
Abstract
This study aimed to establish a complement tolerance test (CTT) as a marker of protein fragility and discuss its clinical significance. Total complement activity (TCA) of serum was measured using a self-hemolysis colorimetric method. Human O-erythrocytes and rabbit anti-human O-erythrocyte antibodies were used to replace sheep erythrocytes and the corresponding hemolysin for the hemolysis test, respectively. The antigen-antibody specific binding activated the classical pathway of complement, generating a membrane attack complex, and the red blood cells rupture. A CTT was established to measure complement heat tolerance according to the sensitivity of complement proteins to temperature, which was calculated according to differences in TCA at different temperatures. The smaller the CTT the stronger the complement resistance to heat. The method was applied to the detection of diabetic patients and healthy controls. The mean value of CTT (mean) = 0.063 ± 0.003 with a coefficient of variation of 4.8% for the same specimen tested for complementary thermal resistance on 5 consecutive days, which is a good stability of the assay. Application of CTT on samples from patients with different ages revealed significantly higher mean CTT values for elderly patients (≥60-years old) relative to those for younger patients (20–40-years old) (p < 0.05). In addition, the mean CTT values for diabetic patients were significantly higher than those for healthy patients (p < 0.001). We successfully established a method that uses complement thermal resistance as a marker of protein fragility, with the results demonstrating the ability of the CTT identify age- and disease-related variations in patient samples and its potential efficacy for clinical application.
Introduction
The gradual inability of cells and organisms to maintain protein homeostasis with age and the reduced ability of proteins to resist external perturbations lead to a decline in the overall health of the organism, inadequate response to stress, and a shortened healthy lifespan. 1 Maintenance of cellular protein homeostasis is a key process that ensures longevity, with primary factors involved in this process, including chaperones and two protein-hydrolysis systems: the ubiquitin–proteasome and the lysosome–autophagy system. 2 Notably, both autophagy and proteasome activity decrease with age, 3 which is accompanied by enhanced protein damage due to oxidation that ultimately interferes with normal chaperone function. These actions result in imbalanced protein homeostasis 4 and increased vulnerability of the proteome to stress in the aging population. 3
In addition, heat treatment, which induces protein denaturation and aggregation, affects protein spatial structure and function due to conformational changes. A previous study identified caloric restriction as an effective intervention to combat aging and improve stress resistance in cultured cells based on improved protein stability, 4 These findings suggest that protein vulnerability to external stimuli might be age-related.
However, the change of protein is also related to the redox state of the body, diseases, and other factors. Compared with the younger group, it was found that the total antioxidant capacity in the older than 75-year age group decreased significantly, along with a decrease in the mass of antioxidant substances and average activity levels in human serum. 5 In contrast to the results in serum, more antioxidants were detected in the urine of the elderly in the healthy population. In addition, more antioxidants were found in urine of tumor patients with same age range. 6 The antioxidant capacity of serum and urine was significantly lower in diabetic patients compared to healthy individuals. 7
Antibody activity was determined by a variety of immunological assays, including precipitation reactions, agglutination reactions, and enzyme immunoassays, to quantitatively assess the effect of oxidants on antigen-antibody binding in vitro. A certain concentration of oxidants significantly inhibited the activity of antibodies, but had little effect on the total antioxidant capacity of serum. 8 In addition, a certain concentration of ammonium ferrous sulfate could significantly inhibit antibody, enzyme, DNA, and diluted serum. Certain concentrations of ascorbic acid resulted in significant inhibition of antibody. The reduction in antibody activity induced by oxidizing agents was partially repaired by a reductant. 9
Aging attenuates the efficiency of bodily functions. Biomarkers of this vulnerability have been identified based on the relationship between aging and age-related diseases or lifespan. These include markers of inflammation (e.g., interleukin-6 and C-reactive protein), the immune response (e.g., white blood cell count), and epigenetic changes (e.g., DNA methylation), as well as clinical markers, such as albumin and fibrinogen levels. 10 Because protein destabilization during aging is related to the pathogenesis of numerous diseases, measurement of protein fragility might enable identification and prediction of those at risk of age-related diseases to optimize intervention and treatment.
The complement system comprises heat-resistant proteins present in normal human and animal serum and plays an important role in host defense against bacteria, the interface between innate and adaptive immunity, and removal of immune complexes and apoptotic cells. 11 The three main complement-activation pathways (classical, lectin, and alternative) promote the formation of a membrane-attacking complex (MAC) that regulates phagocytosis or lysis of pathogenic targets. Changes in the activity/function of any component of this system adversely effect the complement system, thereby altering its ability to regulate the destruction of invading microorganisms and prevent excessive activation of autologous cells and tissues. 12
The activation of complement is a cascade of enzymatic reactions and is very sensitive to temperature. Affected by heat treatment, heat intolerance of any of the proteins of this system leads to changes in the total complement activity (TCA). Thus the fragility of the protein can be reflected by the complement tolerance test (CTT). There are neither detailed studies on complement heat tolerance nor are there any reports using it as a marker of protein fragility. In this study, the change in TCA during heating to reflect protein fragility, which may be associated with the onset of certain diseases, is a new indicator for disease diagnosis.
Moreover, age-related alterations in protein stability can affect the complement system, which is also highly sensitive to changes in temperature. 13 Therefore, evaluation of complement thermal resistance might reflect overall levels of protein stability according to their ability to resist external disturbance. The CTT was established to measure complement heat tolerance according to the sensitivity of complement proteins to temperature, which was calculated according to differences in the TCA at different temperatures.
The main methods used for the determination of TCA include the CP-CH50 method, the AP-CH50 method, the single-tube titration method, and the plate-hemolysis method. It has been established that the complement system is heat-labile and that heating the serum samples above 37℃ could denature some of the complement proteins and thus resulting in lower activity as measured by the CH50 assay. Therefore, in this study, we used a previous technique for determining complement efficacy that uses antigen–antibody complexes to assess 50% hemolytic complement activity (CH50). 14 We then developed a colorimetric method to measure TCA according to the CH50 using human red blood cells (RBCs), 15 which allowed evaluation of changes in complement activity according to temperature and determination of overall complement thermal resistance.
The results demonstrated the utility of the complement heat tolerance as a marker of protein fragility and its relationship with age- and disease-related changes. Meanwhile, the protein fragility in older adults may be related to a reduced capacity for oxidative stress. Oxidative stress itself is not significant when it does not cause protein alterations, but when it does cause protein damage, it affects protein fragility, and protein changes can lead to functional alterations and therefore induce disease. Finally, the complement heat resistance assays are clinically important and can be used as markers for onset of certain diseases.
Materials and Methods
All of the experiments on the subjects were conducted in accordance with the Declaration of Helsinki, the study was approved by the Institutional Ethics Committee of Dalian Medical University and informed consent was waived, as the samples were remnants following clinical use and therefore not specifically collected for this study and without risk to patients.
Establishment of a CTT to measure the complement thermal resistance
We used 2% human O-erythrocytes as a hemolysis-indicator system and the 2U hemolysin to detect the extent of hemolysis. The 2U hemolysin (anti-human O-erythrocyte antibody, trade name rabbit anti-human O-erythrocyte serum, potency 1: 100, supplied by Zhengzhou Baiji Biotechnology Co., Ltd.) was diluted in the buffer mentioned above according to potency (this concentration unit was based on the potency of hemolysin when it caused an agglutination reaction; when the potency of hemolysin was 100, we diluted it 50 times to obtain 2 U of hemolysin). We confirmed complement activity based on MAC generation and erythrocyte rupture and according to correlations between the degree of hemolysis and complement activity. Optical density (OD) values were determined at 37°C and 47°C and were used to calculate TCA, with the difference used to calculate the complement thermal resistance (Fig. 1).

Principle diagram of the complementary thermal resistance experiment. CTT, complement tolerance test; MAC, membrane-attacking complex.
The study subjects were all Chinese, and there was no genetic relationship between them. Serum was obtained by collecting venous blood from patients and healthy controls, leaving it to stand for 1 hour at 4°C, and centrifuged at 2500 rpm (1118 × g) for 5 minutes to separate the serum, which was divided into two 100-μL aliquots that were subsequently incubated at 37°C and 47°C, respectively, in a water bath for 30 minutes. Ensure that the number of samples tested is sufficiently large and that details regarding sample collection, storage, and storage duration were consistent.
Serum samples were then transferred to 1.5-mL tubes, into which the 50-μL anti-RBC antibody (1:100), 50-μL 2% human O-erythrocytes, and 800-μL PBS buffer were added (Fig. 2) for incubation at 37°C for 30 minutes. The mixture was then centrifuged at 2500 r/min for 5 minutes, and 100 μL of supernatant from each tube was added to a 96-well microtiter plate, which was used to determine the OD at 542 nm. TCA was determined by subtracting the OD values at each respective temperature.
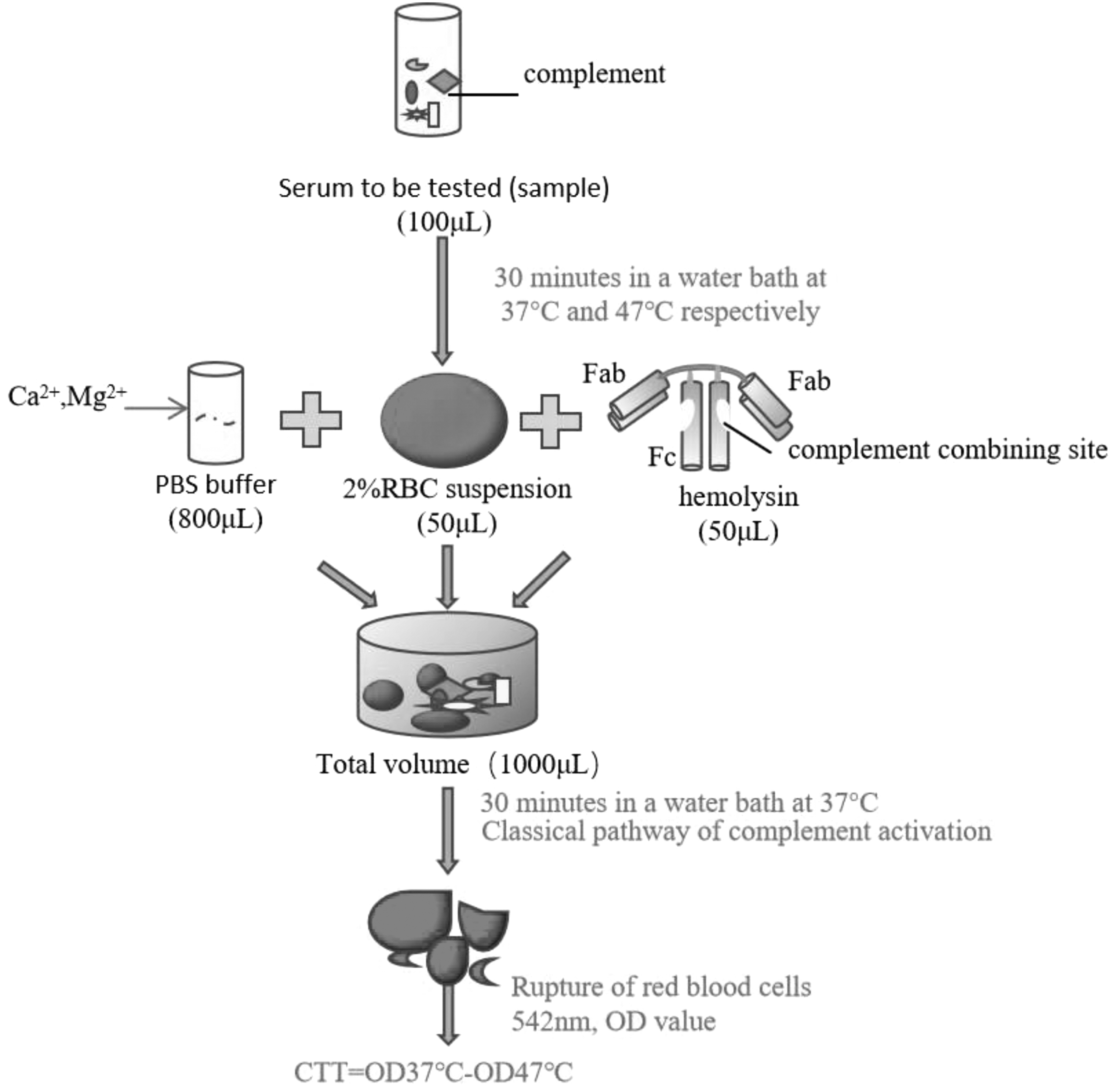
The flowchart of experimental operation of the complement tolerance test. RBC, red blood cell.
Assessment of the complement thermal resistance assay
Serum samples were subjected to measurements of the complement thermal resistance assay for 5 consecutive days to demonstrate method reproducibility. Venous blood was collected and serum isolated, as described, followed by separation into five 200-μL aliquots, one of which was used immediately and the remaining immediately frozen at −20°C until use. Each aliquot was divided into two 100-μL samples that were used to perform the assay described in Establishment of a CTT to Measure the Complement Thermal Resistance section, which was repeated for each of the five samples on separate days.
Measurement of the complement thermal resistance using samples from different age and gender groups
Healthy adult subjects were divided into age (20–40 years old [n = 39; mean: 30.77 ± 6.98 years] and ≥60 years old [n = 49; mean: 75.20 ± 8.13 years]) and gender (25 males; mean: 30.96 ± 7.30 years; 14 females; mean: 30.43 ± 6.62 years). The CTT was performed on samples as described in Establishment of a CTT to Measure the Complement Thermal Resistance section.
Measurement of the complement thermal resistance in diabetic patients
Serum samples were collected from 42 patients (20 males, 22 females) meeting the clinical diagnostic indexes of diabetes mellitus and the World Health Organization criteria for type 2 diabetes (T2D) mellitus at the First Affiliated Hospital of Dalian Medical University (Dalian, China), with sera from 39 healthy patients (21 males, 18 females) used as controls. There were no statistical differences between the mean ages of both groups (control: 68.69 ± 6.10 years vs. diabetic: 69.10 ± 11.97 years).
Statistical analysis
Data dispersion was compared by calculating the coefficient of variation (CV). According to the data homogeneity of variance (Levene's test) and normal distribution (Kolmogorov-Smirnov test), an independent sample t test was used to determine differences between two groups of samples. All analyses were carried out using SPSS statistical analysis software (SPSS, Inc., Chicago, IL). p-Values <0.05 (two-tailed) were considered significant.
Results
CTT stability
Table 1 shows the results of measuring the complement thermal resistance on serum samples from the same healthy volunteer over 5 consecutive days. CTT results were 0.066, 0.066, 0.060, 0.060, and 0.064 (mean: 0.063 ± 0.003), with a CV of 4.8%.
Results of Complement Tolerance Test on Serum Samples from the Same Healthy Volunteer on 5 Consecutive Days
CTT, complement tolerance test; CV, coefficient of variation; SD, standard deviation.
Age-related changes in CTR
Table 2 shows that the mean of the complement thermal resistance measured using the CTT differed significantly according to age (20–40 years old: 0.053 ± 0.007 vs. ≥60 years old: 0.056 ± 0.008) (p < 0.05).
Results of Complement Tolerance Test in Different Age Groups
K-S test, Kolmogorov-Smirnov test.
Gender-related differences in the complement thermal resistance
Table 3 shows no significant difference in the complement thermal resistance according to gender based on the CTT (males: 0.053 ± 0.006 vs. females: 0.052 ± 0.007) (p > 0.05).
Results of Complement Tolerance Test in Males and Females
Differences in the complement thermal resistance between diabetic patients and healthy controls
Table 4 shows a significant difference in the complement thermal resistance between diabetic patients and healthy controls (controls: 0.042 ± 0.008 vs. diabetic: 0.050 ± 0.008) (p < 0.001).
Results of Complement Tolerance Test in Diabetic Patients and Healthy Subjects
Discussion
There is some evidence to verify the reliability of our method. 16 –19 The main methods used to determine TCA include CP-CH50 method, the single-tube titration method, and the plate hemolysis method. However, the CP-CH50 method is a manual, complex, and semiquantitative analysis that requires a long preparation time. In addition, fresh sheep red blood cells are difficult to collect, transfer, and preserve, and their quality is not guaranteed. Dong et al established a method for measuring TCA based on a hemolysis system using own RBCs. 15
Human RBCs were used as a hemolysis indicator system and rabbit anti-human RBC antibody instead of the traditional hemolysin (rabbit anti-sheep RBC antibody) in the new method. TCA using the new method was significantly correlated with the CH50 method and had clinical significance. In this study, the single-tube method was chosen instead of the multitube method and overcame the complicated procedure and poor stability of the CH50 method, simplified the detection of TCA. 20 –22
We established a new method for characterizing parameters of complement activity as a marker of protein fragility. As heat treatment is a physical factor, it is easy to manipulate and can affect the spatial structure and function of proteins. Heat adversely affects protein secondary structure, which alters the function of each complement component and each product of the activation process. In this study, we measured complement activity using cytolysis experiment at two temperature gradients (37°C and 47°C), as well as CTT accuracy for 5 consecutive days, finding a CV of 4.8%, which demonstrated the stability of the test. Furthermore, we confirmed the absence of significant gender-specific differences in CTT results, whereas significantly higher readings were identified in older patients relative to younger patients (old: 0.056 ± 0.008 vs. young: 0.053 ± 0.007, p < 0.05).
These findings indicated that age-related sensitivity to temperature and external stimuli alter complement protein structures. The objective of the study was to establish a CTT as a maker of protein fragility and discuss its clinical significance. While the readout of the assay is OD, the ODs are typically normalized to the OD of water (100% lysis) to calculate % lysis of each sample. This is important because the OD may change from run to run depending on the target cell preparation. This point needs to be clear throughout in the study.
In addition, we performed a case-control study using diabetic patients and age-appropriate healthy controls in the clinical setting to evaluate differences in complement protein resistance to temperature. It shows a significant difference in the complement thermal resistance between diabetic patients and healthy controls (controls: 0.042 ± 0.008 vs. diabetic: 0.050 ± 0.008). The comparison revealed significantly weaker thermal resistance in diabetic patients relative to healthy subjects (p < 0.001). For each batch of experiments, fresh 2% RBCs were prepared again, so the detection system was different. When there were different blood cells in the detection system, OD and CTT values would be slightly different, so each batch of experiments set up its own control group. It was observed that the results of different experiments were slightly different, which had no influence on the conclusion.
There is a strong link between the complement system, the activity of complement regulatory proteins, and the pathogenesis of diabetes and its complications. 23 The content of hemolytically effective molecules of some classical complement components as well as factors of the alternative activation pathway was studied by radio immunodiffusion method and other methods. Levels of C3 and C4, factors B and D were significantly elevated in the patients with insulin dependent diabetes compared with healthy donors. However, if the insulin-dependent diabetes have antigens B18, C4 levels were lower than those of the control group. In noninsulin-dependent diabetes C4, factors B and D were significantly elevated, and C5 levels were reduced. The levels of complement C3 and C5 were decreased and the content of C4 was increased in diabetic patients with diabetic nephropathy. 24
Furthermore, according to proteomic analysis, when comparing gestational diabetes mellitus (GDM) with controls (CG), 78 proteins were significantly changed, related to complement. In GDM, Complement C3 (C3), Complement C5 (C5), C4-B (C4B), C4b-binding protein beta chain (C4BPB), and C4b-binding protein alpha chain (C4BPA) were downregulated, while C7, C9, and F12 were upregulated. 25 Plasma levels of C5a, C3a, and C5b-9 were significantly increased in patients with T2D normal albuminuria. 26 Complement C5a induces renal injury in diabetic kidney disease by disrupting mitochondrial metabolic agility and complement C3d and C5b-9 were abundantly deposited in the choriocapillaris of eyes of patients with diabetic retinopathy. 27 Complement C3 was associated with foot infections in diabetic patients, and alterations in serum complement C3 may result in reduced immune responses leading to delayed wound healing and recurrent infections. 28
In addition, response gene to complement 32 (RGC-32) in endothelial cells might lose expression in T2D retina with diabetic retinopathy (DR) features and played a key role in DR pathogenesis. 29 Proteomic analysis of diabetes genetic risk scores identified complement C2 as predictor of T2D. 30 C1q etc. could be used as potential diagnostic or therapeutic targets for diseases such as T2D. 31
In short, the delicate balance between complement activation and restriction in diabetes can be disrupted in different ways. Autoantibodies to glycosylated and glycosyl oxidized proteins can activate the classical pathway, 32–33 fructosamine activates the lectin pathway by increasing ligand–receptor binding 34 and increased arterial wall age can serve as a new epitope for mannan-binding lectin interactions. 35
Due to the characteristics of the enzymatic reaction cascade involving a series of proteins, changes in any component of complement will affect the cascade, causing problems in the balanced mechanism of complement. Affected by heat treatment, heat intolerance of any of the proteins of this system leads to changes in the TCA. Thus the fragility of the protein can be reflected by the CTT. This method offers pathological significance and will be useful in understanding the pathogenesis of diabetes, as well as predicting the risk of diabetes and possible interventions. Moreover, compared with healthy subjects of the same age, type 2 diabetic patients show reduced complement thermal resistance and increased protein fragility, which predispose them to age-related diseases.
Meanwhile, in reality, protein alterations are also associated with oxidation or other factors. Alterations in oxidation/reduction balance are associated with many pathological and physiological conditions, including aging, tumors, and diabetes. In healthy populations, more antioxidants were detected in the urine of older adults, while the opposite result was found in serum. 6 In addition, it was found that the antioxidant capacity of serum and urine was significantly lower in diabetic patients compared to healthy individuals. 7 However, any alteration in protein vulnerability due to either oxidative stress or age ultimately tends to be pathological and may be an important cause for the pathogenesis of several diseases, making this topic of great research importance. During the study, the age of the subjects in the experimental and control groups was strictly controlled to be consistent, so that the oxidative stress experienced was approximately the same, and its effects could be eliminated in the study.
This method is a blood-based assay that can be used for repeat measurements and is sensitive to age-related differences, enabling it to predict the risk of age-related diseases. Due to oxidative stress, age and other indicators all lead to functional changes through protein changes and then induce diseases. Therefore, compared with oxidative stress and other indicators, it may be more direct to reflect the degree of protein fragility by measuring the total activity of complement, which may more directly assess the redox state of some diseases and reliably reflect the disease state. Thus, it is believed that our method has the advantages of good stability, less interference, simplicity, rapidity, and sensitivity. 36 –39
Given the aging population in China, disease prevention has become a key issue, and further research on reliable indicators related to aging and geriatric diseases is of great importance to increase the health span of individuals and reduce their medical burden.
Conclusions
In summary, due to the fact that complement is not tolerant to heat and complement activation is a cascade reaction involving a series of proteins, a change in any one protein will cause a change in the reaction. In this study, a new index of protein fragility was established, and we created a CTT that uses the complement thermal resistance as a marker of protein fragility. The results indicated that the CTT was able to identify increased vulnerability of complement proteins to heat in type 2 diabetic patients, suggesting its potential clinical efficacy for predicting the risk of age-related diseases and possible interventions.
Footnotes
Authors' Contributions
L.J.H. and X.J.J. did the experimental part. L.J.H. and H.L. wrote the main article text. All authors reviewed the article.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.