
Abstract
Currently, there is no effective strategy for the treatment of spinal cord injury (SCI). A suitable combination of modern hydrogel materials, modified to effectively bridge the lesion cavity, combined with appropriate stem cell therapy seems to be a promising approach to repair spinal cord damage. We demonstrate the synergic effect of porosity and surface modification of hydrogels on mesenchymal stem cell (MSC) adhesiveness in vitro and their in vivo survival in an experimental model of SCI. MSCs were seeded on four different hydrogels: hydroxypropylmethacrylate-RGD prepared by heterophase separation (HPMA-HS-RGD) and three other hydrogels polymerized in the presence of a solid porogen: HPMA-SP, HPMA-SP-RGD, and hydroxy ethyl methacrylate [2-(methacryloyloxy)ethyl] trimethylammonium chloride (HEMA-MOETACl). Their adhesion capability and cell survival were evaluated at 1, 7, and 14 days after the seeding of MSCs on the hydrogel scaffolds. The cell-polymer scaffolds were then implanted into hemisected rat spinal cord, and MSC survival in vivo and the ingrowth of endogenous tissue elements were evaluated 1 month after implantation. In vitro data demonstrated that HEMA-MOETACl and HPMA-SP-RGD hydrogels were superior in the number of cells attached. In vivo, the highest cell survival was found in the HEMA-MOETACl hydrogels; however, only a small ingrowth of blood vessels and axons was observed. Both HPMA-SP and HPMA-SP-RGD hydrogels showed better survival of MSCs compared with the HPMA-HS-RGD hydrogel. The RGD sequence attached to both types of HPMA hydrogels significantly influenced the number of blood vessels inside the implanted hydrogels. Further, the porous structure of HPMA-SP hydrogels promoted a statistically significant greater ingrowth of axons and less connective tissue elements into the implant. Our results demonstrate that the physical and chemical properties of the HPMA-SP-RGD hydrogel show the best combination for bridging a spinal cord lesion, while the HEMA-MOETACl hydrogel serves as the best carrier of MSCs.
Introduction
H
Hydrogels are synthetic scaffolds, which makes them easily amenable to physical and chemical modifications. Our ambition is to develop a modified hydrogel in a step-by-step process that would make the implant most attractive for neural tissue reconstruction. In this study, we focused on three variables (architecture, chemical basis, and RGD peptide sequence) with regard to using the hydrogel as a stem cell carrier as well as a bridging scaffold.
One of the key properties of the implants is their architecture, the inner structure of the building blocks, and the hydrogels' pores. The scaffolds of several hydrogels are based on a web-like inner structure, while others are composed of globular particles with spaces (pores) among them. While both types have been shown to support some tissue ingrowth, no study has assessed which type of structural composition is more advantageous for neural tissue regeneration [3 –6].
Another vital element is the chemical composition of the building blocks, which affects the attachment of stem cells and neural elements. Hydroxyethylmethacrylate (HEMA)- and HPMA-based implants are the most common types of methacrylate scaffolds. There has been, so far, only a single study comparing these two types of scaffolds, and only in a model of traumatic brain injury [7].
Third, the environment of the hydrogel scaffold may be enriched by the attachment of functional groups. Proteins that contain the Arg-Gly-Asp (RGD) attachment site constitute a major recognition component of a cell adhesion system. The RGD sequence is the cell attachment site of a large number of adhesive extracellular matrix, blood, and cell surface proteins [8]. Its attachment to the hydrogel and an evaluation of its usefulness in SCI treatment has led to the conclusion that it enhances the biocompatibility performance of the hydrogel [9]. Nonetheless, no comparative study using the same hydrogel with and without an attached RGD sequence has been performed to determine the effect of the RGD sequence on SCI repair.
MSCs are multipotent progenitor cells. In culture, they can differentiate into several types of cells, such as osteoblasts, chondrocytes, and adipocytes [10]. However, they are often used in regenerative medicine for their ability to promote the production of anti-inflammatory cytokines and growth factors [11]. Their positive effect on functional outcome and tissue preservation in SCI may, therefore, also be explained by providing neurotrophic support for the damaged tissue, as suggested by some studies [12,13]. MSCs can be transplanted either systemically (intravenous, intra-arterial, and intrathecal implantation) or locally (intralesional injection, MSCs seeded on a carrier) [14 –16]. According to some studies, local transplantation seems to be more effective in terms of functional improvement and tissue repair [17]. Using a hydrogel as a carrier of MSCs to the site of injury may be another form of local stem cell transplantation. In light of this data, combining MSCs with hydrogels thus represents a promising approach to SCI repair.
The goal of implanting a hydrogel is to bridge a spinal cord lesion. The best bridge should form a scaffold for the ingrowth of axons, which should ultimately reconnect the caudal and the cranial stumps. Further, the bridge should also provide a scaffold for the ingrowth of blood vessels, providing the nutritional support for tissue regeneration. In addition, the hydrogel should be able to carry MSCs, which provide trophic support to the host tissue and improve functional outcome after SCI. The goal of this study was to find the most appropriate combination of factors in methacrylate hydrogels that would contribute to providing the best scaffold for tissue repair in SCI.
Materials and Methods
Hydrogel preparation
HEMA-MOETACl (HEMA with a positive surface charge)
Macroporous hydrogels based on 2-HEMA with MOETACl were prepared by the radical copolymerization of monomers (HEMA 0.67 g, MOETACl 0.12 g, and ethylene dimethacrylate 0.019 g as a cross-linker) in the presence of fractionated particles of NaCl with a diameter of 50–90 mm (10.02 g) and the solvent polyethylene glycol (MW 400, 3.79 g), using an initiator 2,29-azo-bis-isobutyronitrile (0.0067 g) for 8 h at 80°C. Polymerization was performed in a pelleting apparatus as previously described [18]. After polymerization, the hydrogels were washed with water and physiological saline (once a day for 5 days). The hydrogels thus obtained had communicating pores (2–3×106 pores per cm3) with an average size of 80 μm and a specific pore volume of 0.45 (combined volume of all pores in 1 cm3 of hydrogel). The morphology of the hydrogel is shown in Fig. 1A.

The ultrastructure of HEMA and HPMA hydrogels.
HPMA-SP with and without RGD
Peptide synthesis
The oligopeptide [methacryloyl-glycine-glycine-arginine-glycine-aspartate (MAGGRGD)] was prepared using a solid-phase peptide method, with methacryloylation as the last step. After completing the synthesis, the peptide was cleaved from the resin and deprotected using a mixture of 95% trifluoroacetic acid, 2.5% tri-isopropylsilane, and 2.5% water. After evaporation of the cleavage and deprotecting mixture, the peptide was precipitated in cold ether (0°C), filtered, and dried under vacuum. The MAGGRGD was then purified on HPLC with a UV detector (separative column C18), dried, dissolved into distilled water, and lyophilized. The purity of the cleaned product was measured on MALDI-TOF [MS 529.7 (M+H)] and an HPLC-UV detector (separative column C18, retention time 8.4 min) and was found to be 95%.
Hydrogel synthesis
Macroporous hydrogels were prepared by the radical polymerization of monomers in a pelleting apparatus as described earlier [19] at 60°C for 8 h. The composition of the monomers was as follows: HPMA 0.7 g, PEG 3.79 g, azobis(isobutyronitrile) (AIBN) 0.007 g, EDMA 0.019 g, MAGGRGD 0.007 g, and NaCl 10.02 g. After polymerization, the macroporous hydrogel was removed from the pelleting apparatus, washed in a laminary box with distilled water (10 times for 1 day each) and saline (5 times for 1 day each). The morphology of both hydrogels, including the size and the number of pores, is analogous to that of the HEMA-MOETACl hydrogel. The morphology of the hydrogel is shown in Fig. 1B.
HPMA-HS-RGD
Peptide synthesis
The same procedure as described earlier for HPMA-SP-RGD was used.
Hydrogel synthesis
Macroporous hydrogels were prepared by the radical precipitating polymerization of monomers (HPMA, 0.08 mol%, MOETACl, 0.08 mol%, MAGGRGD, 2.6 wt%) with the cross-linking agent methylenebis(acrylamide) and the initiator AIBN, 0.3 wt%, in a solvent/precipitator mixture (dimethyl sulfoxide/acetone, 10 g in a ratio of 1/13) under a nitrogen atmosphere in a sealed glass ampule at 50°C for 16 h. After polymerization, the macroporous hydrogel was removed from the ampule and washed in a laminary box with absolute ethanol (thrice for 1 day each), 50% ethanol/water (thrice for 1 day each), distilled water (thrice for 1 day each), 0.5% NaHCO3 in water (for 1 day), distilled water (five times for 1 day each), and saline (once a day for 5 days). The hydrogels were macroporous; the communicating (interconnecting) pore fraction of the hydrogel was determined by immersing a dry xerogel in heptane and determining the weight of the heptane that penetrated into the communicating pores. Based on these measurements, 38% of the porous hydrogel was formed by pores, and 95% of these pores were communicating. The estimated water content, which was determined from the weight of the xerogel and the gel swollen to equilibrium, was between 85% and 90%. The mechanical properties of the resulting macroporous structure mimic those of the rat nervous tissue, and all of the properties were generally similar to those of HPMA hydrogels already published [3]. The morphology of the hydrogel was visualized by scanning electron microscopy (SEM, Fig. 1C).
Scanning electron microscopy
A small piece of wet sample was flash frozen in liquid nitrogen and fixed with ice onto the precooled stage (−10°C) of an SEM microscope. The top frozen layer was cut off; then, the freshly cut frozen surface was observed under cryo low-vacuum conditions (T=− 10°C; P=100 Pa; LFD detector).
Seeding of MSCs on hydrogels
To enable the more easily distinguishable and stable tracking of transplanted cells, rat MSCs expressing enhanced green fluorescent protein (GFP) isolated from GFP+ rats were used in our experiments. The transgenic Sprague–Dawley rats [SD-Tg(CAG-EGFP)CZ-004Osb] were kindly provided by Dr. Masaru Okabe (Osaka University, Japan) [20], bred at the laboratory of Dr. Martin Marsala (University of California, San Diego, CA), then subsequently sent to our Institute, and bred in our animal facility.
The cells were isolated by extrusion of the bone marrow into a tissue culture Petri dish. The cells were plated in DMEM/10% fetal bovine serum with primocin (2 μL/mL). After 24 h, the nonadherent cells were removed by replacing the medium. When cells reached 75%–90% confluence, they were detached by trypsin/EDTA treatment and transferred into 75-cm2 cell culture flasks. MSCs from passage 3 were used for in vitro and in vivo experiments. On the day of hydrogel seeding, the cultures were trypsinized with a 0.25% trypsin/ethylenediaminetetraacetic acid (EDTA) solution. Then, 2 million cells per milliliter were placed in a test tube along with a 2×2×2 mm cube of hydrogel and put on a shaker (500 rpm) for 15 min in order to seed the 3D scaffold.
Hydrogel implantation
Sixteen male rats (Wistar, Velaz, Czech Republic) with a weight of 250–300 g underwent a hemisection at the Th8 level. Four implantations of each of the four types of hydrogels seeded with MSCs were performed. The animals were intraperitoneally injected with pentobarbital for anesthesia (0.06 g/1 kg i.p.); one dose of ATB (gentamicin 8 mg/1 kg i.m.), atropine (0.08 mg/1 kg s.c.), and mesocain to enhance local anesthesia (1 mg/1 kg s.c.+i.m.) was administered preoperatively. Further, the rats received cyclosporine (Novartis; 10 mg/kg i.p.) before surgery and then daily until sacrifice. A linear skin incision was performed above the spinous processes of Th7-9; the paravertebral muscles were detached from the laminae Th8-9, and a Th8 laminectomy was performed. The dura was incised, and less than 1 mm3 of spinal cord tissue was excised to form a hemisection cavity. The hydrogels were properly trimmed to adjust to the size and shape of the cavity. The hydrogel was implanted in such a way as to ensure that it would firmly adhere to the edges of the hemisection cavity without causing any undue pressure onto the surrounding spinal cord tissue. The dura was sutured with Dafilon 10/0 thread (BBraun; Aesculap). The muscles and skin were sutured, and the animals were housed two in a cage with food and water ad libitum. This study was performed in accordance with the European Communities Council Directive of November 24, 1986 (86/609/EEC) regarding the use of animals in research and was approved by the Central Commission for Animal Protection of the Academy of Sciences of the Czech Republic in Prague.
Tissue processing and histology
Hydrogels in vitro
Cell density in the hydrogels was evaluated on day 1 (2 h after incubation), and then on the 7th and 14th days of cultivation. Each block of hydrogel was removed from the medium, washed with PBS, and bathed in 10%, 20%, and then a 30%-sucrose solution. From four to seven samples for each hydrogel and time period were prepared for evaluation. The blocks were frozen and cut into 20-μm-thick slices. Twenty slices were randomly selected for each type of hydrogel, and the amount of GFP positivity was calculated.
Hydrogels in vivo
On the 28th postoperative day, animals (n=16) were deeply anesthetized with an intraperitoneal injection of overdose pentobarbital and perfused with physiological saline followed by 4% paraformaldahyde in 0.1 M phosphate buffer. The spinal cord was left in bone overnight, then removed, and postfixed in the same fixative for at least 1 week.
A 3 cm-long segment of the spinal cord containing the lesion site was dissected out, and a series of 40 μm-thick longitudinal sections was collected. Hematoxylin–eosin and cresyl violet stainings were performed using standard protocols, and the slides were specifically evaluated using an Axio Observer D1 microscope (Carl Zeiss Microimaging GmbH) for an adverse foreign-body-type granulomatous reaction and the presence of connective and nervous tissue elements inside the hydrogel. For immunohistochemical studies, the following primary antibodies and dilutions were used: Cy3-conjugated anti-GFAP (1:200; Sigma-Aldrich) to identify astrocytes, anti-NF 160 (1:200; Sigma-Aldrich) to identify neurofilaments, and RECA-1 (1:50; Abcam) to identify endothelial cells of blood vessels. Alexa Fluor 594 goat anti–rabbit IgG (1:200; Invitrogen) and Cy3-conjugated anti-mouse IgM (1:100; Invitrogen) were used as secondary antibodies. Micrographs were taken using an LSM 510 DUO laser scanning confocal microscope (Zeiss).
Calculating MSCs on hydrogels and statistical analysis
Using Axio Vision 4.8 software (Carl Zeiss Microimaging GmbH), a semiquantitative estimate of the number of MSCs was made using 20 slices from four to seven in vitro samples for each hydrogel and time period and 6–7 slices of each spinal cord for the in vivo part of the study. We analyzed the number of green objects regardless of the size of each object (number of areas), the total number of the green objects (sum of areas), and the intensity of the green color on each slice (densitometry). However, when the shape of the object was obviously not an MSC, it was manually excluded in order to avoid counting artifacts. Multiplying the “sum of areas” and the “densitometry” parameters, we obtained a semiquantitative parameter directly related to the number of cells in the hydrogel both in vitro and in vivo.
Further, we randomly evaluated five slices from each hydrogel and time period (day 1, 7 and 14) and calculated the total number of MSCs and the number of spindle-shaped MSCs. The ratio of spindle-shaped MSCs to the total number of MSCs was determined.
The infiltration of the hydrogels by the ingrowth of neural processes and blood vessels was evaluated in two peripheral zones and the central zone of the hydrogel. The ingrowth was quantified using six slices from each spinal cord on average. Each calculation was divided by the area of the hydrogel implant, as the hydrogels did not always perfectly match the shape and size of the analysis window. Thus, the amount of ingrowth of axons and blood vessels was expressed as a percentage of the total area. We used the same software as for MSC quantification.
The mean values are reported as mean±standard error of the mean. Intergroup differences were analyzed using ANOVA and Student's two-sample t-test (probability values<0.05 and <0.01 were considered statistically significant).
Results
MSCs seeded on hydrogels: in vitro study
HEMA-MOETACl hydrogel
On day 1, most MSCs were on the surface, while there were a few in the central part of the hydrogel. Many cells were in clusters, and more than 90% of the cells were spindle shaped (Fig. 2A). On day 7, the number of cells remained practically stable. Many cells were still on the surface; however, many were also diffusely spread throughout the whole volume of the hydrogel. We saw a few MSCs in clusters. On day 14, there was a statistically significant decrease in the number of MSCs compared to days 1 and 7. On days 7 and 14, more than 90% of the cells remained spindle shaped.

Survival of MSCs on hydrogels in vitro. Many spindle-shaped MSCs were present on the HEMA-MOETACl hydrogel
HPMA-SP-RGD hydrogel
The number of MSCs on the HPMA-SP-RGD hydrogel was comparable to that on the HEMA-MOETACl hydrogel on day 1. More than 90% of the cells were globular. On days 7 and 14, we saw a gradual decrease in the number of the MSCs. However, many cells were spindle shaped on day 7 and 14 (more than 50%, Fig. 2B). Despite the trend toward a gradual decrease in the number of cells over time, this did not reach statistical significance. The data are summarized in Fig. 3.

Survival of MSCs on the four modified methacrylate hydrogels on days 1, 7, and 14 in vitro. *P<0.05 (vs. HPMA-HS-RGD), **P<0.05 (vs. HPMA-HS-RGD, † P<0.05 (vs. HPMA-SP), ‡ P<0.01 (vs. HPMA-SP), ▴ P<0.05 (vs. HPMA-SP-RGD).
HPMA-SP and HPMA-HS-RGD hydrogel
Significantly fewer MSCs adhered on the HPMA-SP and HPMA-HS-RGD compared with the HEMA-MOETACl and HPMA-SP-RGD hydrogels on days 1, 7, and 14. Most cells resided on the surface of the hydrogel on day 1, while on days 7 and 14, they were spread more diffusely. A few cells were in clusters, especially on day 1; nonetheless, the majority of MSCs were diffusely spread in both types of hydrogel. A small number (less than 10%) of MSCs were spindle shaped on the HPMA-SP hydrogel, while others were globular in shape (Fig. 2C). On the other hand, 100% of the cells on the HPMA-HS-RGD hydrogel were globular (Fig. 2D). The data are summarized in Fig. 3.
Bridging the spinal cord lesion with hydrogels
During implantation, all three HPMA-based hydrogels were soft and filled the hemisection cavity well with excellent adherence. Both HPMA-SP(-RGD) hydrogels were very soft, very well filling the shape of the cavity, compared with the HPMA-HS-RGD hydrogel. On the other hand, the HEMA-MOETACl hydrogel was harder compared with the three HPMA-based hydrogels. No foreign body-type giant-cell granulomatous reaction was found in all four evaluated hydrogels.
All four hydrogels bridged the hemisection cavity with minimal or no pseudocystic cavities (Fig. 4A–D). All of them adhered well to the spinal cord. A significant infiltration of scar tissue was present in the border zone between the HEMA-MOETACl hydrogel and the spinal cord (Fig. 4E), none in the case of the three HPMA-based hydrogels. The HPMA-HS-RGD hydrogel exerted pressure on the surrounding spinal cord tissue, recognized from small tissue deviation, as opposed to the HPMA-SP and the HPMA-SP-RGD hydrogels. The pores of the HEMA-MOETACl and the HPMA-HS-RGD hydrogels were filled with connective tissue, mostly comprising collagen and fibroblasts (Fig. 4E, F); while the HPMA-SP and the HPMA-SP-RGD hydrogels were loosely filled with connective tissue (Fig. 4G). No astrocytes grew inside any of the four hydrogels (Fig. 4H).
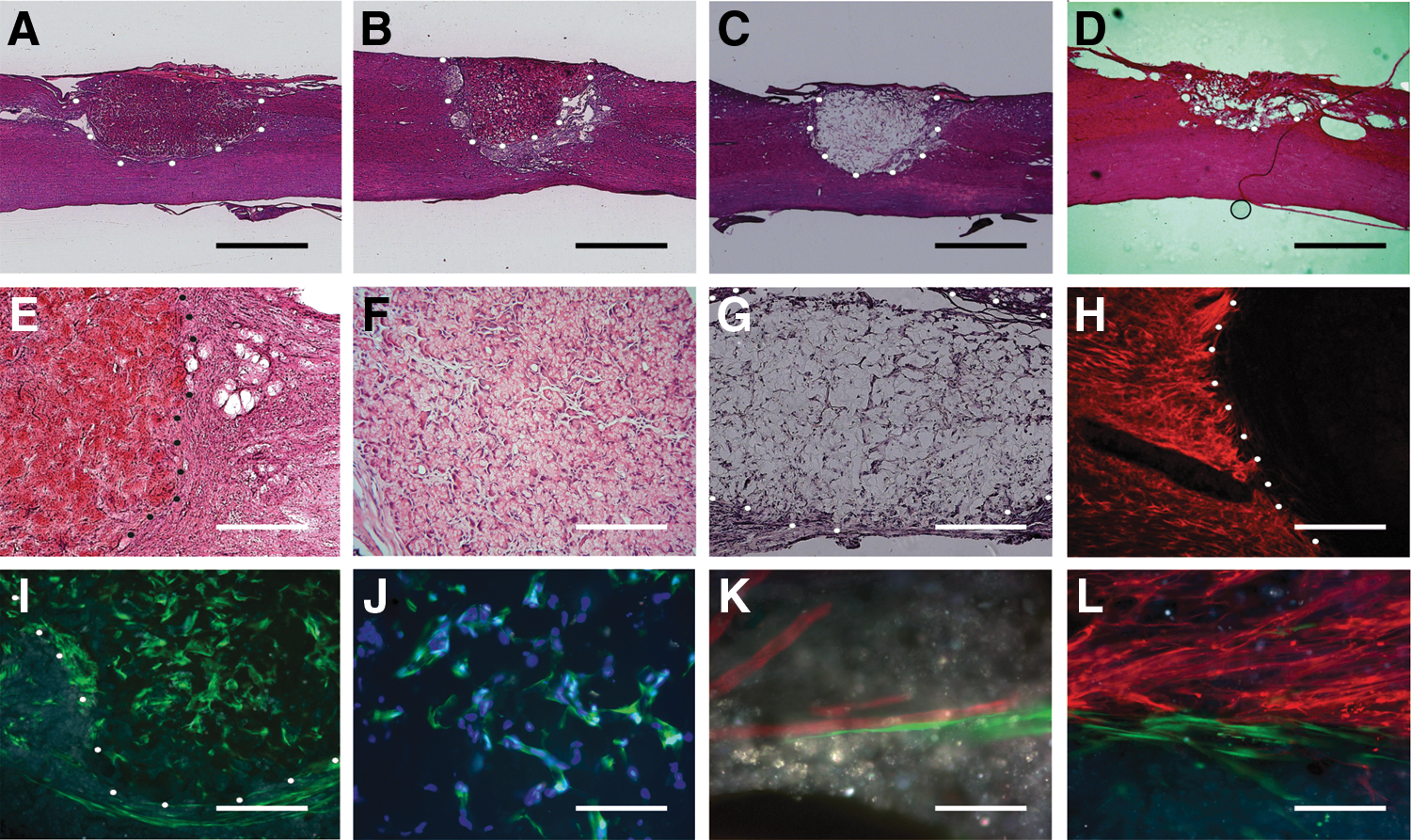
Bridging acute SCI with modified methacrylate hydrogels 1 month after implantation. HEMA-MOETACl
MSCs seeded on hydrogels bridging the SCI
The cells were present predominantly inside all four hydrogel scaffolds, in the bordering spinal cord tissue, and in the scar tissue between the spinal cord and the hydrogel (Fig. 4I). Inside the scaffolds, the cells were diffusely dispersed (Fig. 4J); many were present along newly formed blood vessels (Fig. 4K). In the border scar tissue, the cells were spindle shaped with long processes along the scar tissue, which was especially apparent in the HEMA-MOETACl hydrogels (Fig. 4L).
We evaluated the relative number of MSCs in all four hydrogels 1 month after implantation. MSCs were most abundant in the HEMA-MOETACl hydrogel (mean value=6.69×106±1.81×106). Significantly fewer MSCs were present in the HPMA-SP and the HPMA-SP-RGD hydrogels (0.94×106±0.27×106 in and 0.28×106±0.06×106, respectively) and the fewest cells in the HPMA-HS hydrogel (28.18×103±8.48×103). The data are summarized in Fig. 5.
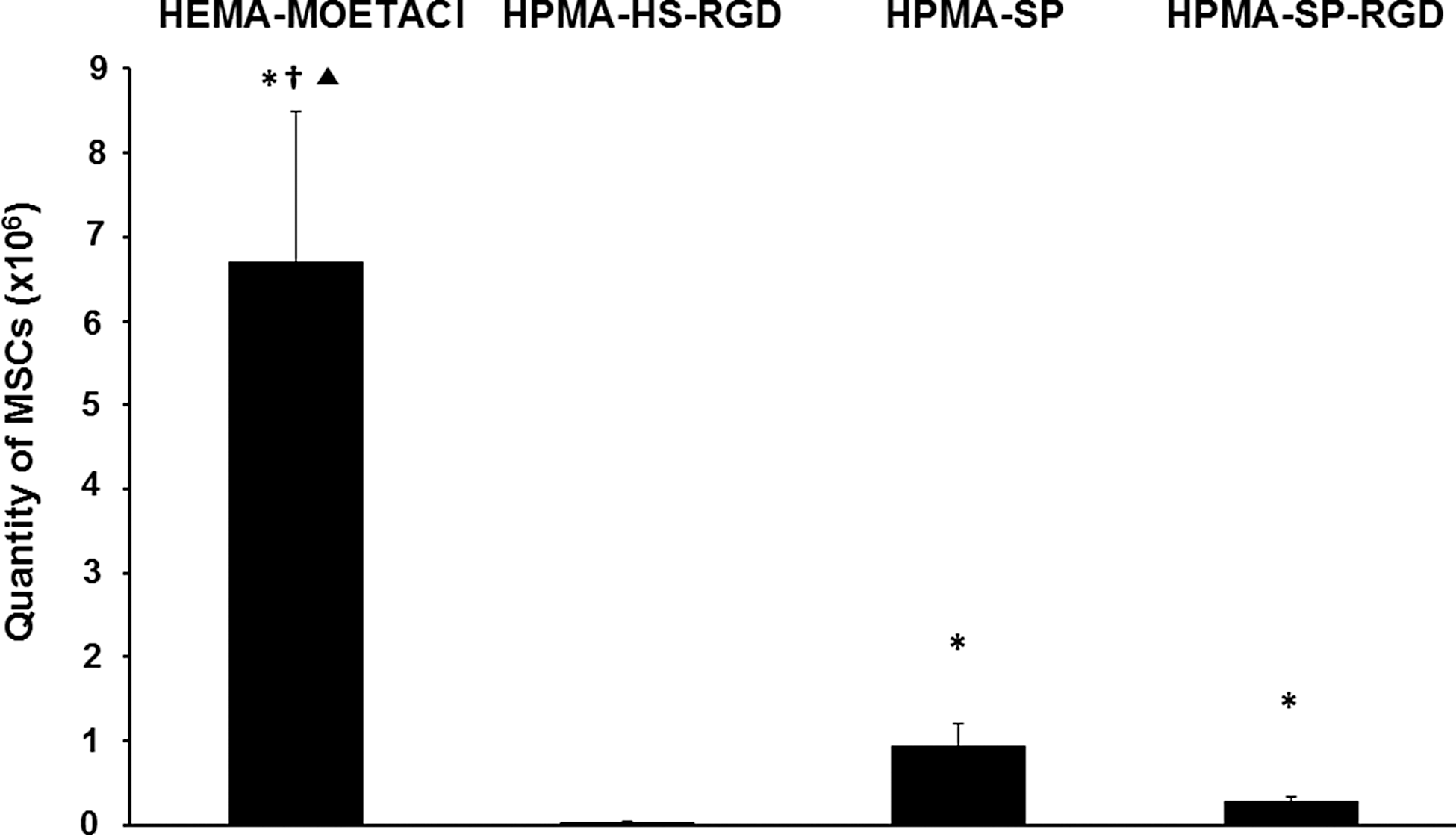
Survival of MSCs on the four modified methacrylate hydrogels on day 28 after implantation in SCI. *P<0.05 (vs. HPMA-HS-RGD), † P<0.05 (vs. HPMA-SP), ▴ P<0.05 (vs. HPMA-SP-RGD).
Axonal growth inside the hydrogels
Peripheral zone of the hydrogels
Axons infiltrated the peripheral parts of all four types of hydrogels. In our analysis, we calculated the positivity of the staining for neurofilaments divided by the area of the implant (expressed in percentage), as explained in detail in the Materials and Methods section. The same procedure was also used for calculating the blood vessels in the hydrogel scaffolds. The greatest amount of axons was found in both HPMA-SP hydrogels: HPMA-SP 4.40%±0.57% and HPMA-SP-RGD 3.90%±0.37%. In the peripheral parts of the HEMA hydrogels, the amount of axons was 3.50%±0.49%, while the fewest were found in the HPMA-HS-RGD hydrogel, 2.38%±0.49%. The only statistically significant difference was found between the number of axons in both HPMA-SP hydrogels and the HPMA-HS-RGD hydrogel (P<0.05). No other statistically significant differences were found. The summary of the data and the statistical analysis are shown in Figs. 6 and 7.
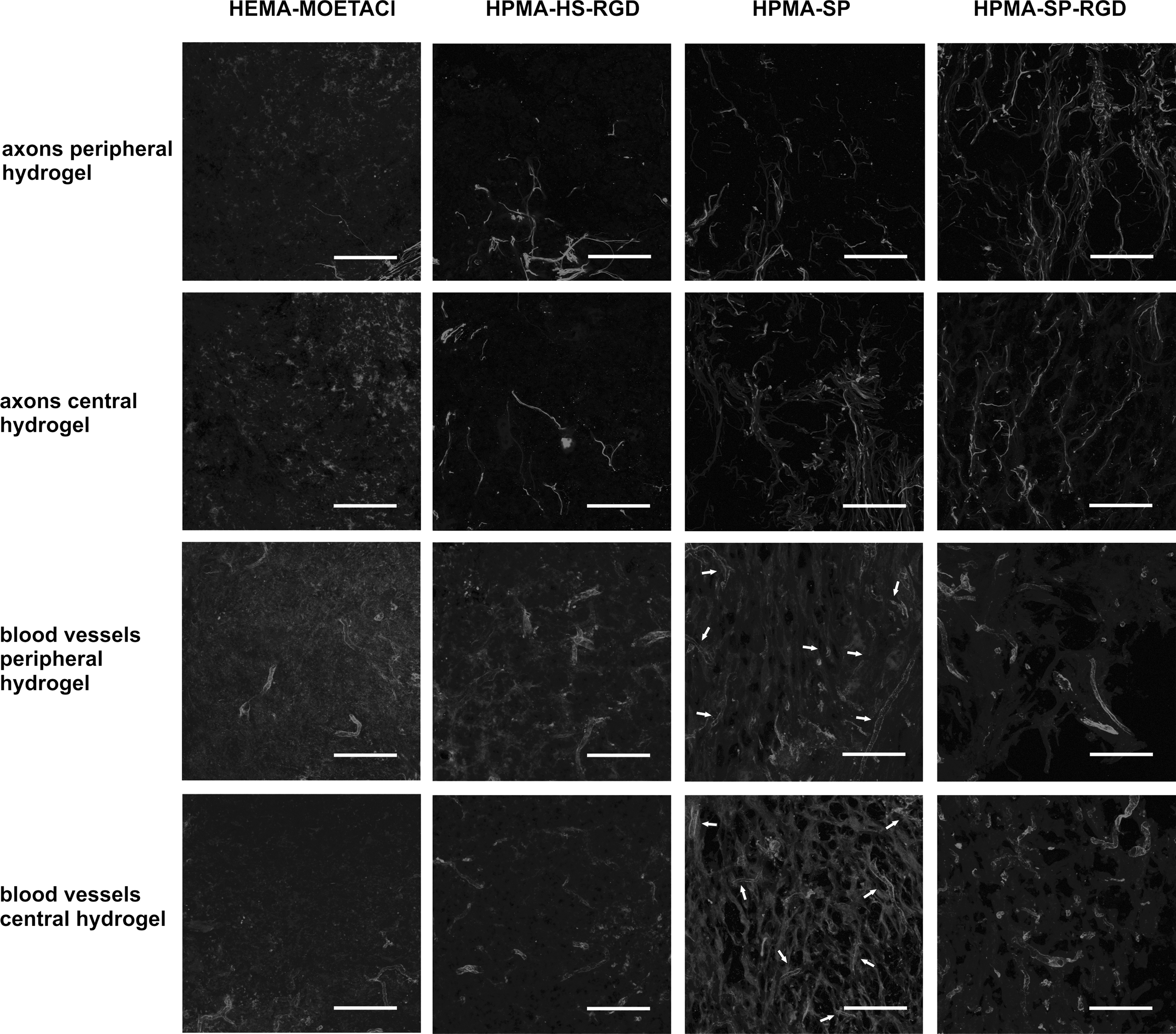
Growth of axons and blood vessels in the peripheral and central parts of the four methacrylate hydrogel scaffolds in SCI. Scale bars=100 μm. White arrows indicate new blood vessels in the HPMA-SP hydrogel to compensate for the autoimmunofluorescence of the hydrogel.
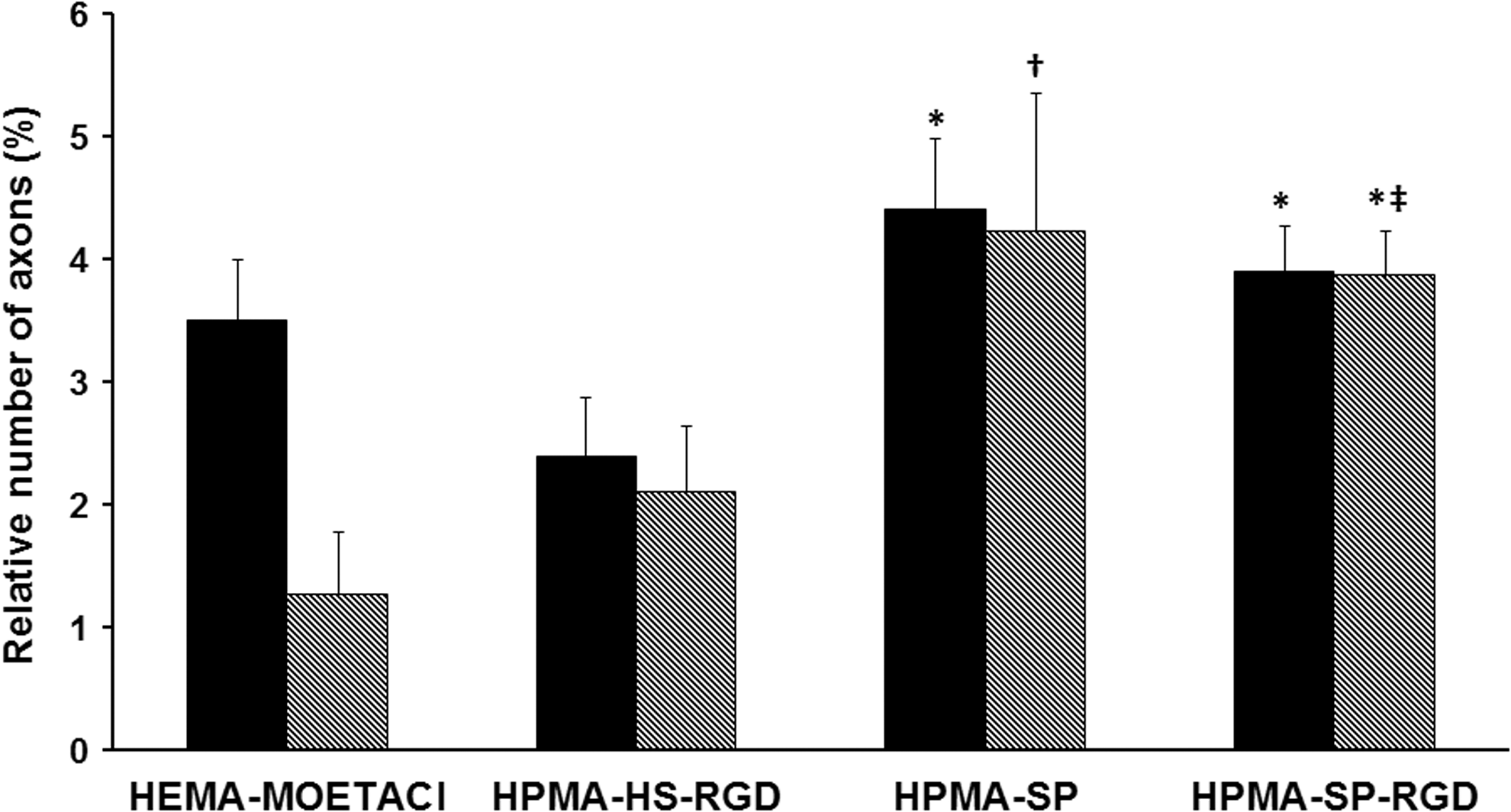
The relative number of axons in the peripheral and central parts of the four methacrylate hydrogel scaffolds in SCI. p, periphery; c, center. *P<0.05 (vs. HPMA-HS-RGD), † P<0.05 (vs. HEMA-MOETACl), ‡ P<0.01 (vs. HEMA-MOETACl).
Central zone of the hydrogels
In the central zone of the hydrogels, the relative amount of axons was similar to that in the peripheral parts in all HPMA-based hydrogels, while it decreased in the HEMA hydrogel. Further, the difference between both HPMA-SP hydrogels and the HPMA-HS-RGD or HEMA hydrogels increased in the central zones of the hydrogels. The amount of axons in the central part of the HPMA-SP hydrogel was 4.22%±1.13%, in the HPMA-SP-RGD hydrogel 3.86%±0.36%, in the HPMA-RGD-HS hydrogel 2.10%±0.55%, and in the HEMA hydrogel 1.26%±0.51%. A summary of the data and the statistical analysis are shown in Figs. 6 and 7.
Growth of blood vessels inside the hydrogels
Peripheral zone of the hydrogels
The ingrowth of blood vessels was different compared with the ingrowth of axons inside the hydrogel scaffolds. The most blood vessels were found in the HPMA-SP-RGD hydrogel, followed by the HPMA-HS-RGD hydrogel. Therefore, the most blood vessels were found in both HPMA hydrogels with attached RGD sequences (HPMA-RGD and HPMA-SP-RGD). The relative amount of blood vessels in the peripheral parts of the scaffolds was 9.04%±0.43% in the HPMA-RGD porous hydrogel, 6.04%±0.56% in the HPMA-RGD hydrogel, 2.07%±0.12% in the HPMA-SP hydrogel, and 1.85%±0.46% in the HEMA-MOETACl hydrogel. A summary of the data and the statistical analysis are shown in Figs. 6 and 8.

The relative number of blood vessels in the peripheral and central parts of the four methacrylate hydrogel scaffolds in SCI. p, periphery; c, center. *P<0.05 (vs. HPMA-SP), **P<0.01 (vs. HPMA-SP), †
P<0.05 (vs. HEMA-MOETACl), ‡
P<0.01 (vs. HEMA-MOETACl),
P<0.01 (vs. HPMA-HS-RGD).
Central zone of the hydrogels
An analogous situation to the periphery was observed in the central parts of the hydrogels, where again most blood vessels were found in the hydrogels with an attached amino sequence RGD (HPMA-SP-RGD and HPMA-HS-RGD). The relative amount of blood vessels in the central zone of the hydrogels was as follows: 10.66%±1.78% in the HPMA-SP-RGD hydrogel, 6.54%±0.90% in the HPMA-HS-RGD hydrogel, 2.06%±0.35% in the HPMA-SP hydrogel, and 1.33%±0.29% in the HEMA-MOETACl hydrogel. The summary of the data and the statistical analysis are shown in Figs. 6 and 8.
Discussion
Experimental research of the last 15 years has shown that the therapy of patients with SCI will probably require a multifaceted approach in the future. Several therapeutic modalities have been tested during this time, and some have shown at least partial improvement in experimental SCI repair [3,12,21,22].
Bridging a spinal cord lesion with a scaffold is one of the key concepts in the experimental treatment of SCI. Methacrylate-based hydrogels represent an important group of 3D bioimplants and have proved to be partially successful in SCI repair [3 –6,23 –25]. Previous studies of ours and others have shown that hydrogel implantation leads to a reduction of tissue atrophy and post-traumatic cavity formation [3,5] while providing guidance for the new growth of blood vessels, axons, and glial elements [3 –6,25,26].
The architecture of hydrogels
The physical properties of hydrogels are one of the key factors to consider when constructing a biomaterial for bridging a cavity while providing a scaffold for tissue regeneration. Several physical parameters have been analyzed in detail and evaluated in many studies, such as the stiffness of the hydrogel, quantified as the compressive modulus [23,27 –32], or the size of the pores [33], or the surface charge [4]. However, surprisingly little attention has been paid to the architecture of the hydrogel scaffold. In this study, we evaluated hydrogels with two different modifications of their architecture. The synthesis of hydrogels prepared in the presence of a SP resulted in a structure resembling a labyrinth spider web (Fig. 1A). The HPMA hydrogel prepared by HS is composed of small globular-shaped microparticles with the spaces between them serving as pores for tissue ingrowth (Fig. 1B). Both types of structure have already been evaluated in previous studies [3,6,25,34].
We compared the effect of these structural differences directly in HPMA hydrogels. We found that the labyrinth spider web-like structure of the HPMA-SP(-RGD) scaffolds promotes the growth of axons inside the scaffold. However, when we compared the HEMA hydrogel, which also has a web-like structure, and the HPMA-HS-RGD hydrogel with a structure based on microparticles, we found that there was no difference in axonal regeneration. Therefore, it is the combination of the HPMA chemistry and the labyrinth spider web-like architecture of the hydrogel that shows the best combination, leading to extensive axonal regeneration. A possible reason could lie in the interaction between the connective tissue with extracellular matrix substances and axons inside the pores of the hydrogel. Both of the HPMA-SP(-RGD) hydrogels were less invaded by connective tissue elements as compared with the HEMA and the HPMA-HS-RGD hydrogels (Fig. 4A–G). Several reports have shown the negative role of collagenous scarring and the positive effect of reducing the scar on axonal regeneration [35 –37]. Extracellular matrix proteins and connective tissue elements may play a similar role after invading the pores of the hydrogels. Their increased concentration may inhibit the ingrowth of axons by occupying the adhesion sites on the hydrogel scaffolds, reducing the overall volume available inside the pores for tissue ingrowth, or by impeding the ingrowth of axons with inhibitory molecules. However, the whole family of extracellular matrix proteins plays a more complex role in modulating the growth of axons based on their concentration, and so on. [37]. A detailed analysis of the interaction between the connective tissue elements inside the scaffolds and the axons will, therefore, be needed.
Modifying the scaffolds with adhesion molecules
An impact to the spinal cord results in immediate damage to the tissue, including blood vessels. Blood vessels are vital for tissue survival [38]. Angiogenesis is a complex process involving receptor proteins–integrins. Most of them recognize the cell-adhesive RGD peptide. The immobilization of RGD on 3D scaffolds improves their bioadhesive properties [39]. According to our study, the RGD sequence seems to be the key factor in promoting the growth of blood vessels inside the scaffold. Both hydrogels with the RGD sequence contained the highest number of blood vessels. It is important to promote the reconstruction of proper vasculature, as it supports the regrowth of axons along the blood vessels [40], and a higher density of vasculature results in significant functional recovery in SCI [41].
Hydrogel scaffolds and MSCs
We placed each hydrogel block in a suspension of MSCs on a shaker for 15 min. Since the hydrogel blocks were floating within the cell suspension, the cells were able to enter the hydrogels from all sides. The HEMA-MOETACl hydrogel contained significantly more cells than all three modifications of the HPMA-based hydrogels both in vitro and after implantation in the spinal cord lesion. When roughly comparing the number of MSCs in vitro (day 1) with the number of MSCs in vivo, it is apparent that MSCs survive in high numbers on the HEMA-MOETACl hydrogel (close to 100%) compared with all three HPMA-based hydrogels, where the survival rate is less than 50%. All of these data show that the HEMA-MOETACl hydrogel is the best carrier of MSCs in vivo as well as in vitro when evaluating these four methacrylate hydrogels.
We have already shown that a positive surface charge increases the attachment of MSCs to the scaffold [1]. As discussed in the paper cited earlier, this is probably mediated by the adsorption of serum macromolecules onto the positively charged quarternary ammonium groups. Nonetheless, when we combine the results of the study mentioned earlier and the current study, the chemical nature of the scaffold seems to be the most decisive factor in MSC attachment, as the attachment of MSCs on the four HEMA-based hydrogels with different surface charges in our previous study was affected significantly less than onto the HPMA-based scaffolds in the current study. This finding is also supported by the very high ratio of spindle-shaped MSCs on the HEMA scaffold and the fact that the number of MSCs was not statistically different between days 1 and 7 as compared with the HPMA-based hydrogels. All in all, HEMA is more attractive to MSCs compared with HPMA, despite various surface modifications.
Another factor that plays a role in MSC attachment is the structure of the hydrogel. The HPMA-SP(-RGD) hydrogels with a spider web-like structure showed the significantly increased attachment of MSCs when compared with the HPMA-HS-RGD hydrogels with microglobules. Improved attachment could also be observed from the spindle shape of some of the stem cells. In all three hydrogels with a spider web-like structure, a certain number of MSCs were spindle shaped, while no spindle-shaped MSCs were observed on the HPMA-RGD hydrogel, the structure of which is based on microglobules. Clearly, the RGD sequence is not sufficient to overcome the unfavorable globular structure of the material. Further, the RGD peptide sequence also supported the attachment of MSCs on the hydrogel scaffold. Thus, a positive surface charge, the architecture of the hydrogel, and the RGD peptide sequence have a positive impact on the attachment of MSCs on hydrogel scaffolds.
Various biomaterials have been studied with regard to the differentiation of MSCs into tissue-of-target cells. This is true especially in peripheral tissues, such as articular cartilage [42]. The goal of therapy in such cases is the replacement of damaged tissue. However, the role of MSCs in CNS repair lies not in cell replacement. A possible explanation for their positive effect could be their ability to secrete substances such as cytokines (interleukins) and trophic factors [13,43], which may facilitate regeneration, rescue partially damaged cells, or support remyelination [44], even leading to functional recovery after SCI [12,13,45,46]. Therefore, one of the functions of the scaffolds is to serve as carriers for local stem cell delivery. Such an approach could be convenient, because the local application of MSCs may be more effective compared with systemic application [17].
Our study shows that a construct comprising a hydrogel seeded with MSCs contains the highest number of cells immediately after seeding. According to our own algorithm, hydrogels are often evaluated first in vitro as carriers of stem cells [1] and only then prepared for in vivo assessment in a model of SCI. However, the ability to attract stem cells does not correlate with the ability of the hydrogel to attract neural tissue elements when implanted into a spinal cord lesion. We need to evaluate the chemical basis, the inner architecture of the hydrogel, and, possibly, any attached functional groups in relationship to the ingrowth of new tissue. When testing a new hydrogel with the intention of using it for tissue engineering in combination with stem cells, it should be tested both in vivo and in vitro independently. Only then can we obtain complete information about the new bioimplant and its potential in tissue engineering.
The role of MSCs in SCI has been well documented in several experimental studies [12,16]. They can be easily harvested and administered intravenously within a few hours in autologous transplantation protocols. The results from preclinical research led to the launching of clinical studies in patients with SCI, in which patients with either subacute or chronic SCI received MSCs intravenously or intra-arterially [14,47]. Preliminary results in patients with subacute injury, as opposed to patients with chronic SCI, have shown some promise, but no definite conclusion can be drawn yet. In patients with chronic SCI, such an approach seems to be insufficient [14]. A chronic spinal cord lesion comprises cystic cavities as well as mesenchymal and glial scarring, which together form a barrier for the growth of neural elements. A combination of a bridging scaffold with MSCs thus seems to be a more appropriate approach.
In one of our previous studies, we compared the effect of bridging a chronic lesion either with an HPMA-HS-RGD hydrogel alone or one seeded with MSCs, 5 weeks after SCI [3]. The combined approach (biomaterial+MSCs) reduced tissue atrophy and improved functional outcome of the rats 6 months after SCI. However, it is the chemical basis, the architecture of the hydrogel, and the presence of adhesion molecules on the hydrogel surface, such as the RGD peptide, that are more significant for the growth of new axons or blood vessels inside the hydrogel bridge than the presence of MSCs on the scaffold. Although there seems to be a dose-dependent effect of MSCs on the functional effect [48], it is still an unresolved question whether increasing the attachment of MSCs on the hydrogel scaffold improves functional outcome and tissue regeneration. Another important factor that is unclear is the effect of the long-term survival of MSCs on the hydrogel. In other words, how long after transplantation are the MSCs effective inside the lesion?
Hydrogels have been utilized as carriers of different types of cells, such as adult brain-derived neural stem/progenitor cells, human fetal spine-derived stem cells, and Schwann cells [49 –52]. The advantage of neural stem cells (NSCs) or Schwann cells, besides their paracrine effect, is their ability to integrate into the tissue and remyelinate spared bare axons or differentiate into more mature neurons, which can then form synapses, even inside the scaffold [53]. This could be important for reconstructing the lost tissue inside the spinal cord cavity after bridging the lesion with a scaffold. On the other hand, when implanted inside a spinal cord lesion, NSCs leave the lesion and migrate outside the scaffold as far as 4 mm into the spinal cord, which may impede their long-term regenerative potential [54]. Further, the sources of NSCs or Schwann cells are limited, which further hinders their clinical use in auto-transplantation protocols. On the other hand, MSCs can be easily harvested and prepared for auto-transplantation in individual SCI patients [14].
Factors to be considered in the light of clinical applications
Hydrogels, and biomaterials in general, are being developed in experimental SCI research with the ultimate goal to apply them in the future to treat clinical SCI. Several factors should be kept in mind when considering the “clinical feasibility” of hydrogels in SCI treatment/therapy.
In this study, we used a hemisection, a quick and easy model, which minimizes the loss of animals due to infections resulting from paralysis in models such as spinal cord transection or severe compression injury. It is, therefore, convenient for evaluating the physical and chemical modifications of newly developed and also well-established types of hydrogels in bridging a spinal cord lesion. It served our goal of looking for tissue growth across the scaffold well. Despite common use in experimental SCI, hemisection does not correspond to the majority of clinical situations, which are blunt injuries, especially compression and contusion. Further, implanting a hydrogel immediately after SCI is not realistic either. There are several experimental models resembling blunt injuries, such as an aneurysm clip model [55], a weight-drop model [56], or a balloon-induced compression lesion [57], more closely resembling the real clinical situation. The blunt types of SCI result in the formation of a syringomyelia in the chronic stage, which is the primary goal target for hydrogel bridging. It will, therefore, be necessary to prepare hydrogels that will be soft enough to adapt to the developed cavity. It would not be clinically feasible, of course, to adjust the lesion to the size of the biomaterial. On the other hand, the hydrogel cannot be too soft, as it should maintain its inner structure, including the proper size of the pores, in order to provide an adequate scaffold for tissue ingrowth. It is necessary, therefore, to test all the biomaterials in blunt-type injuries, not only in section-type lesions, that are commonly used in experimental research and which adapt to the size and shape of the implant.
The problem with adapting the shape and the size of the hydrogel to the lesion cavity could be overcome by using injectable biomaterials. They can easily adapt to the size as well as the shape of the lesion with minimal or no damage to the dura and the remaining vital spinal cord tissue, which often surrounds the central necrosis and glial scar. Both natural and synthetic materials have been applied both in vitro and in vivo. Nonetheless, most experimental SCI research has been performed on section injuries [58]. Further, in some blunt experimental lesions, the injectable material was applied intrathecally rather than inside the lesion, because the injectable hydrogels served as a delivery medium rather than as a bridging scaffold [59 –61]. However, the disadvantage of using injectable hydrogels is that it may be difficult to regulate the inner structure of the hydrogel. HPMA-SP(-RGD) hydrogels, in contrast, are very soft, easily adapt to the size and shape of the pseudocystic cavity, and can be implanted via a small incision, while their structure is well defined and preserved during implantation.
With regard to the site of injury, experimental lesions are most commonly performed at the thoracic level. This is not, however, true for clinical SCI, where cervical lesions are the most common type of injury (
In terms of timing, the acute phase of SCI is dominated by hemorrhage, edema, tissue necrosis, and the influx of immune cells—an environment that is hostile to regeneration. Such processes lead in the following weeks, among other outcomes, to the development of cavities and progressive tissue atrophy. The proper timing of scaffold implantation will be crucial. Delayed implantation will be necessary to avoid the “hostile” environment of the acute phase. A few studies have already proved this concept and have shown that delaying the “bridging” surgery leads to improved axonal regeneration, reduced tissue loss, and better adhesion when compared with acute surgery [5,62]. On the other hand, the surgery should be performed not too late in order to prevent irreversible tissue loss, muscular atrophy, and spasticity. Experimental studies have shown that implantation therapies applied as late as 5 weeks to 3 months after SCI in rats still provide a functional effect [3,25,63].
Conclusions
The fact that hydrogels are synthetic biomaterials provides the possibility of modifying the physical and chemical characteristics of the implants. Hydrogels based on HPMA synthesized in the presence of a SP significantly promote axonal regeneration across the lesion. HPMA hydrogels with an attached RGD sequence promote the ingrowth of blood vessels. Moreover, HEMA hydrogels with a positive surface charge promote the survival of MSCs both in vitro and in vivo. The HEMA-MOETACl hydrogel is the best carrier of MSCs, while the HPMA-SP-RGD hydrogel provides the best combination of properties for tissue regeneration. Its effect on functional improvement is currently being evaluated in an experimental model of blunt compression chronic SCI.
Footnotes
Acknowledgments
The authors thank Hana Hronová, Lenka Kohoutová, Alena Veselá, and Pavlína Macková for excellent technical assistance. They also thank James Dutt for a critical reading of the article. This study was supported by IAA 500390902, GAUK521712, P304/11/P633, and P108/10/1560.
Author Disclosure Statement
No competing financial interests exist.