
Abstract
Thyroid disease, increasingly common among the general population, is also rising among the elderly, which, given that the global population is aging, constitutes a serious public health issue that needs to be urgently addressed. The most common thyroid disease in younger and older individuals alike is hypothyroidism, including subclinical (SCH) and overt disease. Since TSH tends to increase with age due to intrinsic changes of thyroid metabolism and the gradual resetting of the hypothalamic-pituitary-thyroid axis, the diagnosis of “true” hypothyroidism is challenging, another difficulty being distinguishing disease-specific from aging-associated clinical symptoms. Hypothyroidism in the elderly may cause or exacerbate macrocytic anemia, hypercholesterolemia and kidney dysfunction, therefore careful clinical and biochemical control is necessary. Meanwhile, as an increase of TSH in the old and very old has been associated with longevity, a resetting of the TSH normal range according to age is strongly required before any diagnosis is made and treatment is implemented. Levothyroxine, which remains the treatment of choice, should be initiated in the old at TSH>10 mIU/l, starting with 25 μg/daily followed by cautious upward titration. Recent data (the TRUST study) revealed that treatment of SCH in the elderly does not improve hypothyroid symptoms and the tiredness score when compared with a placebo group. Hyperthyroidism is associated with increased mortality in the aged, this dependent upon type and adequacy of treatment. Treatment should be seriously considered in older patients who have endogenous subclinical hyperthyroidism with a TSH between 0.1 and 0.4 mIU/L, with regular monitoring being strongly advised.
“…For age is opportunity no less than youth itself, though in another dress, and as the evening twilight fades away the sky is filled with stars, invisible by day.”
Morituri Salutamus, by Henry W. Longfellow, 1874
Introduction
A
According to the latest United Nations report on World Population Ageing, the number of persons aged 60 years and over is expected to grow by 56% between 2015 and 2030, the global population of older people will double by 2050 to 2.1 billion, while those aged 80 years and over, the oldest-old, are projected to triple in number and reach 434 million by 2050. 2 It is hence evident that a radical reorganization of public health and social structures is urgently required to maintain an optimal level of medical care for older populations worldwide and particularly for the most vulnerable and in need.
Thyroid diseases, which are common in the general population and usually present as chronic conditions, tend to peak in the elderly, with hypothyroidism being the most frequent endocrine disorder among the old. 3
The aim of this short report is to raise awareness not only as to the critical link between thyroid disease and aging but also concerning the importance of coordinated research to close gaps in our knowledge regarding timely intervention for treatment in the old and oldest-old through utilizing evidence-based policies. Due to the existence of certain dilemmas in the diagnosis of hypothyroidism and its treatment with levothyroxine, there will be special focus on hypothyroidism and subclinical hypothyroidism (SCH).
Aging Thyroid
Aging brings about various functional and morphological changes in the thyroid gland. For example, thyroid activity diminishes in the elderly due to local decrease in deioidinase I (DIO1) activity and to influences exerted by nutritive and environmental factors. 4,5 However, these thyroid changes occurring in old age come about in ways that are so subtle and varied that their treatment demands very special scrutiny and discernment. Meanwhile, certain changes in thyroid hormone homeostasis seem, in fact, to contribute to longevity. For example, the studies performed in a thyroid disease-free population of centenarian Ashkenazi Jews in 2009 by Atzmon et al. 6 demonstrated exceptional longevity among this group, and it has also been observed in a number of animal species that reduced thyroid function is often associated with increased longevity. In addition, calorie restriction also among the old has been reported to reduce thyroid hormone levels while extending life and improving health. 7
Serum thyrotropin-stimulating hormone (TSH) concentrations gradually increase in healthy aging, although thyroidal T4 secretion and free T4 (FT4) concentrations remain unchanged, while, in contrast, T4 degradation by outer ring deiodination decreases with age. 8 It has been observed that the pituitary set point of TSH feedback suppression is gradually reset in older people, although this becomes evident only in extreme senescence. Moreover, the fact that TSH nocturnal surge diminishes with increasing age also points to the presence of hypothalamic dysfunction in the elderly. 9
Of some interest is the recently reported effect of age on the anatomic position of the thyroid gland in the anterior neck. The distance between the thyroid gland and the sternal notch was observed to be significantly decreased in the 80+ age group compared with the 18–39 age group. 10 The position of the gland did not change significantly relative to anatomic landmarks in the head or neck; however, the trachea was angled more closely to the horizontal plane in elderly patients, a fact that should be carefully borne in mind when surgery is planned. 10
Hypothyroidism in the Elderly
Hypothyroidism is much more common in the elderly than in younger (30- to 40-year-old) patients, with autoimmune hypothyroidism being particularly prevalent. 11 Due to a number of factors, however, hypothyroidism among older persons is likely to remain undiagnosed. The disease has an insidious onset and progresses slowly over many years so that symptoms are frequently nonspecific, with the result that at present, one of every five women over the age of 65 has a higher than normal level of TSH without being aware of it. Moreover, symptoms of hypothyroidism such as fatigue, depression, forgetfulness, and sleeplessness may be overlooked by both patients and their physicians since it is difficult to determine whether these are merely signs of aging or indications of disease. Indeed, many older subjects prefer to leave such complaints untreated, feeling that they should be passively accepted as part of the process of aging: in either case, quality of life can be seriously affected. The situation involves, of course, much greater risk when hypothyroidism in this population manifests as macrocytic or normocytic anemia, carpal tunnel syndrome, or hypercholesterolemia, the latter condition being especially dangerous as hypothyroidism carries a risk for congestive heart failure. 12,13 There is thus a vital need for elderly persons who suffer from hypothyroidism to be scrupulously checked for high cholesterol levels. While the association of overt hypothyroidism with hypercholesterolemia is clear, the effects of LT4 treatment on lipids are controversial in patients with SCH. 14 Long-term T4 treatment leads to a reduction in total and low-density lipoprotein-cholesterol (LDL-C) measurements in patients over 55 years, but only in those receiving suppressive doses of T4. However, no significant difference in lipids is noted in those with normal serum TSH compared with non-T4-treated controls. 15 Additionally, older patients who present with hypercholesterolemia need to undergo regular thyroid evaluation to determine whether it is thyroid disease that is causing the high cholesterol levels and, if so, what is the degree of thyroid failure.
Meanwhile, a considerable number of the elderly population suffers from some form of mental illness (e.g., dementia or depression) and, again, whether this is due to, for instance, Alzheimer's, or (as is often the case) to thyroid disease is not immediately obvious. A meta-analysis demonstrated a relationship between subclinical hypothyroidism (SCH) and cognitive impairment only in patients younger than 75 years of age. 16 However, a comprehensive literature review did not clarify whether SCH results in mood and cognitive impairments in most older patients. 17 Additionally, of note, the elderly are more susceptible to adverse events if treatment is not promptly initiated, while, by contrast, they are also at more risk than the general population of varying levels of harm from treatment. Yet another confounder is the fact that symptoms of thyroid disease can vary greatly in the elderly according to whether hyperthyroidism or hypothyroidism is present. All the above factors mean that the diagnosis and management of thyroid disorders in older people require very special skill, knowledge, and perspicacity 18 since impaired thyroid function that is left unattended in old age is likely to result in disability, cognitive impairment, and shortened life expectancy. 19 This points to the need to focus particular attention on thyroid status among the elderly. 20
Diagnostic Dilemmas
While it is well established that TSH normally increases with age 21 and that human longevity is sometimes associated with increased serum TSH (as noted above), it has been shown in these studies that the longer life expectancy is related to a heritable phenotype characterized by raised serum TSH. 6 In this line of evidence, it was shown in the Leiden study that a lower family mortality history score of the parents of nonagenarian siblings was associated with higher serum TSH levels and lower FT4 as well as lower FT3 levels in nonagenarian siblings. 22 The data support the abovementioned observation that low thyroid activity in humans constitutes a heritable phenotype contributing to exceptional familial longevity.
Apart from these observations, there is some debate as to whether the elevated TSH levels typically noted in the elderly of the general population reflect an increased prevalence of hypothyroidism or represent a normal aspect of healthy aging, as TSH with age is frequently associated with a higher prevalence of metabolic syndrome-related disorders as well as nutritional and glycosylation changes. 23 For the achievement of a more secure diagnosis, a broader diagnostic approach should be undertaken that will include a detailed clinical picture while crucially taking into account thyroid autoantibodies and thyroid hormones. Serum TSH is negatively associated and serum FT4 is positively associated with age in populations with mild iodine deficiency, whereas an ongoing decrease of TSH and increase of FT4, respectively, are routinely observed following iodine supplementation. 23 It has been reported that among populations who have been exposed to different levels of iodine intake over the years and who now have adequate iodine status, there are nonetheless differences in thyroid function related to each age group, it is therefore being proposed that both the present and the historical iodine status of a population should be taken into account to accurately establish the reference limits of TSH and FT4. 24 Furthermore, since the TSH upper reference limit is often too low, especially in the elderly and in women (and more so in Caucasian than in black women)—this discrepancy possibly leading to unnecessary or even harmful therapy, it appears reasonable to define the reference range on the basis of age, race, gender, and amount of iodine intake while also considering the interindividual and intraindividual variability of TSH levels. 24 Finally, the fact that serum TSH and thyroid hormones exhibit a sizable amount of interindividual variability, with the intraindividual variability lying within a narrow range, highlights the need to individualize levothyroxine treatment in elderly patients with elevated TSH levels.
Levothyroxine Treatment
In the follow-up study to the Leiden 85-Plus Study of 87% of a 2-year birth cohort (1912–1914) in the municipality of Leiden, the Netherlands, 599 participants were followed from age 85 years through age 89 years. 25 Plasma levels of TSH and FT4 were not related to any disability, depressive symptoms, or impaired cognition at baseline or during follow-up, suggesting that high TSH in the oldest-old is not associated with adverse effects and may even sustain longevity. 25
Recently, the association between TSH and FT4 levels and mortality in hypothyroid patients was assessed in 611 patients aged 60–80 years treated with levothyroxine. 26 The study reported increased mortality in patients with median TSH levels of 5–10 IU/L, but no adverse effect was related to FT4 levels. The authors proposed that treatment should aim at achieving euthyroidism to improve survival. 26
A common condition among elderly people is SCH, which is defined as elevated serum TSH with normal circulating FT4. In 2012–2013, a multicenter randomized control studies (RCT) of levothyroxine treatment of SCH was launched. 27 It concerns a randomized, double-blind, placebo-controlled parallel-group trial that started with 50 μg daily of levothyroxine (25 μg in subjects <50 kg body weight or with known coronary heart disease) and involves titration of dosage in the active treatment group in accordance with the TSH level. 27 Recently, the results of the TRUST study were published. The study involved 737 adults of at least 65 years of age who had persistent SCH and serum TSH between 4.60 and 19.99 mIU/L. No difference was observed in the mean change at 1 year in the Hypothyroid Symptoms Score or in the Tiredness Score between the placebo and the LT4 groups. 28 It is thus evident that the results of this study, although of general interest, do not offer any additional data with regard to the effects of LT4 administration in elderly persons with SCH.
According to the American Thyroid Association guidelines for the treatment of hypothyroidism, levothyroxine remains the treatment of choice; however, in the old, and particularly in the older-old, a lower dose is required due to the decreased T4 metabolism and raised target serum TSH 29 (Fig. 1). Indeed, in a recent study examining various parameters affecting the TSH reference intervals, it was demonstrated that the 97.5% confidence interval for the upper limit of the reference interval increased from 6.45 to 7.55 mU/L with age, partially due to progressive increase in the nocturnal TSH surge. 30 Decision to treat should be made carefully on an individual basis and comorbidities and medication need to be taken into account. Treatment is recommended in patients <65 years old with confirmed TSH >5 mU/L, because of the risk of increased mortality without intervention, and in the old at TSH >7.5 mU/L. 31 SCH is associated with an elevated risk of coronary heart disease events and mortality, as well as heart failure events, in patients with high TSH and particularly when TSH levels are ≥10.0 mU/L. 32 In the very old and in centenarians, no TSH cutoff level exists; however, treatment can be considered at TSH >10 mIU/L and, once again, the decision should be strictly individualized (Fig. 1). In a recent survey to determine goal TSH when treating hypothyroidism in elderly patients, other factors, such as tremor and racing heartbeat, were observed as most influencing the desired target. 33 Since these symptoms may indicate overtreatment with levothyroxine replacement, it is clear that dose adjustment is required. Levothyroxine is considered the standard of care for treatment of hypothyroidism as it reverses the symptoms and modifies several signs. 34 In addition, levothyroxine treatment restores endothelial dysfunction, while it decreases various parameters, such as total and LDL-cholesterol, thereby diminishing the risk of arteriosclerosis (Fig. 2). Important factors to be reckoned with when prescribing dosage are already prescribed drugs for comorbidities and their possible interaction with other drugs, declining body mass, and metabolic clearance rate, as well as the slow progression of disease (Fig. 3).

Patients younger than 65 years old should be treated when TSH is confirmed at >5 mIU/L. Those older than 65 years should be treated when TSH is above 10 mIU/L, accompanied by implementation of a balanced and individualized approach. Treatment among the oldest-old (85 plus) should be determined on a case-to-case basis, taking into account comorbidities, medication, and general status. In these patients, treatment is tentatively indicated at a TSH close to or above 20 mIU/L. TSH, thyrotropin-stimulating hormone.
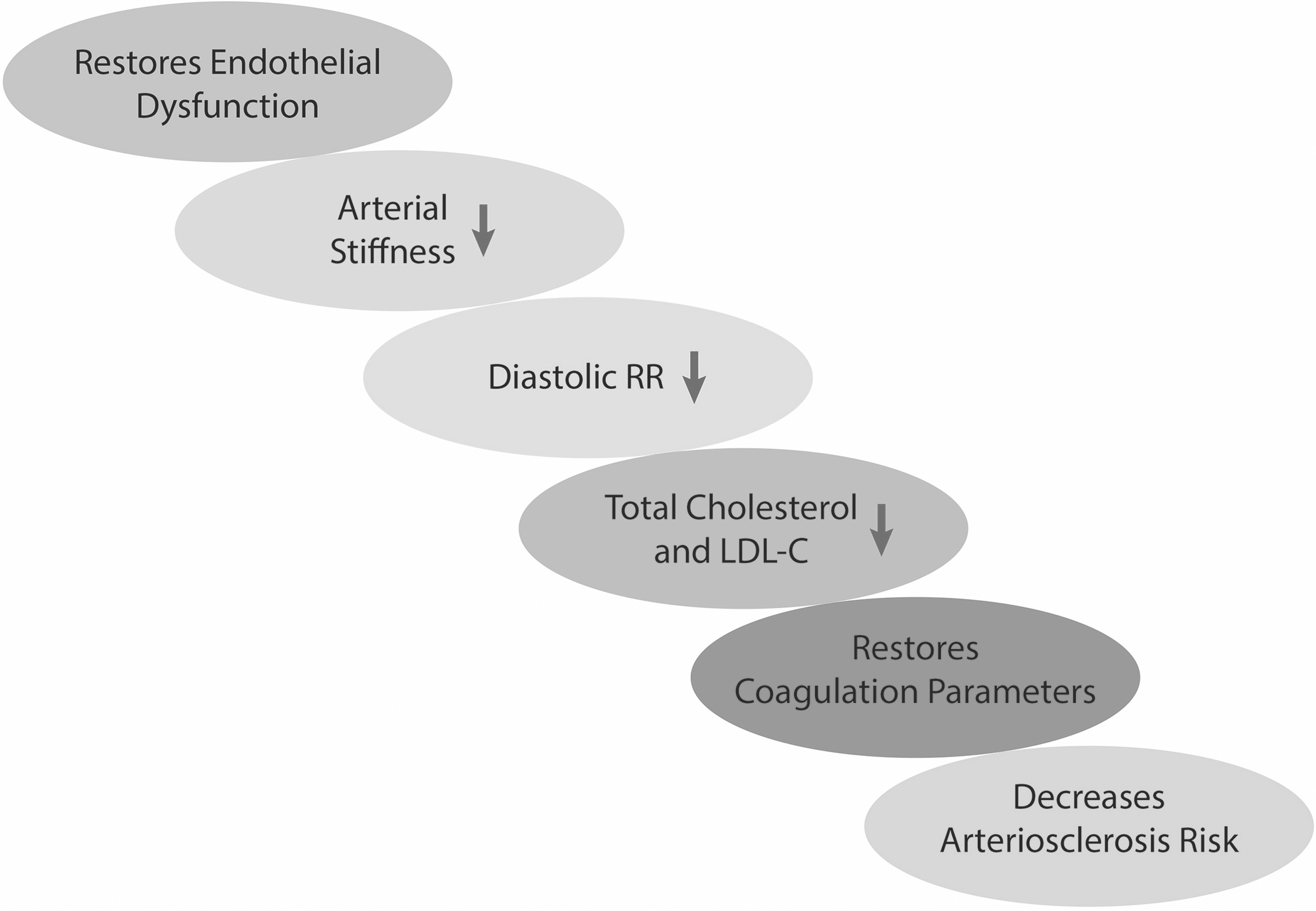
The various effects of levothyroxine in the treatment of hypothyroidism resulting in decreasing the arteriosclerotic risk. LDL-C, low-density lipoprotein-cholesterol.

The dosage of levothyroxine treatment should take into account decreasing body weight in the elderly and the decline of MCR, as well as frequently present comorbidities and comedications. MCR, metabolic clearance rate.
Treatment should be considered in patients with a TSH >10 mU/L, while in elderly patients with TSH <10 mU/L, an individualized approach is strongly recommended to abide by the ancient principle of “do no harm” (οφɛλέɛιν μη βλάπτɛιν).
While it is well established that replacement therapy is necessary for patients with overt hypothyroidism and whose blood TSH concentration is >10 mIU/L, it is also important to identify cases of transient hypothyroidism, a condition that does not call for lifelong treatment. Moreover, in those cases where TSH is only slightly increased, the risk of ascribing nonspecific symptoms to an abnormal laboratory result must be avoided, which might involve prescribing unnecessary treatment. A consensus among physicians as to the role of patient age in the management of hypothyroidism has not as yet been reached, thus the approach to adopt among the elderly who have elevated TSH is one of constant vigilance in lieu of the usual levothyroxine prescription.
Hyperthyroidism
Hyperthyroidism in the elderly is diagnosed in ∼15% of persons over the age of 60: it is mainly caused by toxic nodular goiter and is characterized by cardiovascular symptoms. 35 In a recent study aimed at establishing whether the increase in the prevalence of thyroid disorders continues beyond working age, it was shown that the frequency of morphological and functional thyroid changes did not further increase above the age of 65. 36
Overt and subclinical hyperthyroidism (SHyper) are associated with cardiovascular diseases, such as atrial fibrillation, atrial enlargement, and congestive heart failure, which are prevalent in patients >60 years, particularly in those with underlying cardiac disease, while an increased risk of stroke has been reported in patients >65 years of age with atrial fibrillation. 37 In a longitudinal study in community-dwelling men aged 70–89 years, baseline FT4 and TSH levels were assayed to examine the associations between the concentrations of FT4 and TSH and all-cause mortality in older men without thyroid disease. 38 FT4 level in the high-normal range (18.5–22 pmol/L) was associated with a higher mortality in comparison with FT4 levels in the middle range (11.5–15.0 pmol/L). In addition, TSH levels within the high-normal range (3.0–4.0 mIU/L) were also associated with higher mortality compared with TSH levels within the middle range (1.0–2.0 mIU/L). It is thus evident that the relationship between thyroid function and mortality varies according to age. 38
Two other crucial matters need to be borne in mind when dealing with hyperthyroidism among the old. First, it is established that since primary hyperthyroidism causes osteoporosis, regular bone mineral density scans are mandatory along with appropriate diet and exercise. 39 Second, persistent SHyper might be associated with increased depressive symptoms. That was demonstrated in the Leiden substudy of the Prospective Study of Pravastatin in the Elderly at Risk (PROSPER). 40 The aim was to assess thyroid functional status with depression as determined using the Geriatric Depression Scale 15 (GDS-15) at baseline and after 3 years. In contrast, the results on the association between subclinical thyroid diseases and cognition are conflicting. In a recent study seeking to assess the risk of dementia and cognitive decline associated with subclinical thyroid dysfunction, among 11 prospective cohorts that followed 16,805 participants during a median follow-up of 44.4 months, SHyper was associated with an elevated risk for dementia, while SCH was not. 41
It appears clear that the mortality typically associated with hyperthyroidism varies according to treatment. This fact was strongly indicated in a recent study showing that elevated all-cause mortality discernibly reflected a higher frequency of circulatory death in accordance with the person-years accumulated during treatment with thionamide, as well as following 131-I that was not associated with hypothyroidism. 42
Treatment in older patients with endogenous SHyper with a TSH between 0.1 and 0.4 mIU/L should be seriously considered due to the risk of increased mortality, even though progression to overt disease is rare (∼1% per year). 43 On the other hand, although not indicated by the guidelines, there is general agreement that the need for periodic monitoring of thyroid function in the elderly is highly advisable.
Conclusions and Some Thoughts
Due to the fact that both hypo- and hyperthyroidism often tend to be oligosymptomatic in the elderly, physicians need to regularly carry out clinical and biochemical analyses so as to establish a diagnosis and, if necessary, to promptly start appropriate treatment.
Healthy aging is strongly dependent on a constant euthyroid state since it is a well-functioning thyroid gland that enables the maintenance of homeostasis, this achieved through various mechanisms. For example, by directly acting upon membrane composition and modifying inflammatory responses, thyroid hormones support stem cell renewal as well as synchronization of physiological responses to light, which bring about antiaging effects. 44 There is, further, the hypothesis that limiting thyroid hormone signaling among certain age groups, and particularly during older age, may be beneficial for optimal aging. It is thus evident that such discerning management and judicious interventions may, indeed, aid the old and oldest-old to “see the sky filled with stars invisible by day.”
Footnotes
Author Disclosure Statement
No competing financial interests exist.