
Abstract
The aim of this study was to verify the effects of a high-intensity jump-based aquatic exercise (HIIAE) program on bone mass and functional fitness in postmenopausal women. We randomly assigned 25 women (65 ± 7 years) into two groups: Training group (T, n = 15) and Untrained group (Un, n = 10). The T group was submitted to 24 weeks of HIIAE program, where each session lasted for 30 minutes. The following parameters were assessed before and 6 months following the intervention: bone and physical fitness; lumbar spine (LS), total femur (TF), and whole body (WB) bone mineral density (BMD); agility (time up-and-go, TUG); and leg strength (chair stand test, CS). We observed a significant increase (p < 0.01) in LS, (Un: −0.88 ± 3.55, T: 3.71 ± 3.68; %), TF (Un: −1.38 ± 17.76, T: 6.52 ± 2.71; %), and WB (Un: 2.09 ± 3.17, T: 3.23 ± 4.18) BMD in the T group. Regarding functional fitness, the T group showed improvements in both TUG (before: 6.86 ± 1.24 vs. after: 6.22 ± 1.13 seconds; p < 0.05) and CS (before: 16 ± 4 vs. after: 19 ± 5 repetitions; p > 0.05) tests when compared with the U group's TUG (before: 5 ± 1, after: 6 ± 1 seconds; p < 0.05) and CS (before: 20 ± 2, after: 19 ± 2 repetitions; p > 0.05) scores. Our data suggest that a high-intensity, jump-based interval aquatic exercise program is able to improve BMD and functional fitness parameters in postmenopausal women.
Introduction
H
Among possible treatments suggested, engaging in regular physical exercise has been considered as an efficient nonpharmacological strategy to maintain 5 or increase 6 bone mineral density (BMD). As bone has been classified as a dynamic tissue, regular physical exercise affects bone tissue positively by promoting adaptations through various stimuli, mainly mechanical, which contribute to bone formation. 7 Thereby, resistance and impact-based physical exercise have been highlighted as major nonpharmacological strategies in the treatment of osteoporosis, influencing directly the preservation or improvement of bone mass and functional fitness. 8,9
Even though the effects of the mechanical stimuli resulting from physical exercises on bone tissue are quite clear, there are still doubts about the effectiveness of aquatic exercises on improving BMD in postmenopausal women. Performing motor activities inside an aquatic environment is made easier due to flotation and the inertia of the water, which decreases the mechanical action of friction with the ground on bone tissue. 8 Alternatively, the resistance promoted by water during movements may increase the muscular demand on the body segments recruited, promoting a higher osteogenic effect. 10,11
There are few studies 10,12 –15 available that utilized an aquatic environment as a tool to improve bone mass. Therefore, the aim of this study was to assess the effects of an aquatic jump-based physical training program on the BMD and the functional fitness of menopausal women.
Methods
Participants
We recruited 25 elderly women (aged 57–75 years) from the city of Natal, Brazil. We also searched for an aquatic fitness center as a possible venue to perform the experiment. We randomly assigned the subjects into two different groups: Training (T, n = 15) and Untrained (Un, n = 10). All participants were subjected to clinical examination and answered questionnaires regarding their medical history before being included in our study. Participants included in the study were women, 55 years of age or older, who were able to train three times per week during the 24 weeks of the exercise protocol.
Exclusion criteria included the following: participating in a regular and structured physical activity program for 3 months before experimentation; recent hospitalization; motor deficiency; symptomatic cardiorespiratory disease; noncontrolled hypertension or metabolic syndrome; severe renal or hepatic disease; cognitive impairment or debilitating conditions; marked obesity with inability to exercise; recent bone fracture (during the past 2 years); and participating in fewer than 90% of the sessions stipulated in the aquatic training program. Both Un and T groups were instructed to continue with their daily activity routines. However, only subjects in the T group participated in the aquatic training sessions. Participants were also required to maintain normal dietary intake (monitored by nutrition professional). Participants in the training group were asked not to perform any additional physical activity exercises during the study period. Additionally, all subjects were instructed to refrain from any medication that may affect bone metabolism. All participants read and signed the terms of consent following the Declaration of Helsinki before being included in the study.
Water-based exercise
The water-based exercise program consisted of 30-minute sessions thrice a week, over a 24 week period. Training sessions were performed on three different and nonconsecutive days in each week. The water level was fixed at xiphoid or near xiphoid level, with the temperature at 29°C. Each session was divided into three stages. The first stage consisted of 5 minutes warm-up, comprised of stretching and free movements in the water. The second stage comprised of jump-based (single-leg jump, ankle hops, tuck jumps, jump with hip abduction and adduction) exercises for 20 minutes, performed as high intensity interval exercise, consisting of 20 bouts for 30 seconds of all-out intensity as identified in previous studies by our group. 16 The intensity, although required to be maximal was self-selected by the subjects, who performed 30 seconds of passive recovery between sets. Intensity was monitored using the rating of perceived exertion. Finally, the third stage consisted of cooling-down/relaxation exercises for 5 minutes, composed of slow walking and stretching.
Evaluated parameters
We evaluated both groups prior and following 24 weeks of training. On the test day, participants were instructed to correctly follow the orientations postulated by the researchers. Body mass index (BMI = height/weight2) was assessed, and body fat percentage was calculated according to previous studies. 17,18 We used Dual-energy X-ray absorptiometry to scan lumbar spine (LS) (L1–L4), total femur (TF), and WB mineral density. All exams were analyzed by the same researcher using the DEA–DTX 200 Osteometer (MediTech), blind to subject condition.
Functional fitness
Functional fitness evaluation was composed of two tests used in previous studies to assess the physical performance parameters of mobility and balance in older adults. 17,18 We used the chair stand test (CS) test to evaluate lower limb strength, scored by the number of correctly executed stands within 30 seconds. We assessed agility through the timeup-and-go (TUG) test. The score was considered as the shortest time spent rising from a seated position, walking eight feet, turning back and returning to the seated position.
Statistical analysis
We analyzed comparisons between groups along the time periods using a two-way analysis of variance with repeated measures, followed by Bonferroni's post hoc test. Comparisons between groups concerning relative changes in variables after 24-weeks were performed using unpaired Student's t-test. The Cohen's d approach was used to calculate the effect size. Statistical analyses were performed with GraphPad Prism software (version 4.0, San Diego, CA). Statistical significance was set at p < 0.05.
Results
During the training period, no participants in either group left the study or presented any injuries as result of the exercise program. Before training, there were no significant differences between the groups for all assessed anthropometrics parameters (Tables 1, 2).
Anthropometrics Parameters for Both Groups Before and After 24 Weeks
Values are presented as mean ± standard deviation of Untrained and Trained groups. There were no differences in any of the parameters after the two-way analysis of variance with repeated measures, followed by Bonferroni's post hoc test.
BMI, body mass index.
Percent Change and Effect Size After 24 Weeks
Values are presented as mean ± standard deviation in the Untrained and Trained groups.
p < 0.01 Trained versus Untrained group.
Figure 1 shows the BMD parameters before and after 24 weeks of exercise protocol.
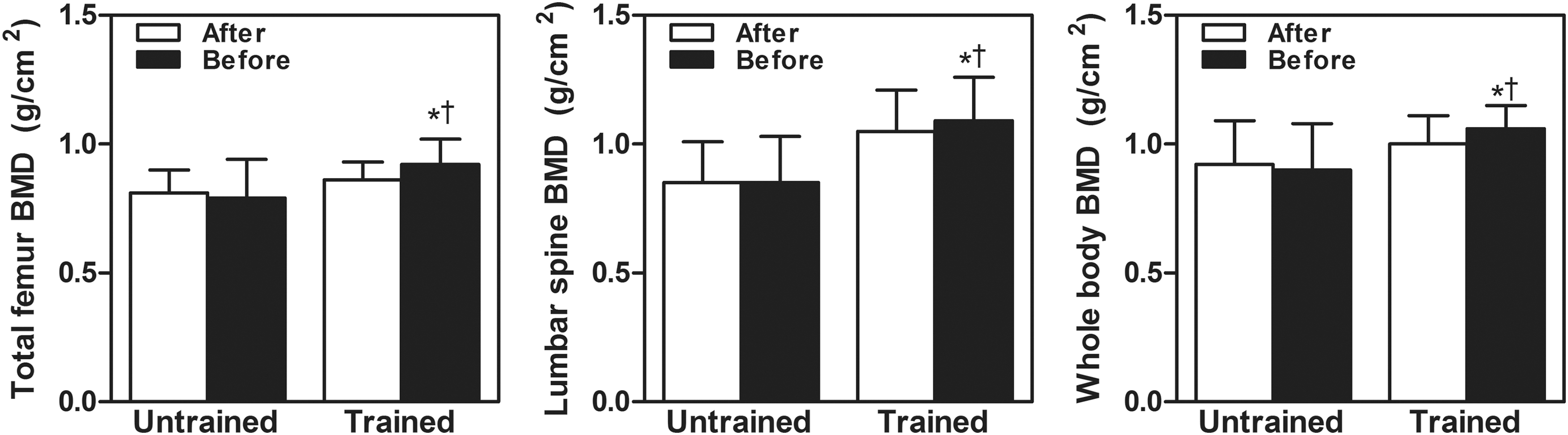
Levels of total femur, lumbar spine, and whole body BMD before and after the 24-week follow-up. *p < 0.001 before versus after. † p < 0.01 Trained versus Untrained group. BMD, bone mineral density.
The T group did not present significant (p > 0.05) reductions in TF (before: 0.881 ± 0.009 vs. after: 0.790 ± 0.15 g/cm2), LS (before: 0.850 ± 0.016 vs. after: 0.850 ± 0.018 g/cm2), and WB (before: 0.920 ± 0.017 vs. after: 0.900 ± 0.018 g/cm2) BMD. However, differences (p < 0.01) were found in the hip (before: 0.860 ± 0.070 vs. after: 1.040 ± 0.100 g/cm2), LS (before: 1.050 ± 0.016 vs. after: 1.090 ± 0.015 g/cm2), and WB (before: 1.000 ± 0.011 vs. after: 1.060 ± 0.009 g/cm2) BMD when compared with the Un group. Similar results were found at % change in all BMD parameters as showed in Table 2.
Regarding functional fitness (Fig. 2), we observed improvements of −11 ± 4% on the TUG test (before: 6.86 ± 1.24, after: 6.22 ± 1.13 seconds; p < 0.05) and 17 ± 3% on CS test (before: 16 ± 4, after: 19 ± 5 repetitions; p > 0.05) in the T group. We did not observe any changes (p < 0.05) on the TUG test (before: 5 ± 1 vs. after: 6 ± 1 seconds) or the CS test (before: 20 ± 2, after: 19 ± 2 repetitions) in the Un group.

Functional fitness of Untrained and Trained groups before and after the 24-week follow-up of jump-based exercise program. *p < 0.001 Trained versus Untrained group.
Discussion
Since flotation diminishes impact, aquatic exercises are typically classified as exercises of low osteogenic effect. However, the results from this study did not corroborate with this information. In our study, the protocol of all-out, jump-based impact exercises in water resulted in increased BMD and improved functional fitness in postmenopausal women.
Over the lifespan, environmental factors, such as mechanical loading, nutrition, hormonal and genetic factors, may influence body mass. 19 It is estimated from clinical studies that genetics correspond for between 60% to 80% of the variance of bone mass during a lifetime. 20 Nonetheless, according to Wolff's law, mechanical stimulus and loading magnitude are considered as active osteogenic stimuli. 21,22
Impact or resistance-based physical activities using muscle traction generally result in strain stress, compression, and shear stress when the bone is strained by many different loadings. 23 These loadings via the bone tissue are detected via mechanotransduction, which is the conversion of a mechanical force into a cellular response, generating more complex biochemical reactions in bone cells. 24 However, it should be highlighted that bone formation only occurs if the physical exercise stimulus exceeds a certain threshold, being capable of generating a loading above the usual everyday standard to which the body has adapted. 25 Indeed, longitudinal studies analyzing the influence of physical exercise on bone mass have demonstrated that active and resisted physical activities can stimulate bone mass in postmenopausal women. 26 –29
Additionally, the hydrodynamic effects of water in increasing resistance to movement, improving muscle and joint effort during walking, jumping, or moving body segments in an aquatic environment, are already recognized. 30,31 Some studies suggest 32,33 that, even with the predominance of impact exercises such as jumping, the effect of muscle action still helps to decrease impact on joints during landing on the ground. This may promote a response in bone cells that may stimulate osteogenesis, since muscular contraction stresses the tendon inserted in the bone, creating deformation that can spread through the fluid flow, activating the osteocytes contained in the canaliculi. 24
It is a consensus that muscle mass has a significant role in the acquisition and maintenance of bone structure, and increases in structure may explain the effects on BMD variance—from 6% to 16%, depending on the assessed bone site. Besides increasing BMD, muscular strength development also promotes improvement in motor coordination, postural stabilization, dynamic balance, and muscular strength, enabling physical autonomy and improving quality of life. 34 In addition to this, recruiting type II muscular fibers, which happens more often during high-intensity exercises, is more likely to stimulate bone tissue development. 35,36
Similarly, to the findings of Nolasco et al., 37 but in contrast to Takeshima et al., 38 the protocol we used in this study did not promote significant changes in body composition parameters. It is possible that this was influenced by the short duration of the training sessions, and the lack of any monitoring of the food intake of the participants. However, this exercise program was efficient in improving the muscular strength of the lower limbs and agility, and is in agreement with previous studies. 17,18,39 As such, our findings suggest that an aquatic exercise program based on high-intensity jumping may help to maintain body mass and improve muscular strength, both of which are parameters recognized as relevant to bone mass. 40 In addition, the findings also suggest that this type of activity maintains or promotes gains in body mass in elderly women.
In conclusion, we found that a high-intensity jump-based aquatic exercise program was efficient in improving bone mass and functional fitness in postmenopausal women. However, some limitations in the study were present, such as a relatively small sample size of a specific population, which does not allow for further generalizations. Therefore, future research in this area should consider the association between diet/dietary restriction, inflammatory cytokines, and assessing functional fitness parameters.
Footnotes
Author Disclosure Statement
No competing financial interests exist.