
Abstract
Acute pulmonary thromboembolism (APTE) has become a non-negligible clinical concern due to its high mortality and complex symptoms. Early diagnosis and prognostic assessment of APTE are of great significance for the long-term benefits of patients, especially elderly patients. Elderly patients with pulmonary embolism (n = 250) who presented to our hospital from January 2018 to July 2021 were recruited into this study. In addition, 50 healthy elderly people with no history of allergies were selected as the control group. An enzyme-linked immunosorbent assay (ELISA) method was used to determine concentrations of D-dimer and signal peptide-CUB-EGF domain-containing protein-1 (SCUBE1) in their plasma. Right ventricular volume contraction time (ICT), ejection time (ET), and isovolumic relaxation time (IRT) were determined by Doppler ultrasound. Right ventricular Tei index was calculated as (ICT + IRT)/ET. High plasma D-dimer, plasma SCUBE1, and right ventricular Tei index are risk factors for poor prognosis in APTE patients after treatment. Plasma D-dimer, plasma SCUBE1, and right ventricular Tei index have predictive value for poor prognosis in APTE patients. Their combined detection (0.256*DD +0.04*SCUBE1 + 10.188*Tei) can improve the sensitivity and specificity of prediction. There is a predictive value of combined plasma D-dimer, SCUBE1, and right ventricular Tei index for the prognosis of elderly patients with APTE.
Introduction
Acute pulmonary thromboembolism (APTE) is a general term for clinical syndromes caused by various thrombi obstructing the pulmonary artery system. 1 APTE is associated with a high mortality rate, and the incidence of APTE increases with age. 2 The clinical features of elderly patients with APTE lack specificity, which makes the early diagnosis and treatment of APTE rather difficult. 3
At present, the clinical diagnosis of APTE is varied. CT pulmonary angiography (CTPA) has high sensitivity and specificity for APTE and is currently the main examination method for diagnosis of APTE. 4 However, the contrast agent of CTPA increases the burden on kidneys, which makes the diagnosis difficult for elderly APTE patients with renal insufficiency. 5 Therefore, the use of early routine examinations to screen and diagnose suspected elderly patients with APTE has become an important clinical issue. 6
Warfarin is currently the drug of choice for anticoagulation in APTE therapy. 7 Warfarin has the advantages of low price, short half-life, and definite curative effect. 8 However, individual differences in the dosage of warfarin and the narrow safe treatment window make its anticoagulant effect unstable. 9 The dose of warfarin needs to be adjusted according to the international normalized ratio (INR). 10 Incorrect administration of warfarin may lead to adverse events of bleeding.
In addition, warfarin interacts with many foods and drugs, and the INR needs to be monitored regularly. 11 The application of warfarin requires patients to visit the hospital regularly for frequent blood draws, but many elderly patients cannot insist on regular follow-up visits. 12 Therefore, it is of great significance to evaluate the prognosis of APTE patients as soon as possible and adopt scientific and reasonable countermeasures to deal with the disease.
This study hypothesized that age-adjusted D-dimer (AADD) levels combined with the right ventricular Tei index and blood signal peptide-CUB-EGF domain-containing protein-1 (SCUBE1) could be effective in diagnosing APTE, avoiding the risk of iatrogenic CTPA injury, including radiation- and contrast-induced nephropathy. In addition, we also explored their role in predicting the prognosis of patients with APTE and guiding the correct oral warfarin medication for patients after discharge.
We hope that our study can further simplify and optimize the diagnostic procedure of pulmonary embolism in the elderly and improve the diagnostic efficiency in elderly patients with diabetic nephropathy, abnormal renal function, or hemodynamic changes that are not suitable for CTPA examination.
Methods
Participants
A total of 250 elderly patients with APTE who visited our department were selected as the research subjects. Another 50 healthy elderly people with no history of allergies were selected as the control group. Inclusion criteria were as follows: (1) diagnosed as having APTE according to the Chinese Medical Association Guidelines for Diagnosis of Pulmonary Embolism; (2) aged ≥60 years; and (3) with complete clinical data.
Exclusion criteria were (1) patients with right ventricular dysfunction caused by other causes and (2) patients with other causes of elevated SCUBE1: acute coronary syndrome; acute myocardial infarction; acute ischemic cerebrovascular disease; and peripheral arterial disease. The study was reviewed and approved by the Cangzhou Central Hospital.
D-dimer and SCUBE1 examination
Three milliliters of fasting peripheral venous blood was collected from APTE patients into EDTA anticoagulation tubes after admission and before treatment, and concentrations of D-dimer and SCUBE1 in their plasma were determined by enzyme-linked immunosorbent assay (ELISA). Healthy volunteers were subjected to the same measures described above.
Ventricular Tei index
Echocardiography was performed on APTE patients and volunteer healthy controls before treatment. A Philips HDII color Doppler ultrasound instrument was used with a probe frequency of 2.0–4.0 MHz. All subjects were placed in the left lateral decubitus position. Transthoracic echocardiography was used for exploration and an electrocardiogram was synchronously connected to measure the following indicators: right atrial transverse diameter (RA), right ventricular transverse diameter (RV), and right ventricular anterior wall thickness (RVAW) and systolic pulmonary artery pressure (SPAP) estimated from tricuspid regurgitation.
The standard views for Doppler measurement of tricuspid regurgitation were the right ventricular inflow tract and right ventricular outflow tract views. Measurement of right ventricular Tei index was done as follows: the tissue Doppler imaging mode was activated in the apical four-chamber view, and the sampling volume was placed at the junction of the right ventricular free wall and the anterior tricuspid valve. The angle was adjusted to make the sampling line and the long axis of the right ventricle as consistent as possible to obtain the best image quality and angle.
The isovolumic contraction time (ICT), ejection time (ET), and isovolumic relaxation time (IRT) were obtained by measuring the isovolumic systolic wave, systolic S wave, and isovolumic diastolic wave duration, respectively. The right ventricular Tei index was calculated as (ICT + IRT)/ET. 13
Study design
All APTE patients in this study were followed up for 30 days to examine the prognosis of patients. The patient's prognosis was recorded within one month after the end of treatment. All APTE-related adverse events at 30-day follow-up were recorded: exacerbation or recurrence of APTE, intubation and ventilator use, and patient death from various complications.
Patients with any of the above conditions were defined as having a poor prognosis. Patients were thus divided into the good prognosis group (n = 178) and poor prognosis group (n = 72).
Statistical methods
Data are presented as mean ± standard deviation or n (percentage). Comparisons of data were done using the Mann–Whitney test or Fisher's exact test or chi-square test. Multivariate logistic regression analysis was used to analyze the risk factors.
Results
Clinical characteristics of APTE patients in the good or poor prognosis group
All APTE patients enrolled in this study were followed up for 30 days after their treatment ended. Patients were thus divided into the good prognosis group (n = 178) and poor prognosis group (n = 72) according to the occurrence of APTE-related adverse events. We analyzed and compared the basic clinical information of patients with good and poor prognosis.
As shown in Table 1, there were no significant differences in gender, primary diseases, smoking history, bleeding history, and APTE location between the two groups of patients. However, there were statistical differences in age (p = 0.005), deep vein thrombosis history (p = 0.004), plasma D-dimer (p < 0.001) and plasma SCUBE1 (p < 0.001) levels, and right ventricular Tei index (p < 0.001) between the two groups.
Baseline Characteristics of Elderly Acute Pulmonary Thromboembolism Patients with Good or Poor Prognosis
Data are presented as mean ± SD or n (percentage). Comparisons of data were done using the Mann–Whitney test, Fisher's exact test, or chi-square test. Chronic lung disease includes chronic obstructive pulmonary disease, active asthma, lung fibrosis, cystic fibrosis, or bronchiectasis.
APTE, acute pulmonary thromboembolism; SCUBE1, signal peptide-CUB-EGF domain-containing protein 1.
APTE patients with poor prognosis had higher age, plasma D-dimer and SCUBE1 levels, and right ventricular Tei index relative to patients with better prognosis.
Risk factors for prognosis of APTE in the elderly
We used multivariate logistic analysis to analyze prognostic risk factors for APTE in the elderly. We used prognosis (0 = good and 1 = poor) as the dependent variable, and age, gender, diabetes, hypertension, hyperlipidemia, coronary heart disease, chronic kidney disease, chronic lung disease, tumor, smoking history, history of deep vein thrombosis, major bleeding, APTE occurrence site, plasma D-dimer, plasma SCUBE1, and right ventricular Tei index were independent variables.
As shown in Table 2, older age, history of deep vein thrombosis, high plasma D-dimer and SCUBE1 concentration, and right ventricular Tei index were risk factors for poor prognosis in APTE patients after treatment (p < 0.05).
Multivariate Logistic Analysis of Predictors for Elderly Patients with Poor Prognosis After Acute Pulmonary Thromboembolism Treatment
CI, confidence interval; OR, odds ratio.
Plasma D-dimer, SCUBE1, and right ventricular Tei index were upregulated in APTE patients compared with normal controls
We have shown that plasma D-dimer, SCUBE1, and right ventricular Tei index have effects on the prognosis of APTE patients. Therefore, we wanted to further explore whether these factors have predictive value for the onset of APTE in the elderly. The differences in plasma D-dimer, plasma SCUBE1, and right ventricular Tei index were compared between 50 healthy controls and APTE patients.
There was no significant difference between the mean age of the control group, 70.41 ± 5.53 years, and mean age of APTE patients, 69.84 ± 6.14 years. The sex ratio of the control group was 28 males to 23 females, and there was no significant difference between the control group and APTE patients.
As shown in Figure 1, plasma D-dimer levels (p < 0.001, Fig. 1A), plasma SCUBE1 levels (p < 0.001, Fig. 1B), and the right ventricular Tei index (p < 0.001, Fig. 1C) were all dramatically upregulated in APTE patients compared with healthy controls.

Comparisons of plasma D-dimer
Correlation of plasma D-dimer, plasma SCUBE1, and right ventricular Tei index in APTE patients
We further analyzed the correlation between plasma D-dimer, plasma SCUBE1, and right ventricular Tei index by Spearman correlation analysis. As shown in Figure 2A, plasma D-dimer and plasma SCUBE1 levels were positively correlated in APTE patients (r = 0.29, p < 0.001). As shown in Figure 2B, the plasma D-dimer level and right ventricular Tei index were positively correlated in APTE patients (r = 0.25, p < 0.001).

Spearman correlation analysis was carried out to measure the correlations of plasma D-dimer with SCUBE1
Similarly, the right ventricular Tei index in APTE patients was positively correlated with the plasma SCUBE1 level (Fig. 2C; r = 0.17, p = 0.006).
Predictive value of plasma D-dimer, SCUBE1, and right ventricular Tei index for the poor prognosis of APTE
To explore whether these factors have predictive value for the prognosis of APTE in the elderly, we first compared the plasma D-dimer, plasma SCUBE1, and right ventricular Tei index in the good prognosis (n = 178) and poor prognosis (n = 72) groups. As shown in Figure 3, the plasma D-dimer level (p < 0.001, Fig. 3A), plasma SCUBE1 level (p < 0.001, Fig. 3B), and the right ventricular Tei index (p < 0.001, Fig. 3C) were all dramatically upregulated in poor prognosis patients compared with the good prognosis patients.
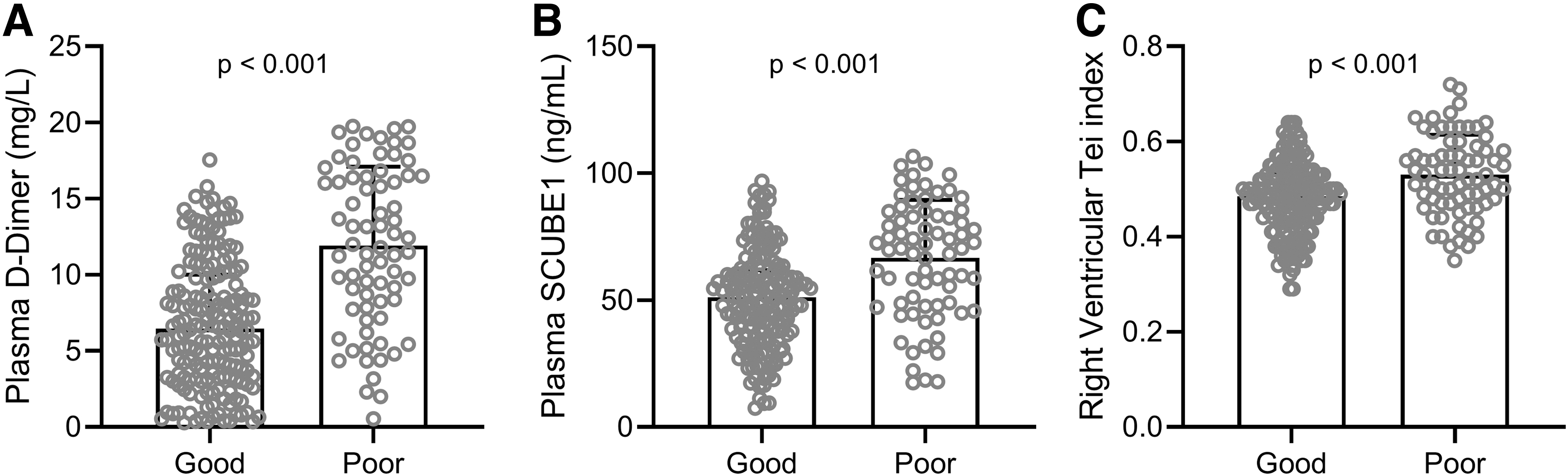
Comparisons of plasma D-dimer
We thus performed an receiver operating characteristic (ROC) analysis to investigate the predictive values of plasma D-dimer, plasma SCUBE1, and right ventricular Tei index and their combination factor (0.256*DD +0.04*SCUBE1 + 10.188*Tei) for the prognosis of APTE patients. Figure 4 and Table 3 together indicate that plasma D-dimer, plasma SCUBE1, and right ventricular Tei index have predictive value for APTE and prognosis.
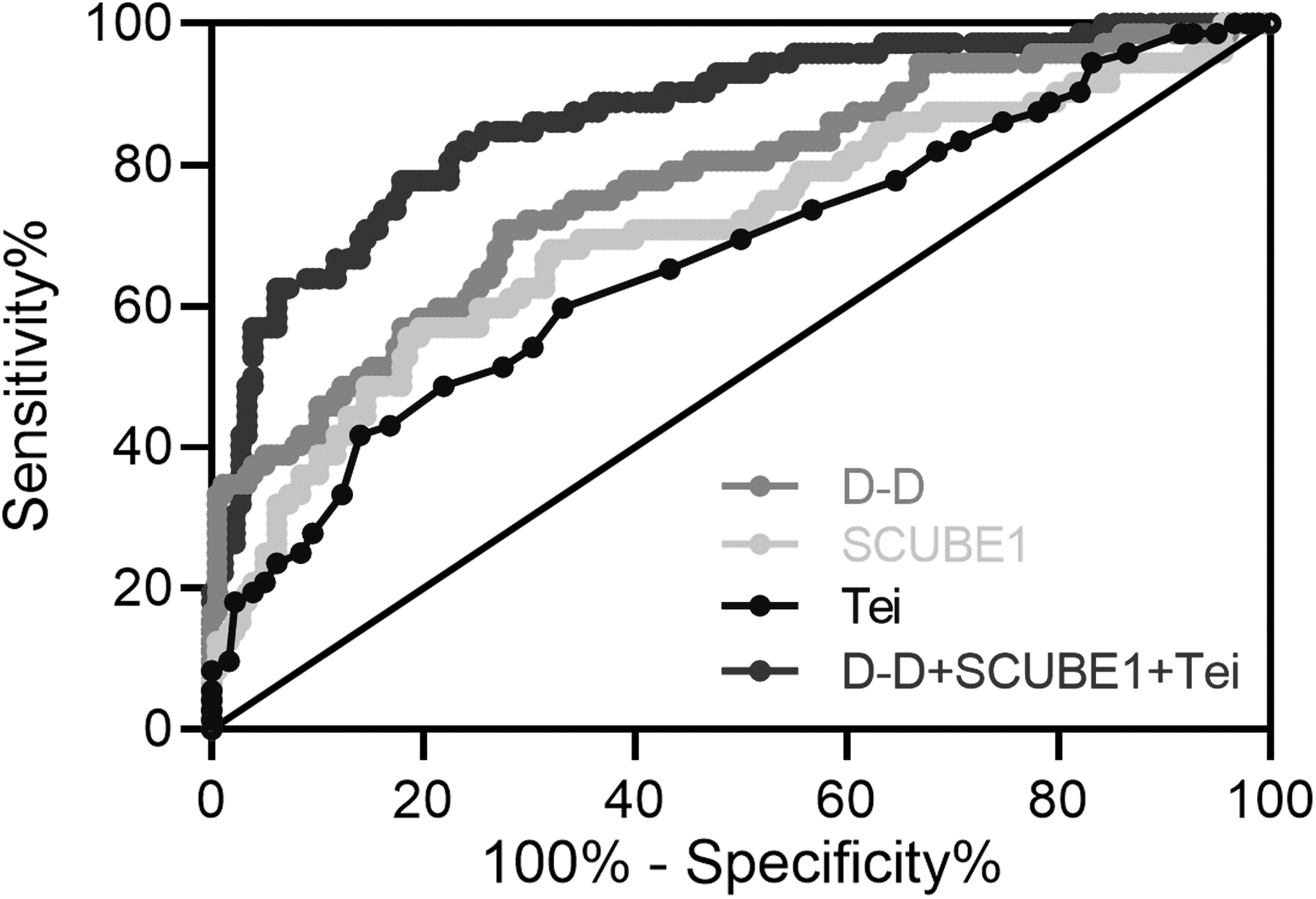
ROC analysis of plasma D-dimer, SCUBE1, and right ventricular Tei index and their combined test for prediction of poor prognosis in elderly patients with APTE. ROC, receiver operating characteristic.
Predictive Values in Receiver Operating Characteristic Analysis
Logit (D-D+SCUBE1+Tei) = 0.256*DD +0.04*SCUBE1 + 10.188*Tei.
AUC, area under curve.
The combined detection model could significantly improve sensitivity and specificity compared with any single factor detection.
Discussion
APTE is a common and seriously life-threatening disease and is one of the three major cardiovascular diseases along with myocardial infarction and stroke. 14 APTE has the characteristics of acute onset, high mortality, and lack of specific clinical manifestations. 15 It is easily confused with other heart and lung diseases and the severity of symptoms can vary widely. The problems of missed diagnosis and misdiagnosis in the process of APTE diagnosis should not be underestimated. 16
At present, the diagnosis of APTE mainly relies on special imaging examinations such as classic pulmonary angiography, CTPA, radionuclide ventilation/perfusion imaging, and magnetic resonance pulmonary angiography. 17 These examinations are time-consuming and expensive and cannot be completed by most critical emergency patients. In addition, the use of contrast media will increase the burden on kidneys and make the differential diagnosis of elderly patients with renal insufficiency difficult. 18
Therefore, simple and effective screening of patients with suspected APTE is crucial. At present, new anticoagulants such as dabigatran and rivaroxaban do not require frequent monitoring of blood coagulation during APTE treatment, which solves the problem of blood drawing for patients and makes it easier for patients to adhere to the medicine. 19 However, new anticoagulants may still lead to adverse bleeding events, and there is a lack of effective antagonists for targeted treatment. 20
Patients taking newer anticoagulants are at greater clinical risk for adverse bleeding events, and there is no monitoring method for anticoagulation status similar to the INR. 21 In addition, many patients are unable to bear the financial pressures of new anticoagulant drugs, so warfarin will not be replaced soon. 22 The unstable anticoagulation effect of warfarin and the potential bleeding risk require us to make an early prediction and assessment of the prognosis of APTE patients so as to provide timely medical detection and intervention. 23
In this study, we attempted to use the predictive value of plasma D-dimer, plasma SCUBE1, and right ventricular Tei index and their binding factors (factors of the joint prediction model are obtained by SPSS analysis: 0.256*DD +0.04*SCUBE1 + 10.188*Tei) for poor prognosis in APTE patients. We first demonstrated that plasma D-dimer, plasma SCUBE1, and right ventricular Tei index were elevated in APTE patients relative to normal subjects and they were also elevated in poor prognosis APTE patients relative to good-prognosis patients. We further demonstrated the predictive value of plasma D-dimer, plasma SCUBE1, and right ventricular Tei index for poor prognosis in APTE patients by ROC analysis.
We hope that our research can further simplify and optimize the diagnostic procedures of pulmonary embolism in the elderly, avoid overexamination, and reduce adverse reactions such as radiation exposure and contrast agent allergy. We hope that our study will help improve the prognosis of APTE in elderly patients with diabetic nephropathy, abnormal renal function, or hemodynamic changes that are not suitable for CTPA examination.
Clinically, D-dimer detection is often used as the primary screening method for APTE, but the level of D-dimer is affected by various factors, such as advanced age, infection, tumor, surgery, trauma, pregnancy, and history of deep vein thrombosis. 24 As a result, the specificity of D-dimer in diagnosing APTE is low, which can easily lead to misdiagnosis, unnecessary examination, and waste of medical resources.
The 2014 edition of the European Society of Cardiology (ESC) guidelines for the diagnosis and management of acute pulmonary embolism proposed the cutoff value of AADD, that is, for patients aged ≥50 years, age × 10 μg/L is used as the cutoff for PTE screening. 25 The plasma D-dimer determination combined with clinical assessment is an important primary screening test for APTE. 26
Correcting the D-dimer threshold using patient age can effectively improve the accuracy of PE diagnosis. In addition, it is equally important to look for other biomarkers or to use a combination of several markers for initial screening of patients with suspected pulmonary thromboembolism.
SCUBE1 is a glycoprotein expressed and secreted on the surface of activated platelets during early embryonic development, which promotes platelet-to-platelet interactions and supports platelet–matrix adhesion. 27 APTE is the terminal event of thrombosis, and an elevated SCUBE1 level indicates the continuous activation of platelets in early thrombus formation, so it may be of great value for early diagnosis of APTE.
Some foreign scholars have reported that the expression of SCUBE1 is elevated in patients with acute pulmonary embolism, while the expression level is extremely low in healthy people, suggesting that SCUBE1 is expected to be a biomarker for early diagnosis of acute pulmonary embolism. 28 However, no studies have investigated the diagnostic value of SCUBE1 for APTE in the elderly Chinese population.
The special physiological characteristics of the right ventricle contribute to many difficulties in the diagnosis of PE clinically, which can increase the misdiagnosis rate and missed diagnosis rate of APTE. 29 Studies have shown that right ventricular dysfunction is one of the important indicators in the diagnosis of clinical APTE patients. 30 In the early stage of PE patients, evaluating the right ventricular function of patients is of great significance for disease diagnosis, staging, treatment, and prognosis. 31
Therefore, to improve the accuracy of clinical screening of PE patients, this study evaluated patients by correcting the D-dimer threshold combined with the right ventricular Tei index and compared the level of SCUBE1 to provide a reference for the diagnosis and prognosis of clinical PE.
Conclusions
In conclusion, we demonstrated the predictive value of combined plasma D-dimer, SCUBE1, and right ventricular Tei index for the prognosis of elderly patients with APTE. The combined detection of plasma D-dimer, SCUBE1, and right ventricular Tei index (0.256*DD +0.04*SCUBE1 + 10.188*Tei) could improve the sensitivity and specificity for poor prognosis of APTE compared with a single factor.
Footnotes
Authors' Contributions
Data curation and analysis were performed by M.Y., Y.L., Y.M., and W.W.; drafting of the manuscript was performed by M.Y. and Y.M.; and concept and design of the study were performed by M.Y. and Y.M.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by the Cangzhou Science and Technology Research and Development Program (213106022).