
Abstract
Total hip arthroplasty (THA) is a highly effective intervention for addressing hip joint issues, yet managing perioperative pain remains a significant challenge. In this study, we aimed to investigate the impact of supplementing ropivacaine with dexmedetomidine in ultrasound-guided continuous pericapsular nerve group block (PENGB) among elderly patients undergoing THA. We conducted a retrospective analysis involving 112 elderly patients who underwent THA. These patients were divided into two groups: the Control group, receiving ropivacaine alone, and the DEX group, receiving ropivacaine combined with dexmedetomidine. We evaluated various parameters including hemodynamic data, postoperative pain levels assessed using the Visual Analog Scale, cognitive status measured with the Montreal Cognitive Assessment, and serum markers (S100β and GFAP). Our findings revealed that the DEX group exhibited improved stability in blood pressure and oxygen saturation following surgery. Moreover, patients in the DEX group reported significantly lower levels of pain at 6 and 12 hours postsurgery, with a prolonged duration of pain relief. Furthermore, dexmedetomidine administration was associated with preserved cognitive function during the early postoperative period. Analysis of serum markers suggested potential cognitive protection conferred by the addition of dexmedetomidine. Overall, our study underscores the multifaceted benefits of incorporating dexmedetomidine into ropivacaine-based PENGB for elderly THA patients.
Introduction
Total hip arthroplasty (THA) is a well-established surgical procedure aimed at relieving pain and restoring function in individuals with hip joint issues, significantly enhancing their quality of life. 1,2 However, perioperative pain is a common challenge for THA patients, often triggering a strong stress response that can impede early postoperative mobility and functional rehabilitation. 3 Although fascia iliaca compartment block (FICB) is a regional nerve block technique used for pain relief in THA, it may not comprehensively address pain associated with certain hip surgeries due to its limitations in targeting the obturator nerve. 4,5
In contrast, the pericapsular nerve group block (PENGB) is a regional anesthesia technique specifically designed to provide targeted pain relief for procedures involving the hip joint and surrounding structures. 6 –8 By blocking pericapsular nerves, including branches of the femoral nerve, obturator nerve, and accessory obturator nerve, PENGB offers effective pain relief, particularly on the inner aspect of the hip joint. 9 Compared with FICB, PENGB has been suggested to provide more comprehensive pain relief for procedures involving the inner aspect of the hip joint, making it a valuable tool in modern anesthesia and pain management. 10,11
Dexmedetomidine, increasingly utilized as an adjuvant in nerve blocks, exerts its analgesic effects through its high selectivity for α-2 adrenergic receptors. 12 When added to ropivacaine, dexmedetomidine extends the duration of nerve blockade by inhibiting potassium and sodium currents, leading to reduced neuronal activity. 13 In addition, it blocks the activation of hyperpolarizing cation currents, thereby prolonging analgesia. 14,15 However, the prolonged analgesic effects of dexmedetomidine as an adjunct to ropivacaine in elderly THA patients remain uncertain. Therefore, this study aims to investigate the effects of adding dexmedetomidine to ropivacaine in ultrasound-guided continuous PENGB among elderly patients undergoing THA.
Methods
Study design and participants
This is a retrospective study. The objective of the study is to investigate the effects of adding dexmedetomidine to ropivacaine in ultrasound-guided continuous PENGB among elderly patients undergoing THA, as well as evaluating the impact of the addition of dexmedetomidine on hemodynamic stability, postoperative pain levels, cognitive function, and serum markers in elderly THA patients. The study was approved by the Second People’s Hospital of Hefei, Hefei Hospital affiliated to Anhui Medical University, and written informed consent was derived from the participants. This study included a total of 112 elderly patients who underwent THA at our hospital between January 2020 and January 2022. They were divided into two groups, including the Control group (n = 56) and the DEX group (n = 56). Control Group: In the Control group, 20 mL of 0.375% ropivacaine was administered through the catheter during the PENGB. DEX Group: In the DEX group, 20 mL of a mixture containing 0.375% ropivacaine and 1 μg/kg of dexmedetomidine was administered through the catheter during the PENGB procedure. Exposure Factors: Administration of ropivacaine alone in the Control group. Administration of a mixture containing ropivacaine and dexmedetomidine in the DEX group.
Inclusion Criteria: Patients aged 60 years or older upon admission. Elective THA procedure. Classified as American Society of Anesthesiologists (ASA) physical status I, II, or III. No history of hip joint surgery on the affected side. No use of analgesic or sedative medications in the 24 hours prior to surgery. No known allergies to the anesthetic agents used in this study. Able to cooperate in completing the assessment scales. Informed consent provided by the patient and/or their family. Montreal Cognitive Assessment (MoCA) score of 26 or higher at the time of enrollment.
Exclusion Criteria: History of previous hip joint surgery on the affected side. Infection at the puncture site. Known allergy to local anesthetic agents. Severe hepatic or renal dysfunction. History of opioid drug dependency. Coagulation disorders. Severe visual, auditory, or language expressive ability impairments.
Pericapsular nerve group block
A low-frequency convex ultrasound probe (2–5 MHz) was positioned over the anterior superior iliac spine, parallel to the pubic ramus, and rotated until an image of the iliopsoas muscle tendon near the pubic ramus prominence was visualized. Following local anesthesia at the puncture site, a 100 mm 19G nerve block needle was used to insert it in an in-plane technique from the outside to the inside, following the fascial plane between the iliopsoas muscle tendon and the pubic ramus. A test injection of saline solution was performed after confirming the absence of blood return. Once the iliopsoas muscle tendon elevated, a catheter was inserted 3–5 cm beyond the needle tip through the tendon. Then, 20 mL of 0.375% ropivacaine was administered through the catheter (in the Control group), or 20 mL of a mixture containing 0.375% ropivacaine and 1 μg/kg of dexmedetomidine was administered (in the DEX group). During the drug injection, the spread of the medication in front of the iliopsoas muscle tendon was monitored, and the catheter’s position was adjusted as needed. The catheter was securely fixed after drug administration.
Anesthesia
The patient underwent preoperative fasting for 8 hours and refrained from drinking for 2 hours. Upon entering the operating room, oxygen was administered, and an intravenous line was established for standard monitoring of heart rate (HR), blood pressure (BP), oxygen saturation (SpO2), and electrocardiography. PENGB was performed before the induction of general anesthesia. Approximately 10 minutes after completing the PENGB procedure, routine monitoring of the Bispectral Index (BIS) for anesthesia depth was initiated, followed by the induction of anesthesia. Following the completion of the surgery, the patient was connected to a patient-controlled analgesia (PCA) pump. The PCA formulation consisted of 2.0 μg/kg of sufentanil and 10 mg of tropisetron, diluted with saline solution to a total volume of 100 mL. The parameters for the analgesia pump were set as follows: a background infusion rate of 2 mL/h, a single bolus dose of 2 mL, and a lockout time of 15 minutes.
Visual Analog Scale
A 10-cm-long horizontal line was drawn on paper, with one end labeled as 0, representing no pain, and the other end as 10, representing severe pain. Patients independently marked the point on the line that best represents their own pain intensity. The distance between the mark and the point indicating no pain on the ruler was measured to determine the pain score, with higher scores indicating more severe pain.
Montreal Cognitive Assessment
The MoCA assesses various cognitive domains, including attention and concentration, memory, executive function, visual-spatial skills, language, abstract thinking, calculation, and orientation. The total score is 30 points, with a score of 26–30 considered normal.
Outcomes
The study evaluates multiple outcome indicators, including hemodynamic parameters such as mean arterial pressure (MAP), HR, and SpO2 measured at different time points. VAS scores are employed for pain assessment, whereas MoCA scores are utilized to evaluate cognitive function. Analysis of serum markers, specifically S100β and GFAP, is conducted to assess cognitive protection. In addition, the duration of effective pain relief is determined by measuring the time to first PCA pump use, total effective PCA pump presses, and sufentanil consumption.
Follow-up time
The follow-up time spans various key data collection points: before the PENGB procedure (T0), at the start of surgery (T1), at the conclusion of surgery (T2), and subsequently at 3 hours (T3), 6 hours (T4), 12 hours (T5), 24 hours (T6), 72 hours (T7), and 7 days (T8) postoperatively.
Statistical analysis
Statistical analysis was conducted using SPSS 20.0 software. Normally distributed continuous data were represented as mean ± standard deviation. Between-group comparisons were performed using one-way analysis of variance (ANOVA), and post-hoc pairwise comparisons were conducted using the Fisher's Least Significance Difference t test. Categorical data were expressed as frequencies and compared using the χ2 test, whereas comparisons of ordinal data were conducted using the rank-sum test. Statistical significance was defined as p < 0.05.
Results
Demographic characteristics
Table 1 presents a comparative analysis of baseline characteristics between 56 elderly hip arthroplasty patients in the Control group and an equal number in the DEX group. No significant disparities were observed in age, gender, ASA classification, presence of hypertension, diabetes, or other factors between the two cohorts. Moreover, surgical duration and blood loss showed no significant variance, indicating baseline equivalence.
Demographic and Clinical Characteristics of the Study Participants
Values are expressed as n (percentage, %) or mean ± SD. p values were derived from Mann–Whitney test. Chi-square test or Fisher’s exact test was used for assessing distribution of observations or phenomena between different groups.
ASA, American Society of Anesthesiologists.
MAP, HR, and SpO2 between the Control and DEX groups
Table 2 delineates the mean MAP, HR, and SpO2 among 56 patients in both the Control and DEX groups at four distinct time points: T0, T1, T2, and T4. Notably, substantial discrepancies emerged at T2 regarding BP and SpO2. The adjunctive administration of dexmedetomidine with ropivacaine appeared to markedly stabilize BP and arterial SpO2 postsurgery, suggesting potential hemodynamic benefits. These findings underscore the importance of monitoring hemodynamic parameters in assessing the impact of dexmedetomidine.
Comparisons of MAP, HR, and Arterial SpO2 Between the Two Groups
Values are expressed as mean ± SD.
p < 0.05 compared with Control at the same time point. Mann–Whitney test.
HR, heart rate; MAP, mean artery pressure; SpO2, oxygen saturation.
Comparisons of VAS scores between the two groups
Figure 1 depicts pain differentials between the two groups. Pre-PENGB VAS scores exhibited no significant variance. However, at 6 hours (T4) and 12 hours (T5) postsurgery, the DEX group reported significantly diminished pain levels, underscoring the efficacy of dexmedetomidine in alleviating postoperative pain during these intervals. This highlights the relevance of VAS scores in assessing pain management strategies.
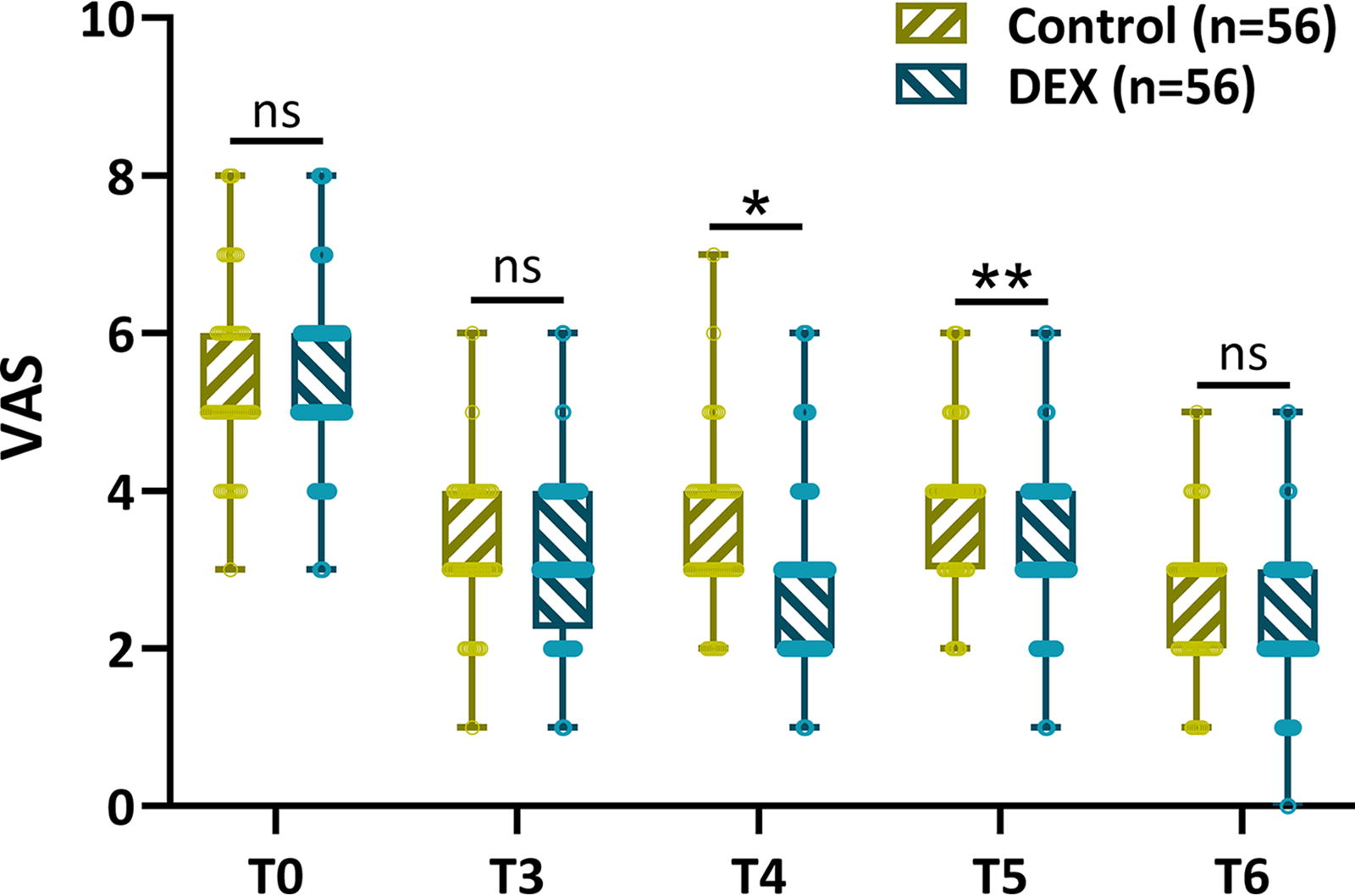
Comparisons of VAS scores between the two groups at the time of before PENGB (T0), 3 hours after surgery (T3), 6 hours after surgery (T4), 12 hours after surgery (T5), and 24 hours after surgery (T6). PENGB, pericapsular nerve group block; VAS, Visual Analog Scale.
Duration of effective pain relief
Figure 2 illustrates the time elapsed until the initial PCA pump activation within the initial 48 hours following surgery, total effective PCA pump activations, and sufentanil consumption between the groups. Patients in the DEX group demonstrated a significantly prolonged interval before the initial PCA pump activation postsurgery, along with a reduction in both effective PCA pump activations and sufentanil consumption compared with the Control group (Fig. 2A–C). These findings suggest that dexmedetomidine adjunctive to ropivacaine extends the duration of effective pain relief and diminishes opioid consumption following surgery. This underscores the potential role of dexmedetomidine in optimizing postoperative pain management.

Comparisons of time of first analgesic pump use postsurgery
MoCA scores between the two groups
MoCA scores evaluated at various time points indicated a decline in cognitive levels postsurgery, albeit partially mitigated with the adjunctive use of dexmedetomidine with ropivacaine (Fig. 3). The transient preservation of cognitive function with dexmedetomidine was evident during the early postoperative period, with disparities between groups diminishing by the seventh day postsurgery. This highlights the importance of monitoring cognitive outcomes and the potential role of dexmedetomidine in preserving cognitive function postoperatively.
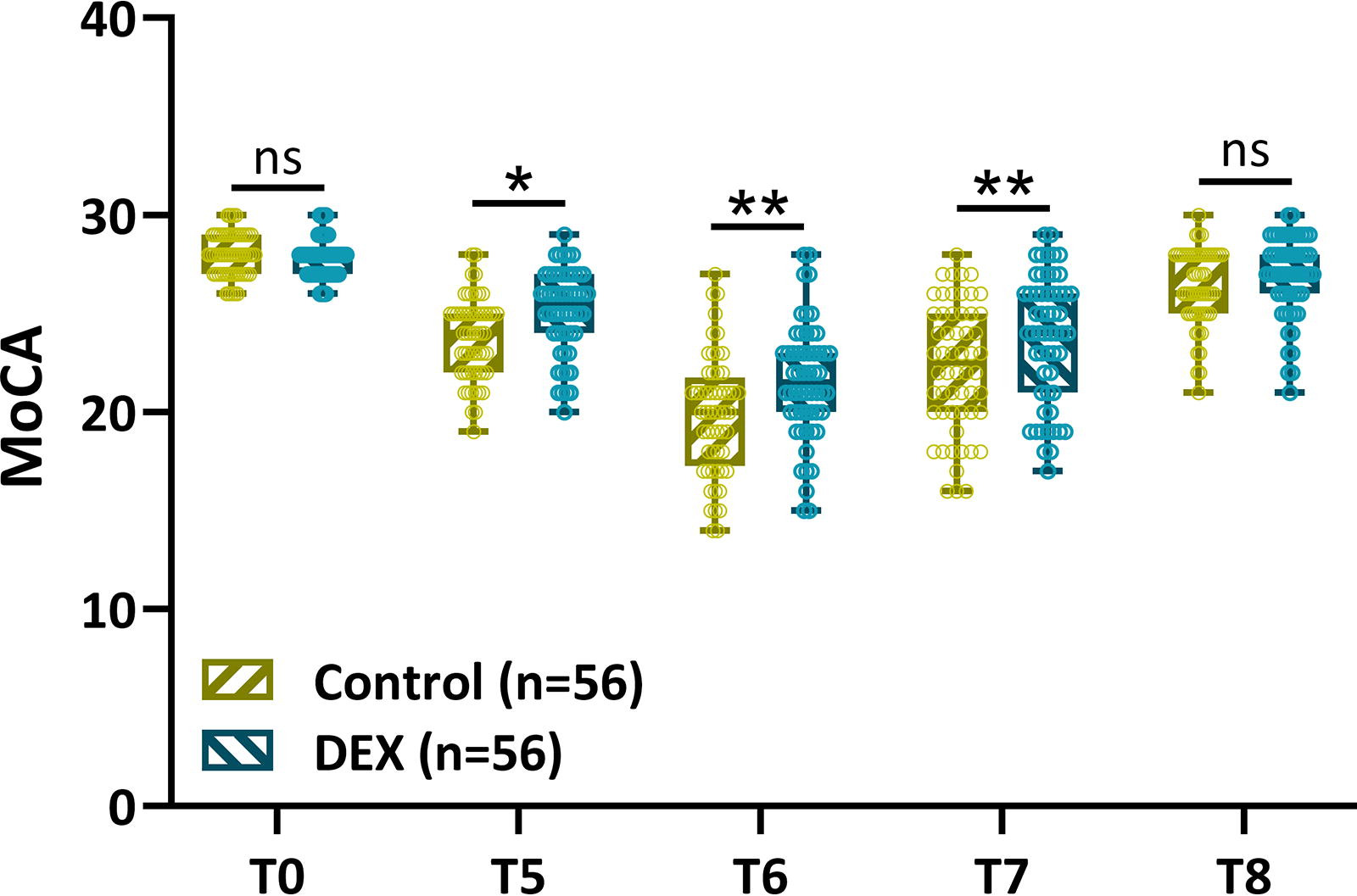
Comparisons of MoCA scores between the two groups at the time of before PENGB (T0), 12 hours after surgery (T5), 24 hours after surgery (T6), 72 hours after surgery (T7), and 7 days after surgery (T8). MoCA, Montreal Cognitive Assessment.
Cognitive-related serum factor analysis
We separately analyzed the levels of S100β (Fig. 4A) and GFAP (Fig. 4B) in the serum at two time points: before the PENGB and 3 days after surgery. S100β and GFAP are specific markers associated with brain injury and neuroinflammation, and their levels in the serum can provide insights into cognitive changes and potential protective effects. 16 The 3-day postoperative time point corresponds to the cognitive injury stage as shown in Figure 3. It is evident that the addition of dexmedetomidine to ropivacaine can mitigate cognitive impairment to some extent. This suggests that the use of dexmedetomidine as an adjunct to ropivacaine may have a protective effect against cognitive injury in the early postoperative period.
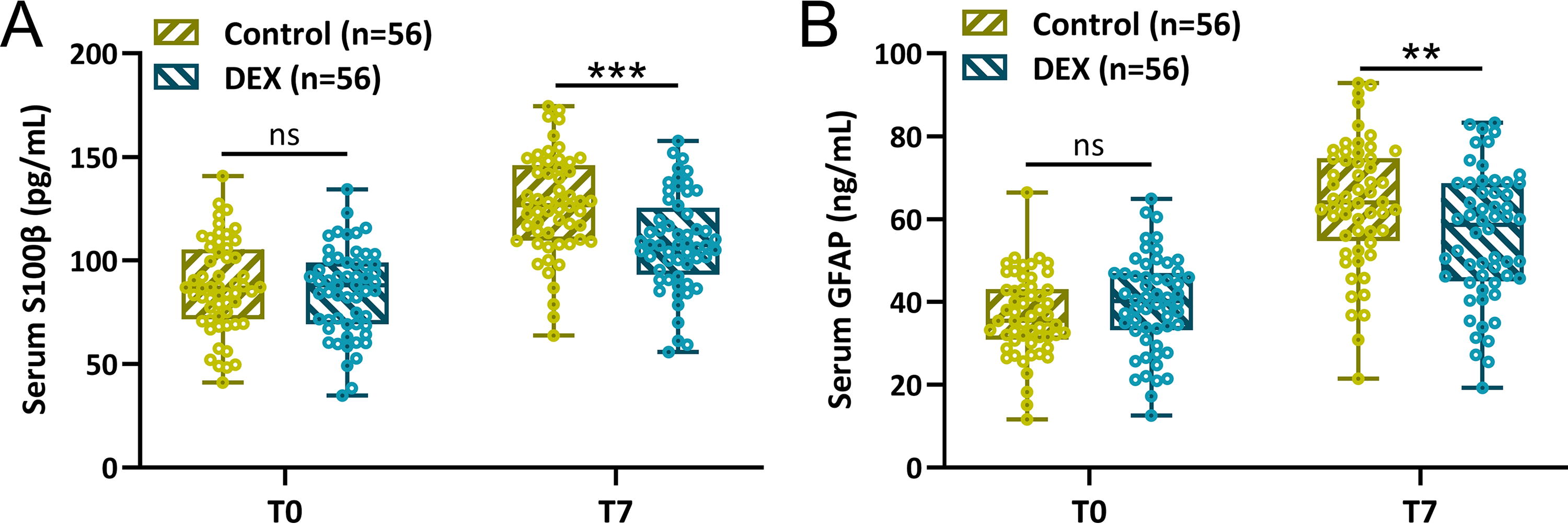
Comparisons of serum S100β
Discussion
PENGB is a novel peripheral nerve block technique that provides analgesia by blocking the major nerve branches around the hip joint while preserving muscle strength in the lower limbs. Continuous nerve block, achieved by continuously infusing local anesthetics through a catheter placed in the perineural or interfascial space, can offer prolonged pain relief, significantly reducing the need for systemic analgesics. To address the short duration of action of single nerve blocks, nerve perineural catheter techniques have emerged in recent years. However, catheter placement is prone to issues such as displacement, increased risk of infection, and management difficulties, limiting its application. 17,18 As a result, adjuncts are increasingly used in nerve blocks, with commonly used ones including dexamethasone and dexmedetomidine. 19
The use of dexamethasone in perineural and intravenous administration may lead to hyperglycemia. Given that elderly patients with hip fractures often have comorbidities such as diabetes and hypertension, this study opted for dexmedetomidine as an adjunct for investigation. The study aims to explore the analgesic effects of dexmedetomidine as an adjunct to ropivacaine in elderly hip surgery patients undergoing PENGB and its role in preventing postoperative cognitive dysfunction.
In this study, the VAS scores revealed that the DEX group had significantly less pain at 6 and 12 hours postoperatively, demonstrating the effectiveness of adding dexmedetomidine in reducing postoperative pain. The duration of effective pain relief was also extended in the DEX group, as evidenced by a longer time to the first press of the PCA pump, lower numbers of effective PCA pump presses, and reduced sufentanil consumption. This suggests that dexmedetomidine’s addition to ropivacaine can provide more prolonged pain relief and reduce opioid consumption postoperatively.
Dexmedetomidine possesses anxiolytic, analgesic, and hemodynamic stabilizing effects, playing a crucial role in improving brain injury and neurological function caused by ischemia and hypoxia. 20 In addition, dexmedetomidine can improve airway pressure and compliance without respiratory depression. 21 Studies have shown that dexmedetomidine can inhibit neuronal apoptosis via the mitochondrial pathway, mediate neuroglobin expression, and exert neuroprotective effects in rats subjected to hypoxia-reoxygenation models. 22,23 However, the mechanism through which it prolongs the duration of nerve blockade when used as an adjunct to ropivacaine remains unclear. There is evidence to suggest that dexmedetomidine inhibits potassium and sodium currents, resulting in reduced neuronal activity. 24 Another study indicates that the addition of dexmedetomidine to ropivacaine can block the activation of hyperpolarizing cation currents, thereby extending the duration of analgesia. 25 α-2 adrenergic receptor agonists can, by inhibiting the central sympathetic nervous system, reduce the systemic inflammatory response and modulate the immune system. 26 They also activate antiapoptotic signal pathways, providing protective effects on damaged cells in various organs, including the brain, heart, liver, lungs, kidneys, and intestines. 27 Dexmedetomidine is a relatively highly selective α-2 adrenergic receptor agonist, known for its sedative, analgesic, and anxiolytic properties. 28 The locus coeruleus in the brainstem is one of the most densely populated areas of adrenergic receptors in the brain and plays a crucial role in the regulation of pain neurotransmitters. Dexmedetomidine acts on the locus coeruleus in the brainstem, where its activation of α-2 adrenergic receptors in the nucleus produces antianxiety, sedative, and hypnotic effects. 29 There have been several studies investigating the effects of dexmedetomidine on cognition using animal models. Its impact on cognitive function in various animal models of neurological disorders and conditions such as ischemia-reperfusion injury, traumatic brain injury, Alzheimer’s disease (AD), and aging-related cognitive decline. 30,31 These animal studies provide valuable insights into the potential cognitive effects of dexmedetomidine. 32
S100β protein, primarily secreted by glial cells in the nervous system, plays a crucial role in maintaining calcium ion stability in the body and is closely associated with cognitive function. 33 It is predominantly found in astrocytes of the central nervous system and serves as a vital biological marker for central nervous system dysfunction and inflammatory reactions, sensitively diagnosing early cognitive impairment. 34 The concentration of S100β protein holds clinical significance in predicting the occurrence of POCD.
GFAP is a type III intermediate filament protein expressed by astrocytes. Due to its rapid release following axonal degeneration and astrocyte proliferation, it serves as a specific marker for astrocytes. 35 Its expression levels are significantly upregulated in neurodegenerative diseases such as AD and Parkinson’s disease (PD). 36 Studies have shown that both cerebrospinal fluid and plasma GFAP levels serve as predictive indicators for longitudinal cognitive decline. 37 Another study indicated that baseline plasma GFAP levels not only exhibit a significant negative correlation with Mini-Mental State Examination scores but also predict the transition from mild cognitive impairment to dementia in patients with PD. 37
In this study, the cognitive status, assessed using the MoCA, showed a temporary cognitive-preserving effect in the DEX group during the early postoperative period. This effect is particularly promising for elderly patients undergoing THA who are at risk of cognitive decline after surgery. Furthermore, the analysis of serum markers S100β and GFAP indicates that the use of dexmedetomidine as an adjunct to ropivacaine may provide some protection against cognitive injury in the early postoperative period.
The safety of anesthesia is also an important factor we consider. In PENGB, the standard dosage recommended by guidelines is 20 mL of 0.375% ropivacaine, a dosage that has been proven safe through extensive clinical practice. 38 In this study, the experimental group received a mixture of 20 mL of 0.375% ropivacaine with 1 μg/kg of dexmedetomidine. Data on patients’ BP, SpO2, pain indicators, and others demonstrated the safety of dexmedetomidine as an adjunct. Furthermore, compared with the standard medication, dexmedetomidine exhibited the ability to better stabilize BP and SpO2 at the end of surgery. It also extended the duration of analgesia and improved early postoperative cognitive dysfunction.
Although this study provides valuable insights, it is essential to acknowledge its limitations. This includes the relatively short duration of the cognitive-preserving effect and the lack of long-term follow-up to assess its sustainability. In addition, future research could explore the optimal dosage and administration of dexmedetomidine to maximize its benefits while minimizing potential side effects. Moreover, other important neural injury biomarkers including Tau protein and NSE can be used as the marker for cognitive impairment. Tau protein is a microtubule-associated protein that normally maintains the stability of microtubule structures in neuronal axons. 39 NSE is a neuron-specific enolase primarily present in neurons and neuroendocrine cells. 39 It is released into the peripheral blood when neurons are injured or die, making it one of the biomarkers for neural system damage. 39 However, due to limitations in time and resources, we did not select these two biomarkers for our study.
Conclusions
In conclusion, the incorporation of dexmedetomidine as an adjunct to ropivacaine in PENGB for elderly patients undergoing THA appears to be a promising strategy for improving pain management, hemodynamic stability, and cognitive outcomes in the early postoperative period. This study adds to the growing body of evidence supporting the use of adjuvants like dexmedetomidine in nerve blocks to enhance perioperative care.
Footnotes
Data Availability
The data could be obtained upon request to the corresponding author.
Ethics Approval and Consent to Participate
The study was approved by the Second People’s Hospital of Hefei, Hefei Hospital affiliated to Anhui Medical University, and written informed consent was derived from the participants.
Authors’ Contributions
X.L., L.C., Y.S., and Y.L. conducted the experiments, collected and analyzed the data, and wrote the original article. X.L. conceived the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding to be declared.