
Abstract
Studies of the effect of aromatherapy on patients with behavioral and psychological symptoms of dementia (BPSD) have yielded contradictory results. One possible explanation for this lack of consistent results is the site of application of the oil. The aim of the study was to evaluate the effect of lavender oil on the rate of BPSD when applied close to and away from the olfactory system. A crossover placebo-controlled study was conducted in the two psychogeriatric long term care departments. Patients in Department A received lavender oil on their face during the first month and on their foot in the second month, sunflower seed oil on their foot in the third month and on their face in the fourth month. Patients in Department B received sunflower seed oil on their face during the first month and on their foot in the second month, and lavender oil on their foot in the third month and on their face in the fourth month. Forty-two patients completed the study. Their mean age was 76.1 ± 11.2 years. After 4 months of treatment, the mean Neuropsychiatric Inventory score in Department A dropped from 13.1 ± 8.3 (median 12.0) to 3.5 ± 3.8 (median 2.0; p < 0.0001) and in Department B it dropped from 9.7 ± 9.6 (median 6.0) to 1.4 ± 2.5 (median 0; p < 0.0001). This reduction was not associated with the type of oil or the site of application. Based on these results, lavender oil has no advantage over sunflower seed oil in the reduction of BPSD, regardless of the place of application.
Introduction
The Consensus Conference from 1996 defined behavioral and psychological symptoms of dementia (BPSD) as “signs and symptoms of disturbed perception, thought content, mood or behavior that frequently occur in patients with dementia.” 1 The prevalence of BPSD is estimated at 75%, 2 –4 and 40% of patients suffer from more than three concomitant types of BPSD. 2 Signs of BPSD are associated with negative health outcomes, including functional decline, 5,6 increased duration of hospitalization, 7 placement in nursing homes, 5 –9 caregiver burden, 6 increased costs, 10 and even increased mortality rates. 9 –11
Neuroleptic drugs are often first-line treatment for BPSD 12 despite evidence for their adverse effects (pneumonia, cerebrovascular accidents, cardiac arrhythmias, negative metabolic, and peripheral vascular effects), increased mortality,13,14 and very limited evidence for their effectiveness. Over the past decade, there has been a growing trend for the use of complementary and alternative medicine, 15 including aromatherapy, 16 –28 to reduce the use of neuroleptic drugs in the treatment of BPSD.
The results of studies of aromatherapy for the treatment of BPSD are not conclusive as some had positive results, 16,19,20,23,26,28 some had negative results, 17,18,22,25 and others had mixed results. 21,24
In a descriptive analysis of six randomized controlled trials, 29 we hypothesized that the difference in the study results could not be explained by differences in the type of study population, in the type of active ingredient (Melissa or Lavender), or in the duration of treatment, but rather in the method of application used. When the aromatic oil was applied close to the olfactory system, the results of the studies were positive. In light of this, we conducted a crossover placebo-controlled study designed to answer two questions: does treatment with the aromatic lavender oil (Lavandula angustifolia) reduce the rates of BPSD and does the application of aromatic oil closer to the olfactory system reduce BPSD to a greater degree than its application at other anatomic sites.
Methods
Participants
The study was conducted from August to December 2017. The participants were recruited from the patients hospitalized in two psychogeriatric long term care departments at the Center for Mental Health of the Israel Ministry of Health for patients with dementia in Beer-Sheva. Twenty-five patients were hospitalized in each department. They were treated by a multidisciplinary team comprising doctors, nurses, occupational therapists, physical therapists, social workers, and a dietitian. The two departments are in the same building with separate entrances and each department has an automatic air conditioning system. The facility environment and the staff models of care are similar for the two departments. The two departments are directed by the same doctor (S.Z.).
All patients over the age of 18 years with a diagnosis of dementia of any type were included in the study. Exclusion criteria included patients with known sensitivity to lavender oil. Written informed consent was obtained from the patients' guardians. The study was approved by the ethics committee of Soroka University Medical Center (reference: 5244) and has the
Interventions
We used lavender oil as the active agent and sunflower seed oil as the placebo. The latter has been shown in the past to have a neutral effect on BPSD. 20 Since the active agent has a strong unique smell, there was no way, in our opinion, to guarantee masking of the department staff or the patients. To separate the patients in the treatment arm from the patients in the placebo arm as much as possible, we decided to begin to start with the lavender oil for all the patients in Department A and the placebo oil in all patients in Department B with a crossover design between the arms. The intervention protocol is given in Table 1.
Monthly Allocation of Active Drug or Placebo, by Department
Lavender or placebo oil was applied by the nurses on duty in the two departments three times a day, about 1 hour after breakfast, in the afternoon and in the evening. Two drops of oil were applied with an applicator on the skin of the face or the foot, in accordance with the group and the intervention phase. The application process did not last more than 1–2 minutes, including approaching the patient, providing an explanation, and the application itself (including removal of the socks, if necessary). The oil was applied to the face above the upper lip in the closest area to the olfactory system. It was applied to the dorsal part of one foot.
Aromatherapy oil
The oil of L. angustifolia was bought from the Israeli company “Light in the Desert” and was supplied in dark glass personal bottles each containing 30 mL. Based on the results of gas chromatography/mass spectrometry/flame ionization detector analysis, the oil contained 106 ingredients, of which 10 had a higher concentration: linalool (27.22%), linalyl acetate (31.75%), cis-β-ocimene (4.99%), terpinene-4-ol (4.46%), β-caryophyellene (3.53%), trans-β-ocimene (3.34%), E-β-farnesene (3.34%), lavandulyl acetate (3.26%), 3-octanone (1.82%), and lavandulol (1.39%). The bottles were stored according to the manufacturer's instructions in a cool place without exposure to direct sunrays.
Study instrument
We used the Neuropsychiatric Inventory (NPI) score. 30 Subjects were evaluated on 10 items (delusions, hallucinations, agitation/aggression, depression/dysphoria, anxiety, elation/euphoria, apathy/indifference, disinhibition, irritability/lability, and aberrant motor behavior). NPI scores are in the range 0–120 (with higher scores indicating greater BPSD severity).
The instrument was chosen since it was already in routine use in the departments that took part in the study. Despite this, a 2-hour workshop was conducted for the nurses to practice their use of the instrument. The assessments were conducted by two nurses (one in each department). The first assessment was conducted a week before the initiation of the intervention and the rest were conducted on a weekly basis throughout the intervention period.
The use of psychotropic drugs during the study
There were no limitations to drug therapy during the study, including psychotropic drugs. Every change in drugs was recorded in the patient's medical chart and was copied to the study chart. The defined daily dose (DDD) was calculated for the following drug groups: neuroleptics, mood stabilizers, benzodiazepines, and selective serotonin-reuptake inhibitors (SSRIs). For example, if a patient received diazepam at a dose of 5 mg/d, for the purpose of calculations, a DDD of 0.5 in the category of benzodiazepines was recorded. If they received olanzapine 2.5 ng/d, a DDD of 0.25 in the category of neuroleptics was used, and so on. To account for slight changes in daily dosages, we calculated a weekly cumulative DDD. For example, if the patient received 0.5 DDD of diltiazem, the cumulative weekly DDD would be 0.5 × 7 = 3.5.
Adverse event reports
Every report of adverse events (local irritation, local erythema, and allergic reaction to the active agent or placebo) was recorded immediately by the department nurses in the study chart. All serious adverse events were reported immediately to the Helsinki committee.
Sample size
The sample size calculation was based on a previous study by Ballard et al. 16 that tested the effectiveness of aromatherapy for agitated behavior among elderly patients. Based on the size effect, f = 0.52737, that was used in that study and originally reported by Fu et al. 18 and using the G*power a priori calculations for analysis of variance for repeat measurements, we calculated a sample size of 46 (23 in each group) with a power of 0.95 and α = 0.05.
Statistical analyses
The demographic and clinical characteristics of the two groups were compared using chi-square for categorical variables and t-tests for continuous variables. Changes in NPI scores were compared with the Friedman test by department over the study period. The differences in NPI scores for each patient were compared at four points in time: TI, the difference in NPI scores between the baseline score and at 4 weeks; T2, the difference in NPI scores between 4 and 8 weeks; T3, the difference in NPI scores between 8 and 12 weeks; T4, the difference in NPI scores between 12 and 16 weeks. We conducted a comparison of the median NPI score at the four points of time between the departments, using the Mann–Whitney U test. In a similar way, we calculated the differences in DDD for the introduction of an additional drug from the neuroleptics, mood stabilizers, and/or benzodiazepine groups. Statistical significance was set at p < 0.05 for all study analyses.
Results
Characteristics of the sample
Over the course of May and June 2017, we obtained signed informed consent from the legal guardians of the 50 patients in the two departments (25 in each). Three participants from Department A and five from Department B dropped out in the first month: two patients in Department A were transferred to another medical institute and one refused persistently to have the oil applied; three patients in Department B were transferred to another medical institute (one of whom passed away a few days after the transfer) and two refused persistently to have the oil applied. The transfer of patients to other institutes was not related to the study. All the dropouts occurred between 10 and 26 days from study initiation. In all, 42 patients completed the 4-month study and were included in the analyses.
The mean age of the patients was 76.1 ± 11.2 years (range 51–95). Twenty-four patients were women (57.2%). The mean Mini-Mental State Examination (MMSE) 31 score was 14.2 ± 8.7 and the mean Barthel Index (BI) 32 score was 13.3 ± 4.4 on a scale from 0 to 20. 33 The sociodemographic data and data on morbidity and medications for both groups are given in Table 2.
Study Population Characteristics, by Department
DDD, defined daily dose; MMSE, Mini-Mental State Examination; SD, standard deviation.
Treatment adherence
Over the course of the 4 intervention months, the adherence rate to treatment (completion of three applications of oil daily over the entire study period) was 96.4% ± 7.9%, without any difference between the groups.
Neuropsychiatric Inventory
The mean NPI score for the entire study population before the intervention was 11.5 ± 9.0 (median = 8.0, minimum = 0, maximum = 32), with a mean score of 13.1 ± 8.3 (12.0; 2–31) in Department A and 9.7 ± 9.6 (6.0; 0–32) in Department B (p = 0.234).
The mean NPI score decreased in both groups between the beginning and the end of the study (Fig. 1). In Department A, the mean score dropped to 3.5 ± 3.8 (median = 2.0; Freidman test: chi-square = 160.4, df = 16, p < 0.0001) and in Department B it dropped to 1.4 ± 2.5 (median = 2.0; Frideman test: chi-square = 142.2, df = 16, p < 0.0001). Table 3 gives the changes in NPI scores by month of treatment. The difference in NPI scores change reached statistical significance in the third month of treatment (T3) only. In that month, the patients in Department A received sunflower seed oil on their feet (a decrease in the median score of 2 points and the patients in Department B received lavender oil on their feet (no change in NPI score).
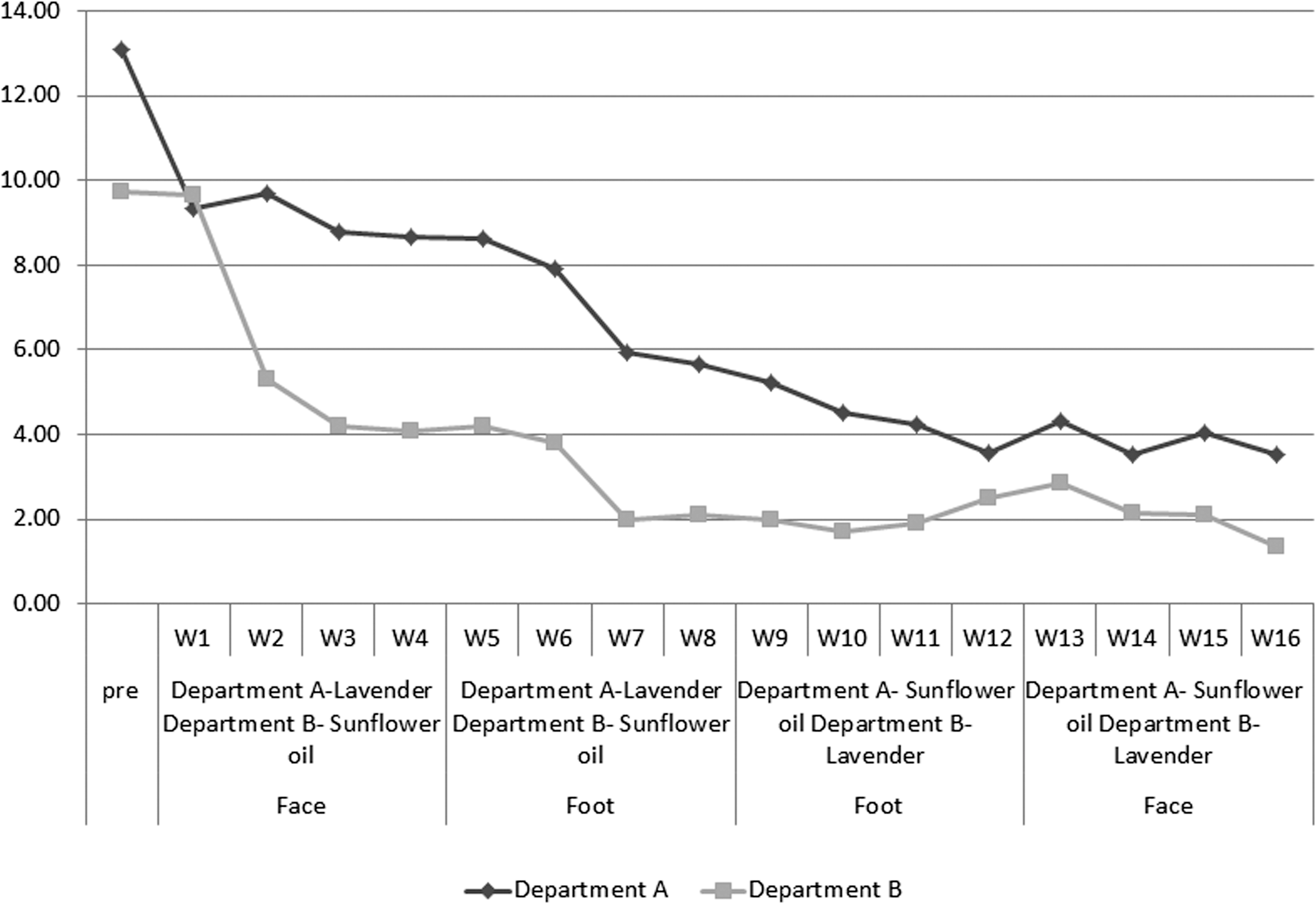
Changes in the mean NPI score by department. NPI, Neuropsychiatric Inventory.
Changes in the Median Neuropsychiatric Inventory Score, by Treatment and Department
MWU, Mann-Whitney U test; NPI, Neuropsychiatric Inventory; T1, difference between NPI scores at initiation of study and at 4 weeks of intervention; T2, difference between NPI scores 4 and 8 weeks of intervention; T3, difference between NPI scores 8 and 12 weeks of intervention; T4, difference between NPI scores 12 and 16 weeks of intervention.
Drug treatment
Before the start of the study, the patients in Department A received 1.9 ± 0.9 (2; 0–3) of all psychotropic drugs and the patients in Department B received 1.3 ± 0.9 (2; 0–2). There were no differences between the departments in the weekly cumulative DDD for any specific psychotropic drug, including neuroleptics, mood stabilizers, benzodiazepines, or SSRIs (Table 2). No changes in drug therapy took place during the course of the study, and there were no differences between the departments over time.
Adverse effects
One patient (Department B) had an exacerbation of chronic pulmonary disease while on placebo. She was hospitalized in an acute care hospital and died a few days later. The case was reported to the Helsinki committee. Other than this unfortunate case, there were 20 reported adverse events (Table 4).
Adverse Effects, by Treatment and Site of Application
Discussion
In this 16-week crossover study, there was no advantage to lavender oil over sunflower seed oil in reducing BPSD as measured by NPI score. Although the mean NPI score decreased significantly in both study groups, this decrease was not associated with the type of oil or the site of application. In effect, the greatest change in NPI scores occurred over the first weeks of the study regardless of whether the patients received the active agent or the placebo (Fig. 1). Furthermore, the only period in which there was a statistically significant decrease in the NPI score in one group (Department A) without a corresponding decrease in the other group (Department B) was when Department A received placebo on the foot and Department B received lavender oil on the foot (Table 3). Thus, the hypothesis that we generated from a previous study, 29 to the effect that application of oil closer to the olfactory system would be more effective than its application at a more distant site (the foot), was rejected by the results of this study.
There are several possible explanations for the negative results of the present study. First, it is possible that sunflower seed oil has therapeutic qualities, similar to lavender oil. This assumption is not reasonable since, in the past, when sunflower seed oil was used in a control group, it did not have a positive effect on BPSD. 20 Another more likely possibility is that we selected patients who were “too healthy” with a mean NPI score of 11.5 ± 9.0 and a median score of 8.0 before the intervention. In contrast, in previous studies that evaluated the effect of lavender oil on BPSD, the NPI score was higher. The study by Lin et al. included patients with a mean NPI score of 24 before the intervention. 20 In another study, the median NPI score was 54 in the intervention group and 33 in the control group. 26
Another possible explanation for the parallel decrease in NPI scores in the two groups is a change in the two departments that could have occurred during the study and was not related to the study itself, such as a change in treatment in the two departments (drugs or otherwise) or another significant systemic change. During the course of the study, there was no change in the staff members in the two departments or in their policies or approaches relating to nonpharmalogical treatment. The fact that there was no change in the use of psychotropic drugs throughout the course of the study, despite the significant decrease in NPI scores in the two groups, raises an interesting question that needs to be addressed. The rationale for the use of aromatherapy was as a potential alternative to treatment with psychotropic drugs. 15 If the department staff members had related to the change in NPI scores in the course of the study, it is possible that they would have reduced the use of psychotropic drugs at that stage. In the study by Lin et al., 20 despite the significant reduction of the NPI score by 7 points during treatment with the active agent, there was no change in the use of psychotropic drugs, so this may reflect a universal phenomenon of difficulty on the part of the staff to reduce drug therapy despite an improvement in BPSD.
There is another possible explanation for the results of the study. The only change that did occur in the two departments during the course of the study was the attention paid to the patients since a nurse approached the patient and touched him/her to apply the oils. So, additional time (no more than 6 minutes per day) was spent with the patients in the two departments.
Yang et al. 27 found that treatment with aroma-acupressure, for up to 15 minutes five times per week for 4 weeks, had a greater effect than aromatherapy when lavender oil was applied to the same sites, but without acupressure. Is it possible that the act of touching the patient for more time rather than the oil itself affects the results of the treatment? Burns et al. used Melissa as the active agent and sunflower seed oil for the placebo group. 17 The oil was massaged into the patients' hands for 1–2 minutes twice daily for 12 weeks. The investigators did not find any difference in BPSD, as measured by NPI score, with a decrease of 10 points in the placebo group and 7.2 points in the Mellisa oil group. The investigators explained the lack of advantage with Melissa oil by the element of touch and social interaction with a member of the care staff. They cited that “It is likely that these non-specific elements of the intervention … confer important benefits and probably explain the substantial improvements in the placebo group …. There are important implications for clinical practice regarding the impact of relatively simple interventions involving touch and interaction even though these may only last a couple of minutes a day.”
In a study by Maseda et al., 34 the effect of a multisensory stimulation such as a Snoezelen room was compared with one-to-one activity sessions such as playing cards, quizzes, or viewing photographs. The investigators found that both types of interventions were effective with regard to mood and behavior. The results of this study also highlight the importance of one-to-one interactions with therapists.
Previous studies of the effect of lavender oil on BSPD reported an absence of adverse effects. 6,20,27,35 As noted, one of the patients who received sunflower seed oil in the first month of the study suffered an exacerbation of chronic pulmonary disease and was hospitalized in an acute care hospital where she died. Several other isolated adverse effects were reported during the study, most of no significance except for one fall that did not result in injury. About a half of the adverse effects occurred on the same day, involving drowsiness in nine participants who had lavender oil applied on their foot. We have no explanation for this one-time occurrence, but it would not appear to be related to the study or the type of treatment. We find it difficult to explain why all the recorded adverse effects of lavender oil occurred in Department A only. The nursing staff member is similar in both departments and, as mentioned above, there were no changes in the treatment or nursing policy in either department that could explain the differences that were recorded in adverse effects in this study.
Strengths and limitations
This study has several advantages including the prospective crossover design that enabled us to compare the two types of oil at different times in the same population, the meticulous recording of psychotropic drugs that enabled us to rule out an effect of drug therapy on the results of the study, and the high adherence rate (over 95%) to the application of the oil that reduced the potential effect of adherence rates of the study results. The study continued for 16 weeks, which reduced the risk that a negative result could have been associated with a short-term exposure to the active agent.
The study also has limitations. The sample size calculation was based on a previous study 16 that used another measurement instrument, the Cohen-Mansfield Agitation Inventory 36 and not the NPI scores. We did this because we did not find any other published reports before the start of our study that used the NPI scores and reported the results in a way that would enable us to calculate the sample size. In fact, the NPI score in our study was lower than that in other studies that evaluated the effect of lavender oil on BPSD using NPI score as a baseline measure. 20,26 In addition, the planned sample size was 46 participants, 23 in each group, but only 42 completed the study. This limitation was caused by the small number of patients in the two departments and the fact that eight patients dropped out of the study at its inception. Since we were not able to continue to determine NPI scores in the patients who dropped out of the study, we were not able to do an intention-to-treat analysis.
The NPI score is a proxy measure, and for this reason it has several potential weaknesses, especially in the part that relates to issues that are not always manifested outwardly, for example, depression, anxiety, delusions, and hallucinations. In those cases, an external assessment is more likely to lead to a misdiagnosis than a direct response from the patient. In this study, we did not use any other self-administered instrument, for example, Patient Health Questionnaire 9 questions 37 for depression, so there is some likelihood that the severity of BPSD could have been underestimated. We think that in a future study, instruments such as NPI should be used in conjunction with self-administered questionnaires, at least in patients who are capable of completing them.
Another limitation is that we could not rule out misclassification of behavioral issues, which can also be related to indirect measurements such as BPSD where, for example, irritability could be misclassified as agitation. In contrast, this would not affect the overall NPI score. As already mentioned, the use of NPI is routine for the department staff and we provided additional training, so we believe that the study results were not affected by a less than optimal use of the instrument.
Another weakness of this study is the lack of follow-up after the treatment period. Did the NPI score go up or remain low? Were there changes in drug therapy in light of the decreased NPI score? Unfortunately, we cannot answer these important questions.
The absence of masking reduces the quality of this study, but it is important to note that lavender oil has a unique smell that makes it very difficult to design a study with masking. In the study by Sakamoto et al., 23 the investigators used an Aromaseal Lavender patch that was attached to the inner side of the patient's clothes. The investigators said that the odor was so gentle that only the patient with the patch could smell it. In the study by Burns et al., 17 in which the investigators used Melissa oil to maintain masking, the evaluator used nose clips. In this study, there was a strong persistent odor in the departments throughout the lavender treatment period. Furthermore, the study papers that were stored in the departments throughout the study continued to smell of lavender for at least 2 months after they were transferred from the departments to the research institute. Thus, we believe that masking was impossible for this study even if the evaluator who scored the NPI score entered the department with nasal clips. In this study, the treatment allocation was by department to minimize the effect of lavender on the participants at the time that they were receiving the placebo agent.
The lack of a washout period between treatments in our study is another weakness because we did not allot time to assess changes in BPSD after the intervention (lavender oil or placebo) and because the smell of lavender oil persisted for a long time in the department in which it was used. Another potential weakness in our study is that crossover designs can be problematic in patients with cognitive impairment, especially those with BPSD. Although these patients are potentially dynamic in terms of their BPSD as well as their willingness to participate in research, we did not observe any of these changes in this study.
In summary, in this crossover study, there was no advantage to the use of lavender oil, unrelated to the distance from the olfactory system, for the treatment of BPSD. In light of the many study design limitations, in this study there is a place for further research with a larger sample size that would test the assumption that it is not the oil itself that leads to the reduction in BPSD, but the investment of additional time and direct contact with the patient.
Footnotes
Acknowledgments
We thank all the nurses who participated in the study for their difficult and dedicated daily work. In particular, we would like to thank the head nurses in the two departments: Michal Shilo, RA, BA, and Maggi Absidris, RA, BA.
Author Disclosure Statement
No competing financial interests exist.