
Abstract
Considering that telomere length can be determined not only by issues related to cell biology but also by aspects related to social factors and environmental exposures, studies on the relationship between social aspects and telomere length can help to better understand the still scarcely known aspects of the human aging process. Thus, this research seeks to verify whether social support networks are associated with telomere length in older adults. This is a cross-sectional study conducted with 448 individuals aged at least 60 years living in the urban area of an inland Brazilian municipality. Relative quantification of telomere length was obtained through real-time qPCR. Social support was assessed through the Medical Outcomes Study Social Support Scale. Descriptive statistics and multiple logistic regression were used in data analysis. The evaluated social support networks for older adults consist in a mean of 16.4 people, and the percentage of older adults who reported up to five members in their network was 27.75%. Shorter telomere length was identified in 25% of the participants, and the older adults who reported having up to five members in their support network were more likely to have a shorter telomere length than those who reported more numerous networks (odds ratio: 1.89, p = 0.011) regardless of gender, age, household arrangement, cognitive decline, and dependence for basic and instrumental activities of daily living, which suggests that measures that stimulate the creation and maintenance of social support networks should be implemented to improve older adults' health.
Introduction
The increase in the number of older adults in the population draws attention to the specific social and health demands of this age group and reinforces the importance of studying aspects that can improve quality of life and health in old age. 1 In this sense, social support—which is understood as the help received and offered within the scope of a social support network (i.e., formal and informal relationships established by individuals)—has been considered an important factor for health and disease among older adults. 2 –4
Studies on social support and health of older adults indicate that receiving satisfactory support is associated with better quality of life, 5,6 better subjective well-being, and better mental health. 7,8 Regarding functional capacity and mortality rate, older adults who offer social support and have more numerous networks are less likely to develop dependence and present a lower risk of death. 9 –11
Advances in research on geriatrics and gerontology can be observed in the increasingly frequent use of biomarkers to objectively demonstrate factors related to biological aging. Among these, telomere length stands out for its ability to predict cellular age and, consequently, the body's real level of deterioration. 12 Telomere length can be influenced not only by issues related to cell biology, but also by aspects related to social factors and environmental exposures. 13 Therefore, studies on the relationship between telomere length and social aspects, such as the characteristics of the social support network, are important to better understand the still scarcely known aspects of the human aging process.
Specific studies on the relationship between social support and telomere shortening are scarce in the literature. One of the articles found sought to verify whether loneliness and lack of perceived social support after wartime captivity could be associated with telomere shortening. A cohort of former Israeli war prisoners took part in the study, totaling 83 individuals. The results showed that loneliness and lack of social support were related to shorter telomere length. 14
Another study portraying the relationship between social support and telomere length was conducted with 4080 African Americans aged at least 50 years. The results showed that the low level of social support received from the family was associated with shorter telomere length. However, this study only evaluated family emotional support, which may limit the possibilities of effect in a broader social support context. 15 Similarly to this study, the research developed by Carroll et al 16 also showed telomere shortening among 948 participants aged from 45 to 84 years who reported low social support levels.
Despite the extensive literature on the beneficial effect of social support on the health of older adults, we observe a gap regarding the objective effect on telomere length and, consequently, on biological aging. Thus, considering the importance of social support as a determinant of health and disease in old age and that there are objective measures of the level of biological aging, this research seeks to verify whether social support networks are associated with telomere length in older adults.
Method
This is a cross-sectional study carried out in the municipality of Alfenas, southern Minas Gerais, Brazil. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for cross-sectional studies.
All procedures were performed in accordance with the ethical standards set forth in the Declaration of Helsinki. This research was submitted to the Research Ethics Committee of the Federal University of Alfenas, being approved under CAAE: 5218518.0.0000.5142/opinion No. 2,668,936. The older adults were included if they signed the informed consent form.
The population-based sample size was calculated considering an estimation of proportions in the order of 0.50, 95% confidence interval, design effect of 1.17, and population of 10,797 older adults, resulting in a minimum sample of 435 individuals. The final sample size was 448 individuals.
The older adults were recruited from selected households to ensure that individuals from all regions of the municipality were included. The sample complementation process carried out in the SABE Study (Saúde, Bem-estar e Envelhecimento) was taken as a basis, a population-based survey carried out in the city of São Paulo, Brazil. 17
The inclusion criteria were as follows: being at least 60 years old and not presenting neurological and/or cognitive conditions that would prevent the older adult from answering the questionnaire (perceived by the interviewer during presentation of the research and invitation to participate). The exclusion criterion was permanent or temporary inability to walk, except with the use of a walking aid device.
The data were collected between July and December 2019 at two different moments. At the first moment, an interview was conducted and, at the second moment, the blood samples were collected.
Study variables
Telomere length assessment
The dependent variable of this study is telomere length. The whole blood samples were processed according to the basic protocol of DNA extraction with affinity columns. Extraction of the material followed, according to the recommendations of the extraction kit manufacturer (PureLink™ Genomic DNA Mini Kit; Invitrogen). All the DNA genetic material was dosed in a Genova Nano spectrophotometer (Jenway), with its concentration corrected to 10 ng/μL in the samples.
The real-time PCRs were conducted using a Power SYBR Green PCR Master Mix as fluorescent marker in an ABI StepOne Real Time PCR System (Applied Biosystems), with a final volume of 10 μL per reaction. Negative and positive controls were added to the reactions.
For telomere identification, the markers described by Cawthon were used, namely, for telomere, the following sequences: telg: 5′ACA CTA AGG TTT GGG TTT GGG TTT GGG TTT GGG TTA GTGT3′ and telc: 5′TGT TAG GTA TCC CTA TCC CTA TCC CTA TCC CTA TCC CTA ACA3′, as well as markers for the control gene, human beta-globulin hbgu: 5′CGG CGG CGG GCG GCG CGG GCT GGG CGG ctt cat cca cgt tca cct tg3′ and hbgd: 5′GCC CGG CCC GCC GCG CCC GTC CCG CCG gag gag aag tct gcc gtt3′.
To reach the relative mean telomere length, a mathematical model was used based on the exponential proportion of the number of telomere sequence copies of each individual, compared with a number of copies of the single copy gene. 18
The distribution of the relative mean telomere length per quartile was adopted to categorize the variable in the current study. 19 Older adults with relative mean length in the last quartile, that is, among the 25% of the sample with the largest difference in relation to the single copy gene, were classified as “shorter telomere length.”
Evaluation of the social support network parameters
The independent variables of interest are as follows: size of the support network; material support; affective support; positive social interaction; and emotional/information support.
The size of the network was estimated by the answers to the following question: “Approximately how many close friends or relatives do you have? (People with whom you are comfortable and can talk about anything you want. People you can count on when you need help.)” Categorization of the variable was as follows: (0) more than five members; (1) up to five members.
The different types of support were evaluated using the Social Support Scale of the Medical Outcomes Study (MOS). This scale was originally elaborated by Sherbourne and Stewart 20 and later translated into Portuguese and validated in Brazil. 21 The questionnaire consists of 19 items, covering the following functional dimensions of social support: material; affective; and positive and emotional social interaction/information. The “low,” “average,” and “high” support classification was used, according to Zanini et al. 22 Considering the reduced number of older adults in the “high” classification of all the social support dimensions, for logistic regression analysis, the “high” and “average” classifications were merged.
Socioeconomic and health characteristics
The descriptive and adjustment variables are as follows: gender (male; female); age group (60–69 years old; 70–79 years old; 80 years and older); schooling (years of study); marital status (with a partner; without a partner); mean family income (in R$); household arrangement (lives alone; does not live alone); cognitive decline (Cognitive Abilities Screening Instrument-Short Form) 23,24 ; depressive symptoms—≥6 points on the Geriatric Depression Scale 25,26 ; multimorbidity (two or more self-reported chronic diseases); polypharmacy (reported continuous use of five or more medications); performance in basic activities of daily living 27 ; and performance in instrumental activities of daily living. 28
Data analysis
All the statistical analyses were conducted in the Stata software, version 13.0. In the data descriptive analysis, distributions of frequencies, means, medians, and standard deviations (SDs) were estimated for the continuous variables of the study. For the categorical variables, their proportions were estimated. The differences between the groups were estimated using Pearson's χ 2 and Fisher's exact tests. For the association analysis, multivariate logistic regression was used, and the magnitude of the association was estimated by the unadjusted and adjusted odds ratio (OR). The variables with p-values lower than 0.20 in the univariate analysis were included in the final model through the stepwise forward procedure. The variables presenting no statistical significance were maintained in the final model for adjustment. A significance index of 5% was used in all the analyses.
Results
Among the 448 older adults evaluated, we observed a higher proportion of women (70.76%); of individuals aged between 60 and 69 years (45.31%); with four or fewer years of study (66.07%); living with a partner (52.23%) and who do not live alone (81.47%); and the mean number of people per household was 2.5 (SD = 1.3). The mean family income was R$ 2355.30 (SD = 2022.52), with 44.20% reporting family incomes between one and two minimum wages and 20.98% reporting family incomes less than or equal to one minimum wage. Regarding health status, most of the sample is independent for basic (87.05%) and instrumental (64.51%) activities of daily living; and the majority has no cognitive decline (70.54%) or depressive symptoms (65.40%). Regarding the presence of diseases, 69.87% of the older adults reported having two or more chronic diseases (multimorbidity) and 41.74% continuously use five or more medications per day (polypharmacy).
Considering the distribution by quartiles, 25.00% of the older adults presented length above 148.7 (relative telomere length—T/S ratio), considered shorter telomere length, as they presented the greatest differences in relation to the human beta-globulin values. Figure 1 shows telomere length distribution among the 448 individual samples according to the age and size of the support network.
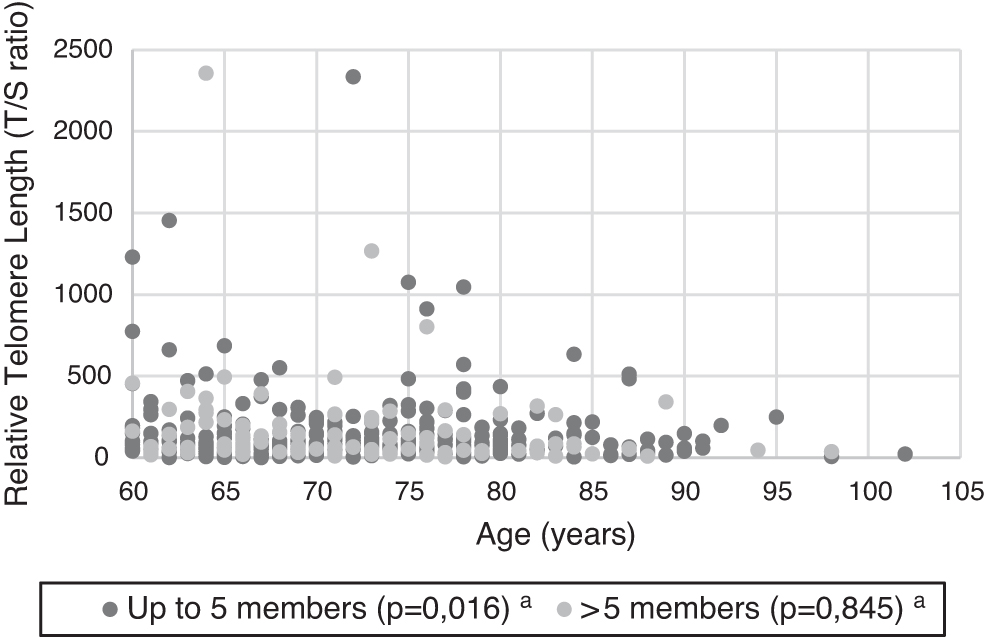
Relative telomere length (T/S ratio) distribution among the 448 individual samples according to age and size of the support network. aSpearman's correlation test.
The social support networks of the older adults evaluated consist in a mean of 16.4 people (SD = 22.2), with a median of 10. The percentage of older adults who reported up to five members in the network was 27.68%.
Most of the older adults reported average level of material support (77.95%), affective support (89.55%), positive social interaction (61.36%), and emotional support/information (69.32%). The dimensions with the highest percentage of older adults who reported low levels of perceived support were positive social interaction (38.17%) and emotional support/information (30.80%), and no older adult reported high levels of emotional support/information.
Regarding the relationship between socioeconomic and health characteristics and shorter telomere length, a statistically significant difference was only observed regarding the size of the social network, and the proportion of older adults with networks consisting of up to five people was higher among the individuals with shorter telomere length (Tables 1 and 2).
Percentage Distribution of the Older Adults According to Social Support and Shorter Telomere Length Characteristics
Alfenas, MG, Brazil, 2019. (n = 448).
Pearson's χ 2 test.
CI, confidence interval; OR, odds ratio.
Percentage Distribution of the Older Adults According to Socioeconomic, Health, and Shorter Telomere Length Characteristics
Alfenas, MG, Brazil, 2019. (n = 448).
Pearson's χ 2 test.
Current minimum wage = R$ 998.00.
BADL, basic activities of daily living; IADL, instrumental activities of daily living.
According to the multivariate logistic regression model, the older adults who reported having up to five members in their support network are more likely to have shorter telomere length than those who reported more numerous networks (OR: 1.89; 95% confidence interval: 1.16–3.08), regardless of gender, age, household arrangement, cognitive decline, and dependence for basic and instrumental activities of daily living (Table 3).
Multivariate Logistic Regression Model
Alfenas, MG, Brazil, 2019. (n = 448).
Discussion
This study sought to analyze the association between the social support network and telomere length in older adults, having found results showing that small networks (up to five members) are associated with shorter telomere length. We observed no association between any type of support and shorter telomere length, even though the proportion of older adults who reported low levels of affective support, positive social interaction, and emotional support/information, among those with shorter telomere length, was greater than the proportion of those who reported an average level of these types of support.
Although research indicates that there is an association between social support and telomere length, studies on this theme are scarce in the literature. As far as we know, this is the first study developed only with older adults, using the social support scale from the MOS and a measure of the size of the participants' social network.
Among the studies that we found, the first evaluated 948 individuals aged between 45 and 84 years participating in the Multi-Ethnic Study of Atherosclerosis and revealed that limited social support was related to shorter telomere length in the sample studied. 16
The second study that we found was developed by Mitchell et al 29 and sought to investigate the association of child socioeconomic status, child trauma, and social support with telomere length in a sample of 81 women evaluated at the beginning, middle, and end of pregnancy, as well as 7 to 11 weeks after delivery. The results revealed that low family social support was associated with shorter telomere length.
The third study to indicate the relationship between social support and telomere length evaluated whether loneliness and low social support influenced telomere length. The sample consisted of 83 former Israeli war prisoners with a mean age of 63.6 years. The results revealed that loneliness and low perceived social support were significantly associated with shorter telomere length. 14
The fourth study was developed by Hailu et al 30 with 1153 adults aged between 45 and 80 years and sought to evaluate the association of reports of discrimination with telomere length and modification of the effect measure by the perceived level of social support. The authors found no association between any of the discrimination measures and telomere length, although there was evidence of change in the effect by social support, and the individuals with low levels of social support and who reported moderate to high daily discrimination presented shorter telomere length.
As for the neurobiological aspects that may explain the relationship between support networks with few members and shorter telomere length, John Cassel's Stress Theory (1976) framework can be used, according to which social support is a resource that helps to face stressful situations, stressors cause a disturbance in the neuroendocrine balance that makes the body more susceptible to the occurrence of diseases, and chronic exposure to these stressors accelerates aging. 31
In this sense, the neurobiological effect of the reduced size of the social network in shortened telomere length can be understood from the deleterious effect of stress caused by social isolation. According to a systematic review conducted by Vlachos et al, 32 which sought to describe the neurobiological paths of social isolation and post-traumatic stress, social isolation exerts an effect of physiological overload, which would explain the deleterious effects at the cellular level, evidenced by the reduction in telomere length. According to this review, social isolation increases oxidative stress, release of proinflammatory cytokines, and baseline cortisol levels, as well as occurrence of diseases such as obesity and type II diabetes, thus influencing immunity, inflammation control, and genes that regulate responses to glucocorticoids in a negative way.
Thus, considering that one of the factors contributing to telomere shortening is oxidative damage and that social isolation is related to the greater presence of free radicals, by analogy, having small social networks can exert a similar effect.
In addition, the effect on telomere length can be understood by the fact that brain plasticity is also affected by the stress caused by social isolation. The dorsolateral bed nucleus of the stria terminalis, a subregion of the extended amygdala, plays a critical role in stress-induced plasticity, regulating the activity of the hypothalamic–pituitary–adrenal axis. It mediates between the corticolimbic system by receiving stressful stimuli and sending GABAergic projections to the paraventricular nucleus of the hypothalamus, where the corticotropin-releasing hormone is released and the response to peripheral stress is initiated under pituitary activation. Social isolation seems to cause a decrease in the long-term potential of the dorsolateral bed nucleus of the stria terminalis, reducing the response to stress, which, consequently, can cause cellular damage. 32 –34
When analyzing the size of the support network, we observed that it consists in a mean 16.4 people and that the mean number of family members is higher than that of friends. This network size is higher than that found in another two studies conducted in Brazil. 11,35,36 Also regarding size of the networks, a study conducted with a sample of 7284 older adults participating in the National Health and Nutrition Examination Survey (NHANES) evaluated the association between size of the social support network and risk of mortality rate among people with and without diabetes. 37 Approximately 60% of the NHANES sample reported having a network of up to five members, while in this study, only 23.50% mentioned networks with such size. 36 Cultural differences and the fact that developed countries are at a more advanced stage of the demographic transition may help explain the higher proportion of smaller networks among North Americans. 38
The strengths of this study are its larger sample size when compared with other national studies that measured telomere length in older adults and the fact of considering the biological effect of a social aspect on aging. By using telomere length as a biomarker of aging, this study contributes to knowledge in this area, as the role of genetics in the aging process depends on environmental factors, including the cultural environment in which a person lives and the relationships that remain throughout life. In general, the results of this study are in line with the current tendency to relate genetics to social aspects and, thus, help to better understand how people age.
Limitations
The limitations of this study include the use of a social support measure that has not been specifically validated for older adults and the arbitrary categorization of telomere length, as there are no parameters established in literature.
Conclusions
These findings suggest that there is an association between the number of members of the social support network and telomere length among the older adults evaluated, as well as networks consisting of up to five members are associated with shorter telomere length.
Footnotes
Authors' Contributions
A.R.C.B., D.B.L., F.A.C., D.S.P., and T.R.P.d.B.: Funding acquisition; conceptualization; writing—original draft; formal analysis; and writing—review and editing. D.P.N., J.B.N., A.A.d.S.O., G.d.S.R., and L.P.C.: Methodology; resources; and writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This article was supported by the National Council for Scientific and Technological Development (CNPq) (Grant No. 429823/2018-5-MCTIC/CNPq No. 28/2018) and by Fundação de Amparo à Pesquisa do Estado de Minas Gerais—FAPEMIG (Grant No. APQ-01168-18; 001/2018).