
Abstract
Physical exercise is a potential intervention to revert or attenuate frailty syndrome, which may be accomplished by traditional center-based and home-based programs. This study aimed to compare the effectiveness of a home-based and center-based exercise program on frailty status, physical and muscle function of frail older women. Thirty-one frail older women were allocated in two different groups: home-based group (n = 17, 71.5 ± 6.5 years) or center-based group (n = 14, 68.4 ± 6.4 years). The exercise program lasted 12 weeks (3 days/week), 60 minutes/session, including strengthening, balance, and gait exercises. Frailty status, knee, and hip strength, and physical function were assessed before and after the intervention. After the exercise program, frailty was reversed in 76% of the participants independently of the exercise group. Muscle strength and physical function improved in both groups, where the home-based program presented a high adherence rate, and the center-based program was more suitable to reverse the frailty status. In conclusion, a home-based exercise program is as effective as center based to improve strength, physical function, and to reverse frailty status.
Introduction
Frailty is a state of vulnerability to stressful events, resulting from reductions of morphological and physiological systems associated with the aging process. 1 Those reductions may present multiple causes, being determined by impairments on strength, resistance, and physiological functions. 2,3 Frailty is one of the main predictors of death and institutionalization, 4 increasing the susceptibility to illnesses, falls, physical inactivity, and functional decreases. 5 Whenever frailty is detected during the early stages (i.e., prefrail), it may be treated, aiming to prevent or even reverse the frailty status. 6
Physical exercise is an effective intervention to revert or attenuate frailty, restoring the independence of prefrail older adults and delaying the accumulation of functional deficits due to frailty progress. 7 Besides that, it highlights the importance of physical exercise programs focused on prefrail older adults, since without these preventive actions to maintain/recover the muscle strength, they may become even frailer and begin a downward spiral of accumulation of morbidity. 7 Evidence suggests that interventions through multicomponent physical exercise are recommended to promote muscular strength, balance, and physical function enhancements, which may be considered an effective alternative in traditional center-based and home-based programs. 8 –10 However, traditional center-based interventions may present a lower adherence rate to the exercise programs, mainly due to the dependence on family members or caregivers to bring the older adult to the training center. 11 Therefore, home-based programs have been considered a viable option for older populations.
Home-based exercises are a viable option and may be able to promote the independent training by the older adult, maintaining the training habits and facilitating the participation in exercise programs, mainly because there is no need to leave their homes, being possible to adequate the training to their routine. 10,11 However, the effect of home-based exercise in physical function is still contradictory, with studies showing similar results to traditional programs, 12 lower effects compared with traditional interventions, 11,13 and studies demonstrating a lack of effectiveness of home-based exercise. 14
Some factors may explain the variability of results in the home-based programs, where the control of frequency and intensity of physical exercise, often accomplished through phone calls and by the self-reported calendar, may influence the study outcomes. 11 These methods of control depend on a memory bias, and home-based programs should have an objective measurement to control the intensity and frequency of the exercise to guide the participants. Thus, it is necessary to investigate the effects of a higher accuracy degree in the control of exercise in home-based exercise interventions, including accelerometry, home visits, phone calls, and electronic messages frequently made by the exercise program supervisors.
Therefore, the study aimed to compare the effectiveness of a home-based multicomponent exercise program with a higher control degree to a traditional center-based program, analyzing the frailty status, muscle, and physical function in prefrail older women.
Materials and Methods
Study design and population
The study was a quasiexperiment clinical trial conducted in the Study Center of Motor Behavior at the Federal University of Paraná, Brazil, between April 2017 and June 2018, with two input blocks. The participants were placed by convenience into home-based exercise or group-based exercise to increase attendance and compliance. All pre- and postmeasurements and analyses were conducted by blinded testers that are not aware of the participants' group assignment. The Ethics Committee of the Federal University of Paraná approved this study (CAAE: 60950016.9.0000.0102), registered in the Brazilian Registry Clinical Trials Registry (No. RBR-825cgv), following the Consolidated Standards of Reporting Trials guidelines.
Volunteer recruitment was made in Curitiba Healthcare Units and through digital media, including local digital newspaper and Facebook. Those interested in participating were assessed for eligibility by an in-person screening visit based on the following inclusion criteria: women, 60 years of age or more, not engaged in regular physical activity in the previous 6 months, and prefrail based on Fried frailty phenotype. 1 The exclusion criteria were: neurologic disease, arrhythmia, physical restrictions to perform the tests and exercises, reduced cognitive capacity based on the Mini-Mental State Examination (MMSE) scores adjusted by educational profile, 15 and medical contraindications for participation in an exercise program. All the participants signed an informed consent form and were instructed not to start other structured physical activities during the study protocol.
The sample size calculation was done using the G*Power 3.1 software, and the following parameters were considered: (1) F test (analysis of variance [ANOVA]); (2) a 95% confidence level; (3) a sampling error of 5%; (4) power analysis of 85%; (5) number of groups = 2; (6) number of measures = 2 (pre- and postevaluation); and (7) addition of 10% margin for possible sample loss, totalizing an estimated sample size of 31 older adults.
Initially, 55 older women from the local community were recruited. After applying the inclusion and exclusion criteria, 31 women were allocated into 2 groups: home-based (HB) group (HB = 17; 71.5 ± 6.5 years, 68.9 ± 14.3 kg, 1.57 ± 0.05 m) and center-based (CB) group (CB = 14; 68.4 ± 6.4 years, 69.0 ± 9.9 kg, 1.56 ± 0.05 m). The process of recruitment and allocation is shown in Figure 1.
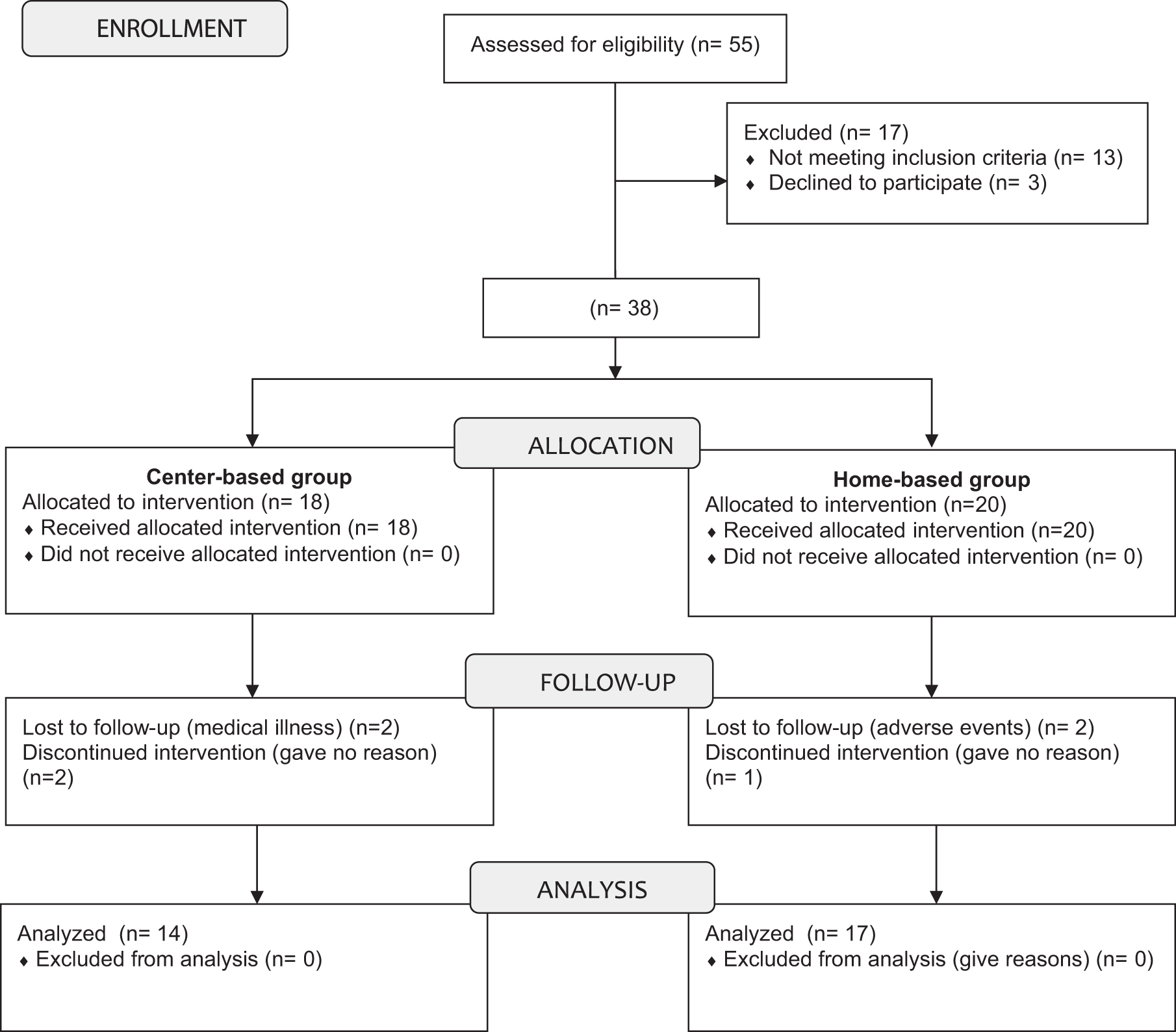
Schematic representation of participant recruitment and allocation.
Procedures
Participants attended two visits in nonconsecutive days to the laboratory. Trained evaluators administered the tests. In the first visit, they performed the following assessments: frailty phenotype, anthropometric measurements, physical function (timed-up-and-go test, the five times sit to stand test, and walking speed), and a familiarization session with the isokinetic dynamometer (Biodex Medical Systems, Inc., Shirley, NY) aiming to reduce possible learning effects. In the second visit, the participants performed the dominant lower limb isokinetic strength test and received activity monitors (accelerometers).
The prefrail status was verified when one or two criteria 1 were present: unintentional weight loss (4.5 kg in the past year), self-reported exhaustion, weakness (grip strength), slow walking speed, and low physical activity (Minnesota Leisure Activity Questionnaire 16 ).
Lower limb strength was tested in a Biodex Multi-Joint System 3 dynamometer. Participants were positioned following the Biodex manufacturer specifications. 17,18 The testing protocol included two sets of three repetitions of hip and knee concentric flexion/extension performed at 60°/s and 180°/s, with a 2-minute interval between sets. 19 Participants were verbally encouraged to exert the highest strength possible. Data were acquired at 1000 Hz, and all strength tests were analyzed using the Biodex System 3 Advantage software, version 3.2.
The physical function was assessed by a set of four tests accomplished in a standard order. Participants performed a familiarization trial for each test: five times sit to stand test in an armless chair with both hands crossed over the chest 20 ; timed up-and-go (TUG) test by walking 3 m and returning to a seated position using a usual gait speed 21 ; 4-m walk test (usual gait speed) 22 ; and 10-m walk test (maximum gait speed). 23
The intensity and the spent calories during the exercise sessions were assessed by an accelerometer (Actigraph, Model GT3X), wore by participants for 7 consecutive days in two different moments (baseline and 10th week). The participants were instructed to wear the device all day during those 7 days, taking it off only to sleep and water activities, including bathing. The accelerometer was attached to the ankle of the dominant leg above the lateral malleolus, and data were collected at 60 Hz. Data were analyzed when it included at least 10 hours/d for at least 4 days/period. Data of the average amount of calories spent per day/period were analyzed using the Actilife software. 24
Exercise program
The multicomponent exercise programs were conducted for 12 weeks, with three sessions of 60 minutes/week, following the recommendations of the American College of Sports Medicine 25 and the position standard of exercise prescription to reverse frailty. 7 The intervention groups performed similar exercise sessions that involved the lower limb strength and balance exercise, including gradual increases in the volume, intensity, and complexity of the exercises.
The exercise session included: a 10 minutes warm-up, 25 minutes for lower limb strength exercises, 15 minutes of dynamic balance exercises, and 10 minutes cool down. The lower limb strength was composed of 2–3 sets of 8–12 repetitions of the knee and hip flexion/extension, hip adduction/abduction, ankle dorsiflexion/plantarflexion, and glutes exercises with 60-second intervals between sets. The load adjustments were made when the subjects performed 8–12 repetitions without compensation or reaching fatigue using ankle cuff weights from 1 to 4 kg. The dynamic balance exercises were composed of single-leg, semi-tandem, and tandem stance, forward, backward, and lateral displacements, and plantar and dorsiflexion walk. The progression in balance exercise was made by decreasing the base of support, adding unstable surfaces, and closing the subject's eyes. Exercise intensity was assessed using the Borg Rating of Perceived Exertion (Borg scale 6–20), being gradually increased as the participants acclimated to the exercise. The exercise program had three intensity levels: weeks 1–4, the intensity of exercises was fairly light (11–12); weeks 5–8, the intensity was somewhat hard (13–14); weeks 9–12, the intensity was hard (15).
The HB group performed all individualized sessions at home. The CB group performed all supervised group sessions in a room at the Physical Education Department of the Federal University of Paraná conducted by physical educators and physiotherapists. Before the beginning of the exercise program, all the participants of the HB group underwent a home visit, where they received recommendations and demonstrations regarding the correct form to perform exercises safely. Besides the recommendations, the participants received ankle weights cuffs and a booklet with illustrations and instructions to reinforce execution of proper exercises. The booklet had an exercise log with day and time when the exercise was performed. Additionally, the HB group received visits every 2 weeks for load progression and electronic messages through WhatsApp Messenger (WhatsApp, Inc.) at training days as an incentive to perform the exercises.
The attendance rate was assessed based on attendance to the center-based sessions, and by weekly exercise logs for the home-based sessions. Moreover, the average calorie expenditure per day was recorded by the accelerometer at baseline and week 10 26 to analyze the exercise intensity. All participants had an attendance rate above 75%.
Statistical analyses
Descriptive statistics with mean and standard deviation were performed to characterize the groups. Data normality and homogeneity of variance were tested using the Kolmogorov–Smirnov and Levene tests. For comparison of initial characteristics, the independent t-test and the Mann–Whitney test were used. The logarithm transformation (log10) was performed when the data presented a non-normal distribution. Group comparisons before and after the intervention were performed using the ANOVA Mixed Models with Bonferroni post hoc test. Furthermore, the Pearson's correlation coefficient r was calculated to check the magnitude of the observed effects, considering r = 0.10 as a small effect, r = 0.30 as a medium effect, and r = 0.50 as a large effect size. 27 The significance level was set at p < 0.05, and the statistical procedures were performed in SPSS software, version 25.
Results
The initial characteristics of the participants are presented in Table 1. No significant differences were observed between groups before the intervention. There were no reports of adverse effects, such as falls, muscle soreness, injuries, or any other relevant problem related to the intervention. Exercise attendance rates were 87% for HB group and 77% for the CB group. After the intervention, there was a decrease in the frailty state prevalence in 11 older adults (65%) of HB group becoming robust, as well as 13 older adults (92%) of the CB group (Table 2).
Comparison of Initial Characteristics Between-Group Preintervention
Data presented as mean (standard deviation).
AB, abdominal circumference; BMI, body mass index; MMSE, Mini-Mental State Examination.
Classification of Frailty Status Before and After Completing a 12-Week Exercise Program
There were no significant differences in the average calorie expenditure per day between groups (HB vs. CB) at baseline (600 ± 270 vs. 705 ± 283 kcal/d) and at the week 10 (700 ± 291 vs. 849 ± 196 kcal/d). In the exercise session, it was observed a significant difference between groups in the sedentary time (p = 0.01), light activity time (p = 0.03), and very vigorous activity time (p = 0.01). The HB group spent more time in sedentary activity, and the CB group spent more time in light activity. In general, the HB group spent 54% of the exercise session in light and moderate activity, whereas the CB group spent 67% of the time in the same activity level. Details are present in Table 3.
Comparison of Caloric Expenditure and Time Spent (%) in the Three Sessions of Training in the 10th Week Between Groups
Data presented as mean (standard deviation).
Significant intergroup difference.
Muscle power of knee flexors increased in the CB group from 24.9 ± 4.7 W preintervention to 28.4 ± 5.4 W postintervention [F (1,29) = 4.4, p < 0.046, r = 0.36] at 60°/s and from 39.2 ± 7.1 W preintervention to 43.8 ± 8.4 W postintervention [F (1,29) = 4.2, p < 0.05, r = 0.36] at 180°/s with medium effect size. The muscle power of knee flexors increased in the HB group from 39.1 ± 9.4 W preintervention to 44.3 ± 13.5 W postintervention [F (1,29) = 6.3, p < 0.018, r = 0.42] and the total work from 182.3 ± 58.4 J preintervention to 209.3 ± 77.2 J postintervention [F (1,29) = 4.8, p < 0.036, r = 0.38] at 180°/s, both with medium effect size (Table 4).
Muscle Function Analysis of the Knee Extension and Flexion Movements in 60°/s and 180°/s Angular Velocities at Pre- and Postintervention
Data presented as mean (standard deviation).
Significant intragroup difference (from pre- to postintervention instants).
Significant intergroup difference (postintervention instant).
CB, center-based; EXT, knee extension; FLEX, knee flexion; HB, home-based; POw, muscle power; PT, peak torque; PT/BM, peak torque normalized by body mass; r, effect size; TT, total work.
Muscle power of hip flexors increased at 60°/s in both groups, where the HB group increased from 45.3 ± 16.7 W preintervention to 51.5 ± 16.5 W postintervention [HB group: F (1,29) = 6.1 p < 0.02, r = 0.42] and the CB group increased from 46.8 ± 11.6 W preintervention to 53.6 ± 8.4 W postintervention [CB group: F (1,29) = 6.1, p < 0.02, r = 0.42] with medium effect size. Muscle power increased for the hip extensors from 91.2 ± 23.8 W preintervention to 104.9 ± 27.3 W postintervention [F (1,29) = 9.2, p < 0.005, r = 0.49] and total work from 193.6 ± 49.7 J preintervention to 220 ± 58.3 J postintervention [F (1,29) = 5.6, p < 0.025, r = 0.40] at 60°/s with medium effect size.
Muscle power of hip extensors increased in the HB group from 44.5 ± 47 W preintervention to 62.1 ± 59.6 W postintervention [F (1,29) = 10.3, p < 0.003, r = 0.51] and the CB group from 36.6 ± 33.05 W preintervention to 39.3 ± 21.2 W postintervention [F (1,29) = 5.7, p < 0.024, r = 0.41] at 180°/s. The total work of hip extensors increased in the HB group from 93.6 ± 104.6 J preintervention to 126.1 ± 124.2 J postintervention [F (1,29) = 9.9, p < 0.004, r = 0.50] and in CB group from 69.5 ± 62.5 J preintervention to 77.3 ± 44.1 J postintervention [F (1,29) = 5.5, p < 0.026, r = 0.40] at 180°/s. The HB group increased the peak torque/body weight at 180°/s for the hip flexors from 0.69 ± 0.18 N·m/kg preintervention to 0.79 ± 0.26 N·m/kg postintervention [F (1,29) = 6.4, p < 0.017, r = 0.43] with medium effect size. The CB group increased muscle power of hip flexors at 180°/s from 65.1 ± 16.1 W preintervention to 78.7 ± 11.6 W postintervention [F (1,29) = 4.2, p < 0.05, r = 0.36] with medium effect size (Table 5).
Muscle Function Analysis of the Hip Extension and Flexion Movements in 60°/s and 180°/s Angular Velocities at Pre- and Postintervention
Data presented as mean (standard deviation).
Significant intragroup difference (from pre- to postintervention instants).
Significant intergroup difference (postintervention instant).
Both groups presented decreased in the time to complete a 4-m usual walk, where the HB group reduced the time from 4.17 ± 1.06 seconds preintervention to 3.43 ± 0.53 seconds postintervention [F (1,29) = 18.1, p < 0.01, r = 0.62] and the CB group from 3.51 ± 0.72 seconds preintervention to 3.05 ± 0.47 postintervention [F (1,29) = 5.6, p < 0.0246 r = 0.39]. In the 10-m maximum walk the HB group decreased from 7.6 ± 2.14 preintervention to 6.6 ± 1.8 postintervention [F (1,29) = 20.1, p = 0.01, r = 0.64] and the CB group from 7.28 ± 1.33 preintervention to 6.4 ± 0.72 postintervention [F (1,29) = 11, p < 0.002, r = 0.52]. In the five sit to stand test, the HB group reduced from 12.9 ± 3.5 seconds preintervention to 11.11 ± 2.2 seconds postintervention [F (1,29) = 7.2, p = 0.012, r = 0.45] and the CB group from 11.46 ± 3.5 seconds preintervention to 11.11 ± 2.2 seconds postintervention [F (1,29) = 9.9, p < 0.004, r = 0.50] (Table 6).
Physical Function at Pre- and Postintervention in the Home-Based and Center-Based Groups
Data presented as mean (standard deviation).
Significant intragroup difference (from pre- to postintervention instants).
TUG, timed up-and-go.
Discussion
The purpose of the present study was to compare the effectiveness of a home-based versus center-based exercise program on frailty status, physical function, and muscle strength of prefrail older women. The main finding was that both groups reversed the frailty status, enhanced muscle strength, and physical function after the training program. However, the CB exercise group had higher rates of reversal of frailty status, whereas the HB exercise group exhibited a more noticeable increase for muscle power.
Regarding the state of frailty, there was an average reversal rate of 76%, which indicates that both application modalities of the exercise program were effective. More specifically, there was a 92% and 65% reversal rate of frailty status for CB and HB groups, respectively. These results are consistent with those found in the literature, such as in Faber et al. (2006), 28 indicating that older people who participated in a 20-week multicomponent exercise program were less likely to progress in their state of frailty and reduced their risk of becoming frail by 61%. In the same way, Gill et al. (2002) 29 obtained similar results with a 6-month home-based exercise program.
Physical exercise is recognized as one of the best interventions to modify the frail status among older adults and should involve multicomponent exercises. 7 The reason behind that relies on the fact that frailty affects concurrently multiple physiological systems, and the application of different types of physical exercise allows older adults to increase their residual physiological reserves to overcome any physical deficits. 7,30
Exercise has also been proposed to improve physical and muscle function in frail older adults. In the present study, improvements in the knee flexor muscle power at 60°/s and 180°/s were observed in the CB group, while the HB group increased the knee flexor muscle power and total work at 180°/s. Similar results were found for hip flexor and extensor muscles in both groups, with effects more pronounced in the HB group at 60°/s. These findings are consistent with the literature, where Opdenacker et al. found an increase in the muscle strength of hip flexors and extensors in home-based exercise and center-based exercise. 31
These findings are relevant since hip and knee muscle groups are essential for performing daily activities, such as walking, climbing, and descending stairs, and sitting and rising from a chair. 32 Hortobágyi et al. found that older adult performs a higher relative force for their daily tasks compared with young adults, using 78%–88% of the maximum strength to climbing and descending stairs and to stand off a chair, respectively. It is known that small increases in muscle strength in frail older adults will provide functional improvements, and is one of most important valences that contribute to the physical function of older adults. 33
In the present study, increases in muscle strength may have contributed to improved physical function. These findings are showed in the decrease of the time to sit to stand up from a chair, 4- and 10-m walk by 6%, 22%, and 15% in the HB group and 3%, 15%, and 13% in the CB group, respectively. Thus, it can be concluded that increases in muscle strength are directly related to improvements in physical function in the prefrail older adults, showing that home-based exercise programs are a viable option for the prefrail older adult.
In fact, the decrease in the time to perform the sit to stand test confirmed the gains in both groups in the muscle strength after the exercise program. Another research also revealed no significant differences between exercise groups (traditional × HB), since the performance of functional activities improved after both exercise programs. 12 Likewise, Fahlman et al. found an improvement in lower limb muscle strength after 16 weeks of resistance training with functionally limited older adults, assessed by the sit to stand test. However, it was attributed to the principle of specificity of training, since in their program, the exercise of sit to stand was performed, as in the current research. 34
Previous studies have also observed improvement in gait speed after 12 weeks of lower limb muscle strengthening in prefrail older women, 35,36 indicating enhancements in physical functional capacity. In contrast, in Mair et al. study, there are no improvements in gait speed after 6 weeks of a home-based weighted step exercise program. 37 However, the duration of the proposed program was half the time than the present study.
The results found in the present study are relevant as the reduction in gait speed is related to the development of dementia, since the motor and cognitive functions share similar neuroanatomical and psychological processes. 38 Also, the gait speed is shown as a predictor of physical function and survival, essentially the displacement speed, since older people walking above 1.0 m/s are considered physically functional, and speeds from 1.2 m/s may be related to increased survival in the community's older adults. 39
Although we did not find any significant difference in time to perform the TUG test in both groups after the intervention, the results found in the present study are above from the recommended cutoff values for age of the subjects. Bohannon et al. (2012) 40 consider that people with an average age of 70 years who perform the test in 12.6 seconds or less have excellent functional performance. In the present study, the participants presented an average of 9.56 seconds.
Regarding caloric expenditure comparison between groups by accelerometry in the 10th week, there was no difference in the average of the three exercise sessions. Nevertheless, although the HB group had a longer sedentary time, the similarity in the caloric expenditure of both groups occurred due to the longer time spent in light and very vigorous activities. Also, it is recognized that when the exercise is performed individually at home, the older adults probably take longer intervals between sets, and therefore, produce a longer sedentary time. Despite these differences observed between groups regarding the caloric expenditure level, it seems that it does not compromise the final results.
Limitations of the study include the impossibility of randomizing the sample due to the characteristics of the participants, classified as prefrail and dependent on a family member to take them to the center training. Therefore, the allocation between groups was made for convenience. However, statistical analyses indicated that the groups were homogeneous before the beginning of the exercise program, not affecting the quality of the study.
Conclusion
The results of the present study demonstrated that the home-based exercise program could be as effective as a center-based exercise program. Thus, the home-based program showed high adherence, and the center-based program showed a better reversal rate of frailty status. Regarding muscle function and physical function, both groups had similar developments in the postintervention period. Some factors may have contributed to the results found in the home-exercise group and should be used in future studies that use home-based programs, such as the incentive to exercise through social media (WhatsApp, Inc.), guidance, and frequent home visits. Therefore, individual home-based training may be a viable approach to exercise programs for prefrail older women and can be used in other settings outside of research institutions. Outside the research framework, considering nonfrail older adults, the data of the present study may be suitable for general older populations. However, some exercise intensity adjustments may be necessary, considering that robust older adults may need higher training overload because of their better physical condition.
Footnotes
Acknowledgments
The authors gratefully thank all volunteers who participated and cooperated in this study, the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES), and the Programa de Pós Graduação em Educação Física (UFPR).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was financed by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 88887.373894/2019-00.