
Abstract
The present study was conducted to evaluate the application and efficacy of autologous bone marrow infusion (ABMi) for improvement of liver function in patients with alcoholic liver cirrhosis (ALC). Five subjects and 5 control patients with ALC who had abstained from alcohol intake for 24 weeks before the study were enrolled. Autologous bone marrow cells were washed and injected intravenously, and the changes in serum liver function parameters, and the level of the type IV collagen 7S domain as a marker of fibrosis, were monitored for 24 weeks. The distribution of activated bone marrow was assessed by indium-111-chloride bone marrow scintigraphy. The number of cells infused was 8.0±7.3×109 (mean±standard error). The serum levels of albumin and total protein and the prothrombin time were significantly higher during the follow-up period after ABMi than during the observation period in treated patients, whereas no such changes were observed in the controls. In the patients who received ABMi, the Child-Pugh score decreased in all 3 who were classified as class B; the serum levels of type IV collagen 7S domain improved in 4 of the 5 patients; and bone marrow scintigraphy demonstrated an increase of indium-111-chloride uptake in 3 of the 4 patients tested. ABMi for patients with ALC helps improve liver function parameters in comparison with observation during abstinence and ameliorates the degree of fibrosis in terms of serum markers and bone marrow activation in most cases.
Introduction
L
BM cells have been shown to be capable of differentiating into the liver cell lineage, and transplantation of BM cells has considerable potential for regeneration of liver tissue [3 –6]. The degree of liver function and fibrosis as well as survival rate have been shown to improve significantly as a result of BM cell transplantation in animal models of severe liver injury [7,8]. We have experimentally investigated the potential of BM stem cells to differentiate into the hepatocyte lineage both in vitro or in vivo with a view to possible application for clinical trials aimed at liver regeneration [9 –12]. In this context, the effectiveness of CD34+ hematopoietic stem cell injection into the liver via the portal vein or hepatic artery had been shown to improve the serum levels of albumin and bilirubin [13,14]. Our research group has already reported the therapeutic effectiveness of whole-BM peripheral infusion, referred to as autologous BM cell infusion (ABMi) therapy for patients with cirrhosis with hepatitis B or C [15,16].
Alcoholic liver injury is a common liver disease worldwide. Although disease activity may be decreased by abstinence in the initial phase, it eventually progresses to cirrhosis and finally to death unless patients receive appropriate therapeutic intervention for both liver injury and alcohol abuse. Even if patients discontinue alcohol intake, those in whom the disease has progressed to advanced cirrhosis with marked liver fibrosis have a poor prognosis because of serious complications and liver cell dysfunction. Therefore, such patients require some form of liver-regenerative therapy, as well as abstinence, to improve the liver function. Since such patients are free of pathogens such as hepatitis B or hepatitis C that cause continuous liver necro-inflammation, ABMi might facilitate a degree of liver regeneration if abstinence is maintained along with appropriate nutritional care. Pai et al. reported that autologous infusion of expanded mobilized BM-derived CD34+ cells into patients with alcoholic liver cirrhosis (ALC) via the hepatic artery improved the serum levels of both bilirubin and transaminase, as well as the Child-Pugh score [17].
To investigate the effectiveness of ABMi for patients with ALC, we applied it to such patients and examined the resulting changes in liver function parameters. In addition, using indium-111-chloride (111In) BM scintigraphy, we tracked the infused BM cells after ABMi.
Patients and Methods
Patients
Patients with a diagnosis of advanced liver cirrhosis due to alcoholic liver injury were enrolled. All the patients were negative for both anti-hepatitis C virus antibody and hepatitis B surface antigen and had a history of excessive alcohol consumption exceeding 60 g/day of ethanol for >5 years. The patients were interviewed, and those who had abstained for >24 weeks before the interview were entered into the study. The inclusion criteria for clinical parameters were as follows: platelet count >50,000/mm3, total bilirubin <3 mg/dL, and absence of liver cancer on computed tomography (CT). Both heart and lung function were screened to confirm whether general anesthesia was possible. As a control group, we used patients who were not given ABMi, but who agreed to the use of their clinical data for study. Those patients had also been diagnosed as having ALC, and were matched to the subjects who received ABMi for age, sex, medication, and various biochemical parameters; their liver function parameters were compared with those of the subjects who received ABMi during the study period.
Autologous BM cell preparation and infusion into patients
A total of 400 mL BM was harvested from the ilium according to the standard procedure under general anesthesia and collected in a plastic bag containing heparin. After fat had been removed from the top of the bag, hydroxyethyl starch was added to a final concentration of 1%. Red blood cells were precipitated after 40 min of incubation at room temperature. We used an automated bench-top device (Cytomate; Takara Bio Inc., Otsu, Shiga, Japan), which is a functionally closed system incorporating a spinning membrane connected to a filter wash bag, for washing and concentrating the mononuclear cells (MNCs). The final cell products were washed, concentrated, and made up to a final volume of 105 mL. Five milliliters of the final cell product was subjected to the trypan blue dye exclusion test, endotoxin test, and fluorescence-activated cell sorting analysis. CD34+, CD44+, CD45+, and CD117+ cells were determined by flow cytometry at the central laboratory of SRL Inc., Tokyo, Japan. At 6 h after BM harvest, the final MNCs preparation was administered to each patient via the cubital vein by drip infusion. All the study protocols were approved by the ethics committee of Yamagata University School of Medicine, and written informed consent was obtained from all participants.
Follow-up of serological tests for liver function and fibrosis
The patients were followed up, and laboratory data were analyzed for 48 weeks in total, which included analyses once a month for 24 weeks before and after ABMi therapy. Patients who consumed more than 20 g alcohol/day during the analysis period were considered to have dropped out and excluded from further analysis. Primary outcomes were the safety and feasibility of ABMi therapy for ALC. The serum parameters representing liver function, including serum albumin, total protein, and prothrombin time, were evaluated before and after ABMi therapy. The Child-Pugh score calculated by summing the total points for the serum levels of albumin and total bilirubin, prothrombin time, ascites, and encephalopathy was used to evaluate the overall condition of patients with cirrhosis. To evaluate the changes in the degree of liver fibrosis in patients receiving ABMi, the serum levels of the type IV collagen 7S domain was monitored during the follow-up period. The liver function parameters of the control patients who succeeded in maintaining abstinence were followed up for the same period as that of patients who received ABMi.
Liver function calculated by single photon emission CT analysis
Analysis of the liver using single photon emission CT (SPECT) with a radiolabeled, specific hepatic binding protein, technetium 99m galactosyl-human serum albumin (Tc-GSA), was carried out according to the procedure we have previously reported [18]. SPECT analysis is useful for assessment of hepatic functional reserve [19,20]. Briefly, Tc-GSA (185 MBq) was injected intravenously, and SPECT data were obtained from 12 min 30 s to 17 min 30 s after the injection using a triple-headed camera (MULTISPECT 3; Siemens Medical Systems, Erlangen, Germany). The liver uptake ratio, that is, the actual percentage of the administered Tc-GSA dose incorporated into the liver, was quantified by calculating the percentage of the hepatic SPECT value relative to the preinjection syringe value. The liver volume was obtained from the SPECT data and calculated by the outline extraction method to determine the functional liver volume in cm3. The liver uptake ratio was then divided by the functional liver volume to obtain the liver uptake ratio per unit volume (liver uptake density; %/cm3). We assessed the obtained liver uptake density values of patients receiving ABMi before the treatment and 2 weeks after.
BM imaging by 111In scintigraphy
BM scintigraphy using 111In was performed in 4 of the 5 patients before and 1 week after ABMi therapy. BM scintigraphy is useful for evaluating the distribution of activated BM, mainly hematopoietic stem cells. The scintigraphy was conducted 48 h after an intravenous injection of 111In (74 MBq). The total 111In count was divided by the total number of pixels on the computer screen to obtain the 111In count per pixel, and this was used as an index of BM activation in patients before and 1 week after ABMi.
Statistical analysis
Statistical analysis was performed using t-test for paired or unpaired samples. Time courses of measurements of liver function parameters were analyzed by repeated-measures ANOVA. A 2-tailed P value of <0.05 was considered statistically significant. The data were expressed as mean±standard error. Analyses were performed using SPSS version 15.0 for Windows (SRSS, Chicago, IL).
Results
Patients characteristics
Five patients received ABMi therapy and were followed up. The baseline demographic features and clinical characteristics of these 5 patients are shown in Table 1. All the patients were men with a mean age of 64 (range: 59–75) years. One patient had ascites, and the other 4 had a history of ascites. All patients had previously undergone endoscopic sclerosing therapy for esophageal varices. CT demonstrated macroscopic cirrhosis with a high degree of liver deformity, and all patients had undergone liver biopsy before the study, which confirmed cirrhosis histologically. The baseline data for the patients who received ABMi in comparison with those for the controls with alcoholic cirrhosis who were matched for age, sex, medication, and liver function parameters are shown in Table 2. There were no significant differences in these baseline data between the 2 groups.
Number in parentheses indicates points in total Child-Pugh (C-P) score.
History of ascites.
History of endoscopic sclerosing therapy.
T.protein, total protein; T.bilirubin, total bilirubin; PT, prothrombin time activity; ICG-R15, indocyanin green test, retention 15 min.
N.S., not significant (t-test). The data are expressed by mean±standard error.
BCAA, branched chain amino acids; ABMi, autologous bone marrow infusion.
Cell products for ABMi and their characteristics
The characteristics of the cell products for ABMi are shown in Table 3. From 400 mL of autologous BM harvested from the ilium of each patient, the mean number of infused MNCs was 8.0±7.3×109. The viability of the MNCs was >90% in all cases. The percentages of CD34+, CD44+, CD45+, and CD117+ cells were 6.0%±1.8%, 90.1%±5.6%, 81.2%±6.4%, and 12.0%±3.5%, respectively.
MNC, mononuclear cell.
Changes in biochemical parameters before and after ABMi
The 5 patients receiving ABMi therapy were followed up for 48 weeks in total: for 24 weeks before and for 24 weeks after ABMi. The 5 controls were also followed up for a total of 48 weeks. Medication was not changed during the study period in any of the patients. The changes of liver function parameters, including serum albumin, total protein, and prothrombin time, are shown in Fig. 1. These parameters all showed an improvement in the patients who received ABMi; the mean level of serum albumin before and 24 weeks after ABMi improved from 3.3±0.2 to 3.8±0.2 g/dL, that of total protein improved from 6.9±0.2 to 7.7±0.1 g/dL, and the prothrombin time improved from 76.6%±6.1% to 87.6 %±6.0%. The levels of serum albumin, total protein, and prothrombin time during the follow-up period after ABMi were significantly higher than those during the period before ABMi (serum albumin; P=0.02, total protein; P=0.03, prothrombin time; P<0.01). However, no significant changes were observed in the levels of serum albumin and total protein, or prothrombin time, in the controls during the 48 weeks of observation. The Child-Pugh score decreased from 6.8±1.3 before ABMi to 5.8±0.8 at 24 weeks after ABMi. All of the 3 patients who were classified as Child class B with 7 points or higher before ABMi showed a decrease in their scores after ABMi therapy, and the remaining 2 patients classified as Child class A with 6 points or lower showed no change in their scores (Fig. 2).
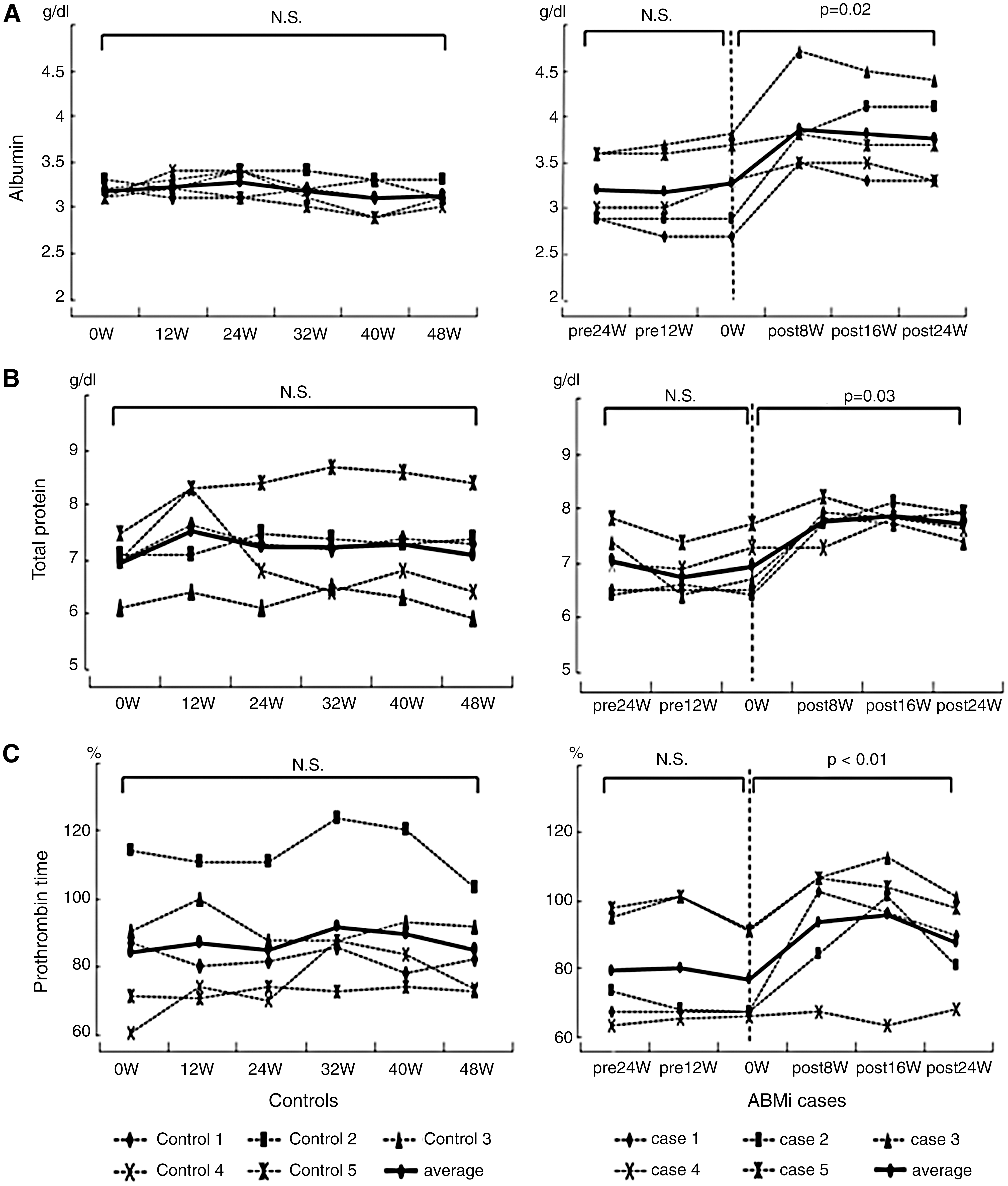
Changes in biochemical parameters before and after ABMi. The levels of serum albumin

Changes in Child-Pugh score after ABMi in comparison with those before. The Child-Pugh score decreased from 6.8±1.3 before ABMi to 5.8±0.8 at 24 weeks after ABMi. All of the 3 patients classified as class B, scoring 7 points or higher before ABMi, showed a decrease in their scores after the therapy.
Changes in liver fibrosis markers
The serum level of the type IV collagen 7S domain was evaluated in patients before and 24 weeks after ABMi. Improvement was observed in 4 of the 5 cases except for case no.5 at 24 weeks after ABMi therapy. The serum levels of the type IV collagen 7S domain decreased from 10.0±3.9 ng/mL before to 8.1±2.3 at 24 weeks after ABMi (Fig. 3), although the change was not significant (P=0.33), given the small number of cases examined.
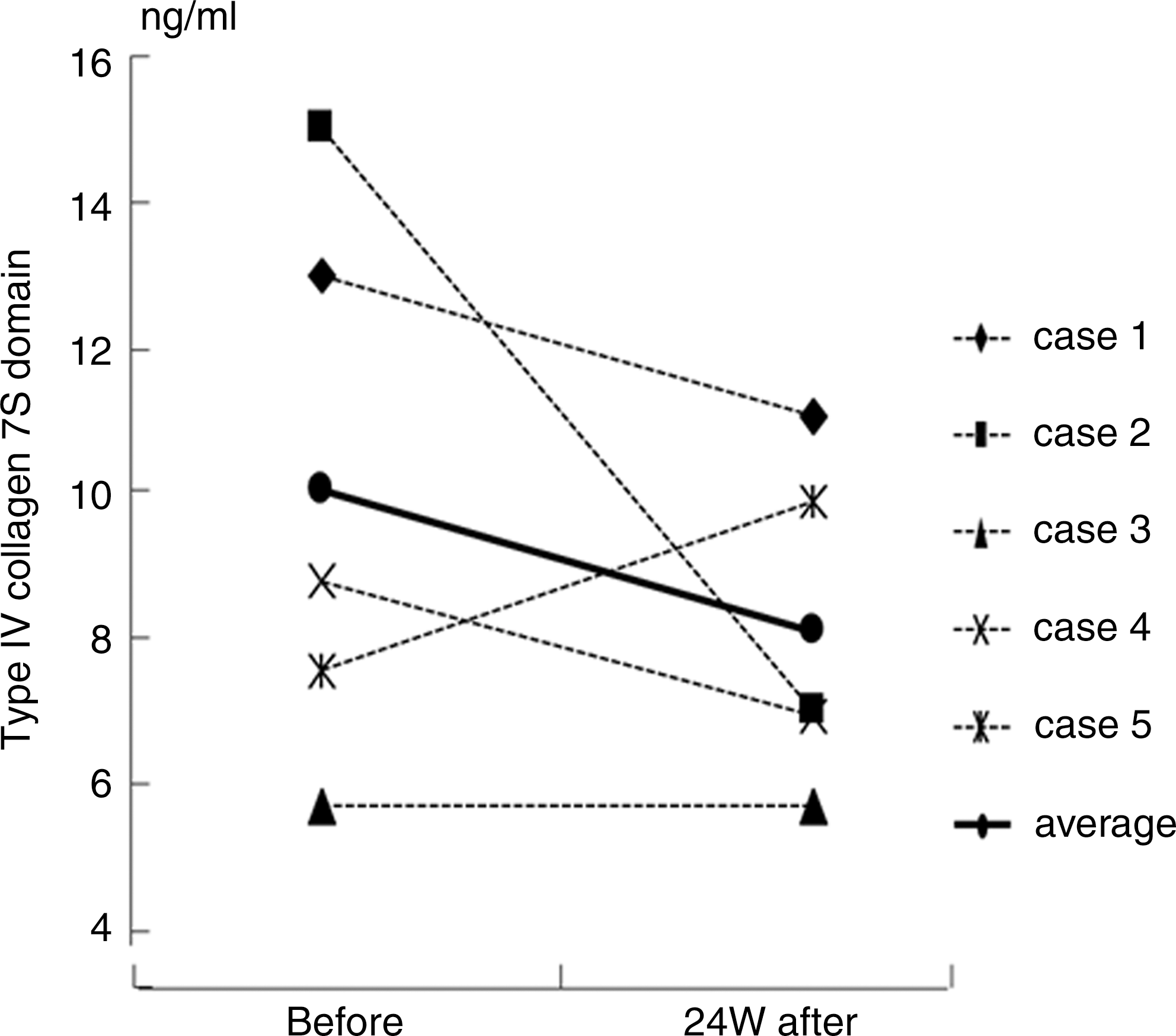
Changes in the levels of a liver fibrosis marker after ABMi in comparison with those before. The level of the type IV collagen 7S domain improved in 4 of the 5 cases, with the exception of case no.5, at 24 weeks after ABMi therapy, and their serum levels decreased from 10.0±3.9 ng/mL before to 8.1±2.3 ng/mL at 24 weeks after the therapy.
Estimation of liver function using Tc-GSA SPECT
The functional index was improved at 2 weeks in 4 of the 5 patients who received ABMi therapy, and was unchanged in one (case no.1). The mean functional index calculated by Tc-GSA SPECT tended to increase from 2.4±0.5×10−2 before ABMi to 2.7±0.6×10−2 at 2 weeks after (P=0.09) (Fig. 4).
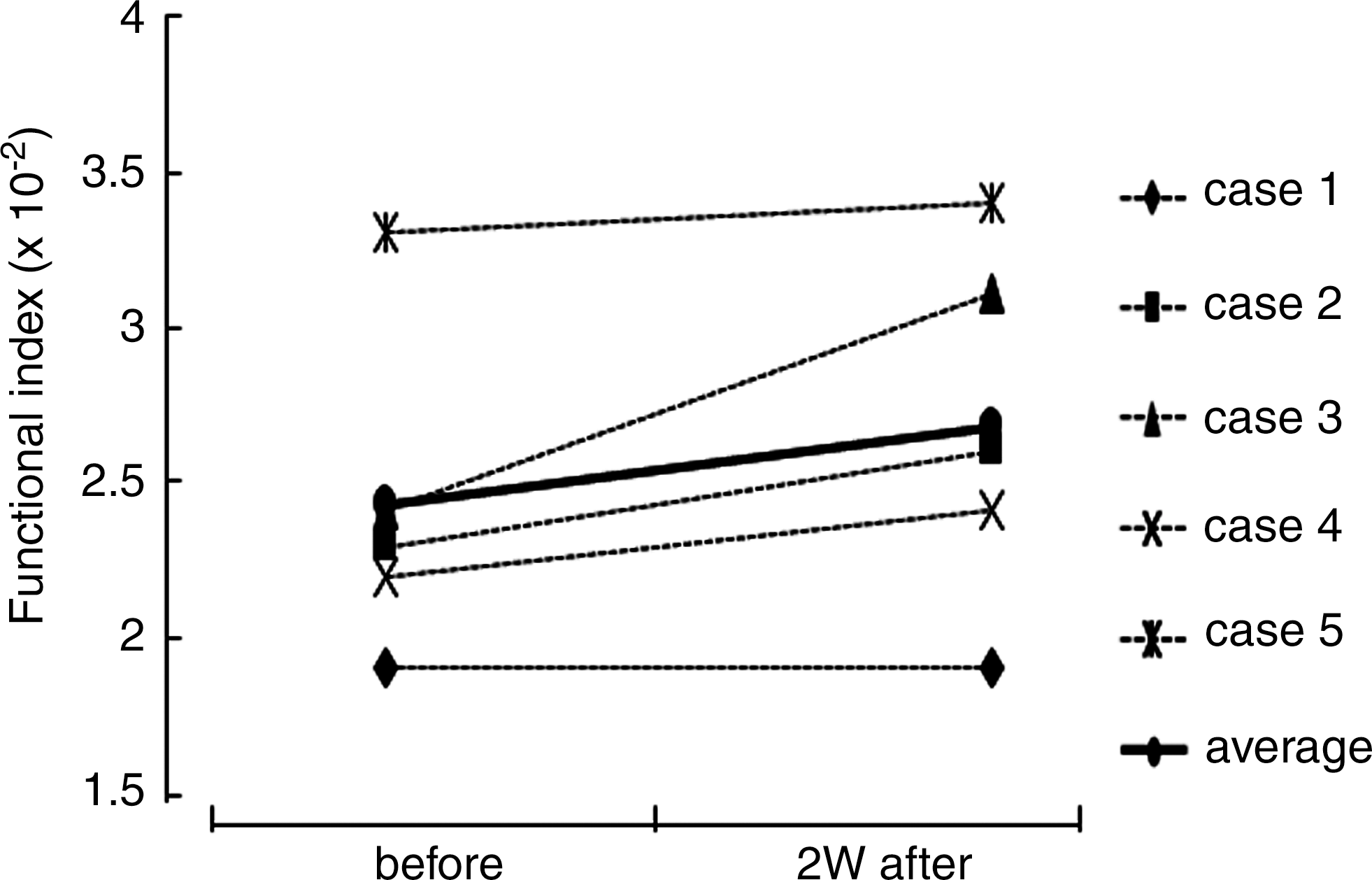
Estimation of liver function using technetium 99m galactosyl-human serum albumin single photon emission computed tomography. The functional index improved in 4 of the 5 cases, and did not change in one (case 1) after ABMi. The mean functional index tended to increase from 2.4±0.5×10−2 before ABMi to 2.7±0.6×10−2 at 2 weeks after (P=0.09).
Activated BM distribution assessed by 111In scintigraphy
The 111In count per pixel was increased in 3 of the 4 patients tested at 1 week after ABMi therapy, but was not increased in case no.5. The average 111In count per pixel in these 4 cases increased from 3.7±0.9 before ABMi to 4.4±1.3 at 1 week after (Fig. 5A), although the changes were not significant (P=0.23), given the small number of cases. The BM image in case no. 2, with the highest increase in the 111In count after ABMi therapy, is shown in Fig. 5B. Activation of BM cells in case no.2 was demonstrated by an increase in the 111In count per pixel from 4.5 before to 6.3 at 1 week after ABMi.
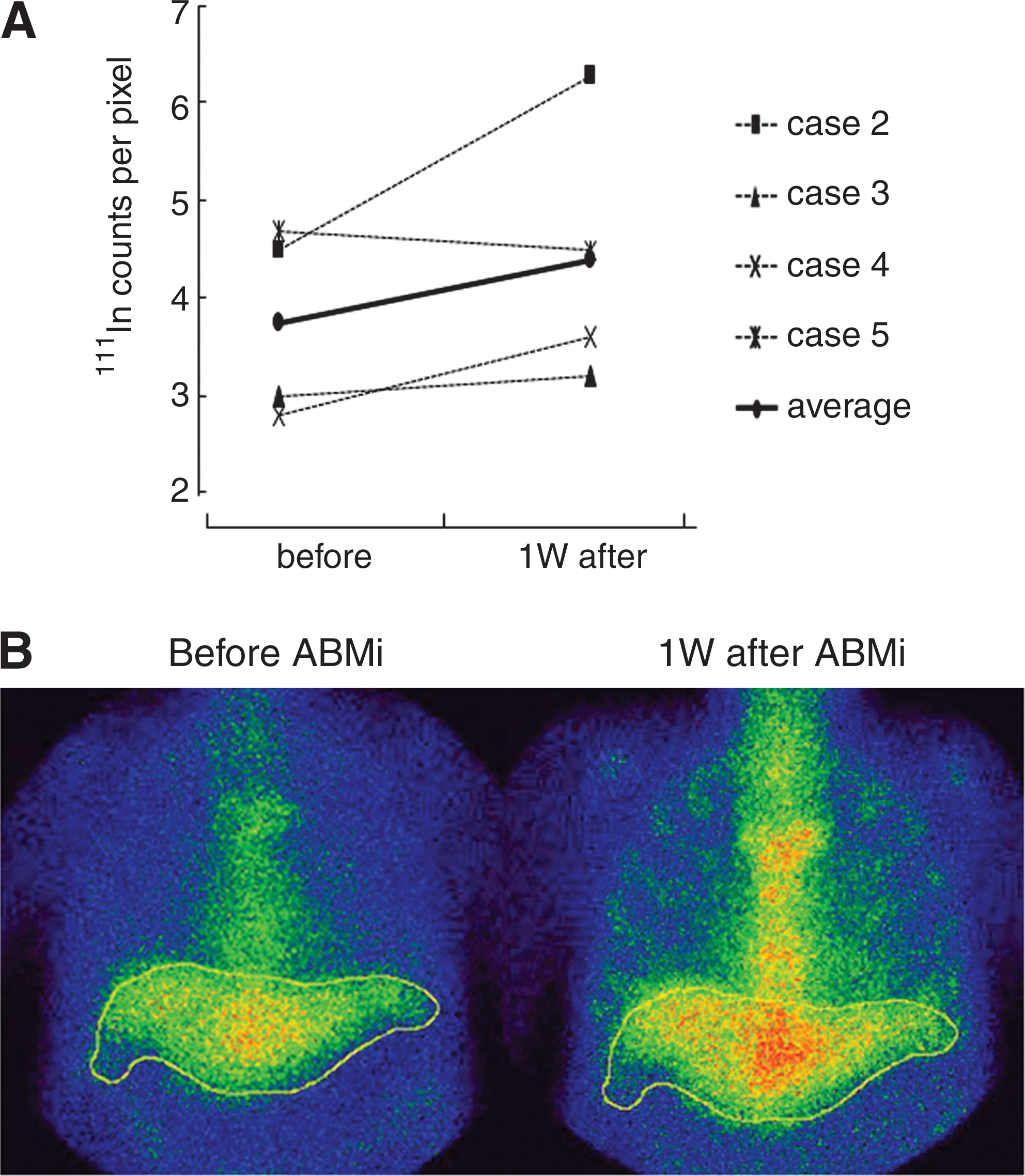
Activated BM distribution demonstrated by indium-111-chloride (111In) scintigraphy.
Complications
None of the 5 patients who received ABMi therapy exhibited any serious complications during or after the procedure.
Discussion
This study showed that ABMi for patients with ALC could be performed safely under general anesthesia and that it improved their liver function parameters including the serum levels of albumin and total protein and the prothrombin time. The Child-Pugh score also improved in all 3 patients who had a score higher than 7, which was classified as class B. Further, ABMi resulted in induction of hepatic functional reserve, as suggested by Tc-GSA SPECT imaging as well as reduction of the serum levels of the fibrosis marker in 4 of the 5 cases examined.
It is generally accepted that the results of laboratory tests can be modified by drug administration or infusion of albumin products or plasma. Although both patients treated with ABMi and controls had received several types of medication, the administered drugs were not changed during the study period, whereas the patients abstained from alcohol and no blood products were supplied. Abstinence is an important factor to consider when selecting patients for ABMi, because ALC is an irreversible liver condition resulting from chronic inflammation attributable to the toxic effect of ethanol on the liver. For enrollment in the present study, patients who showed marked deformity of the liver on CT, and histologically proved cirrhosis, were required to have abstained from alcohol for at least 24 weeks. No changes in liver function parameters were found as a result of an abstinence in either the controls or the patients treated with ABMi in the period before ABMi. However, the results of the present study suggest that liver function parameters can be improved by ABMi in patients with ALC. A recent study has shown that patients who undergo orthotropic liver transplantation for alcoholic liver disease have a rate of recidivism as high as 28% at 9 years [21]. Therefore, both careful observation and adequate intervention in relation to abstinence may be required for patients after ABMi.
Although BM stem cell treatment for liver cirrhosis is an attractive strategy in the field of liver regenerative cell therapy, many concerns need to be addressed [22,23]. It is still unclear how infused BM cells work for the improvement of liver function. We have demonstrated experimentally that BM cells transplanted into the spleen of rats with liver damage induced by carbon tetrachloride express liver-specific proteins such as alpha-fetoprotein in their cytoplasm in the recipient liver [10]. A clinical trial of ABMi for patients with cirrhosis has also demonstrated that the number of alpha-fetoprotein-positive cells was increased significantly in the liver, relative to the situation before ABMi. In addition, ABMi appeared to induce hepatocyte proliferation in the liver, as expression of proliferating cell nuclear antigen, a marker of hepatocyte proliferation, was significantly increased after ABMi in comparison with the pretreatment situation [15]. Another study has shown that intraportal administration of autologous CD133+ BM cells and subsequent portal venous embolization of right liver segments resulted in a 2.5-fold increase in the mean proliferation rate of the left lateral segment, in comparison with controls not receiving BM transfusion [24]. These data suggest that transplanted BM cells have a potential role in liver regeneration and proliferate in the recipient liver and that this process is likely to occur early after ABMi, as Tc-GSA SPECT analysis in the present study demonstrated an increase in the liver function index of most patients 2 weeks after ABMi. However, since it is still unclear whether fully functional hepatocytes are induced by ABMi, the characteristics of BM stem cells that show hepatocyte differentiation should be elucidated further. In addition, to elucidate the cell-cell communication in the extracellular microenvironment that would be important for tissue repair, many markers originating from the different cell types among MNCs should be investigated in the future.
The tracking of BM cells infused into the human body as a means of monitoring cell engraftment after ABMi has not been previously reported. In the present study, BM scintigraphy using 111In before and after ABMi showed that the distribution of activated BM was enhanced systemically after ABMi, including the liver, in 3 of the 4 patients examined. Although the process of migration of infused BM cells to the liver remains unknown, clarification of the factors responsible could yield important data for improving the efficiency of transplantation. In fact, ABMi case no. 2, in which the greatest increase in the 111In count was observed 1 week after ABMi, showed a marked decrease in the concentration of the type IV collagen 7S domain, as shown in Fig. 3, as well as a marked improvement of liver function parameters, as shown in Fig. 1. In contrast, ABMi case no.5 was only one showing no change in the 111In count at 1 week after ABMi, and the only case in which the level of the type IV collagen 7S domain did not decrease after ABMi. Effective migration of infused BM cells to the liver may ameliorate liver fibrosis, because such cells have been shown experimentally to produce and secrete anti-fibrosis factors such as matrix metalloproteinase-9 [7]. At this time, the factors that determine the difference between effectiveness and noneffectiveness are unclear. Collateral circulation resulting from the portal vein disorganization that characterizes liver cirrhosis may affect the flow and effective migration of infused BM cells to the liver, and, thus, migration of infused cells to the liver may partly depend on the portal venous pressure. Further, the expression levels of cellular adhesion molecules associated with the attachment of infused cells to liver tissue may vary a great deal among patients. It is important to determine the adhesion molecules that are induced in the liver tissue of patients receiving ABMi. Further studies are needed to clarify the mechanisms involved in the migration of infused BM cells to the liver.
The present study did not demonstrate the long-term effectiveness of this therapy in terms of survival rate or improvement in the quality of life. Such effects will need to be evaluated by a randomized controlled study in the future. In addition, improvements in the methods of delivering infused BM cells to the human body should also be investigated further. We are currently conducting experiments aimed at improving the effectiveness of this therapy by investigating the long-term culture conditions for BM cells, the optimum cell population to be employed, the effectiveness of repeated transplantation of BMCs, and the optimum route of cell delivery. We have already confirmed both the safety and short-term efficacy of ABMi therapy for various liver diseases [15,16], and these basic data are expected to be of value for improving ABMi therapy in the near future.
In summary, ABMi therapy for patients with alcoholic cirrhosis has been shown to improve liver function parameters, in contrast to observation accompanied by abstinence from alcohol. The markers of liver fibrosis, hepatic functional reserve, and BM cell activation were improved in most of the patients who received ABMi therapy. However, the degree of effectiveness of ABMi is likely to differ among patients, and the present results should still be considered in terms of a pilot study. Further investigation of factors associated with the effectiveness of this therapy is warranted, and future studies will need to assess the safety of this therapy and its effect on liver function in a large number of patients, together with its long-term effectiveness, in terms of survival rate and quality of life.
Footnotes
Acknowledgments
This study was supported in part by a grant from the Ministry of Health, Labor, and Welfare of Japan, and also in part by a Grant-in-Aid from the Global COE program of the Japan Society for the Promotion of Science. The authors thank Dr. K. Okita for his support toward this study.
Author Disclosure Statement
The authors declare that they have no conflict of interest.