
Abstract
Astragali radix (AR) and anemarrhenae rhizoma (AAR) are used clinically in Chinese medicine for the treatment of chronic heart failure (CHF), but the exact therapeutic mechanism is unclear. In this study, a total of 60 male C57BL/6 mice were divided into 5 groups, namely sham, model, AR, AAR, and AR-AAR. In the sham group, the chest was opened without ligation. In the other groups, the chest was opened and the transverse aorta was ligated to construct the transverse aortic constriction model. After 8 weeks of feeding, mice were given medicines by gavage for 4 weeks. Left ventricular ejection fraction (LVEF) and left ventricular fractional shortening (LVFS) were detected by echocardiography. Heart weight index (HWI) and wheat germ agglutinin staining were used to evaluate cardiac hypertrophy. Hematoxylin–eosin staining was used to observe the pathological morphology of myocardial tissue. Masson staining was used to evaluate myocardial fibrosis. The content of serum brain natriuretic peptide (BNP) was detected by enzyme-linked immunosorbent assay kit. The content of serum immunoglobulin G (IgG) was detected by immunoturbidimetry. The mechanism of AR-AAR in the treatment of CHF was explored by proteomics. Western blot was used to detect the protein expressions of complement component 1s (C1s), complement component 9 (C9), and terminal complement complex 5b-9 (C5b-9). The results show that AR-AAR inhibits the expression of complement proteins C1s, C9, and C5b-9 by inhibiting the production of IgG antibodies from B cell activation, which further inhibits the complement activation, attenuates myocardial fibrosis, reduces HWI and cardiomyocyte cross-sectional area, improves cardiomyocyte injury, reduces serum BNP release, elevates LVEF and LVFS, improves cardiac function, and exerts myocardial protection.
Introduction
Chronic heart failure (CHF) is a set of complex clinical syndrome due to primary myocardial injury and abnormal myocardial load caused by hypertension, coronary heart disease, and myocardial infarction (MI), which can result in ventricular filling and ejection dysfunction. 1 The morbidity and mortality of CHF are increasing year after year, posing a severe threat to human life and health. 2 Currently, clinical drug therapy is based on diuretic, angiotensin-converting enzyme inhibitor (ACEI), angiotensin II receptor antagonists (ARB), β-blockers (β-RB), mineralocorticoid receptor antagonist (MRA), and so on. 3 Nevertheless, the continued use of these drugs can bring about serious adverse reactions. For example, diuretic has electrolyte loss, hypotension, and deterioration of renal function; 4 ACEI has mild renal insufficiency, hypotension, and coughing; 5 ARB has dizziness and headache, cough, and angioneurotic edema; 6 β-RB has bronchospasm, bradycardia, and hypoglycemia; MRA has primary and secondary aldosteronism, hypertension, and hypokalemia. 7
Therefore, it is urgent to seek new treatment strategies. In the treatment of CHF, Traditional Chinese Medicine (TCM) shows mild and long-lasting efficacy, fewer side effects, and has the characteristics of multicomponent, multitarget, and multibiological processes. 8
TCM believes that qi deficiency and yang deficiency of the heart is the basic pathogenesis of CHF, in which qi is important to promote the vital activities of the human body and yang is warming substance. 9 Qi and yang work together in the body to encourage and nourish the heart. 10 If qi and yang of the heart is sufficient, it can push the body's blood to run and promote the normal metabolism of fluid. On the contrary, if qi and yang of the heart is deficient, it cannot push the blood to run and the blood will be stop in the veins, resulting in the formation of stagnant blood, which affects the heart's pumping function, thus damaging the heart and triggering CHF. 11 Therefore, the key to the treatment of CHF is to benefit qi and warm yang. 12 Astragali radix (AR)–anemarrhenae rhizoma (AAR) coupled herbs are well known for invigorating qi and elevating yang and are therapeutically utilized in Chinese medicine to treat CHF. 13
Coupled herbs are the combination of two kinds of herbs, which have synergistic effects. It is the connotation embodiment of TCM treatment based on pattern differentiation. 14 AR is the dried root of Astragalus membranaceus Fisch. ex Bunge. or A. membranaceus (Fisch.) Bge. var. mongholicus (Bge.) Hsiao. It has the effect of tonifying qi and rising yang, secures the exterior and stops sweating, and induces urination and resolves edema. 15 The main chemical components of AR include flavonoids, saponins, and polysaccharides. Astragaloside IV, a representative of AR, possesses a variety of bioactivities, such as cardioprotection, anti-inflammatory, and anticancer properties. 16 AAR is the dried rhizome of Anemarrhena asphodeloides Bge. of Liliaceae. It has the effect to clear heat and reduce fire, nourishes yin, and moistens dryness. 17
The primary chemical components of AAR include flavonoids, saponins, polysaccharides, and organic acids. According to the published research, flavonoids are among the most significant active ingredients; they have pharmacological actions that include cardioprotective, hepatoprotective, neuroprotective, anti-inflammatory, and antitumor properties. 18 AR-AAR is recorded in the “Intergrating Chinese and Western Medicine” written by Zhang Xichun and has the effect of benefiting qi and raising yang, inducing diuresis, and eliminating swelling. 19 Current pharmacological research has demonstrated that AR-AAR has the effect of enhancing the body's immunity, regulating blood pressure, and so on. 20 However, the mechanism of the AR-AAR in the treatment of CHF is unclear.
Proteomics is an important branch of systems biology; proteomics studies protein interactions in organisms from a holistic concept. 21 Yan et al. used proteomics to explore the mechanism of nutmeg-5 on myocardial fibrosis after MI and found that myristoyl-5 exerted cardioprotective effects by inhibiting the expression of extracellular matrix (ECM) receptors. 22 Wang et al. utilized proteomics to explore the mechanism of Salviae Mitiorrhizae and Cortex Moutan extract in the treatment of MI and found that Salviae Mitiorrhizae and Cortex Moutan extract exerted cardioprotective effects by regulating energy metabolism. 23 The above studies suggest that the application of proteomics to TCM can help to elucidate the mechanism of TCM in treating diseases, discover specific biomarkers, and provide new ideas for the diagnosis and treatment of disease. 24
The complement system is an crucial component of innate immunity, with physiological functions such as defense against infection, connection to adaptive immunity, and clearance of apoptotic cells and immune complexes. 25 When the complement is overactivated, it can cause damage to the body and lead to disease. 26 Previous research has indicated that complement activation plays a role in the pathophysiology of cardiovascular illnesses, such as atherosclerosis, MI, and CHF. 27 Complement component 3 (C3) in the heart is a common product of the three action pathways of complement classic, alternative, and lectin. C3 overactivation can lead to bradycardia, impaired left ventricular contractility, and atrioventricular conduction disturbances, further exacerbating myocardial injury. 28
Pål et al. 29 found that protein expression of complement component 1s (C1s), C3, and terminal complement complex 5b-9 (C5b-9) was significantly elevated, and the complement system was activated in patients with CHF compared with healthy controls, involving the classical pathway, the alternative pathway, and the lectin pathway, suggesting that the complement system is involved in the development of CHF. In addition, 30% of the immune cells that form immunity originate in the heart, that is, the autonomic nervous system, which produces hormones that affect the function of the immune system. 30 Therefore, it is expected to be a new strategy for treating CHF by regulating the body's immune balance.
This study uses transverse aortic constriction (TAC) to construct CHF mouse model and to observe the cardioprotective effects of AR, AAR, and AR-AAR in CHF model mice. The potential mechanism of AR-AAR in treating CHF was analyzed and verified by proteomics.
Materials and Methods
Instruments and reagents
Shanghai Enzyme-linked Biotechnology Co., Ltd., provided the brain natriuretic peptide (BNP) enzyme-linked immunosorbent assay (ELISA) kit (lot: E20230602-20519A). Sigma–Aldrich (Shanghai) Trading Co., Ltd., was the supplier of dithiothreitol (DTT) (lot: D0632). Sigma–Aldrich (Shanghai) Trading Co., Ltd., was the supplier of iodoacetamide (IAA) (lot: I1149). Beijing Biosynthesis Biotechnology Co., Ltd., was the supplier of the C1s antibody (lot: bs-15088R). Shanghai Qingmu Biotechnology Co., Ltd., provided the complement component 9 (C9) antibody (lot: DF3964). Beijing Biosynthesis Biotechnology Co., Ltd., was the supplier of the C5b-9 antibody (lot: bs-2673R). Beijing Mike Biotechnology Co., Ltd., provided the immunoglobulin G (IgG) kit (Batch No: E026-1).
The Sartorius firm in Germany was the source of the electronic analytical balance (model: BSA124S). Shanghai Luxiangyi Centrifuge instrument Co., Ltd., was the source of the desktop centrifuges (model: TD4). Hunan Xiangyi Company (model: H2050R) was the source of the low-temperature high-speed centrifuge. Beijing Mike Biotechnology Co., Ltd., was the source of the automatic biochemical analyzer (model: C800). A fully automatic snowflake ice maker (model: IMS-20) was bought from Changshu Xueke Electric Co., Ltd. Shenzhen Mindray Biomedical Co., Ltd., was the source of the microplate reader (model: MR-96A).
Thermo Fisher Scientific Shier Technology Company was the seller of the high-performance liquid chromatograph (model: EASYnLC1200). Thermo Fisher Scientific Shier Technology Company was the seller of the mass spectrometer (model: Q-Exactive HFX). Beijing Renewal Biotechnology Co., Ltd., sold the chromatographic column (model: ReprosilPur 120 C18AQ). Shanghai Jingxin Industrial Development Co., Ltd., offers a cell ultrasonic crusher (model: JY96-IIN). Shanghai Yiheng Scientific Instrument Co., Ltd., was the seller of the constant temperature shaker (model: THZ-100).
Plant material
Medicinal granules of AR (2 g per bag, equivalent to 10 g of AR, lot: 1039052) and AAR (2.5 g per bag, equivalent to 10 g of AAR, lot: 1070712) were purchased from Guangdong Yifang Pharmaceutical Co., Ltd.
Animals
The Fourth Military Medical University's experimental animal center provided SPF-grade male C57BL/6 mice (body weight 20–25 g), with the production number SCKX (military) 2020-001 and use license number SYXK (Shaanxi) 2019-001. The Shaanxi University of Chinese Medicine's Ethical Review Board authorized the animal experimental procedure (No. SUCMDL2022104002). The mice were kept in individual cages, fed at a consistent temperature and humidity level, and exposed to light for 12 hours every day.
Construction of CHF model and experimental design
A clean laboratory operating table served as the platform for the TAC operation. A combination of 0.5–1.0 L/min 100% O2 and 2% isoflurane was used to anesthetize the mice. An animal ventilator set to cycle at 125–150 breaths per minute and 0.1–0.3 mL tidal volume was attached to a PE90 endotracheal tube. The degree of anesthesia was verified by whether the mice had righting reflex or not. After the mice were anesthetized, they were operated to open the chest on the operating table to identify the transverse aorta. Two loose knots are tied around the transverse aorta and a small piece of a 27-gauge blunt needle is placed parallel to the transverse aorta. Then, the two nodes are rapidly struck, resulting in a 0.4 mm contraction of the artery. In the sham group, the chest was opened without ligation.
In the other groups, the chest was opened and the transverse aorta was ligated to construct the TAC model. After the surgery, the chest cavity was sewn with a 6.0 Prolene suture. 31 After 8 weeks, the mice were divided into 5 groups at random, each including 12 animals. The groups were called the sham group (0.9% saline), model group (0.9% saline), AR group (converted to mouse dose according to human daily intake of 30 g), AAR group (converted to mouse dose according to human daily intake of 15 g), and AR-AAR group (converted to mouse doses by 30 g AR and 15 g AAR per day given to humans). They were each given continuous gavage for 4 weeks.
Echocardiography was used to evaluate the cardiac function
After 4 weeks of gavage, the chest hair of mice was removed. The mice were anesthetized with a mixed gas of 2% isofluorocarbon and 0.5–1.0 L/min 100% O2 and connected to the Vevo 2100 imaging system to evaluate the heart function. Left ventricular ejection fraction (LVEF) and left ventricular fractional shortening (LVFS) were measured by M-mode of middle nipple in mice.
The heart weight index and wheat germ agglutinin staining were used to evaluate cardiac hypertrophy
Mice were anesthetized with 2% pentobarbital sodium after echocardiographic examination. The chest cavity was opened and the heart was removed immediately and then washed with 1 × phosphate-buffered saline. The heart weight to body weight (HWI) ratios were calculated after the hearts were weighed to look for signs of cardiac hypertrophy.
The heart tissues were fixed in 4% paraformaldehyde solution. Then, paraffin sections were dewaxed to water and antigen repair. The cardiomyocyte cross-sectional area was visualized by wheat germ agglutinin (WGA) staining, and images were taken under a fluorescence microscope.
Hematoxylin–eosin staining was used to observe the abnormal morphology of cardiac tissue
Cardiac tissues were fixed in 4% paraformaldehyde solution, dehydrated with ethanol gradient, and made into 5 μm thick sections. Hematoxylin–eosin (HE) staining was used to evaluate the changes in mice heart morphology and injury.
Masson staining was used to observe the degree of cardiac fibrosis
The dehydrated myocardial tissue was embedded in paraffin and made into 5 μm thick sections. The degree of myocardial fibrosis in mice was evaluated by Masson staining. An intelligent biomicroscope was used to enlarge the micrograph to 400 × . Quantitative digital image analysis system (Image Pro Plus 6.0 software) was used to quantify the percentage of blue collagen fiber area to total area.
ELISA kit was used to detect serum BNP content
Mice orbital blood was collected and rested at room temperature for 30 minutes. Blood was centrifuged at 3500 rpm for 10 minutes, and the supernatant was separated for detecting the BNP level, according to the instructions of mouse ELISA kit.
Immunoturbidimetry was determined by the serum IgG content
Reagents were prepared according to the instructions of IgG determination kit and the remaining mouse serum was taken for computer detection. The automatic biochemical analyzer was set according to the basic parameters of the instrument.
Proteomics discusses the mechanism of AR-AAR
Sample preparation
The myocardial tissues of the model group and the AR-AAR group were taken out from the refrigerator at −80°C, and one fourth of samples were weighed and 300 μL RIPA lysate was added to the new eppendorf tube (EP). After grinding with steel balls at low temperature, ultrasonic treatment was performed in a cell ultrasonic instrument for 20 minutes. After the tissues were fully broken, they were centrifuged at 12,000 rpm at 4°C for 10 minutes, and the supernatant was transferred to a new EP tube. Protein concentration was determined by BCA quantitative kit. Weigh 100 μg of each sample group, dilute with RIPA lysate to 1 mg/mL, add five times of precooled acetone to the samples, mix well, and leave overnight at −20°C, centrifuge at 4°C for 10 minutes, and discard the supernatant. Then, add 200 μL precooled 80% acetone to moisten and wash the precipitate for two to three times and centrifuge at 4°C for 10 minutes.
After the precipitate is dried, add 100 μL of protein complex solution and ultrasonic wave in water bath for 3 minutes to dissolve the protein precipitate. After dissolution, add DTT to 5 mM, incubated with shaking at 55°C for 20 minutes, and when the sample is allowed to stand at room temperature, add IAA to 15 mM and react in the dark for 30 minutes. According to the trypsin:protein ratio of 1:50, trypsin was mixed with the sample and incubated overnight by shaking. Then, 300 μL of 2% trifluoroacetic acid was slowly added and mixed and centrifuged at 12,000 rpm at 4°C for 10 minutes to extract the polypeptide in the precipitate, and the extraction was repeated for two to three times, combine the supernatant fractions, centrifuge the supernatant into a new EP tube to obtain the peptide samples, the peptide samples were eluted by a C18 column, activated and dried, and then set aside.
Nano Liquid Chromatography-Tandem Mass Spectrometry analysis
Each sample is collected from 2 μg of total peptides, separated by the nano-ultra performance liquid chromatography liquid-phase system EASY-nLC1200 and combined with the Q-Exactive HFX. The color separation was performed using 100 μm ID × 15 cm reverse column color (1.9 μm, ReproSil-Pur 120 C18-AQ; Dr. Maisch). The flow phase uses the ethanol–water–methyl acid system, in which the fluid phase A is a 0.1% methyl–98% water solution (ethanol is 2%), and the B is relative to 0.1% ethanol–80% solution (water is 20%). After the column is balanced at 100% A phase, the sample is automatically inserted by the sampler directly to the column and then separated by the color column gradient, with flow speed of 300 nL/min and graduation time of 120 minutes. Fluid phase B ratio: 2%–5% lasting 2 minutes, 5%–22% lasting 88 minutes, 22%–45% lasting 26 minutes, 45%–95% lasting 2 minutes, and 95% lasting 2 minutes.
The mass spectral analysis uses the data-dependent acquisition model, with a total analysis duration of 120 minutes, using the positive ion detection model. The full scan range is 350–1600 m/z with a resolution of 120k (at 200 m/z), the Automatic gain control (AGC) is 3E6, the maximum ion injection time (max IT) is 50 ms, and the 20 ions with the highest intensity (top 20) in the first scan are scanned with HCD cracks after quaternary pole filtration. The isolation window is 1.2 m/z, the standardized impact power (NCE) is 27%, the AGC is 1E5, and the max IT is 110 ms. Secondary scan resolution is 15k. Depending on the peak width of the spectrum, the dynamic exclusion time is set to 45 seconds; a single charge and >6 values of ions are not secondary scanned.
Identification of differential proteins
The source data file is analyzed using the Proteome Discoverer software (PD) (version 2.4.0.305; Thermo Fisher Scientific) and the built-in Sequest HT search engine. Database matching parameter settings: databases: uniprot-Mus musculus-reviewed-10090-2022-11.fasta; enzyme: trypsin. Fixed modification: carbamidomethyl/+57.021 Da (C); variable modification: acetyl/+42.011 Da (N-terminus) oxidation/+15.995 Da (M); max missed cleavages: two; peptide tolerance: 10 ppm; Tandem Mass Spectrometry (MS/MS) tolerance: 0.02 Da; peptide and peptide-spectrum matches (PSM) false discovery rate (FDR): ≤0.01; protein quantification: unique peptide+razor peptide; normalization: total peptide amount.
Statistical analysis of proteomics
Protein was extracted from three myocardial tissues in the model group and the AR-AAR group. The fold change (FC) of protein was calculated according to the average relative quantitative value of protein in the two groups, and whether there was significant difference in protein was calculated according to the detection frequency of protein in the two groups (p < 0.05). The criteria for screening differentially expressed protein (DEP) are as follows: unique peptide ≥1, FC ≥1.2 or ≤0.83, and p-value <0.05.
Western blot determined the expression of C1s, C9, and C5b-9 proteins in cardiac tissue
Myocardial tissue of mice was mixed with the precooled RIPA lysate (containing 1% protease inhibitor and 1% phosphatase inhibitor). The tissue was then allowed to decompose completely on ice for 30 minutes, suspended once every 5 minutes, and centrifuged for 5 minutes at 4°C and 12,000 g. The tissue protein extract was obtained from the supernatant. Protein concentration was determined by BCA protein quantitative kit, and protein samples were made after heating denaturation.
The prepared protein sample was added to 10% sodium dodecyl sulfate–polyacrylamide gel electrophoresis (SDS-PAGE) for electrophoresis. After electrophoresis, transfer the gel with the protein sample to polyvinylidene fluoride membrane by wet method, seal it in 5% skimmed milk for 2 hours at room temperature, then add primary antibodies C1s, C9, and C5b-9 for incubation at 4°C overnight, rinse for 30 minutes, and then add secondary antibodies and incubate at 37°C for 2 hours. The strip with protein was put into the automatic chemiluminescence imager, developed with ultrasensitive enhanced chemiLuminescence reagent, scanned with quantitative image analysis software after taking pictures, and the gray value of the strip was calculated for statistical analysis.
Statistical analysis
The data are expressed as mean ± standard deviation and were statistically analyzed with GraphPad Prism 8 software. The analysis of variance (ANOVA) was employed for the overall comparison of means among experimental groups, followed by Tukey's method for pairwise comparison. p < 0.05 was considered statistically significant.
Results
AR-AAR significantly enhances the heart function in CHF model mice
As shown in Figure 1, the echocardiographic results showed that LVEF and LVFS in the model group decreased significantly (p < 0.01) compared with the sham group. Compared with the model group, LVEF in the AR group increased significantly (p < 0.05), and LVFS showed an upward trend, but there was no statistical difference. LVEF and LVFS in the AAR group showed an upward trend, but there was no statistical difference. LVEF and LVFS in the AR-AAR group increased significantly (p < 0.01).

AR-AAR significantly enhances the heart function of CHF model mice.
AR-AAR markedly reduces cardiac hypertrophy in CHF model mice
As shown in Figure 2, the heart morphology of mice in each group showed that compared with the sham group, the HWI in the model group was significantly increased (p < 0.01). Compared with the model group, the HWI in the AR group decreased significantly (p < 0.05). The HWI in the AAR group showed a downward trend, but there was no statistical difference. The HWI in the AR-AAR group decreased significantly (p < 0.05).
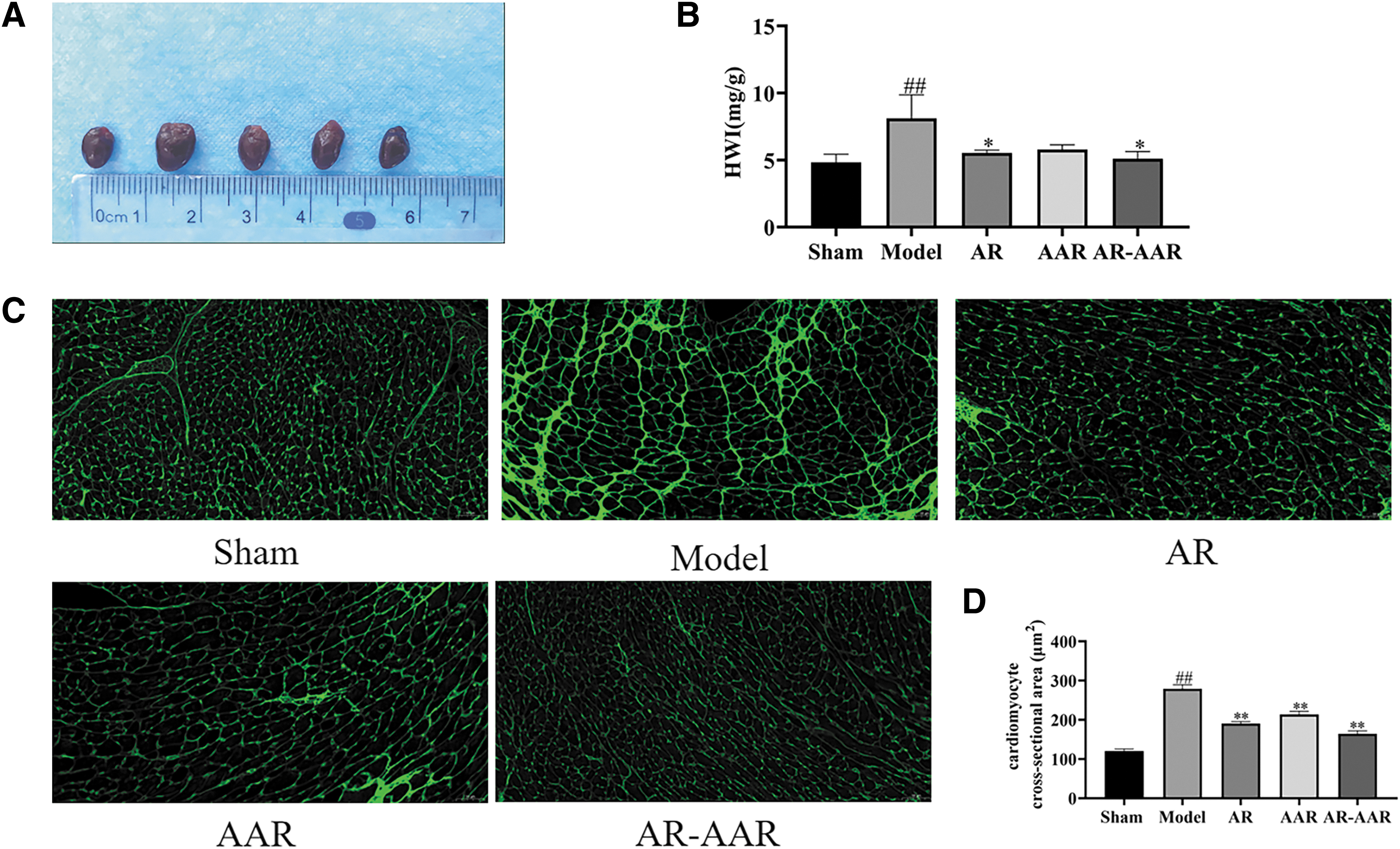
AR-AAR markedly reduces the cardiac hypertrophy in CHF model mice.
As shown in Figure 2, WGA staining of mice in each group showed that compared with the sham group, the cardiomyocyte cross-sectional area in the model group was significantly increased (p < 0.01). Compared with the model group, the cardiomyocyte cross-sectional area in the AR, AAR, and AR-AAR groups significantly decreased (p < 0.01).
AR-AAR improves myocardial pathological morphology in CHF model mice
As shown in Figure 3, the results of HE staining showed that compared with the sham group, the myocardial fibers in the model group were thicker and disordered, and there were a lot of inflammatory cells infiltrating and blood vessels dilating between tissues. Compared with the model group, the myocardial fibers in the AR group were disordered and inflammatory cells infiltrated between tissues. In the AAR group, the myocardial arrangement was orderly, and inflammatory cells infiltrated between tissues. In the AR-AAR group, myocardial fibers were arranged neatly, and a small amount of inflammatory cells infiltrated between tissues.
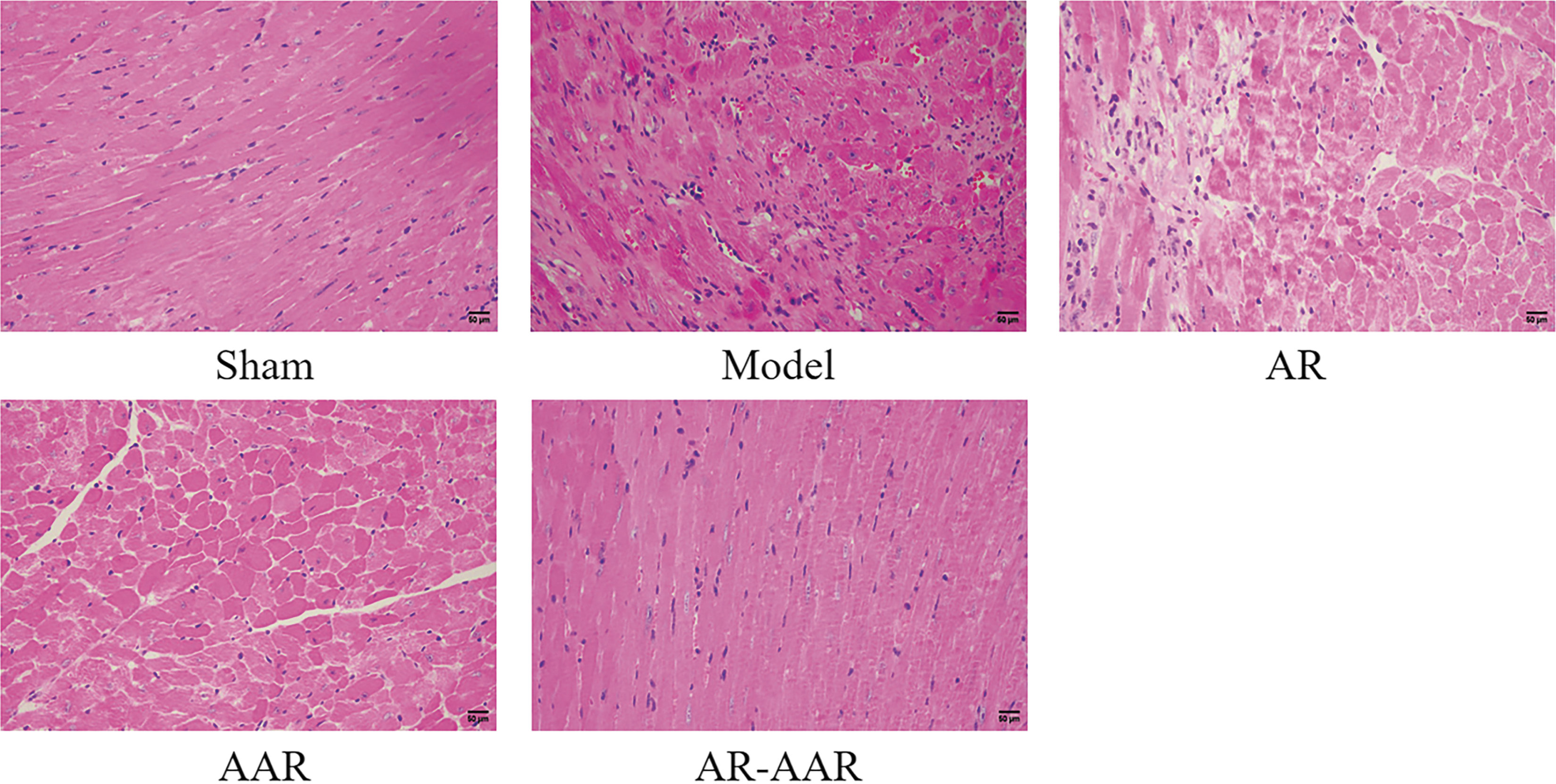
AR-AAR improves the myocardial pathological morphology in CHF model mice. HE staining (n = 3). HE, hematoxylin–eosin. Color figures are available online.
AR-AAR significantly inhibits myocardial fibrosis in CHF model mice
As shown in Figure 4, Masson staining results showed that blue collagen fibers in the model group increased significantly (p < 0.01) compared with the sham group. Compared with the model group, blue collagen fibers in the AR, AAR, and AR-AAR groups were significantly reduced (p < 0.01).
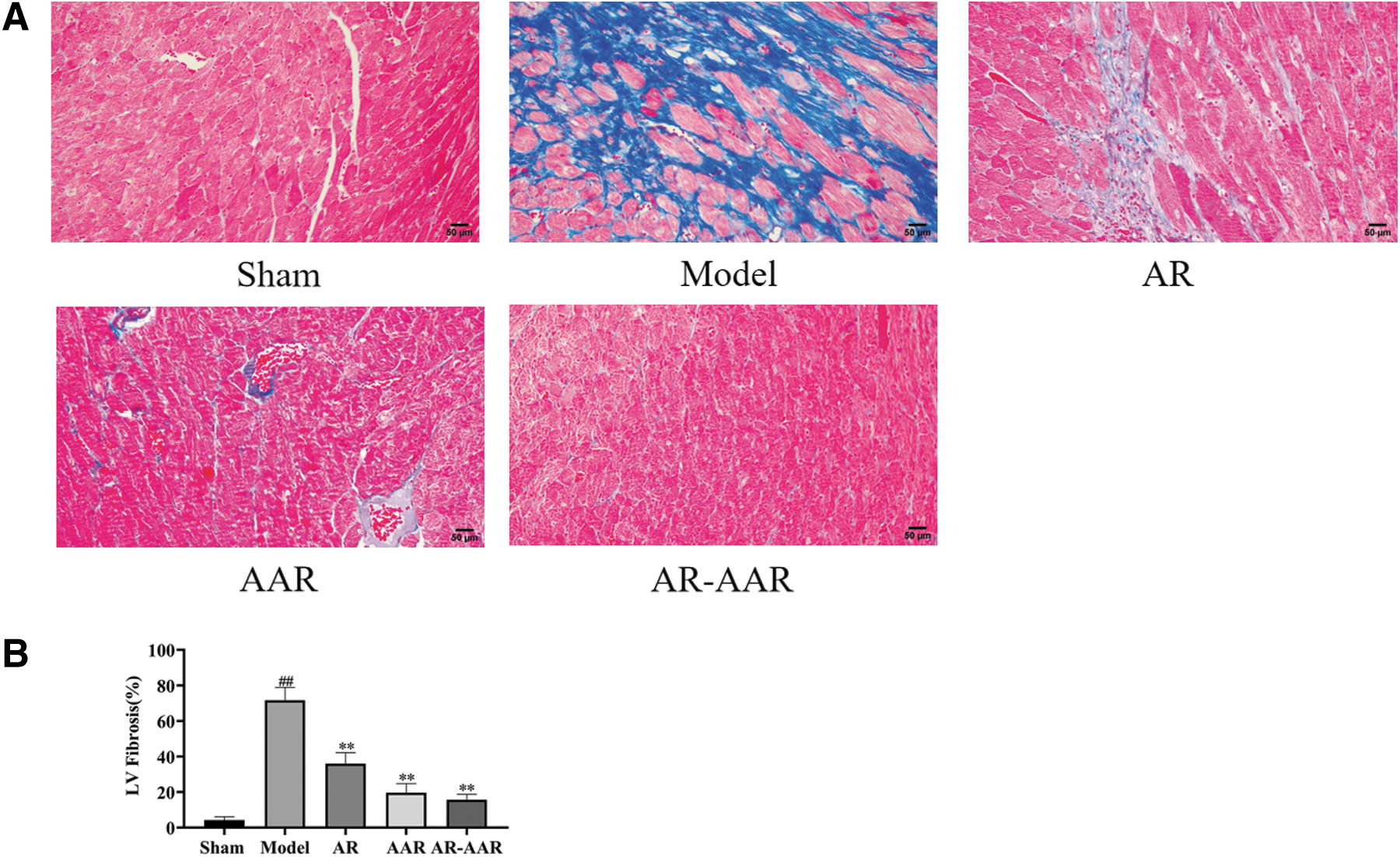
AR-AAR significantly inhibits the myocardial fibrosis in CHF model mice.
AR-AAR markedly reduces the level of serum BNP and IgG in CHF model mice
As shown in Figure 5, the results of ELISA showed that compared with the sham group, BNP in the model group increased significantly (p < 0.05). Compared with the model group, BNP in the AR and AAR groups showed a downward trend, but there was no statistical difference. BNP in the AR-AAR group decreased significantly (p < 0.01).

AR-AAR markedly reduces the serum BNP and IgG content in CHF model mice.
As shown in Figure 5, the results of immunoturbidimetry showed that compared with the sham group, IgG in the Model group was significantly increased (p < 0.01). Compared with the model group, the content of serum IgG in the AR group decreased significantly (p < 0.05). The content of serum IgG in the AAR group has a downward trend, but there was no statistical difference. The content of serum IgG in the AR-AAR group decreased significantly (p < 0.01).
Proteomics
Identification of DEPs
A total of 2758 proteins were analyzed by Liquid Chromatography-Tandem Mass Spectrometry for label-free quantitative analysis of myocardial tissues from the model group and the AR-AAR group. Screening DEPs with “unique peptide ≥1, FC ≥1.2, and p < 0.05 was upregulated protein. Unique peptide ≥1, FC ≤0.83, and p < 0.05 are downregulated protein” as the standard. Unique peptide ≥1, FC ≤0.83, and p < 0.05 are downregulated protein. A total of 62 DEPs were screened out, including 36 upregulated proteins and 26 downregulated proteins (Fig. 6A). Volcano analysis of DEPs, red represents the protein that is significantly up-regulated and blue represents the protein that is significantly down-regulated, which is used to show the difference of protein expression level between the two groups (Fig. 6B). Hierarchical clustering analysis of DEPs, red indicates high expression of protein and blue indicates low expression of protein, which is used to indicate the affinity of differential proteins (Fig. 6C).
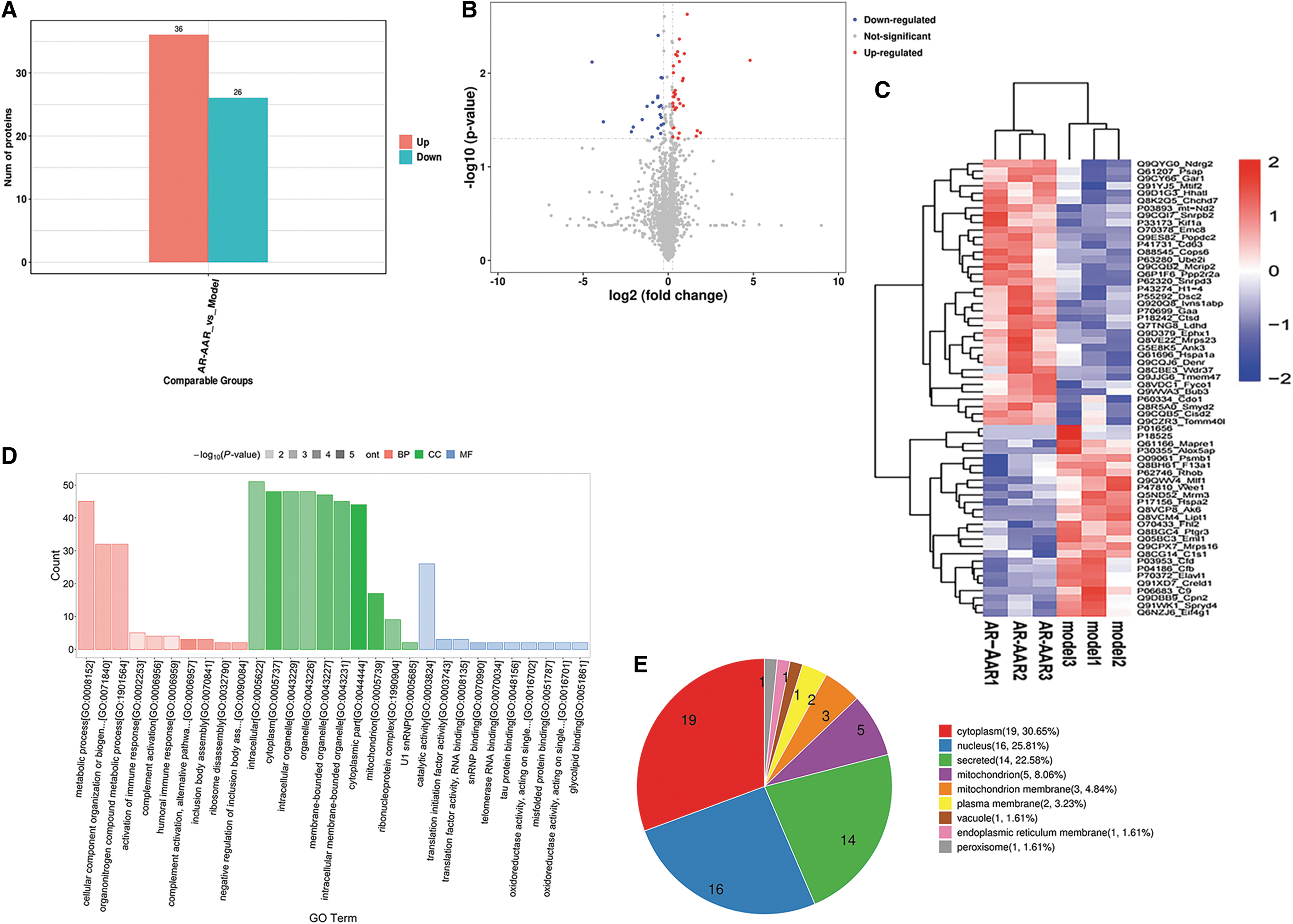
Proteomics.
DEP enrichment analysis
DEPs were analyzed by Gene Ontology (GO) annotation enrichment analysis, subcellular location analysis, Kyoto encyclopedia of genes and genomes (KEGG), and PPI network analysis. GO analysis showed that DEPs were related to biological processes such as complement activation, alternative pathway of complement activation, activation of immune response, humoral immune response, cellular component organization, or biogenesis (Fig. 6D).
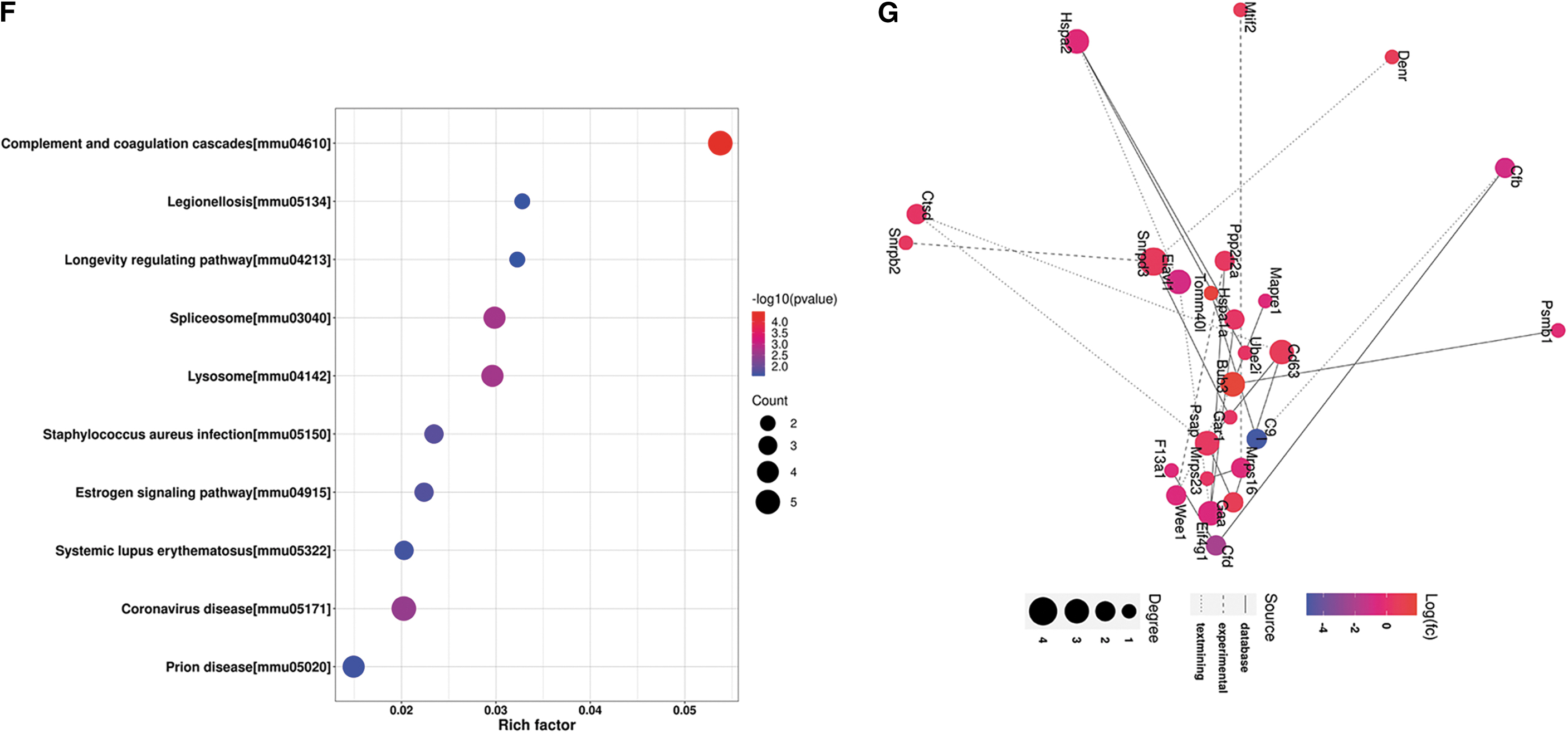
Subcellular location analysis showed that DEPs are mainly distributed in the cytoplasm (30.65%), nucleus (25.81%), mitochondrion (8.06%), and mitochondrion membrane (4.84%) (Fig. 6E). KEGG analysis showed that DEPs were mainly involved in signal pathways such as complement and coagulation cascades (mmu04610), lysosome (mmu04142), longevity regulating pathway (mmu04213), spliceosome (mmu03040), estrogen signaling pathway (mmu04915), and coronavirus disease (mmu05171) (Fig. 6F). The analysis of PPI network construction shows that DEPs are highly correlated with Snrpd3, Gar1, Elavl1, Denr, and Snrpb2 genes (Fig. 6G).
AR-AAR significantly suppresses the expression of C1s, C9, and C5b-9 proteins in cardiac tissue of CHF model mice
As shown in Figure 7, the results of Western blot showed that compared with the sham group, C1s, C9, and C5b-9 proteins in the model group increased significantly (p < 0.05). Compared with the model group, the protein C1s and C5b-9 in the AR and AAR groups showed a downward trend, but there was no statistical difference. In the AR-AAR group, C1s, C9, and C5b-9 proteins decreased significantly (p < 0.05). Each western blot image with the MW markers is shown Supplementary Figure S2.
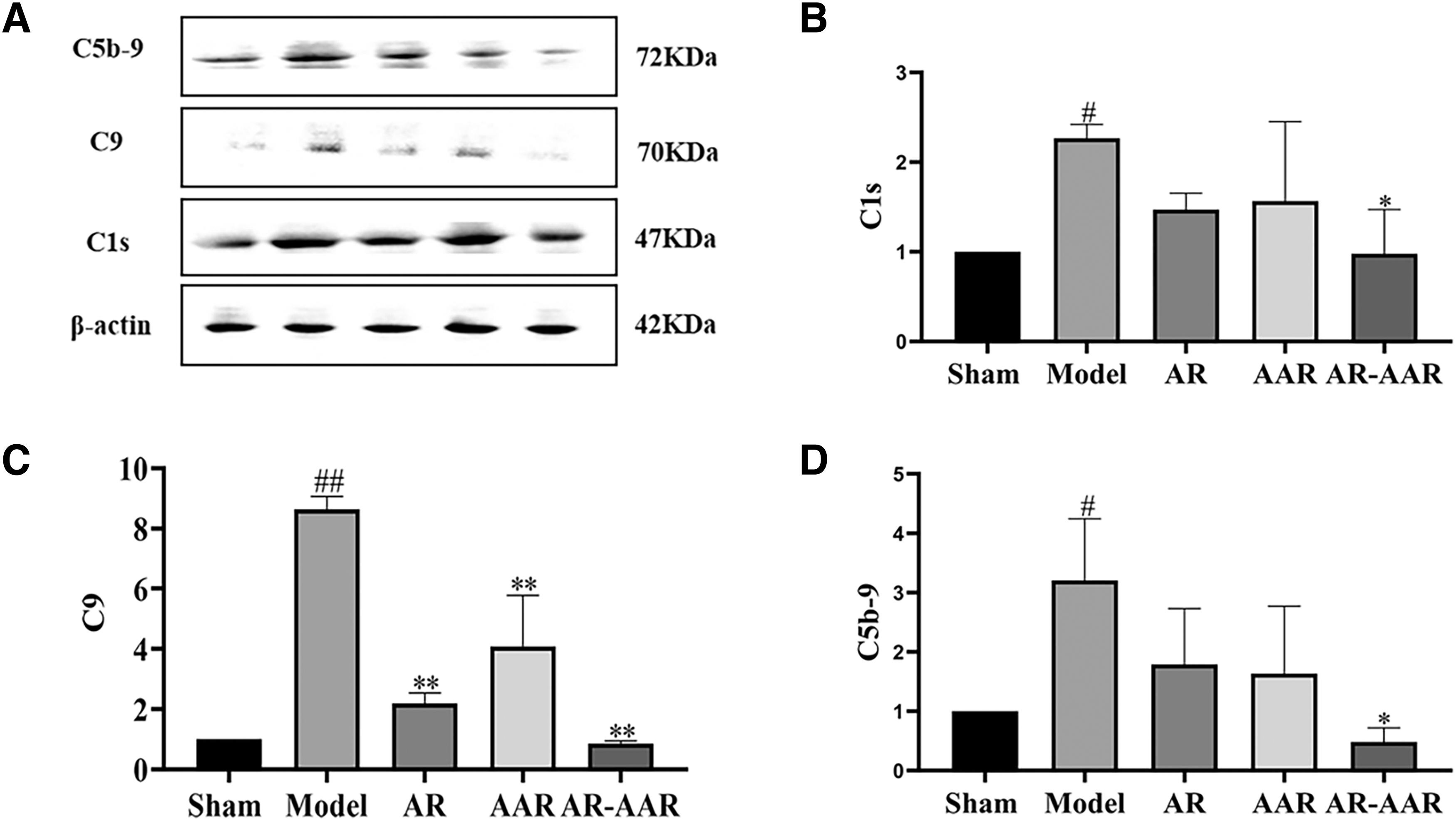
AR-AAR significantly suppresses the expression of C1s, C9, and C5b-9 proteins in cardiac tissue of CHF model mice.
Discussion
CHF is the end stage of cardiovascular disease, and the heart pumping function has been unable to meet the metabolic needs of the whole body, thus forming a vicious circle to further aggravate CHF. 32 The key to the TAC model constructed in this study is to narrow the transverse aortic diameter, which increases the cardiac load and initiates the process of myocardial hypertrophy right after surgery. Compensatory hypertrophy has a role in maintaining cardiac function at early stage, which is beneficial for enhancing myocardial contractility, decreasing ventricular wall tension, and maintaining cardiac output. However, the sustained pressure overload leads to the stretching of cardiomyocytes, the deposition of collagen fibers in myocardial interstitium, the abnormal dilation of ventricles, a large number of edema and coagulation necrosis of cardiomyocytes, which constantly stimulates the synthesis and release of BNP from myocardial cells, promotes ventricular remodeling, and gradually weakens the compensatory response, and finally enters the decompensated period, causing CHF. 33
Currently, most of the CHF studies use the TAC model. 34 –36 The results showed that in the model group, myocardial fibrosis increased, HWI increased, LVEF and LVFS decreased, inflammatory cells in myocardial tissue increased, serum BNP released increased, and cardiac function was damaged. After 4 weeks of intervention with AR, AAR, and AR-AAR, myocardial fibrosis decreased, HWI decreased, LVEF and LVFS increased, inflammatory cells in myocardial tissue decreased, serum BNP released decreased, and cardiac function improved.
Cardiac function is a key index in clinical and scientific research. Echocardiography can detect abnormal movement and structural changes of the heart and is one of the main methods to measure the cardiac function. 37 LVEF is the percentage of the blood volume pumped out by the heart in one beat to the end-diastolic volume of the ventricle. LVFS is the percentage of the difference between the left ventricular end-diastolic inner diameter and the left ventricular end-systolic inner diameter. LVEF and LVFS are important indicators for evaluating left ventricular systolic function and key indicators for determining the severity of CHF. 38
When CHF occurs, the contractile function of cardiomyocytes is weakened, which leads to a weakening of the heart's contractile function, causing a decrease in LVFS. At the same time, the left ventricle is not pumping enough and fails to maintain normal cardiac circulation, which leads to a decrease in LVEF. On the contrary, when LVFS and LVEF increase, it indicates that the pumping function of the heart is restored and cardiac function is enhanced. 39 The results showed that LVEF and LVFS of the AR, AAR, and AR-AAR groups have been improved in different degrees compared with the model group. It is suggested that AR, AAR, and AR-AAR can enhance the myocardial contractility of CHF mice and play a role in myocardial protection.
Cardiac hypertrophy is an adaptive response of myocardial tissue caused by physiological stimuli such as exercise and pregnancy, and pathological stimuli such as increased pressure–volume loading in the heart. HWI and WGA staining are important parameters for measuring myocardial hypertrophy. 40 Persistent pressure overload leads to irreversible pathological cardiac hypertrophy, which eventually leads to CHF. 41 As the major pathological feature in the occurrence and development of CHF, cardiac hypertrophy can directly affect the cardiac function. 42
The findings demonstrated that in contrast to the model group, the HWI and cardiomyocyte cross-sectional area of the AR, AAR, and AR-AAR groups are all reduced to varying degrees. Previous studies have shown that astragalosides (AST) and total saponins of anemarrhena (TSA) can significantly reduce the heart rate, inhibit cardiac hypertrophy, prolong the survival time of running, swimming, and hypoxia in mice, and enhance the cold and heat tolerance of mice. 43,44 It is suggested that the myocardial protective effects of AR and AAR on CHF may be related to the therapeutic effects of AST and TSA on cardiac hypertrophy in CHF mice.
Caused by the deposition of ECM proteins, myocardial fibrosis is a typical pathophysiological hallmark of cardiovascular disorders. It represents the process of heart repair or maladjustment. 45 ECM is a highly dynamic three-dimensional network scaffold structure, which is mainly composed of fibrous collagen. 46 After TAC-induced injury and stimulation, the changes of matrix composition and structure, the induction of cytokines, the increase of mechanical stress, and the release of neurohormonal factors can all promote the transformation of cardiac fibroblasts (CFs) into myofibroblast (MFs). 47 Excessive activation of CFs and MFs can lead to the deposition of collagen fibers, produce a large number of structural and unstructured ECM proteins, and formation of stable scars, causing myocardial fibrosis and aggravate CHF. 48
Masson staining is an authoritative and classic technical method for collagen fiber staining. After staining, muscle fibers can be red and collagen fibers can be blue. Therefore, myocardial fibrosis was observed by Masson staining in this study. The results showed that AR, AAR, and AR-AAR could significantly improve myocardial fibrosis in CHF mice in different degrees. It is suggested that AR, AAR, and AR-AAR may inhibit the transformation of CFs into MFs and reduce the deposition of collagen fibers.
BNP, also known as B-type natriuretic peptide, is a polypeptide containing 32 amino acids. It is a cardioprotective hormone produced by myocardial stretching caused by pressure or volume overload. It has the functions of expelling sodium, promoting diuresis and vasodilation, and is the gold standard for clinical diagnosis and prognosis of CHF. 49 BNP in normal heart is mainly secreted by ventricular myocytes on demand and participates in cardiovascular homeostasis. 50 In the early stage of CHF, the decrease in cardiac output triggers the activation of the renin–angiotensin–aldosterone system (RAAS) and sympathetic nervous system (SNS), as a compensatory mechanism to maintain the circulatory system. In the middle and late stage of CHF, the long-term activation of RAAS and SNS leads to tissue remodeling, and BNP acts as a neurohumoral regulator to resist the adverse effects of neurohormonal system activation.
At this time, the body enters the decompensation stage from compensatory stage. BNP is secreted and produced in large quantities, but the continuous activation of RAAS will hinder the beneficial effects of BNP. 51 The results showed that BNP in the AR, AAR, and AR-AAR groups decreased in different degrees after treatment. Previous studies have shown that AR can inhibit the activation of RAAS, reduce the pressure of ventricular wall, delay the decline of myocardial contraction function, and reduce the release of BNP. 16 AAR inhibited the concentration of plasma catecholamine and suppressed the SNS activity. 52 It is suggested that the synergistic inhibition of SNS by AAR on the basis of RAAS inhibition by AR may be related to the joint cardioprotective effects of AR and AAR in the treatment of CHF.
This work investigated the possible mechanism of AR-AAR in the therapy of CHF using proteomics. The results showed that proteomics identified 62 DEPs, of which 36 were upregulated and 26 were downregulated. GO analysis showed that DEPs were related to biological processes such as complement activation, alternative pathway of complement activation, activation of immune response, humoral immune response, cellular component organization, or biogenesis (Fig. 6D). Subcellular location analysis showed that DEPs are mainly distributed in the cytoplasm (30.65%), nucleus (25.81%), mitochondrion (8.06%), and mitochondrion membrane (4.84%) (Fig. 6E).
KEGG analysis showed that DEPs were mainly involved in signal pathways such as complement and coagulation cascades (mmu04610), lysosome (mmu04142), longevity regulating pathway (mmu04213), spliceosome (mmu03040), estrogen signaling pathway (mmu04915), and coronavirus disease (mmu05171) (Fig. 6F). According to the results of GO and KEGG analyses, AR-AAR can downregulate C1s and C9 complement proteins and regulate the biological process of complement activation. It is suggested that AR-AAR may be related to complement the classical pathway in the treatment of CHF.
Studies have shown that cardiac immunity accounts for 30% of human immunity. 53 Cardiac immune cells are not only involved in cardiac development, physiology, and aging but also involved in regulating ventricular structure and function. 54 B cell activation is the process of being activated in response to the immune stimulus and secreting specific antibodies. It is an important part of the immune response. 55 The complement system is a key component of innate immunity that plays an important role in the developmental process of CHF. C1s is the constituent protein of C1 that activates the promoter of the classical pathway of complement and is important for blocking the entire complement system. C9, by binding C6, C7, and other complement proteins to form C5b-9, directly attacks the cardiomyocyte membrane leading to cardiomyocyte necrosis, causing left ventricular remodeling and aggravating CHF. 28
Therefore, the inhibition of B cell activation and the expression of C1s, C9, and C5b-9 are expected to be a novel therapeutic strategy for CHF. Li et al. analyzed the serum from 20 healthy subjects and 60 CHF patients and showed that the level of C5b-9 was significantly higher in serum from CHF patients compared with healthy subjects. 56 Oliveira et al. compared the serum from 12 healthy subjects with 36 patients with CHF and showed that the level of C5b-9 was significantly higher in patients with CHF compared with healthy subjects. 57 The above studies illustrate that the complement system is activated in patients with CHF, initially suggesting that our intervention on complement activation may be a new way to treat CHF. The TAC model constructed in this article causes sporadic death of myocardial cells, interacts with antigen-presenting cells such as B cells, and causes B cells to differentiate into plasma cells and produce specific antibodies. 58
It has been shown that the large amounts of IgG are deposited in the hearts of CHF patients. 59 IgG easily spreads to the extravascular space and activates the classical pathway of the complement system. 60 Therefore, we hypothesized that in CHF mice, the activation of the classical pathway of complement may rely on the activation of B cells into plasma cells producing IgG antibodies that bind to complement components. The experimental results showed that the serum IgG level and the expression of C1s, C9 and C5b-9 proteins in myocardial tissue in the model group were significantly increased, which confirmed the correctness of the conjecture. After treatment with AR, AAR, and AR-AAR, IgG and complement-related proteins decreased significantly (p < 0.05). It is suggested that AR-AAR can inhibit the activation of B cells in CHF mice, thus inhibiting the activation of the classical pathway of complement.
The proteomics KEGG results suggested that the DEPs were most relevant to the “complement and coagulation cascades” signaling pathway, which was enriched to the “C1s, C9” DEPs. The diagram of the “complement and coagulation cascades” signaling pathway is shown Supplementary Figure S1. Current studies have shown that after myocardial tissue injury, cardiomyocytes release a class of substances into the interstitial space and the blood circulation, which has been termed “damage associated molecular pattern (DAMP).” DAMP is recognized by Toll-like receptors (TLRs), which interact with antigen-presenting cells (e.g., B cells) and cause B cells to activate into plasma cells that produce specific antibodies, including IgG and IgM.
But, IgG easily diffuses into the extravascular space and combines with complement proteins to activate the complement classical pathway, inducing immune response, causing endothelial dysfunction, vascular remodeling, and exacerbating CHF. 61 Therefore, we speculate that the molecular mechanism of AR-AAR in the treatment of CHF may be to inhibit the recognition of DAMP and TLRs, thereby inhibiting the activation of B cells to produce IgG, modulating the C1s/C9/C5b-9 signaling pathway and inhibiting the biological process of “immune stress-complement activation,” which improves the cardiac function and thus exerts cardioprotective effect.
Western blot results suggested that AR could significantly reduce the expression of C9, and there was a tendency to reduce the expression of C1s and C5b-9, but there was no significant difference. AAR had a tendency to reduce the expression of C1s and C5b-9, but there was no significant difference. But when co-administered with AR-AAR, it could significantly reduce the expression of C1s, C9, and C5b-9, which indicated that the effect of combining the two medicines was better than that of single medicine, suggesting that AR and AAR might produce synergistic effects to reduce the complement protein and play a myocardial protective effect.
In this study, we found that the complement system was activated in CHF model mice, and the complement system was inhibited after AR, AAR, and AR-AAR treatment, thus exerting cardioprotective effects. It is initially suggested that monitoring the immune function status of patients in the daily treatment of CHF patients is helpful in observing the severity and efficacy of CHF and also suggests that intervention on complement activation may become a new avenue for the treatment of CHF.
The clinical treatment of Chinese medicine often adopts the use of multimedicine combinations to enhance clinical efficacy, with the therapeutic characteristics of multitargets and multibiological processes, which may be caused by the synergistic effect between medicines. The efficacy of AR and AAR in the treatment of CHF in Chinese medicine clinics is accurate and has a long history, but the interaction between the two medicines for the treatment of CHF is unclear and the interaction mechanism is unknown. Later, we will analyze the interaction and the interaction mechanism of the AR and AAR compatibility for the treatment of CHF, so as to improve our study.
Conclusions
The study demonstrated that AR-AAR inhibits the expression of C1s, C9, and C5b-9 by inhibiting the production of IgG antibodies from B cell activation, which further inhibits the complement activation, attenuates myocardial fibrosis, reduces HWI and cardiomyocyte cross-sectional area, improves cardiomyocyte injury, reduces serum BNP release, elevates LVEF and LVFS, improves cardiac function, and exerts myocardial protection. But the effective substances of AR-AAR in the treatment of CHF need further study.
Data Availability
Data will be made available on request.
Footnotes
Authors' Contributions
Q.D.: Investigation, methodology, writing—original draft. S.Z.: Investigation, methodology, writing—original draft. W.L.: Investigation, methodology, writing—original draft. K.L.: Resources, software. X.T.: Software. C.L.: Investigation. H.Y.: Data curation. F.M.: Data curation. S.C.: Software. J.L.: Software. P.W.: Writing—review and editing. F.G.: Writing—review and editing. M.X.: Funding acquisition, project administration, writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the projects of the National Natural Science Foundation of China (No. 81903837 and 81470174); Innovation Capability Support Program of Shaanxi (No. 2023-CX-PT-23); the Cultivation Project of the National Natural Science Foundation of the Second Affiliated Hospital of Shaanxi University of Chinese Medicine (No. 2023GPMS-001).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.