
Abstract
Elevated substance P can be utilized to predict early mortality during the first week of cerebral infarction. Whether aprepitant, a substance P receptor blocker could be utilized to alleviate poststroke pneumonia which is investigated in this study. Intraluminal monofilament model of middle cerebral artery occlusion (MCAO) was constructed in C57BL/6J male mice, and the relative expression of substance P was detected in collected bronchoalveolar lavage fluid (BALF) and lung tissue homogenate at 24 hours, 48 hours, and 72 hours poststroke. On the other hand, different concentrations of aprepitant (0.5, 1, and 2 mg/kg) were atomized and inhaled into MCAO mice. Inflammation cytokines and bacterial load were detected in collected BALF and lung tissue homogenate at 72-hour poststroke, and lung injury was revealed by histological examination. Aprepitant administration decreased total proteins, total cells, neutrophils, and macrophages in BALF. The concentrations of interleukin (IL)-6, IL-1β, tumor necrosis factor-α, interferon γ, monocyte chemoattractant protein-1, and IL-10 in lung tissue homogenates were also diminished by the administration of aprepitant. In conclusion, aprepitant could attenuate poststroke pneumonia in mice suggesting its potential therapeutic use in the clinic.
Introduction
As a common cerebrovascular disorder affecting focal neurological function with high mortality and disability, ischemic stroke can affect 16.9 million people yearly. 1 Aging is the strongest nonmodifiable risk factor for ischemic stroke. Aged stroke patients demonstrate higher mortality and morbidity and poorer functional recovery than their young counterparts. Poststroke complication mainly determines the outcome of a stroke. 2 –4 Among these complications, poststroke pneumonia can affect one-third of patients with acute stroke and generally occurs within 7 days of stroke onset. The presence and severity of poststroke pneumonia are linked to a longer hospital stay, higher healthcare expenses, and a three-fold increased risk of hospital mortality within 1 month. 5,6 Although antibiotic prophylaxis treatment may benefit some patients, there are no standardized antibiotic recommendations for poststroke pneumonia. 7,8
Stroke-associated pneumonia is frequently caused by aspiration, attenuated cholinergic pathways, and the unbalance of the oral microbial ecology. 9 Antibiotic prophylaxis, postural modification, systemic oral hygiene care, β-blockers, cilostazol, and statins have been recommended to prevent poststroke pneumonia with not well-satisfied clinical effect. Understanding the pathological mechanisms will greatly facilitate the treatment of stroke-related pneumonia.
As a neuropeptide belonging to the tachykinin family, substance P can be produced by neurons, eosinophils, macrophages, dendritic cells, and lymphocytes. Mechanistically, substance P can bind to the neurokinin-1 receptor (NK-1R) to function as a neurotransmitter or neuromodulator of primary nociceptive afferents. 10 On the other hand, substance P is reported to regulate leukocyte migration, infiltration, and biochemical activity in respiratory, gastrointestinal, and musculoskeletal systems. 11,12 Clinically, glucocorticoids might inhibit neurogenic inflammation by downregulation of NK-1R expression in inflammatory cells and epithelial cells to block the interaction between substance P and NK-1R. All of these indicate the potential to utilize NK-1R antagonists to alleviate inflammatory diseases.
In respiratory inflammation, substance P can promote the adhesion of neutrophils to pulmonary vascular endothelium and the migration along the subendothelial barrier layer through NK-1R. 13,14 Such pathology is also testified in the development of acute lung injury. 15,16 On the other hand, CP-96345, a potent nonpeptide NK-1R antagonist, is effective in the treatment of inflammatory and chronic pain aspects of asthma. 17 In a mouse model of smoke inhalation and burn injury, CP-96345 can block lung vascular leakage and inflammation effectively. 18
At the same time, the role of substance P in poststroke pneumonia is not deciphered. As a substance P antagonist, aprepitant can block NK1-R to prevent nausea and vomiting after surgery and chemotherapy, 19,20 which is approved by the U.S. Food and Drug Administration. 21 Whether aprepitant could be utilized to alleviate poststroke pneumonia is investigated in this study, and the treatment benefit of aprepitant is deciphered.
Methods and Materials
Middle cerebral artery occlusion
As previously reported, middle cerebral artery occlusion (MCAO) could induce poststroke pneumonia. 22 In this study, a similar procedure was followed. In brief, C57BL/6J male mice (8–10 weeks, 26–28 g) (Cyagen Biosciences Inc., Suzhou, China) were anesthetized with the inhalation of 3% isoflurane. A midline neck incision was cut to expose the left carotid artery, and a 5-0 nylon suture (Central Infusion Alliance) with a blunted tip was utilized to insert into the middle cerebral artery origin to induce focal cerebral ischemia for 30 minutes. Then the nylon suture was withdrawn to achieve reperfusion. In total, 0.5, 1, and 2 mg/kg aprepitant (Merck) were dissolved in 4 mL of phosphate-buffered saline (PBS), which were further atomized and inhaled (n = 8). An equal amount of PBS was atomized and inhaled into C57BL/6J male mice as a vehicle group. All experimental procedures were approved by the Ethics Committee of the Zibo Central Hospital (#2023.01.08-d52). In total, 96 mice were used in this study. No animal death was reported or found during the whole model construction and treatment periods.
To examine the degree of lung injury in mice, the lung index was calculated using the following formula:
Bacteriological and immune cell analysis
Mice were held in an upright position, and a tube was inserted into the trachea and 750 µL PBS was applied. The bronchoalveolar lavage fluid (BALF) was retrieved by aspiration while slowly moving the mouse into a dorsal position. BALF per sample was further centrifuged (200×g) and resuspended with 200 μL PBS. Total cells in BALF, neutrophils in BALF, and macrophages in BALF were counted after H&E staining. On the other hand, lung tissue homogenates were plated on blood agar plates and incubated at 37°C. After 18 hours, the colony-forming unit (CFU) was counted and calculated as positive colonies per milliliter BALF or lung tissue homogenates.
Enzyme-linked immunosorbent assay
The serum substance P and monocyte chemoattractant protein-1 (MCP-1), tumor necrosis factor (TNF)-α, interferon (IFN)-γ, interleukin (IL)-6, IL-1β, and IL-10 in lung tissue homogenate were measured with relevant enzyme-linked immunosorbent assay (ELISA) kits (eBioscience, San Diego, CA) at pre-, 24 hour, 48 hour, and 72 hour after MACO (n = 8). Optical density was detected with a SpectraMax M5 microplate reader (Molecular Devices, Sunnyvale, CA) at the wavelength of 450 nm.
Western blotting
Lung tissues were homogenated, and the soluble supernatants (20 µg) were separated by 12% sodium dodecyl sulfate-polyacrylamide gel electrophoresis and transferred to polyvinylidene fluoride membranes. After blocking with 5% nonfat dry milk, the membranes were incubated with the primary antibodies specific for SP (Invitrogen, PA5-106934, Waltham, MA) and β-actin (Abcam, Ab8226, Cambridge, MA) at a 1:1000 dilution at 4°C overnight, which were further incubated in peroxidase-conjugated secondary antibody (Sigma-Aldrich, St. Louis, MO) at a 1:1000 dilution for 1 hour at room temperature and developed with an electrochemiluminescence system (GE Healthcare Life Sciences, Little Chalfont, Buckinghamshire, United Kingdom). The relative intensity of the bands of interest was calculated by correcting for β-actin with NIH-Image J1.51p 22.
H&E staining
Lungs were fixed and embedded in paraffin, as described by the previous report. 23 Lung sections were cut at 2 µm and deparaffinized to stain with Hematoxylin and Eosin Staining Kit (Beyotime, China). To quantify the histological changes, we evaluated five pathological variables including pulmonary inflammation, hemorrhage, edema, hyaline membrane formation, and atelectasis. The extent of alteration of each variable was scored according to the affected field as 0 (no injury), 1 (less than 25%), 2 (25%–50%), 3 (more than 50% but less than 75%), and 4 (diffused injury). The scores of all five variables were added and averaged as the histological score of each sample (n = 8 in sham, vehicle, and Apr2 groups). All the assessment procedure was performed in a double-blinded way.
Statistical analysis
Differences between groups were determined using one-way ANOVA, followed by Dunn’s multiple comparisons test (p value <0.05). All statistical analyses were performed using GraphPad Prism (Version 8.3.0).
Results
Cerebral ischemia/reperfusion induces substance P expression
Upregulated substance P was detected in the serum (Fig. 1a, pre-: 43.65 ± 7.82 pg/mL; 24 hours: 70.32 ± 15.55 pg/mL, p = 0.004 compared with pre-; 48 hours: 109.48 ± 16.02 pg/mL, p < 0.001 compared with pre-; 72 hours: 121.22 ± 18.99 pg/mL, p < 0.001 compared with pre-), BALF (Fig. 1b, pre-: 135.39 ± 17.95 pg/mL; 24 hours: 248.03 ± 33.76 pg/mL, p < 0.001 compared with pre-; 48 hours: 442.14 ± 44.97 pg/mL, p < 0.001 compared with pre-; 72 hours: 489.58 ± 53.83 pg/mL, p < 0.001 compared with pre-), and lung tissue homogenates (Fig. 1c and d) at 24, 48, and 72 hours poststroke (p < 0.05), which demonstrated time course upregulated trend. All of these data indicated that cerebral ischemia/reperfusion-induced systemically upregulated expression of substance P.
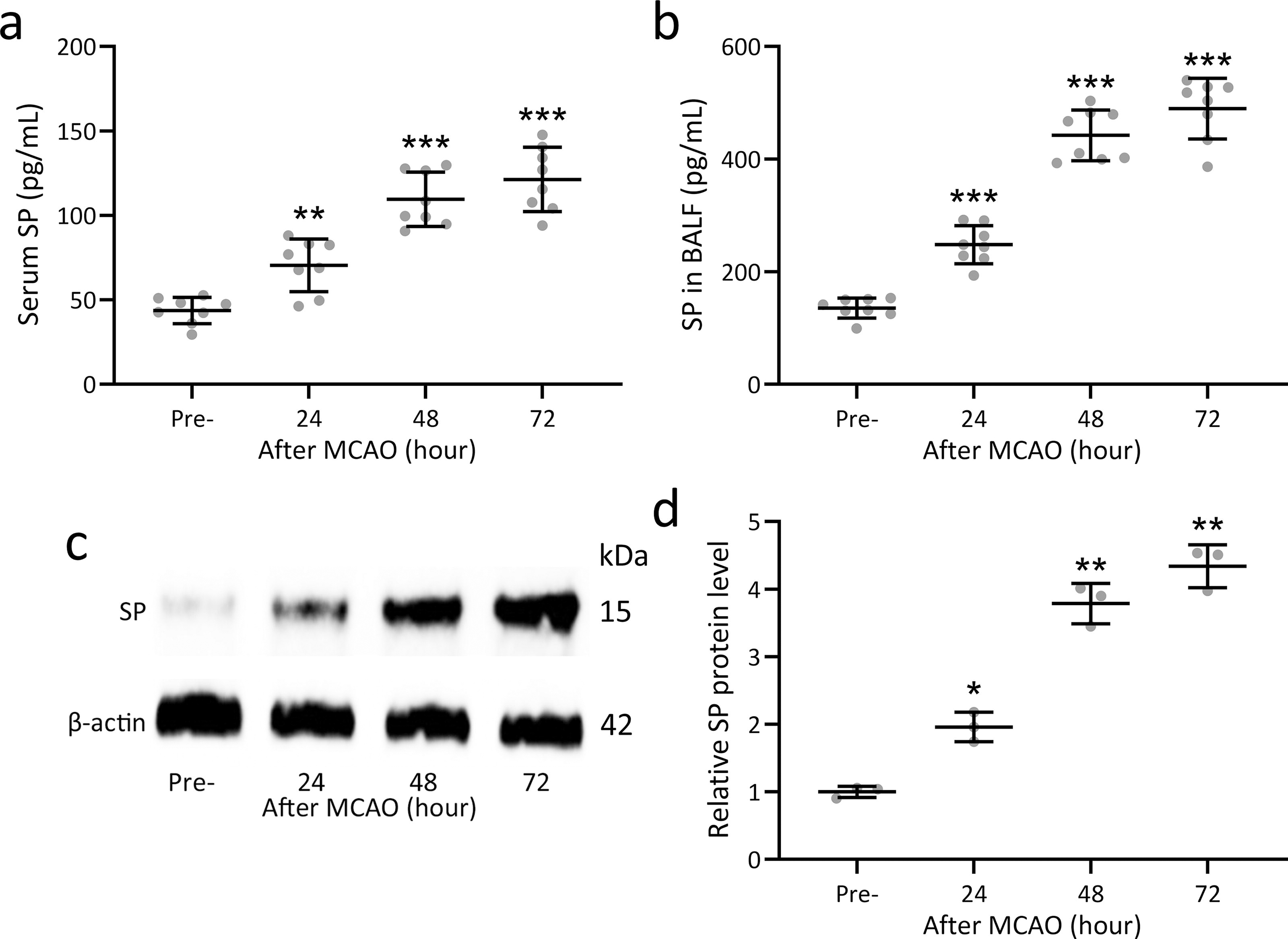
Substance P was upregulated after cerebral ischemia/reperfusion in mice. The concentrations of substance P in serum
Aprepitant inhibits substance P expression after cerebral ischemia/reperfusion
To test the effect of aprepitant on substance P expression, MCAO mice were challenged with different concentrations of vaporized aprepitant (0.5, 1, and 2 mg/kg). Downregulated substance P was detected in the serum (Fig. 2a, Sham: 44.27 ± 7.95 pg/mL; Vehicle: 124.61 ± 20.85 pg/mL, p < 0.001 compared with Sham; Apr0.5: 91.57 ± 15.05 pg/mL, p = 0.012 compared with Vehicle; Apr1: 76.58 ± 14.48 pg/mL, p < 0.001 compared with Vehicle; Apr2: 35.82 ± 9.46 pg/mL, p < 0.001 compared with Vehicle), BALF (Fig. 2b, Sham: 143.75 ± 19.61 pg/mL; Vehicle: 497.39 ± 58.73 pg/mL, p < 0.001 compared with Sham; Apr0.5: 359.72 ± 70.32 pg/mL, p = 0.003 compared with Vehicle; Apr1: 274.91 ± 48.45 pg/mL, p < 0.001 compared with Vehicle; Apr2: 181.39 ± 35.46 pg/mL, p < 0.001 compared with Vehicle), and lung tissue homogenates (Fig. 2c and d) were detected at 72 hours poststroke, which also demonstrated aprepitant dose-dependent substance P inhibition effect.
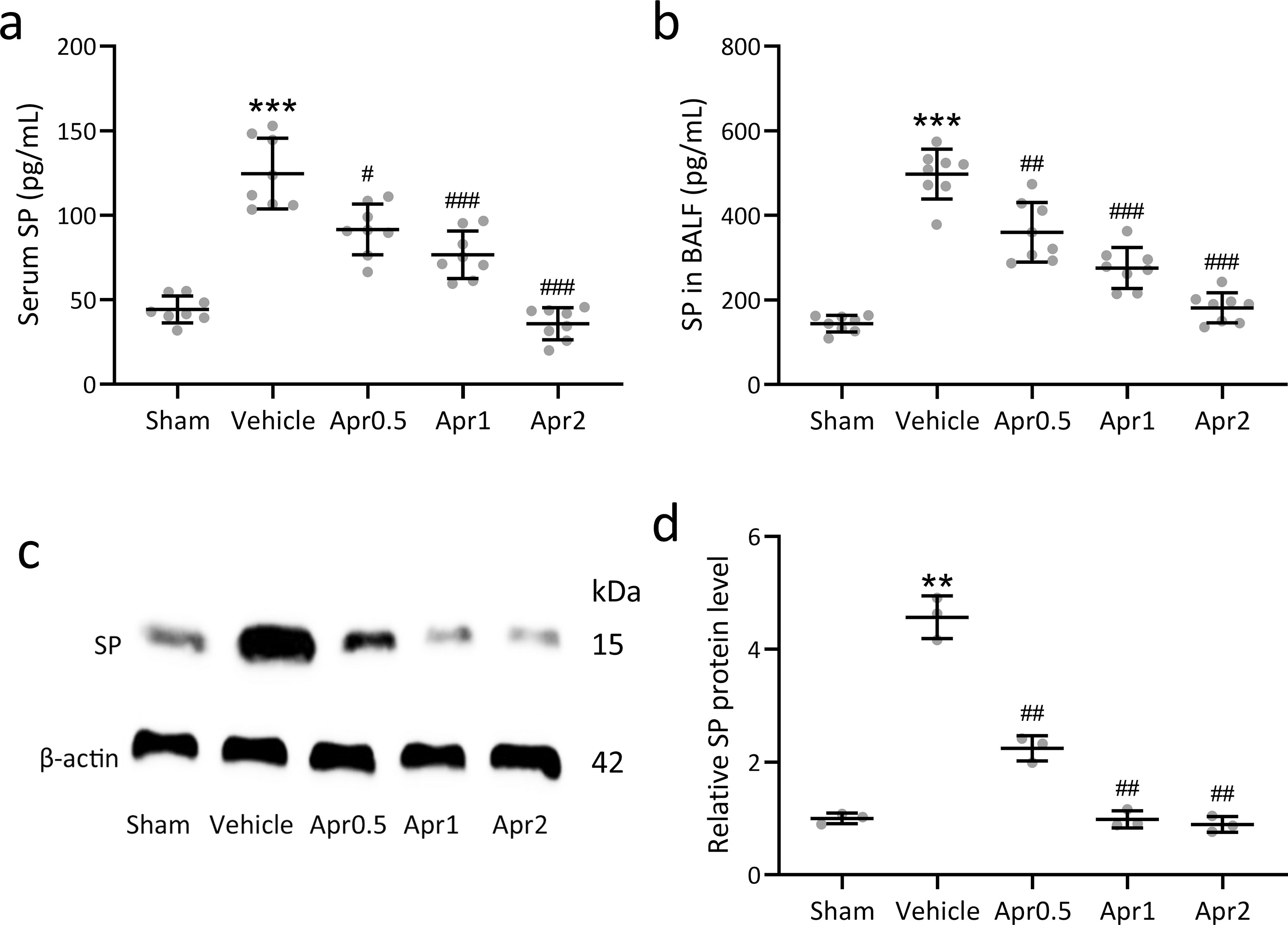
Aprepitant inhibited substance P after cerebral ischemia/reperfusion in mice. The mice were challenged with different concentrations of vaporized aprepitant. At 72 hours post MCAO, the concentrations of substance P in serum
Aprepitant inhibits inflammatory response in BALF after cerebral ischemia/reperfusion
The levels of total protein (Fig. 3a, Sham: 273.16 ± 68.91 μg/mL; Vehicle: 759.72 ± 119.80 μg/mL, p < 0.001 compared with Sham; Apr 0.5: 683.28 ± 117.66 μg/mL, p = 0.579 compared with Vehicle; Apr 1: 538.62 ± 98.82 μg/mL, p = 0.005 compared with Vehicle; Apr 2: 376.48 ± 77.25 μg/mL, p < 0.001 compared with Vehicle), the number of total cells (Fig. 3b, Sham: 1.72 ± 0.53 × 105; Vehicle: 6.63 ± 1.45 × 105, p < 0.001 compared with Sham; Apr 0.5: 4.81 ± 1.06 × 105, p = 0.049 compared with Vehicle; Apr 1: 3.79 ± 0.83 × 105, p = 0.002 compared with Vehicle; Apr 2: 2.58 ± 0.71 × 105, p < 0.001 compared with Vehicle), the number of neutrophils (Fig. 3c, Sham: 0.98 ± 0.17 × 105; Vehicle: 3.56 ± 0.74 × 105, p < 0.001 compared with Sham; Apr 0.5: 2.67 ± 0.52 × 105, p = 0.041 compared with Vehicle; Apr 1:2.26 ± 0.48 × 105, p = 0.004 compared with Vehicle; Apr 2:1.65 ± 0.38 × 105, p < 0.001 compared with Vehicle), and the number of macrophages in BALF (Fig. 3d, Sham: 0.46 ± 0.09 × 105; Vehicle: 0.89 ± 0.18 × 105, p < 0.001 compared with Sham; Apr 0.5: 0.71 ± 0.14 × 105, p = 0.160 compared with Vehicle; Apr 1: 0.59 ± 0.14 × 105, p = 0.012 compared with Vehicle; Apr 2: 0.50 ± 0.11 × 105, p = 0.001 compared with Vehicle) were significantly upregulated after stroke, which testified the occurrence of poststroke pneumonia. On the other hand, aprepitant also demonstrated a dose-dependent (0.5, 1, and 2 mg/kg) inhibition effect. Thus, in the following experiments, 2 mg/kg aprepitant was utilized.
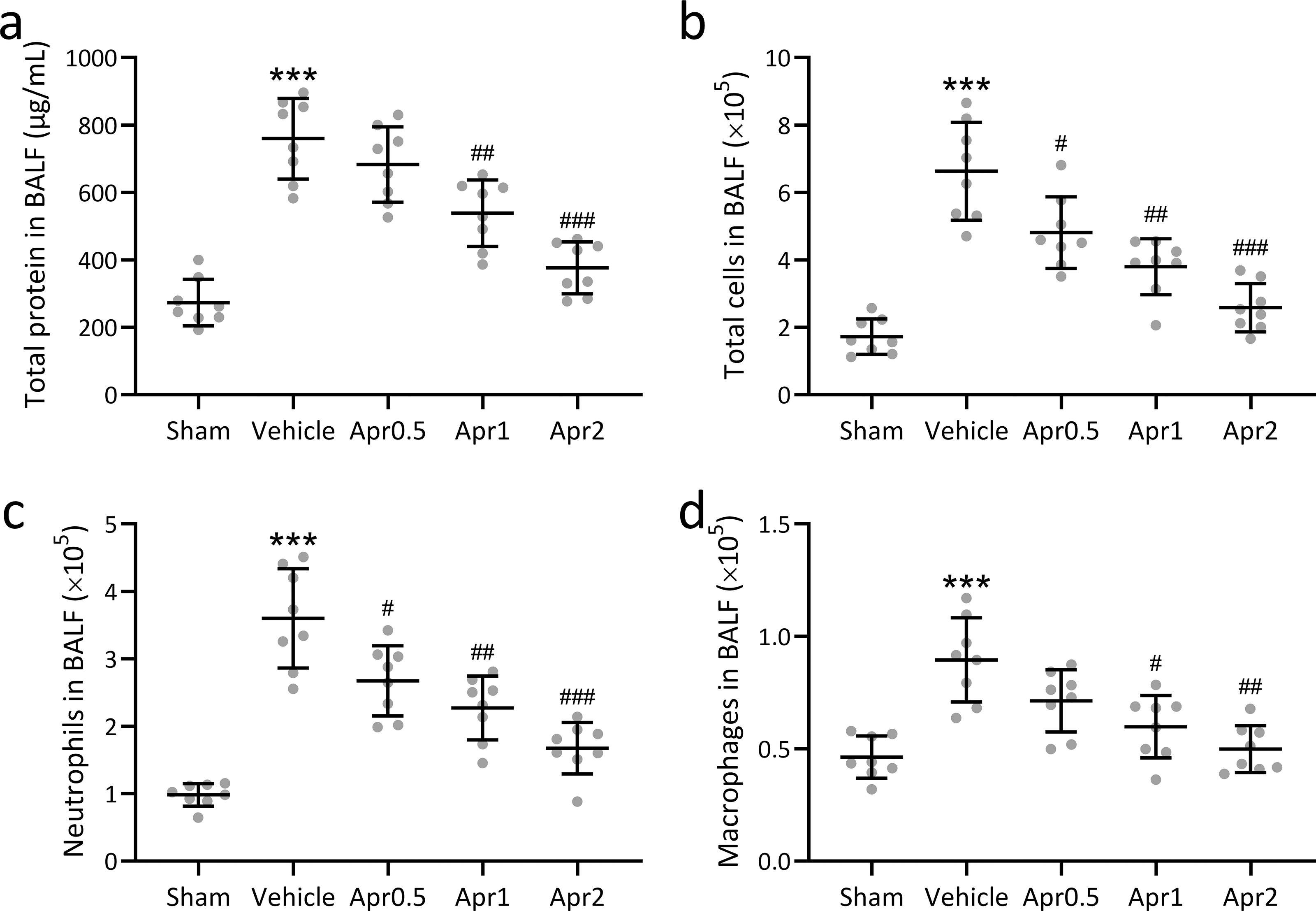
Aprepitant inhibited inflammatory response in bronchoalveolar lavage fluid (BALF) after cerebral ischemia/reperfusion in mice. The mice were challenged with different concentrations of vaporized aprepitant. At 72 hours post MCAO, total proteins in the BALF
Aprepitant attenuates pulmonary injury after cerebral ischemia/reperfusion
In this study, cerebral ischemia/reperfusion-induced lung damage was demonstrated with increased lung index, bacterial loading, and histological scores. Aprepitant treatment could significantly decrease MCAO-induced upregulation of lung index (Fig. 4a, Sham: 0.76 ± 0.09%; Vehicle: 1.13 ± 0.12%, p < 0.001 compared with Sham; Apr 2: 0.95 ± 0.09%, p = 0.008 compared with Vehicle), bacterial loading (Fig. 4b, Sham: 0.086 ± 0.035 (Log10 CFU mL−1); Vehicle: 5.741 ± 0.952 (Log10 CFU mL−1), p < 0.001 compared with Sham; Apr 2: 2.453 ± 0.594 (Log10 CFU mL−1), p < 0.001 compared with Vehicle), and histological scores (Fig. 4c, Vehicle: 3.25 ± 0.62; Apr2: 1.68 ± 0.44, p < 0.001 compared with Vehicle). The morphological changes, such as lung consolidation, intra-alveolar inflammatory infiltration, and thickened alveolar septa were also demonstrated in Figure 4d.
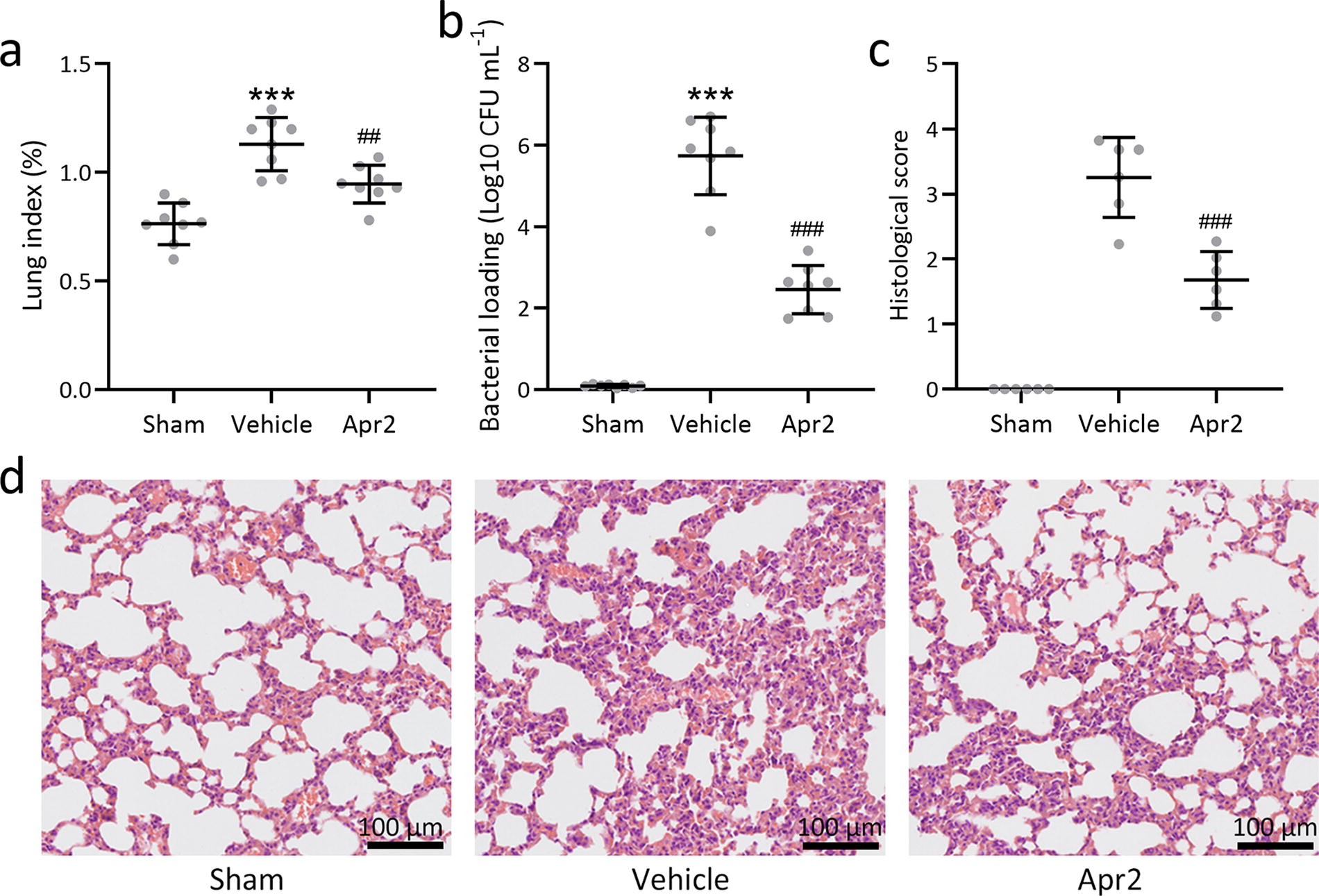
Aprepitant attenuated pulmonary injury after cerebral ischemia/reperfusion in mice. The mice were challenged with 2 mg/kg of vaporized aprepitant. At 72 hours post MCAO, the lung index was compared
Aprepitant attenuates pulmonary inflammatory response after cerebral ischemia/reperfusion
Upregulated concentrations of IL-6 (Fig. 5a, Sham: 34.53 ± 5.11 pg/mg tissue; Vehicle: 72.14 ± 11.12 pg/mg tissue, p < 0.001 compared with Sham; Apr 2: 53.07 ± 11.55 pg/mg tissue, p = 0.009 compared with Vehicle), IL-1β (Fig. 5b, Sham: 23.74 ± 4.99 pg/mg tissue; Vehicle: 53.81 ± 8.93 pg/mg tissue, p < 0.001 compared with Sham; Apr 2: 36.84 ± 7.15 pg/mg tissue, p = 0.002 compared with Vehicle), TNF-α (Fig. 5c, Sham: 14.26 ± 3.45 pg/mg tissue; Vehicle: 38.95 ± 6.26 pg/mg tissue, p < 0.001 compared with Sham; Apr 2: 24.44 ± 4.93 pg/mg tissue, p < 0.001 compared with Vehicle), IFN-γ (Fig. 5d, Sham: 25.86 ± 6.11 pg/mg tissue; Vehicle: 39.22 ± 7.54 pg/mg tissue, p = 0.004 compared with Sham; Apr 2: 30.06 ± 4.28 pg/mg tissue, p = 0.025 compared with Vehicle), MCP-1 (Fig. 5e, Sham: 18.73 ± 3.58 pg/mg tissue; Vehicle: 29.84 ± 5.85 pg/mg tissue, p = 0.001 compared with Sham; Apr 2: 22.17 ± 4.82 pg/mg tissue, p = 0.019 compared with Vehicle), and IL-10 (Fig. 5f, Sham: 19.84 ± 3.75 pg/mg tissue; Vehicle: 25.39 ± 5.27 pg/mg tissue, p = 0.041 compared with Sham; Apr 2: 40.78 ± 7.36 pg/mg tissue, p < 0.001 compared with Vehicle) in the lung tissue homogenate of MACO mice were detected by ELISA, while aprepitant treatment could significantly decrease the relative expression of IFN-γ, IL-6, TNF-α, IL-1β, and MCP-1, and increase the relative expression of IL-10. All of these results demonstrated that aprepitant inhibited the expression of the inflammatory cytokines and promoted the expression of regulatory cytokine.
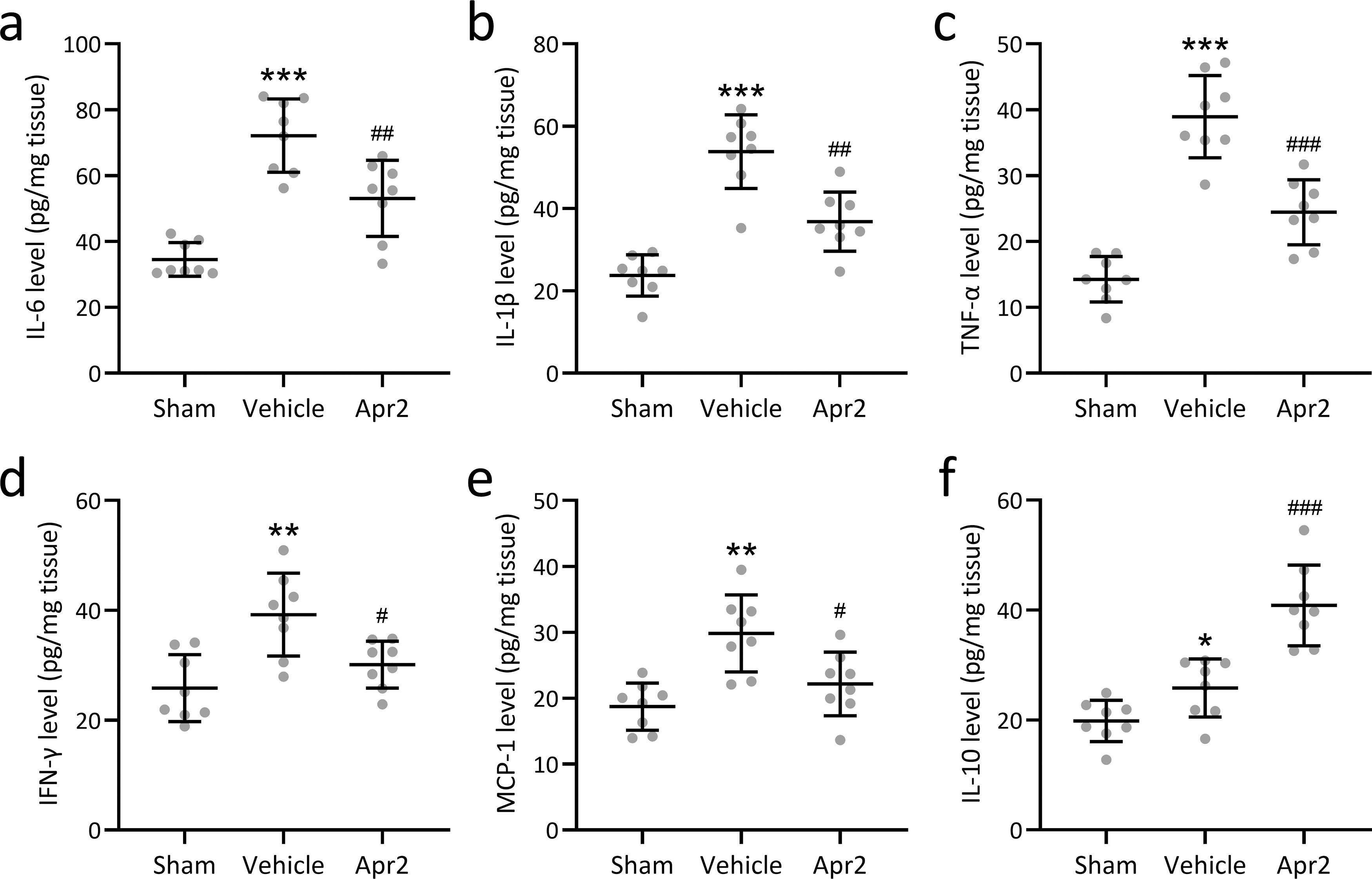
Aprepitant attenuated pulmonary inflammatory response after cerebral ischemia/reperfusion in mice. The mice were challenged with 2 mg/kg of vaporized aprepitant. At 72 hours post MCAO, the concentrations of IL-6
Discussion
Upregulated inflammatory cells of neutrophils and macrophages and lung damage are observed in the BALF of MACO mice with increased lung index, bacterial loading, and histological scores. All of these indicate that 30-minute MCAO could be utilized as a model to imitate poststroke pneumonia. Cerebral ischemia/reperfusion upregulates substance P expression, which could be inhibited by aprepitant administration with diminished inflammatory response and lung injury. All of these data demonstrate that aprepitant can be utilized to alleviate poststroke pneumonia.
Serum substance P could be utilized to predict early mortality during the first week of cerebral infarction. 24 It is further testified that substance P contributes to the development of traumatic brain injury-induced encephaledema, blood-brain barrier permeability, and functional deficits. On the other hand, substance P can stimulate monocytes and macrophages to release inflammation cytokines, promote neutrophil degranulation and granules release, and induce TNF-α and IL-1β production. 25,26 All of these indicate that substance P receptor antagonist might improve the outcome of reversible ischemia. 27,28
As a highly selective NK-1R antagonist, aprepitant is widely used for chemotherapy or operation-induced nausea and vomiting prophylaxis. 29 While no relevant research about substance P receptor antagonist on poststroke pneumonia has been performed. In this study, we testify that aprepitant could be used to alleviate stroke-associated pneumonia with diminished lung injury, inflammation, and bacterial load. Mechanically, substance P/NK-1R can activate ERK1/2 and NF-kappa B to upregulate prostaglandin E metabolite and cyclooxygenase-2 in burn-induced lung injury. 30 In tumor cells, substance P/NK-1R promotes the antiapoptosis, migration, invasion, and metastasis biological processes through the Hairy and Enhancer of Split 1 (Hes 1)/Notch1 pathway or NF-kappa B pathway. 31
As one of the vital chemokines, MCP-1 can bind CCR2 to regulate monocyte/macrophage migration and infiltration. Clinically, MCP-1 is a potential predictor of the severity of community-acquired pneumonia. 32 The level of MCP-1 in BALF and serum can be utilized to discriminate idiopathic pulmonary fibrosis from other interstitial lung diseases and to predict the outcome of interstitial lung diseases. 33,34 In this study, upregulated MCP-1 secretion could be inhibited by the administration of aprepitant. On the other hand, CP-96345, another nonpeptide NK-1R antagonist, has been reported to downregulate constitutive substance P mRNA expression in human mononuclear cells. 35 In this study, attenuated macrophage and neutrophil infiltration and inflammation cytokine production are induced by aprepitant administration. All of these indicates that mononuclear cells might be the potential target cells of aprepitant.
Some limitations should be indicated. In this study, the treatment effect of aprepitant on poststroke pneumonia could be attributed to the interaction with substance P/NK-1R interaction, while the level of NK-1R is not deciphered in this investigation. Further detailed analysis of substance P/NK-1R interaction should be performed in the future. In this study, only the poststroke pneumonia model is applied; other stroke-associated pneumonia models should be discussed in the future.
Conclusion
Aprepitant alleviates poststroke pneumonia in MCAO mice, which could be considered as the new treatment therapy.
Footnotes
Authors’ Contributions
Z.X., M.X., F.Y., and X.Z. conducted the experiments, analyzed the data, and wrote the article. F.Y., and X.Z. conceived the study. X.X. supervised the project. All authors read and approved the final article.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
All experimental procedures were proved by the Ethics Committee of the Zibo Central Hospital.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.