDI), which is a measure of droplet size distribution in the sample, was measured. 3 UV spectrophotometer was used to determine percentage transmittance. Formulation (1 mL) was diluted with methanol (500 times), and percentage transmittance was noted at 630 nm by taking methanol as blank. 18 One to two drops of nanoemulsion was placed on slide, and refractive index was measured thrice using an Abbe type refractometer (Nirmal International). Viscosity was measured without dilution using a Brookfield DV III ultra V6.0 RV cone and plate viscometer (Brookfield Engineering Laboratories, Inc., Middleboro, MA). All the measurements were carried out at a temperature of 25°C ± 0.5°C using Rheocale V2.6 software. Surface charge of nanoemulsion was determined by measuring the electrophoretic mobility. Measurements were performed by diluting 20 μL of sample up to 10 mL with distilled water and analyzed by zeta potential measuring instrument (PCS, Zetasizer-1000 HAS; Malvern Instruments). CoQ10 nanoemulsion was studied for surface morphology using transmission electron microscopy (TEM) after proper dilution with water (1:1000). A drop was taken and deposited on a wax paper, which was further stained with 2% (w/v) phosphotungstic acid and air-dried. The prepared slide was observed for surface morphology with the help of Morgagni 268D transmission electron microscope (FEI, Hillsboro, Holland) operated at 70 kV. 21
In Vitro Release Studies Using Dialysis Bag
In vitro studies were performed to compare the release of CoQ10 from nanoemulsion formulations (A10, B6, B7, and C7) with CoQ10 suspension. One milliliter of nanoemulsion formulation (10 mg/mL) and CoQ10 suspension were filled in dialysis bag (MWCO 1200 g/mol; Sigma-Aldrich), and these dialysis bags were placed in basket of USP apparatus (type I) containing 250 mL of phosphate buffer (pH 6.8), which was maintained at temperature of 37°C ± 0.5°C and stirring rate of 100 rpm. Five milliliter samples were withdrawn at regular time intervals (5, 10, 20, 30, 60, 120, 180, 240, 300, and 360 minutes) and analyzed for CoQ10 content using UV spectrophotometer at 275 nm.
In Vitro Release Studies Using Intestinal Segment
To check whether our developed nanoemulsion formulation releases more CoQ10 in comparison to CoQ10 suspension, the in vitro release studies using intestinal segment was carried out. As droplet size is one of the important factors for oral drug delivery of drug to the brain because nano size droplets have more surface area and favors more permeation of drug through intestinal membrane resulting in more drug release from nanoemulsion leading to rapid absorption and enhanced bioavailability. All animal experiments were carried out after approval of protocol by Institutional Animal Ethics Committee (approval no. 173/GO/Re/S/2000/CPCSEA), Hamdard University, New Delhi, India and their guidelines were adhered for the complete study. To determine the release using rat intestinal segment, rats were sacrificed and their abdominal cavity was opened by a midline incision and the small intestine was exposed. About 5 cm segment of the duodenum was incised and cleaned with Kreb solution (pH 6.5) to remove excretory product present in the duodenum by flushing. The proximal end of each duodenum section was tied up before introducing formulation (A10, B6, B7, and C7) and CoQ10 suspension through a syringe. Other end of duodenum section was also tied. Integrity of duodenum was assessed visually. Release study was performed in freshly prepared 150 mL of Kreb solution (pH 6.5). The magnetic stirrer was adjusted to 100 rpm at a temperature of 37°C ± 0.5°C and was provided with adequate aeration. Duodenum was kept inside the beaker. At different time intervals 5 mL samples were taken out. The withdrawn samples were analyzed spectrophotometrically for the drug content at 275 nm, and the volume withdrawn at each sampling time was replaced by same volume of Kreb solution (pH 6.5).
Everted Gut Sac Studies
Everted gut sac studies were carried out to evaluate permeation rate of formulation through intestinal permeation. The small size droplet of nanoemulsion ensured better permeation due to increased surface area resulting in more quantity of CoQ10 absorption through gastrointestinal tract (GIT) membrane and drug being rapidly transported across the brain through BBB thus increasing availability of CoQ10 in brain resulting in increased therapeutic effect. For this purpose, duodenum segments (∼5 cm) were used which were washed with Kreb solution (pH 6.5) and ligated with nylon thread at one end and carefully everted on the glass rod. The everted gut sac was filled with 1 mL of Kreb solution (pH 6.5), ligated, and placed inside the beaker containing 20 mL of A10 nanoemulsion formulation, and CoQ10 suspension continuously bubbled with atmospheric air at 13–19 bubbles per minute and was maintained at temperature of 37°C ± 0.5°C. Kreb solution (pH 6.5) outside the sac was termed as mucosal fluid, and the solution inside the gut sac was termed as serosal fluid. Amount of CoQ10 that permeated across the intestine in serosal fluid was determined spectrophotometrically at predetermined time period (0.5, 1, 1.5, and 2 hours). Permeability coefficient (Papp) of CoQ10 was calculated from mucosal to serosal direction according to the equation:
where dQ/dt is the rate of drug permeation from the tissue, A is the cross-sectional area of the tissue, and C0 is the initial CoQ10 concentration in the donor compartment at t = 0.
Antioxidant Activity
Antioxidant activity of pure CoQ10 and nanoemulsion (A10) were compared with that of ascorbic acid which was taken as the standard antioxidant using DPPH method.
18
Stock solutions (1 mg/mL) in methanol were prepared for ascorbic acid, pure drug CoQ10, and optimized formulation (A10). Then further serial dilutions (1–50 μg/mL) were performed in methanol for all samples. Simultaneously, 1 mm of DPPH solution was added to 1 mm of each dilution of samples. After 0.5 hour, absorbance (at 515 nm) of each sample was recorded using UV spectrophotometer by taking methanol as blank. Percentage inhibition was determined using following equation:
where A0 is absorbance of blank (without drug), and A1 is absorbance of samples. Mean percentage inhibition was plotted against log concentration, and 50% inhibitory dose (IC50 value) was determined by extrapolation using GraphPad software and was compared with standard.
Pharmacodynamic Study
Wistar albino rats of either sex (200–250 g) were divided into four groups each containing three rats. Motor impairment was induced with haloperidol and determined by photoactometer, swimming, catalepsy, and rotarod tests as reported earlier. 21 On the day of experiment, group A rats were treated with only saline vehicle (0.9% w/v NaCl, 100 μL) orally. Group B rats were treated with haloperidol (2 mg/kg, intraperitoneally [i.p.]). Group C rats were treated with haloperidol by i.p. route and after 30 minutes they were treated with CoQ10 suspension orally. Group D animals were treated with haloperidol and after 30 minutes they were administered CoQ10 nanoemulsion orally. After giving treatment, different behavioral studies such as locomotor activity, forced swimming test, catalepsy, rotarod test, and akinesia test were carried out.
Locomotor activity test
Locomotor activity of all the four groups was carried out using digital photoactometer (Inco Photoactometer, India). The instrument was validated manually before each test by interrupting the infrared rays and verifying the actual number of rays which break with the number recorded. Before experiment, rats were habituated for 15 days in photoactometer chamber. Rats were placed in the chamber for 1 hour after oral administration of formulations. Six beams of infrared light were focused 2 cm above the floor into the photocells on opposite side. Each beam interruption was noted automatically on a digital screen. The behavior of rats in each group was compared. 21 –24
Forced swimming test
Forced swimming test was carried out by placing animals in a transparent water tub (40 cm height × 25 cm diameter) filled with fresh water to a depth of 30 cm (25°C ± 2°C), which allowed the rats to swim or float without their hind limbs touching bottom of tub. Behavioral analysis of rats was recorded at the end of each 5 minute period during the test session. The effect of treatment on mean immobility time, climbing time, and swimming time was observed and recorded. Immobility time was noted when the rat was making the less movements required to stay afloat. Climbing time was recorded when the animal made vigorous thrashing movements with its fore paws, usually directed against the sides of tub. Swimming time was recorded as an active behavior when the animals actively swim around the tub. 25
Catalepsy
The test was performed by placing animal with their fore paws in half rearing position on a horizontal bar. The bar was kept at 9 cm above from the parallel base. Each rat was tested thrice in succession with a maximum cutoff time of 2 minutes. Time for full descent (no longer in contact with the horizontal bar) was recorded. Animals were considered as cataleptic if one of their paws stayed on the bar for more than 30 seconds. 21
Muscle coordination test
Muscle coordination test was carried out using Rota-rod apparatus (Omnitech Electronics, Inc., Columbus). Rats from all the groups were trained thrice daily for three successive days. The rotation per minute of rotating rod was set at 2–6 rotations/min. The time period for which rats stayed on the rotating bar was noted. Maximum trial length was 180 second per trial. Time at which the rats fell on base from the rod was automatically recorded. 21
Akinesia test
Akinesia measurement was performed as described by Olsson et al. 26 by recording the latency in seconds of animals to move all the four limbs. Study was terminated when latency exceeded 3 minutes. Time taken by each animal to move the entire four limbs was recorded.
Pharmacokinetic Studies
Pharmacokinetic studies were carried out using Wistar albino rats and performed by the procedure previously described by Sharma et al. 22 to compare the plasma profiles of CoQ10 formulations (nanoemulsion and suspension). Rats were divided into two groups each containing six rats. Group A received CoQ10 suspension orally at a dose of 5.4 mg/250 gm, whereas group B received CoQ10 nanoemulsion orally at a dose of 5.4 mg/250 gm. The blood samples were obtained after 1, 2, 4, 6, 8, and 24 hours from retino-orbital vein of eye, and the concentration of CoQ10 in blood was analyzed by validated HPLC method.
Bioanalytical HPLC method and plasma sample preparation
A reverse phase-HPLC method was used to determine CoQ10 content in blood sample using a mixture of methanol and n-hexane (in a ratio of 78:22 v/v) as mobile phase. A quaternary pump HPLC system (Shimadzu, Tokyo, Japan) consisting of a pump (LC-10AT), Rheodyne injector, and UV detector (SPD-10A) was used for liquid chromatography separation. Analysis was performed on a LiChrospher®C18 column (250 × 4.6 mm, 5 μm in particle size; Merck, Germany) by maintaining a flow rate of 1 mL/min and retention time of 5 minutes. Liquid/liquid extraction technique was used for CoQ10 extraction from plasma. To 100 μL of plasma samples about 10 μL of p-benzoquinone solution (2 mg/mL) was added and then shaken with 2-propanol (400 μL) for 1.5 minutes using vortex mixer. The mixture was centrifuged at 8000 rpm for 3 minutes, and supernatant was collected and dried. Finally, the residue was dissolved in methanol (100 μL), and about 20 μL of sample was injected into the HPLC column for CoQ10 quantification. 27
Determination of pharmacokinetic parameters
Plasma CoQ10 concentration-time profile after oral administration of CoQ10 formulations was evaluated by pharmacokinetic software (Microsoft Excel PK Function, CA). Parameters like maximum plasma concentration (Cmax), time to reach the maximum concentration (Tmax) in plasma, and area under the curve (AUC) were determined.
Biochemical Estimation
Haloperidol antagonizes dopamine D2 and to a lesser extent D1 receptor. Blockage of dopamine transmission in striatum leads to abnormal downstream firing within the basal ganglia circuits, which is manifested as symptoms of catalepsy and muscle rigidity within 1 hour of haloperidol (0.5–5 mg/kg, i.p.) injection. Rigidity and catalepsy are features of Parkinson's disease. As a biochemical mimic of Parkinson's disease, administration of haloperidol decreases the dopamine level in striatum. 28 Many antiparkinson drugs have shown efficacy in the haloperidol model, including L-DOPA, bromocriptine, pramipexole, trihexyphenidyl, and amantadine, 29 –32 supporting the predictive validity of this model.
Haloperidol induces formation of reactive oxygen species (ROS) as it increases the level of thiobarbituric acid reactive substances (TBARS) and decreases the level of antioxidant enzymes, which act as markers of oxidative stress. Oxidative nigrostriatal damage in haloperidol-induced rats has been reported in previous studies. 24,25,33 Thus, ROS-scavenging antioxidants help in the prevention of Parkinson's disease and combat against oxidative stress-induced progressive neurodegeneration.
Biochemical estimation study was carried out in rats. Rats were divided into four groups. Group A rats were administered with saline and were considered as normal group. Group B animals were administered haloperidol (i.p.) to cause biochemical changes. Group C animals were administered haloperidol (i.p.) along CoQ10 suspension orally. Group D animals were administered with haloperidol (i.p.) and after half an hour they were treated with CoQ10 nanoemulsion administered orally. Glutathione (GSH) and TBARS content for all groups were evaluated.
GSH estimation
About 500 mg brain were weighed and put into the test tube containing 2.5 mL of 0.02 M EDTA and homogenized using tissue homogenizer and then volume was made up to 5 mL mark with 0.02 M EDTA. Homogenate (5 mL) was mixed with water (4 mL) and 1 mL of 50% trichloroacetic acid (TCA). Tubes were shaken intermittently for about 10–15 minutes and then centrifuged at 3000 rpm for 15 minutes. After that, 2 mL of supernatant were mixed with 4 mL of 0.4 M Tris buffer (pH 8.9). To this mixture 0.1 mL of 0.01 M 5, 5′-dithiobis-(2-nitrobenzoic acid) (DTNB) was added. Absorbance (at 412 nm) was recorded against a reagent blank (i.e., 4 mL distilled water, 1 mL of 50% TCA, 4 mL of 0.4 M Tris buffer, and 0.01 M DTNB). The amount of GSH in the tissue was calculated from the following equation.
34
where E and D are extinction coefficient of DTNB and dilution factor, respectively.
TBARS estimation
About 0.2 mL of homogenate was mixed with 0.2 mL of 8.1% sodium dodecyl sulfate. About 1.5 mL of 20% acetic acid was added to the mixture. pH of solution was adjusted to 3.5 using NaOH. Then 1.5 mL of 0.8% aqueous solution of thiobarbituric acid (TBA) was added, and mixture was diluted up to 4 mL using distilled water followed by heating the mixture at 95°C for 1 hour. After cooling, distilled water (1 mL) and 5 mL mixture of pyridine and n-butanol (1:15 w/v) were added. The mixture was further centrifuged at 4000 rpm for 10 minutes. The organic layer was collected, and the color produced by chemical reaction was recorded at 540 nm against a blank reaction mixture (3 mL distilled water, 0.6 mL sodium dodecyl sulfate, 4.5 mL acetic acid, and 4.5 mL TBA). Content of malondialdehyde (MDA) present in homogenate was determined using the following equation
35
:
where O.D. is optical density at 540 nm.
Histopathology of Brain Section
Hematoxylin and eosin staining method was used to study the histopathology of brain section. 25 The examination was performed to assess the neuronal damage caused by haloperidol and the role of CoQ10 loaded nanoemulsion to improve the damage. Normal brain (negative control), haloperidol treated brain (positive control), haloperidol treated brain followed by CoQ10 suspension, and haloperidol treated brain followed by CoQ10 nanoemulsion were fixed immediately in 10% formalin and embedded in paraffin after isolation. Brain tissue was washed with isopropyl alcohol and placed in acetone for 30 minutes. Brain tissue was treated with xylene and embedded in paraffin wax. Fine cutting of brain tissues (3–5 μm) was done and stained. The stained sections were then observed under the optical microscope at 40 × magnifications.
Statistical analysis
For a statistical analysis of the data, group means was compared by one-way analysis of variance (ANOVA) followed by Dunnett's multiple comparison test, which can be used to identify differences between groups. p Value <0.05 was considered significant.
Results and Discussion
Selection of oil phase
Oil is one of the most important excipients used in preparation of nanoemulsion, which can solubilize sufficient amount of the drug and would help the nanoemulsions to maintain the drug in solubilized form and provide good stability as forced solubility of drug in oil could lead to precipitation of drug. Oil phase was selected on the basis of CoQ10 solubility in it. CoQ10 showed solubility of 190.00 ± 11.13, 110.00 ± 18.02, 130.00 ± 20.00, and 40.00 ± 13.22 mg/mL in vitamin E, Captex GTO, Capryol 90, and Capmul MCM, respectively (Table 2). Labrafac lipophile WL 1349 showed maximum solubility of drug (250.00 ± 8.66 mg/mL). Labrafac lipophile WL 1349 is a medium chain triglyceride comprising of glyceryl esters. Generally, it is triglycerides of caprylic and capric acids. It is used in SEDDS/SMEDDs for oral bioavailability enhancement of drug.
SD, standard deviation.
Selection of surfactant and cosurfactant
Surfactant plays an important role in formation of a stable nanoemulsion. Selection of surfactant is also critical as the selected surfactant should not only lower the interfacial tension but also should be safe at concentration used. Nonionic surfactants are considered to be less toxic than the ionic surfactants. From the solubility studies it was observed that CoQ10 exhibited maximum solubility in Tween 80 (20.00 ± 2.64 mg/mL), Solutol HS 15 (20.00 ± 4.58 mg/mL), and Unitop FFT 40 (20.00 ± 3.51 mg/mL), but Solutol HS 15 was selected as surfactant because it showed good miscibility with the selected oil phase (Labrafac lipophile WL 1349) (Table 2). Chemically, Solutol HS 15 is polyethylene glycol (15)-hydroxystearate. It is a nonionic solubilizer and emulsifier. Surfactant alone cannot reduce the interfacial tension to a very low value. To further reduce the interfacial tension and to obtain flexible interfacial film, cosurfactants are usually used. These assist further minimization of bending stress of interface and provide sufficient flexibility to interfacial film. 21,25 Selection of cosurfactant was done on the basis of miscibility with Labrafac lipophile WL 1349 oil and surfactant (Solutol HS 15). Transcutol P was selected as cosurfactant because it showed miscibility with selected oil and surfactant. It is diethylene glycol monoethyl ether and is used as solubilizer for various drugs.
Phase diagram construction
Phase diagram construction was carried out using Labrafac lipophile WL 1349 as oil phase, Solutol HS 15 as surfactant, Transcutol P as cosurfactant, and distilled water as aqueous phase. Different ratios of Smix were tried and it was found that the area of nanoemulsion region was different with each Smix (Fig. 1). In Smix ratio 1:1, the area of nanoemulsion was less than 1:2 indicating that the solubilization of the oil phase by Smix was less. In Smix ratio 2:1 it increased further and maximum area was found in 3:1 Smix ratio indicating that this Smix was able to solubilize more amount of oil resulting in the formation of a clear solution. When Smix ratio was increased to 4:1, the area slightly decreased indicating that on further addition of surfactant no more emulsification was taking place. Therefore, it was concluded that maximum nanoemulsification was achieved in 3:1 Smix ratio. From each phase diagram, various formulation points were chosen on the basis of oil concentration such that it dissolved 100 mg of drug and had less Smix ratio and more water content (Table 3).
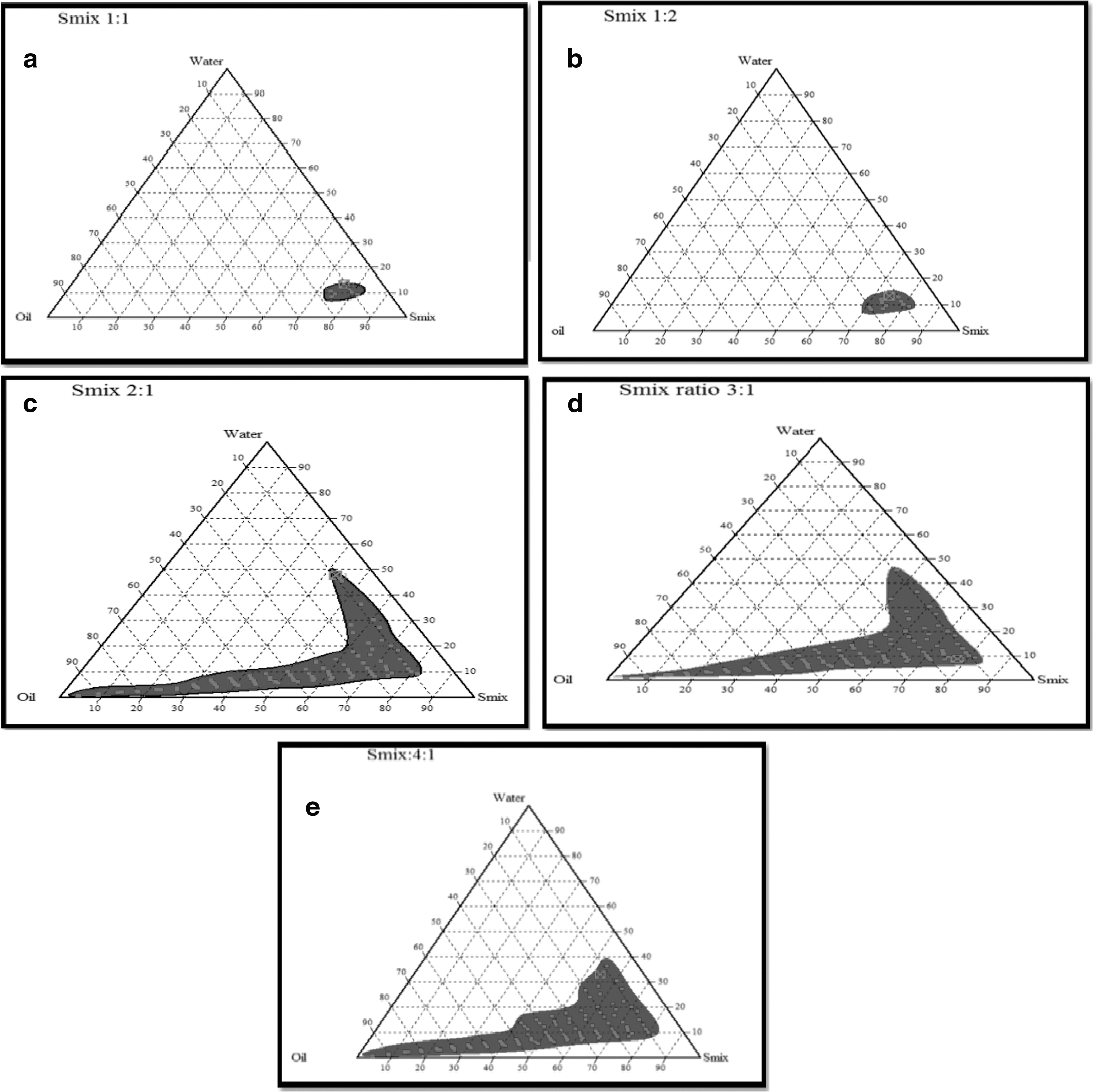
Pseudo ternary phase diagram showing existence of o/w nanoemulsion region for different surfactant: cosurfactant ratios (or Smix).
CF, centrifugation; Disp, dispersibility; F/T, freeze–thaw; H/C, heating–cooling cycle.
Selection and optimization of formulations
Nanoemulsions are kinetically stable system produced at a specific amount of oil, Smix, and water. Selected formulations were subjected to different stress conditions as represented in Table 3. The physical stability testing was done to determine the stability of prepared formulations at low and higher temperature and at high shear. The results of physical stability test showed that few nanoemulsions failed the test, that is, they either showed turbidity or phase separation. The reason may be coalescence of oil droplets which may be due to Ostwald ripening. 36 Another reason may be temperature quenching which leads to phase separation.
Drug loading
Physically stable placebo formulations were subjected to drug loading. The composition of the drug loaded formulation is represented in Table 4. When drug loaded nanoemulsions were subjected to physical stability testing, some formulations became unstable and were discarded. The stable nanoemulsions were further characterized.
CoQ10, Coenzyme Q10.
Characterization of formulation
Formulation had droplet size in the nano range with low values of polydispersity. Average droplet sizes and PDI of the optimized formulations were in the range of 20.05 ± 2.53 to 30.69 ± 2.58 nm and 0.121 ± 0.053 to 0.310 ± 0.058, respectively (Table 5 and Fig. 2). Droplet size of the nanoemulsion plays a key role in deciding the rate and extent of drug release. 37 Droplet size of formulation is one of the important parameters for oral delivery of drugs as nanosize droplets exhibit higher surface area and favor high permeation of drug through GIT membrane leading to more release of drug from formulation and hence resulting in enhanced bioavailability. PDI value indicates the uniformity of droplet size within the nanoemulsion. The higher the value of polydispersity, the lower is the uniformity of droplet size in the formulation. The values more than 0.50 suggest broader size distribution; on the other hand value below it suggests narrow size distribution. 38 Among all nanoemulsion batches, formulation A10 exhibited smallest droplet size; thus was considered for further studies.
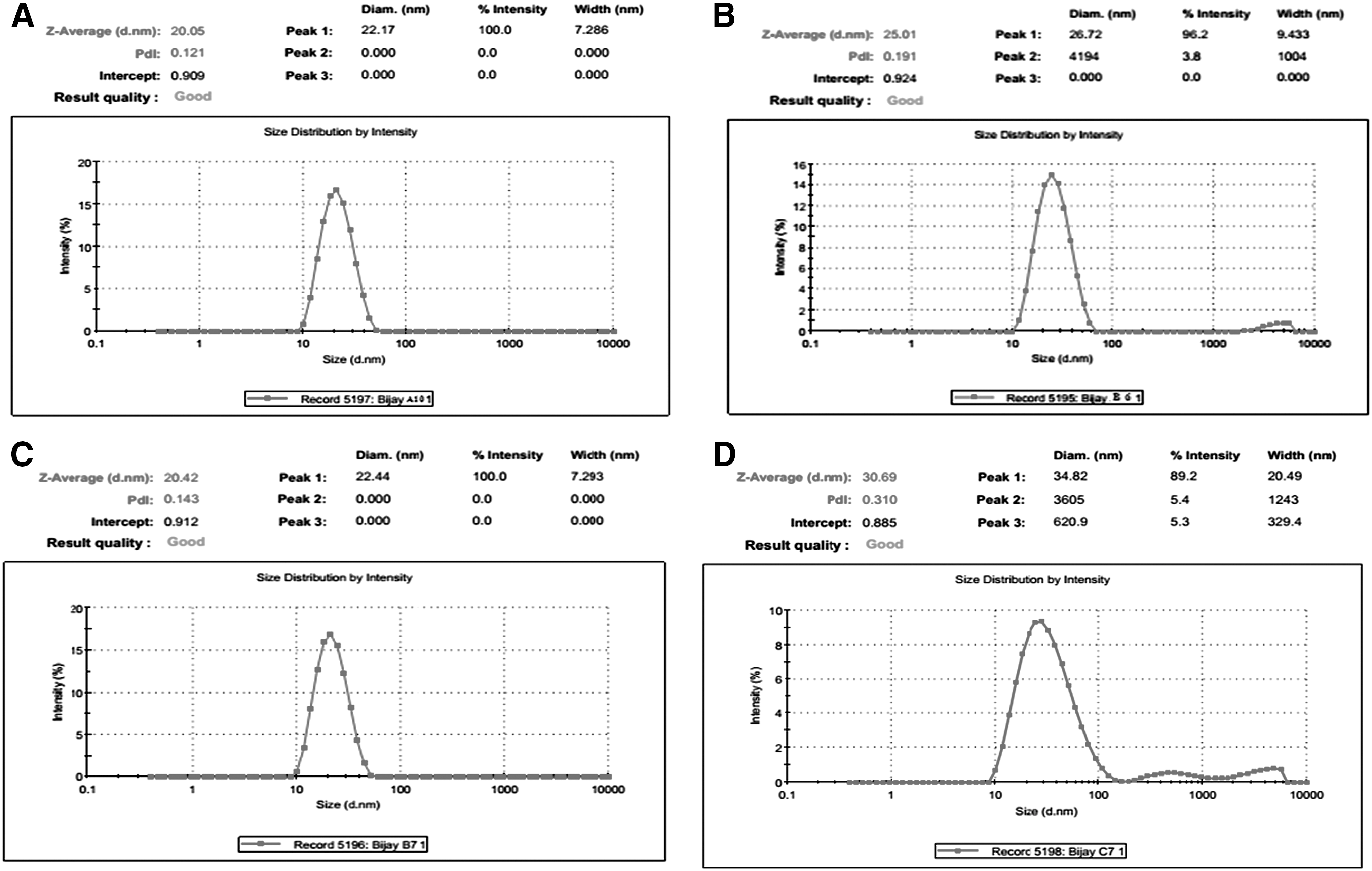
Droplet size and PDI
PDI, polydispersity index.
Nanoemulsion droplets were studied for morphology which showed spherical droplets with size of 60.00 ± 15 nm (Fig. 3). No aggregation was observed. Zeta potential indicates the physical stability of the emulsion. A value of ±30 mV for zeta potential represents significant distance between charged droplets in the dispersion system, thus preventing the chances of coalescence of droplets in the nanoemulsion system. 19 The zeta potential values of optimized formulations were found to be in the range of −18.23 ± 0.24 to −24.40 ± 0.16 mV (Table 5 and Fig. 4). The formulation A10 exhibits zeta potential value of −24.40 ± 0.16 mV suggesting more stable formulation. Negative charge on the nanoemulsions is possibly due to free fatty acids present in oil phase used.

TEM image of CoQ10 nanoemulsion (A10). CoQ10, coenzyme Q10; TEM, transmission electron microscopy.

Zeta potential of nanoemulsion formulation (A10).
As represented in Table 5, the viscosity of the formulation A10 was found to be 30.54 ± 2.86 cP, which is less than 50 cP hence confirming better tolerance on oral administration. Refractive index characterizes the isotropic nature of the formulation and also signifies the chemical interaction among drug and excipients. 19 No significant difference in the refractive index was observed between drug loaded nanoemulsion and placebo formulation, which revealed that the nanoemulsion formulation was chemically stable. Moreover, the value of refractive index indicates that the produced formulation is isotropic in nature (Table 5). Refractive index of optimized formulation (A10) was found to be 1.41 ± 0.02, showing isotropic nature of formulation. Transmittance of the formulation was found to be 100.50% ± 0.86%. The resulted transparency of formulation was due to the reason that maximum size of the droplets of oil was not more than one fourth of the visible light wavelength.
In vitro release using dialysis bag
In vitro release experiments in phosphate buffer (pH 6.8) were performed to compare the release of CoQ10 from nanoemulsion formulations (A10, B6, B7, and C7) with CoQ10 suspension. A significant increase in percentage drug release was achieved in case of nanoemulsion compared to that of CoQ10 suspension. In CoQ10 suspension, drug release was too slow with only 43.45% after 360 minutes, and drug precipitation was observed in the dialysis bag. The maximum release was found to be 93.22% after 360 minutes for A10 nanoemulsion formulation. A minimum release of 64.12% was observed for C7 nanoemulsion formulation after 360 minutes. This could have been due to the bigger droplet size, which might have slowed down the release of the drug. All the nanoemulsion formulations showed better results compared to CoQ10 suspension because of small droplet size (Fig. 5). The release kinetic was determined by fitting the data obtained from in vitro release studies of A10 nanoemulsion formulation into standard release equation, that is, Zero order, First order, Higuchi, and Korsmeyer–Peppas. The model that fits best the release data was selected based on correlation coefficient value of various models. R 2 of zero order, first order, Higuchi, and Korsmeyer and Peppas model for optimized formulation was found to be 0.9275, 0.9671, 0.9895, and 0.9757, respectively. The result suggested that release of drug (A10) follows Higuchi model as indicated by higher R 2 value, that is, 0.9895.
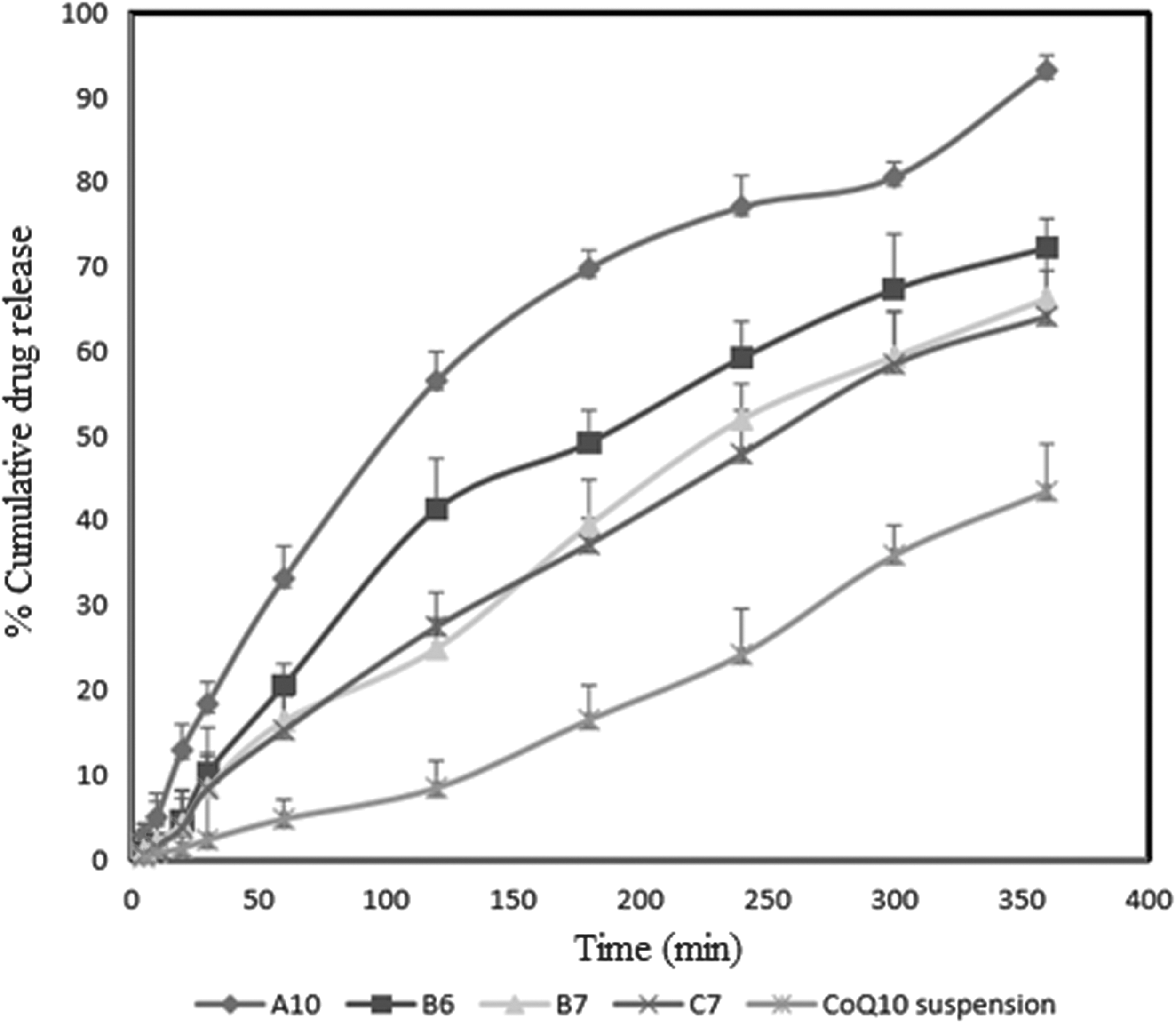
In vitro release profile of CoQ10 nanoemulsion (A10, B6, B7, C7) and CoQ10 suspension.
In vitro release using intestinal segment
Formulation A10 showed a maximum release of 95.137% at 360 minutes compared to CoQ10 suspension, which showed 56.65% release at 360 minutes as shown in Figure 6. More release from nanoemulsion was because of decreased size of formulation in nanometric range. Availability of CoQ10 at the molecular level in the form of nanosized emulsion droplets has a remarkable enhancing potential on drug release from nanoemulsion. It was further observed that as there was reduction in droplet size the drug permeation increased. CoQ10 present in nano droplets diffused from the membrane and appeared in the medium which was dependent on the size of droplets. But in the case of CoQ10 suspension, there was little appearance of CoQ10 in medium indicating that CoQ10 was not properly solubilized and therefore showed less permeation through the duodenum. Hence, availability of CoQ10 at the molecular level in the form of nanosized emulsion droplets had a remarkable enhancing potential on drug release from nanoemulsion.

Release studies (using intestinal segment) of CoQ10 developed nanoemulsion (A10, B6, B7, and C7) and CoQ10 suspension.
Everted gut sac studies
The main aim of everted gut sac method was to determine intestinal membrane permeability on the basis of drug transport across the membrane from the donor compartment to the receiver environment. CoQ10 suspension showed Papp of 4.44 × 10–6 cm/h with flux of 0.0444 μg/(cm2·h) at 2 hours, whereas in same time CoQ10 loaded A10 nanoemulsion produced a Papp up to 7.77 × 10−6 cm/h with flux of 0.0777 μg/(cm2·h) (Table 6). Enhancement ratio of nanoemulsion formulation (A10) was found to be 1.75-fold higher than the CoQ10 suspension. Permeability study results indicated that CoQ10 in suspension form poorly permeated across the duodenum but when CoQ10 was loaded in the nanoemulsion, the droplet size decreased, and CoQ10 was easily solubilized in the donor compartment and permeated from the duodenum. This indicated that the absorption of CoQ10 occurred within the oil droplet. The CoQ10 present in nano size droplets permeated from the mucosal side and appeared in the serosal medium basically due to the nano size of droplets. The improved permeability of nanoemulsion is considered to be an important technique for enhancing the bioavailability of drug.
Antioxidant activity
Antioxidant activity of CoQ10 on DPPH radical scavenging is because of hydrogen donating ability. 19 CoQ10 is an antioxidant and it inhibits lipids, protein, and DNA oxidation. Moreover, it inhibits the peroxidation of lipoprotein lipids. 39 The effect of CoQ10 to reduce DPPH radical was obtained by determining the decrease in absorbance at 515 nm, which was also visually noticeable as a discoloration from purple to yellow. A significant decrease in the DPPH radical content was obtained because of free radical scavenging activity of CoQ10, nanoemulsion formulation, and ascorbic acid (standard antioxidant). Percentage inhibition obtained was maximum for optimized formulation A10 (82.49%) compared to pure CoQ10 (59.74%) as shown in Figure 7. Antioxidant activity for the optimized formulation may be because of more solubilization of drug in it. Fifty percent inhibitory dose (IC50 value) was determined by extrapolation and it was found to be 10.00, 14.99, and 20.00 μg/mL for ascorbic acid, nanoemulsion (A10), and pure drug, respectively.
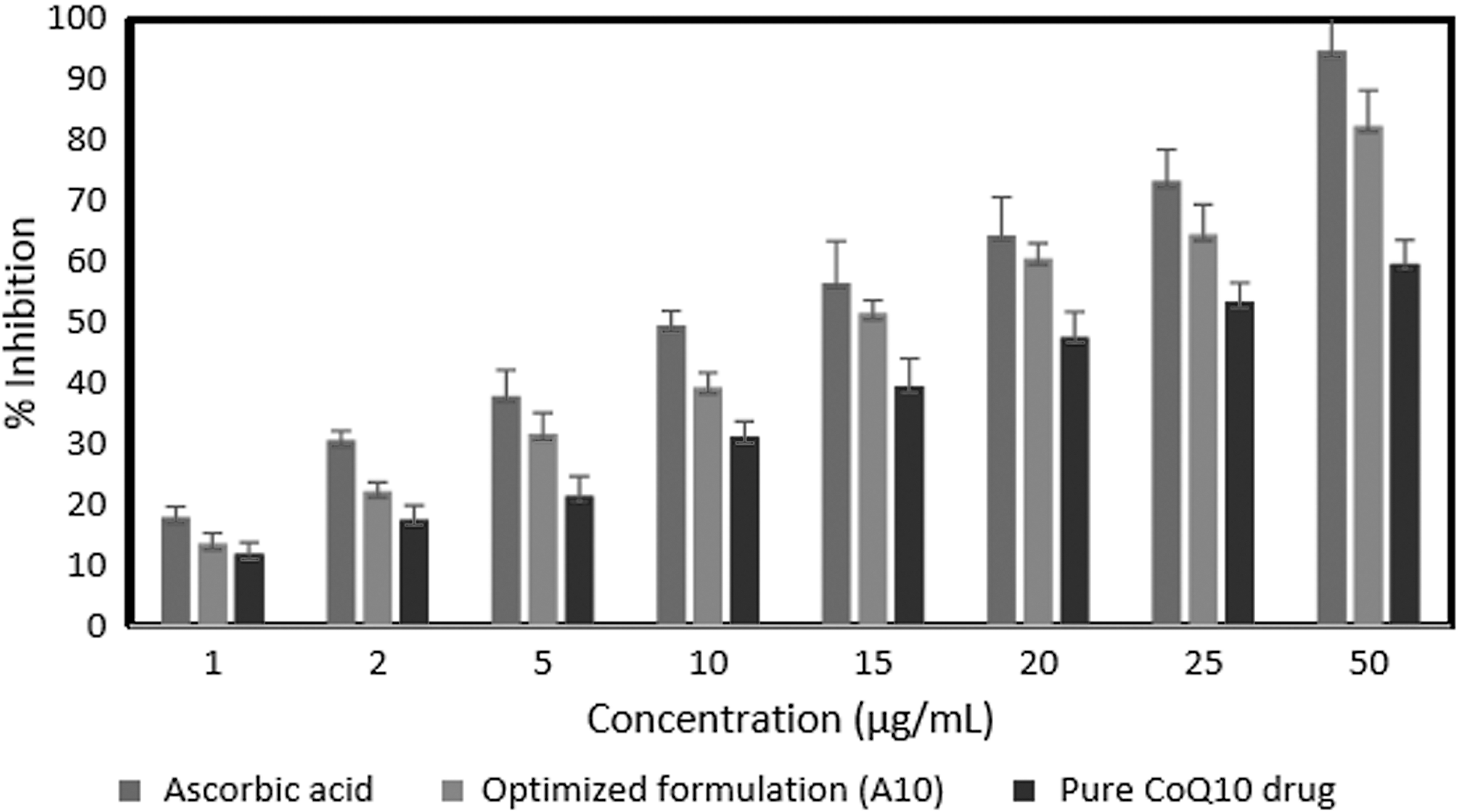
Comparison of antioxidant activity of ascorbic acid, A10 and pure drug (CoQ10).
Pharmacokinetic studies
Observations of in vitro properties of CoQ10 loaded nanoemulsion encouraged to clarify the possible improvement in the bioavailability of CoQ10 by the assessment of the pharmacokinetic behavior of CoQ10 loaded nanoemulsion formulations in rats. CoQ10 loaded nanoemulsion (A10) and CoQ10 suspension were orally administered to Wistar albino rats for conducting oral bioavailability studies. It was found that nanoemulsion showed a Cmax of 2.90 ± 0.27 μg/mL compared to CoQ10 suspension, which had a Cmax of 1.21 ± 0.21 μg/mL (Table 7 and Fig. 8). Similarly, the Tmax was 2.00 ± 0.65 and 4.00 ± 0.68 hour for nanoemulsion formulation (A10) and CoQ10 suspension, respectively. The AUC0–24 of optimized formulation (A10) was found to be 29.25 ± 3.41 μg/mL·h compared to 16.08 ± 2.91 μg/mL·h of CoQ10 suspension indicating an increase in the extent of drug absorption of CoQ10 when it was loaded in the nanoemulsion formulation. Similarly, the AUC0–∞ and Kel were 48.98 ± 1.87 μg/mL·h, 0.05 hour−1 and 39.70 ± 2.18 μg/mL·h, 0.01 hour−1 for nanoemulsion formulation (A10) and CoQ10 suspension, respectively. Relative bioavailability of nanoemulsion formulation (A10) was found to be 1.82-fold higher than the CoQ10 suspension. These results showed that incorporation of CoQ10 into nanoemulsion formulation (A10) resulted in its enhanced absorption after oral administration due to smaller droplet size and large surface area. 40,41
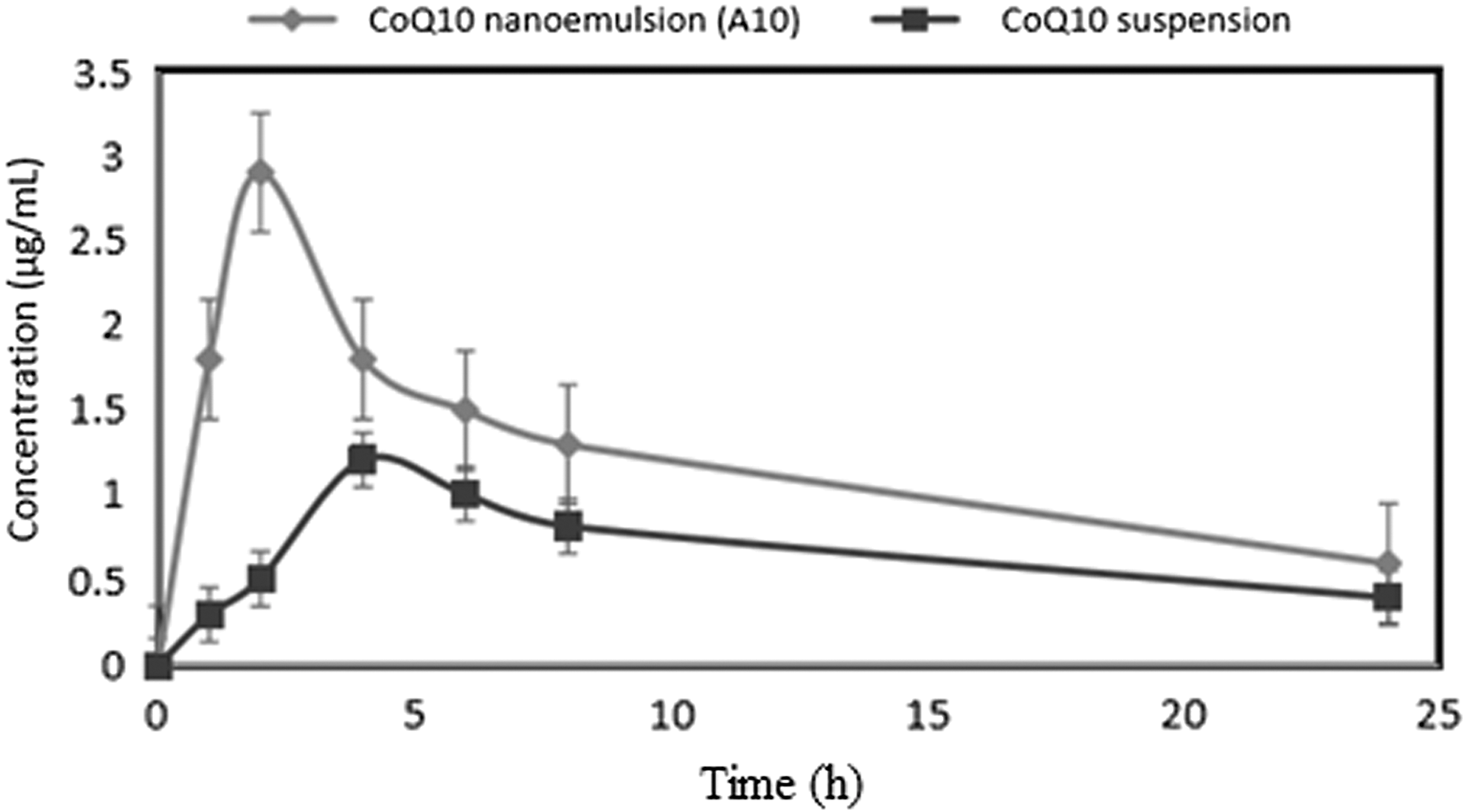
Comparative in vivo absorption profile of CoQ10 nanoemulsion (A10) and CoQ10 suspension.
AUC, area under the curve.
Pharmacodynamic study
Angulo et al. demonstrated that by haloperidol treatment, D2 mRNA and receptor levels were reduced in the anterior and medial aspects of the caudate–putamen and the nucleus accumbens. 42 CoQ10 protected against dopamine depletion. This has been confirmed by studies carried out by Beal et al., Cleren et al., and Yang et al. 43 –45 In the present work, by administering CoQ10 the level of dopamine increases as observed by behavioral studies. The motor activity is directly related with dopamine level, that is, dopamine depletion leads to reduced behavioral activity and vice versa.
In Parkinson's disease there is a direct relationship among disease duration, extent of dopamine loss, and motor dysfunction. Behavioral studies were performed to evaluate the efficacy of antiparkinson drug and to provide information regarding the neurotransmitters functioning in brain, which affects the motor and behavioral activity of rats. 16,46 Haloperidol-induced Parkinson disease Wistar rats were used to determine the pharmacodynamic potential of developed CoQ10 nanoemulsion for oral administration in comparison to other dosage (suspension). Various behavioral studies were performed to evaluate the effect of prepared formulations on reducing the disease symptoms in haloperidol Parkinson disease induced rats. Generally forced swimming test is based on the principle of inducing immobility in animals and then determining its reversal by antiparkinson drug. The immobility state indicates decreased muscle movements due to altered neurotransmitter levels (like decreased dopamine level which is responsible for movements of body) and induces symptoms of Parkinson's disease. Locomotor activity study is based on a hypothesis that increase in locomotor activity is because of increased dopaminergic activity in the mesolimbic system. Catalepsy study evaluates the incapability of animal to rectify an externally forced posture. This test was performed to determine the effect of delivery system in improving the cataleptic behavior of haloperidol challenged rats. Akinesia represents the delay in initiating a movement, which is a general abnormality in motor function in Parkinson's disease. This test is simple, rapid, and helpful in providing information regarding the upper limb motor function.
Locomotor activity test
Locomotor activity test was done using CoQ10 formulation in haloperidol challenged rats, and results are shown in Figure 9a. Haloperidol-induced locomotor activity was evaluated in Wistar albino rats by administering haloperidol at a dose of 2 mg/kg i.p. Haloperidol challenged group treated with CoQ10 nanoemulsion formulation (group D) showed significantly higher locomotor activity compared with the haloperidol challenged group (group B) (p < 0.001) and haloperidol challenged group treated with CoQ10 suspension (group C) (p < 0.001). The result demonstrated that the CoQ10 nanoemulsion (A10) showed greater therapeutic efficacy to improve locomotor activity than CoQ10 suspension.
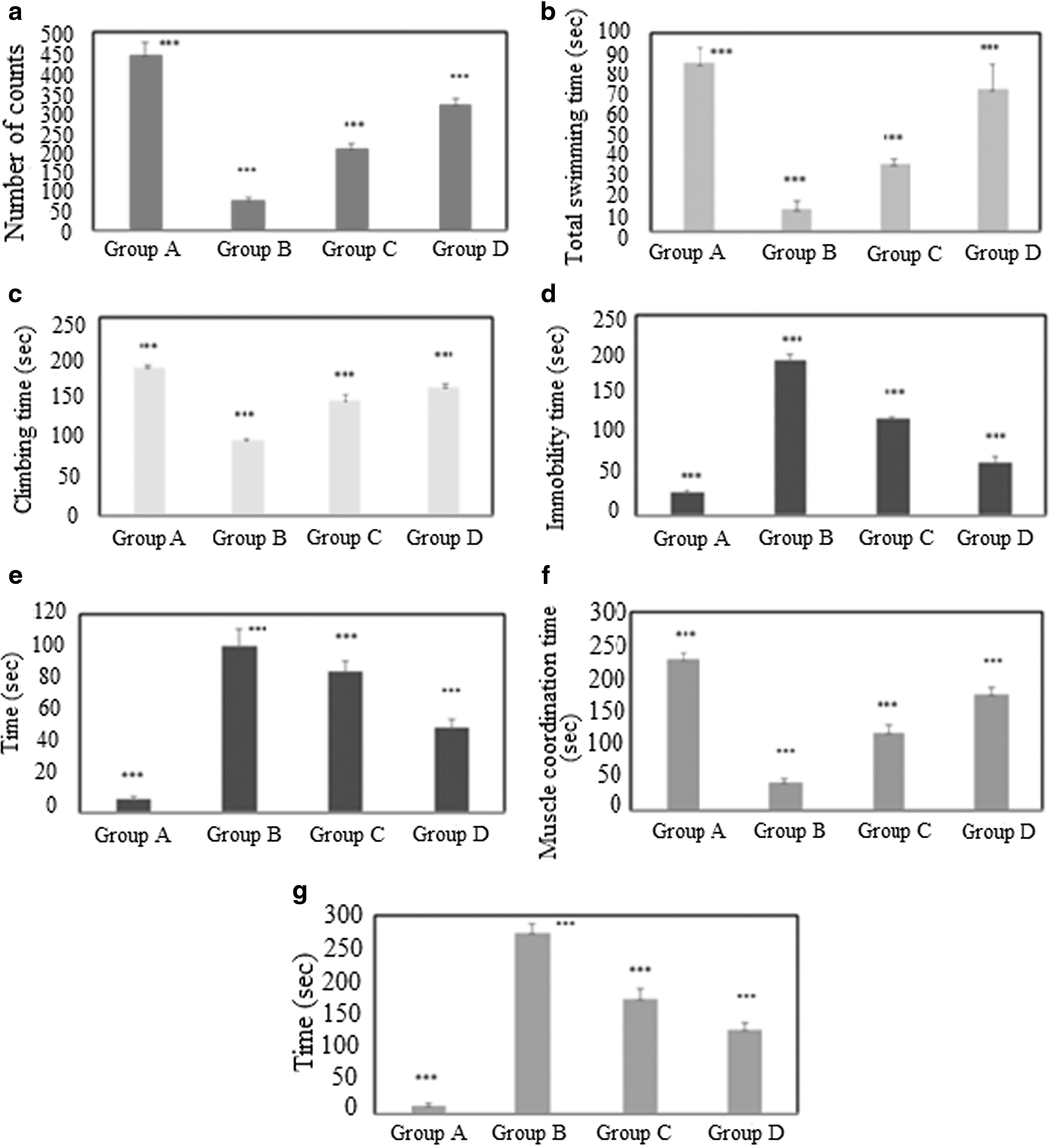
Pharmacodynamic behavior studies of Wistar albino rats
Forced swimming test
Forced swimming test was performed for 300 seconds in Wistar rats as shown in Figure 9b–d. Saline group (group A) showed swimming, climbing, and immobility behavior for 85.00 ± 7.87, 187.00 ± 3.51, and 28.00 ± 2.08 seconds, respectively, while haloperidol challenged group (group B) showed very insignificant behavior of swimming, climbing, and immobility for 11.00 ± 4.31, 95.50 ± 2.08, and 194.00 ± 7.93 seconds, respectively (Fig. 9b–d). Haloperidol challenged group rats treated with CoQ10 suspension (group C) showed swimming, climbing, and immobility behavior for 34.00 ± 2.53, 145.00 ± 6.74, and 121.00 ± 1.85, whereas group D showed swimming, climbing, and immobility for 72.00 ± 12.42, 162.00 ± 4.89, and 66.00 ± 7.82 seconds, respectively. Swimming and climbing time were increased in group D compared to group C, but immobility was decreased in group D compared to group C which was found to be statistically significant (p < 0.001).
Catalepsy
As shown in Figure 9e haloperidol challenged group treated with CoQ10 suspension (group C) showed significant (p < 0.001) improvement in cataleptic behavior in comparison to saline group (group A). Haloperidol challenged group treated with CoQ10 nanoemulsion formulation (group D) showed least cataleptic behavior compared to saline group (group A). The result demonstrated the maximum attenuation of cataleptic behavior after administration of nanoemulsion (p < 0.001).
Rotarod (muscle coordination test)
Animals in haloperidol challenged group (group B) showed a significant depletion in muscle coordination (p < 0.001) compared to the saline group (group A). Muscular coordination was increased in haloperidol challenged group treated with CoQ10 nanoemulsion formulation (group D) compared to haloperidol challenged group treated with CoQ10 suspension (group C). The maximum muscular coordination was found in the group A. The result demonstrated the effectiveness of CoQ10 nanoemulsion formulation to reverse muscle coordination in Parkinson's induced rats as shown in Figure 9f.
Akinesia test
Haloperidol challenged group (group B) showed the inability to move due to akinesia for 273.33 ± 15.38 seconds (Fig. 9g). Rats treated with haloperidol challenged group treated with CoQ10 suspension (group C) and haloperidol challenged group treated with CoQ10 nanoemulsion formulation (group D) showed akinesia score for 173.33 ± 15.38 and 127.50 ± 9.35 seconds, respectively, which were found to be statistically significant (p < 0.001). The least akinesia score was shown by saline group (group A). The results demonstrated a sharp decrease in akinesia score after treatment with CoQ10 nanoemulsion formulation A10, thereby demonstrating efficacy of formulation in treatment of Parkinson's disease. Data were subjected to ANOVA followed by Tukey–Kramer test (p vs. L), and values are expressed as mean ± standard deviation. ***p < 0.001 versus L represents the statistical analysis.
CoQ10 nanoemulsion administered orally elicited improved motor and behavioral activity in haloperidol challenged rats; hence there was improvement in locomotor activity, muscle coordination, climbing, and swimming time, and there was reduction in cataleptic and akinesia symptoms. We report in this study an appreciably more rapid improvement in behavioral activity due to restoration of dopamine following treatment with CoQ10 nanoemulsion. This is likely due to the fact that CoQ10 rapidly got absorbed and reached to brain more quickly than suspension. Nanoemulsion showed more drug permeation through the GIT membrane. Small droplets of nanoemulsion presents more surface area for the interaction between the drug and the cells, thus more amount of drug uptake through the membrane. Small droplet size and high lipophilicity of nanoemulsion make it easy to enter into systemic circulation. These findings demonstrate that nanoemulsion could be a promising drug delivery carrier for oral delivery of CoQ10 for better management of Parkinson's disease.
Biochemical estimation
GSH estimation
Saline group (group A) showed GSH concentration of 1474.76 ± 206.58 nM/mg of protein in brain tissues (Table 8). Concentration of GSH in haloperidol challenged group (group B) found to be 875.87 ± 23.81 nM/mg of protein in brain tissues was significantly lower compared to saline group (group A) (## p < 0.01). GSH concentration of haloperidol challenged group treated with CoQ10 suspension (group C) was found to be 1096.06 ± 34.44 nM/mg of protein in brain tissues, which was statistically not significant compared with haloperidol challenged group (group B) (## p > 0.05). GSH concentration in haloperidol challenged group treated with CoQ10 nanoemulsion formulation (group D) (1379.35 ± 339.76) showed significantly higher GSH level compared to Group B (## p < 0.01), whereas it also showed significant results in group A.
TBARS, thiobarbituric acid reactive substances.
TBARS estimation
MDA content in saline group (group A) was 155.78 ± 10.83 nM/mg of protein (Table 8). Haloperidol challenged group (group B) showed the highly significant increase (1024.76 ± 65.73 nM/mg of protein) in MDA content compared to group A (## p < 0.01). Small decrease in MDA content was observed in rats treated with haloperidol challenged group treated with CoQ10 suspension (group C) (791.65 ± 44.18 nM/mg of protein), which showed highly significant results among each other (## p < 0.01) and were also found significant compared to haloperidol challenged group treated with CoQ10 nanoemulsion formulation (group D). However, group D showed significantly lower MDA content (451.54 ± 58.64 nM/mg of protein) compared to group B (p < 0.01). When group A was compared with group B, C, and D, it was found to be highly significant (**p < 0.01) with each other.
Lipids and proteins, the major structural and functional components of the cell membrane, are the target of oxidative modification by free radicals in Parkinson's disease. Brain tissues are exposed to free radicals generated by oxidative metabolism, and in various diseases, endogenous defense mechanisms against free radicals may be weakened and/or overwhelmed, which can be effectively protected by the use of various antioxidants. Oxidative damage to dopaminergic neurons is believed to be one of the reasons of neurodegeneration in Parkinson's disease. The present work on the neuroprotective effect of CoQ10 on neuronal dysfunctions and biochemical alterations in rats demonstrated that CoQ10 nanoemulsion significantly reversed the behavioral deficits and biochemical alterations seen in brain. The reduced level of TBARS in brain of group D rats suggests reduction in the levels of lipid peroxidation. Moreover, there was a simultaneous increase in glutathione levels and antioxidant enzymes.
Histopathology of brain section
To study the degenerative effect of haloperidol and protective role of different formulations, histopathological examination was performed. Motic images software version 2.0 was used to collect the images. In negative control (normal brain, group A), all the neurons have round vesicular nuclei with prominent nucleoli. Moreover, there was amphiphilic cytoplasm (Fig. 10). In positive control group B, pronounced vacuolation and shrinkage of nuclei were observed with prominent histological degeneration. The CA1 region of haloperidol induced and CoQ10 suspension treated brain showed improvement in histological alterations with an increase in number of vesicular nuclei with prominent nucleoli and amphiphilic cytoplasm. Similarly, treatment with CoQ10 loaded nanoemulsion showed decrease in degenerative changes with large vesicular nuclei in most of the neurons. The brain tissues of this group showed few numbers of eosinophilic lesions compared to positive control group.
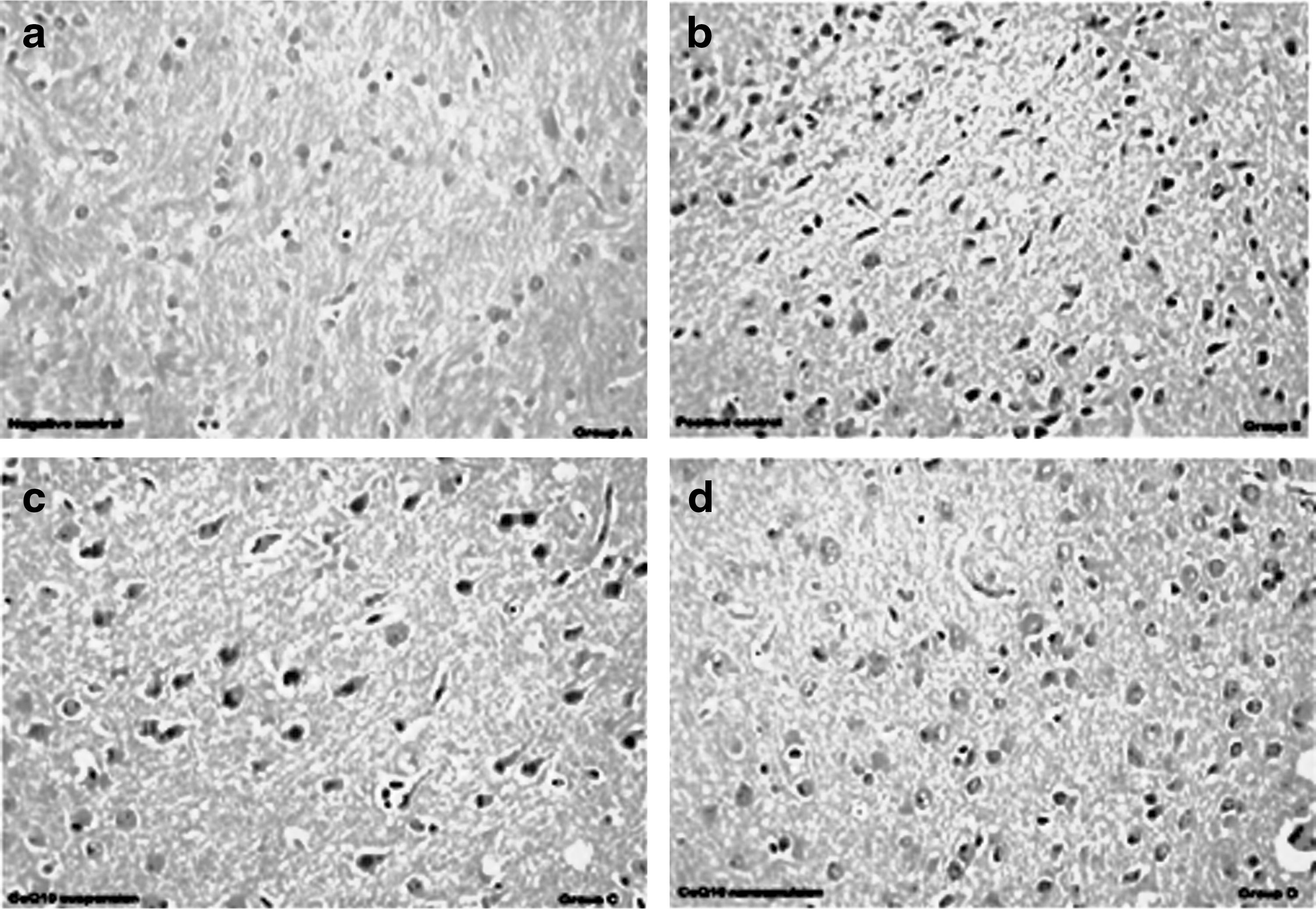
Brain section of
Conclusion
CoQ10 loaded nanoemulsion was formulated by spontaneous emulsification method in an attempt to increase its solubility and oral bioavailability. The CoQ10 loaded nanoemulsion formulation showed significant improvement in solubility, in vitro release, and antioxidant activity compared to CoQ10 suspension. In ex vivo permeation study, enhancement ratio of optimized formulation was found to be 1.75-fold higher than the CoQ10 suspension. The in vivo study in Wistar albino rats gave significantly higher AUC, Cmax and was found to be 1.82-fold higher than CoQ10 suspension. During pharmacodynamic studies, haloperidol challenged group treated with CoQ10 nanoemulsion exhibited significantly higher locomotor activity, improved muscular coordination, decreased cataleptic behavior, decreased akinesia, and significant reversal of swimming disability compared to CoQ10 suspension. In biochemical estimation, CoQ10 nanoemulsion treated rats showed significantly lower MDA content compared to haloperidol treated rats and the concentration of GSH increases in CoQ10 nanoemulsion group compared to suspension group.
Footnotes
Acknowledgments
Authors are thankful to Mr. Sandeep and SAIF, AIIMS, New Delhi for carrying out TEM.
Author Disclosure Statement
No competing financial interests exist.