
Abstract
In this study, we report the pharmacokinetics and in vivo fate of intra-articularly transplanted human mesenchymal stem cells (MSCs) in comparison with those of intravenously administered cells. Bone marrow-derived human clonal mesenchymal stem cells (hcMSCs) were transplanted to nude mice through intravenous or intra-articular routes. The numbers of hcMSCs in blood and tissue samples were measured by the quantitative real-time–polymerase chain reaction (qPCR) with human Alu (hAlu) as a detection marker. Following intra-articular transplantation, the blood levels of hcMSCs peaked 8 h postdose and gradually diminished, showing a 95-fold higher mean residence time than hcMSCs delivered through the intravenous route. Unlike intravenously administered hcMSCs, intra-articularly injected hcMSCs were mainly retained at injection joint sites where their levels 8 h postdose were 116-fold higher than those in muscle tissues. Regardless of injection routes, biodistribution patterns did not significantly differ between normal and osteoarthritis-induced mice. Quantitative analysis using hAlu-specific qPCR revealed that hcMSC levels in joint tissues were significantly higher than those in muscle tissues 120 days postdose. These dramatic differences in kinetic behavior and fate of intra-articularly transplanted hcMSCs compared with intravenously administered hcMSCs may provide insights useful for the development of human MSCs for arthritis therapeutics.
Introduction
S
MSCs have been administered systemically or locally for the treatment of arthritis [9 –14]. Intravenous administration of human adipose tissue-derived MSCs was shown to prevent and suppress arthritis in collagenase-induced arthritis in mice [9]. Infusion of MSCs before the onset of adjuvant-induced arthritis in rats was shown to ameliorate subsequent symptoms [10]. Both intraperitoneal and intra-articular transplantation of murine MSCs were shown to suppress proteoglycan-induced arthritis in mice [11]. Direct injection of monkey MSCs into an injured cartilage site was reported to exert a healing effect on the cartilage lesion in a cynomolgus monkey arthritis model [12]. Intra-articular transplantation of bone marrow-derived MSCs into the joints of goats with experimentally induced defects was shown to improve cartilage regeneration compared with single bone marrow stimulation [13]. A pilot study of intra-articular transplantation of autologous bone marrow-derived MSCs demonstrated clinical efficacy and safety in patients with chronic knee osteoarthritis [14].
Despite the potential of MSCs as a regeneration medicine in arthritis, our current understanding of the in vivo fates of intra-articularly transplanted MSCs compared with those of intravenously administered MSCs is limited. A few groups have reported the joint retention and biodistribution of MSCs after intra-articular transplantation [15,16]. Iron oxide-labeled adipose tissue-derived MSCs were reported to exhibit preferential migration to the thymus and gastrointestinal tract at 4 weeks after intra-articular administration to dogs [15]. Fluorescent dye-labeled, adipose tissue-derived MSCs were detected for 20 days in knee joints of rabbits after intra-articular transplantation [16]. However, both studies were based on the qualitative detection of MSCs using artificially modified MSCs, which may possess altered properties. Moreover, there is lack of knowledge about differences in the in vivo fates of intra-articularly transplanted MSCs from those of intravenously administered MSCs. Thus, it is important to quantitatively compare the pharmacokinetics and in vivo trafficking of intact MSCs transplanted through these two different routes.
In this study, we thus tested the pharmacokinetics and in vivo trafficking of intra-articularly transplanted MSCs in comparison with those of intravenously administered stem cells. Quantitative real-time–polymerase chain reaction (qPCR) was employed for the sensitive quantitative detection of intact MSCs. As MSCs, we used bone marrow-derived human clonal MSCs (hcMSCs) isolated with a subfractionation culturing method [17]. In this study, using this quantitative approach, we report the substantially prolonged mean residence time and persistence of intra-articularly transplanted hcMSCs in joint tissues.
Materials and Methods
Isolation, culture, and characterization of hcMSCs
HcMSCs were isolated and cultured using a subfractionation culturing method, as described [17], and characterized with respect to cell surface marker expression, differentiation potential, and in vitro immunosuppressive activity. Cell surface marker expression was examined by flow cytometry using specific antibodies against CD14, CD34, CD44, CD45, CD73, CD90, CD105, CD119, CD146, HLA-I, HLA-DR, and PODXL, and isotype control antibodies; all antibodies were purchased from BD Pharmingen (San Diego, CA). For selection of hcMSCs, three mesenchymal cell clones were independently induced and assessed by cell type-specific cytostaining. Adipogenic, osteogenic, and chondrogenic differentiation was assessed as described [17]. Among several hcMSC candidate clones, the hcMSCs that showed full differentiation potentials (Fig. 1A–C) were selected for further studies. Other clones, which showed partial differentiation potentials (Supplementary Fig. S1; Supplementary Data are available online at
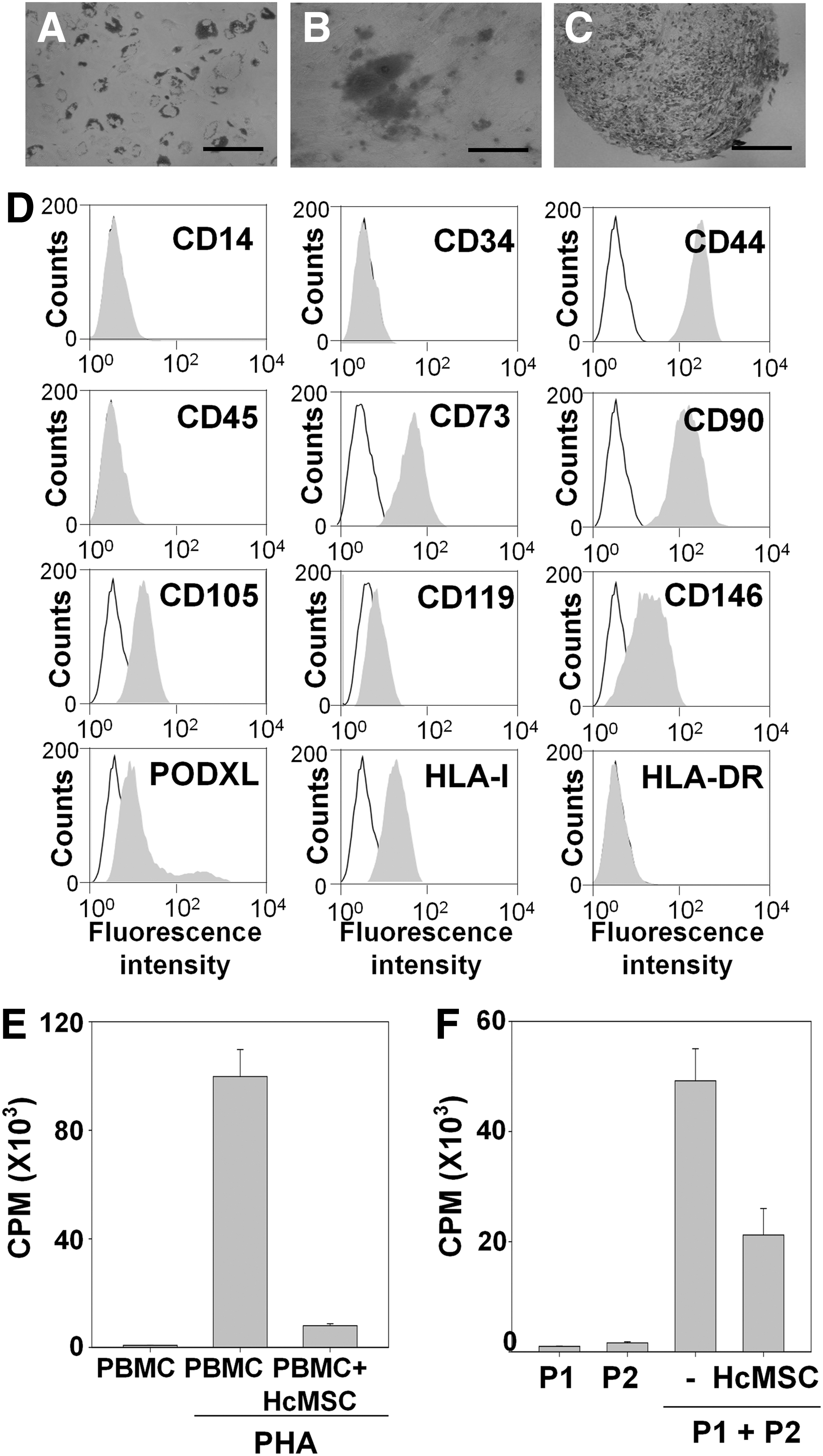
Characterization of human clonal mesenchymal stem cells (hcMSCs). The multilineage differentiation potential of hcMSCs was evaluated by cell type-specific cytostaining using Oil Red O
In vivo transplantation of hcMSCs
All in vivo experiments were performed using 6-week-old female Balb/c or Balb/c athymic nude mice supplied by Orient Bio, Inc. (Seungnam, Kyonggi-Do, Republic of Korea). Animals were raised under standard pathogen-free conditions at the animal center for pharmaceutical research in Seoul National University. All animal experiments were conducted in accordance with the Guidelines for the Care and Use of Laboratory Animals of the Institute of Laboratory Animal Resources, Seoul National University, and were approved by our institution's Animal Care and Use Committee (experimental protocol number SNU-130129-3-1). Mice were injected with 5×105 hcMSCs through the tail vein for intravenous injection or in joint sites for intra-articular injection.
Induction of osteoarthritis in mice
Osteoarthritis was induced with monosodium iodoacetate (MIA; Sigma-Aldrich), as previously described [19]. Balb/c mice were intra-articularly injected with 5 μL of MIA (10 mg/mL) dissolved in phosphate-buffered saline (PBS, 50 mM, pH 7.4) into the right knee. Transplantation of hcMSCs was conducted 2 weeks after MIA treatment.
Extraction of genomic DNA from blood, tissues, and joint sites
For pharmacokinetic studies, blood samples were obtained from the tail vein at various time points after administration of hcMSCs using capillary tubes. For biodistribution studies, mice were sacrificed by CO2 inhalation at various times after injection of hcMSCs, and the spleen, kidney, liver, lymph nodes, muscle, lung, heart, and brain were excised and collected. In the case of joint site samples, a region around the cartilage with a radius of 50 mm was dissected after removing muscles. Genomic DNA (gDNA) was extracted and purified using a DNeasy Tissue Kit (Qiagen, Hilden, Germany) as described by the manufacturer.
qPCR assay of hAlu
A human Alu (hAlu) element in hcMSC gDNA was detected by amplifying 20 ng of gDNA template by qPCR using LightCycler FastStart DNA Master CYBR Green I (Roche Diagnostics Gmbh, Mannheim, Germany). Primers were 5′-GCCTGTAATCCCAGCACTTT-3′ for sense, and 5′-CACTACGCCCGGCTAATTT-3′ for antisense. The amplification conditions were as follows: 94°C for 10 min (initial denaturation), followed by 45 cycles of 20 s at 94°C (denaturation), 20 s at 58°C (annealing), and 20 s at 72°C (extension). The size of the qPCR product was 127 base pairs.
Pharmacokinetic data analysis
Noncompartmental pharmacokinetic parameters were calculated using WinNonlin software (Scientific Consulting, Inc., Lexington, KY). The mean residence time was calculated by dividing the area under the momentum curve by the area under the curve (AUC).
In vivo imaging with fluorescent marker-labeled hcMSCs
HcMSCs in vivo were visualized by staining the membranes of hcMSCs with a fluorescent dye using a PKH67 green fluorescent cell linker kit (Sigma-Aldrich), according to the manufacturer's protocol. Briefly, hcMSCs (5×105 cells) were washed with a serum-free medium and centrifuged for 5 min at 400 g. After discarding the supernatant, cell pellets were suspended in 1 mL of diluent C of the kit and stained with 1 mL of PKH67 solution (4 μM) for 5 min at room temperature in the dark. The staining process was stopped by adding an equal volume of serum to the mixture. The solution was centrifuged at 400 g for 10 min and washed twice with the complete medium. After collecting by centrifugation and suspending in 50 μL of PBS, PKH67-labeled hcMSCs were intra-articularly injected into mice. Retention of hcMSCs at injected joint sites was observed using a molecular imaging system. At various time points, the in vivo distribution of fluorescent hcMSCs was determined using an eXplore Optix system (Advanced Research Technologies, Inc., Montreal, Canada). The excitation and emission spots were raster scanned in 2.5-mm steps over the region of interest to generate emission wavelength scans.
Statistics
An analysis of variance (ANOVA) with a post hoc Student–Newman–Keuls test was used for statistical evaluation of experimental data. All statistical analyses were done using SigmaStat software (version 3.5; Systat Software, Richmond, CA); a P-value <0.05 was considered significant.
Results
Characterization of hcMSCs
HcMSCs were identified on the basis of stem cell markers, differentiation potentials, and immunosuppressive activity (Fig. 1). The adipogenic, osteogenic, and chondrogenic differentiation potentials of hcMSCs were verified by Oil Red O (Fig. 1A), Alizarin Red S (Fig. 1B), and Safranin O (Fig. 1C) staining, respectively, after treating with differentiation-stimulating factors. A flow cytometry analysis revealed that the cells were positive for MSC markers (CD44, CD73, CD90, CD105, CD119, CD146, PODXL, and HLA-I), but negative for hematopoietic/endothelial markers (CD14, CD34, CD45, and HLA-DR) (Fig. 1D). The [3H]-thymidine incorporation study revealed that hcMSCs possessed in vitro immunosuppressive activity in the PHA-stimulated condition (Fig. 1E) and mixed lymphocyte condition (Fig. 1F).
Quantification and pharmacokinetics of intra-articularly transplanted hcMSCs
Using human-specific hAlu as a detection marker, we quantified hcMSC numbers in samples by reference to a standard curve of hAlu cycle threshold (Ct) value in qPCR assays generated using known numbers of hcMSCs. An effective primer pair for qPCR of hAlu was selected based on the range of detection and Ct value. The primer set used in this study showed a wide range of detection (101–105 pg of template). The Ct values obtained using the hAlu primer set were well correlated and linearly related to the number of hcMSCs (Supplementary Fig. S2).
Pharmacokinetic profiles of intra-articularly transplanted hcMSCs substantially differed from those of intravenously administered cells (Fig. 2). Three minutes after intravenous administration of hcMSCs into mice, the concentration of hcMSCs in blood was 2,693±646 cells/mL and rapidly declined thereafter (Fig. 2A). One hour postdose, the blood concentration of hcMSCs was 87±52 cells/mL. Unlike intravenously administered hcMSCs, intra-articularly transplanted cells exhibited a peak concentration in blood of 408±71 cells/mL at 8 h, and then gradually decreased (Fig. 2B). The AUC of hcMSCs after intra-articular administration was 15,549±2,367 cells·h/mL, a value 15.4-fold higher than that after intravenous administration (1,008±287 cells·h/mL). The mean residence time of intra-articularly administered hcMSCs was 35.3±5.4 h or 95.0-fold longer than that of intravenously administered hcMSCs (0.4±0.1 h).
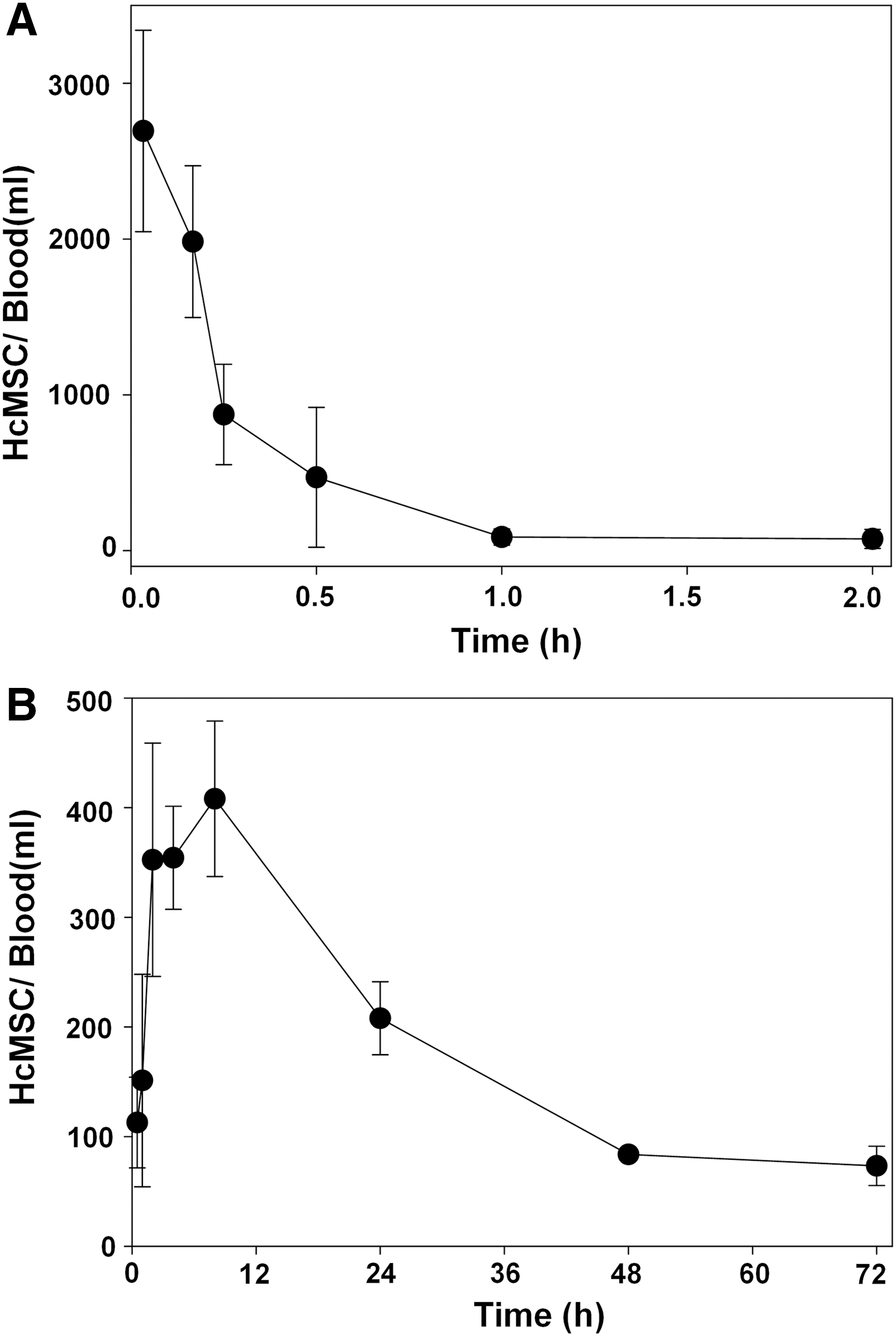
Blood concentration-time profiles of intravenously or intra-articularly transplanted hcMSCs. Mice were intravenously
Biodistribution of hcMSCs in normal and osteoarthritis-induced mice models
Regardless of injection routes, biodistribution of hcMSCs did not differ significantly from that of conventional hMSCs, in both normal and MIA-treated osteoarthritis animal models. In normal mice, intravenously (Fig. 3A) or intra-articularly (Fig. 3B) transplanted hcMSCs and hMSCs showed comparable levels of distribution to the lung and joint tissues, respectively. Compared with normal mice, MIA-treated mice showed little differences in distribution patterns following intravenous (Fig. 3A) and intra-articular (Fig. 3B) injection with hcMSCs. Moreover, hcMSC clones, which differed in their differentiation potentials, did not show significant differences in biodistribution patterns following intravenous (Supplementary Fig. S3A) and intra-articular (Supplementary Fig. S3B) injections in normal mice.

Biodistribution of hcMSCs in normal and osteoarthritis-induced mice. Normal or monosodium iodoacetate (MIA)-treated mice were intravenously
In vivo trafficking of intra-articularly transplanted hcMSCs
Compared with intravenously administered hcMSCs, intra-articularly transplanted hcMSCs showed in vivo trafficking patterns highly localized to the joint tissue (Fig. 4). At 15 min postdose, intravenously administered hcMSCs showed a greater distribution to lung tissue than other organs, including the spleen, kidney, liver, muscle, heart, brain, and lymph nodes (Fig. 4A). At 30 and 60 min after intravenous administration, the distribution patterns of hcMSCs were similar to those at 15 min postdose. At 60 min postdose, the levels of hcMSCs in the lung tissue were at least 14-fold higher than those in other tissues. Following intra-articular transplantation, hcMSCs were mainly distributed to the joint tissue (ie, the injection site). Eight hours after intra-articular injection, the levels of hcMSCs in the injected joint tissue were higher than those in other tissues and were 116-fold higher than those in muscle tissue (Fig. 4B). The levels of hcMSCs in joint tissue decreased over time from 299±43 hcMSCs per 100 ng of gDNA at 8 h to 73±12 hcMSCs per 100 ng gDNA at 72 h, at which point the levels of hcMSCs were 99-fold higher than those in muscle tissue.
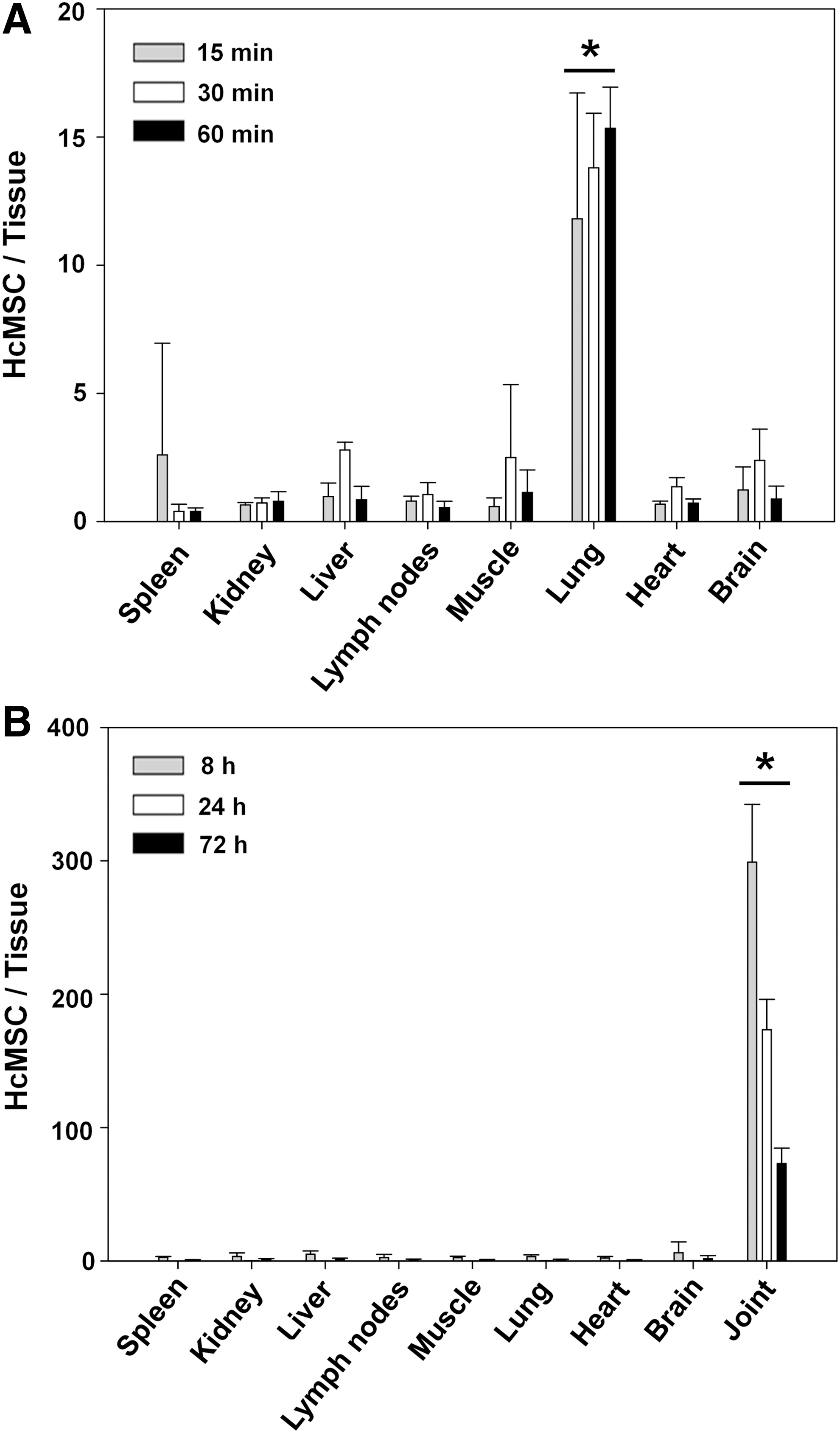
Biodistribution of hcMSCs following intravenous or intra-articular transplantation. Mice were intravenously
Retention of hcMSCs at joint tissue
Although intravenously administered hcMSCs showed clearance at the lung in less than a few days, intra-articularly transplanted hcMSCs retained at the joint tissues for more than 100 days. The retention time of hcMSCs in the major site of distribution differed depending on the injection route. Following intravenous injection, the retention of hcMSCs in the lung was evaluated over 48 h. At 6 and 48 h, the levels of hcMSCs decreased to 12% and 1.2%, respectively, of those at 1 h (Fig. 5). In contrast to intravenously administered hcMSCs, intra-articularly administered hcMSCs showed a more prolonged retention in joint tissue. Thus, their retention was evaluated over a much longer time frame (120 days). At 14 days after injection, the levels of hcMSCs in joint tissue were more than two orders of magnitude greater than those in muscle tissue (Fig. 6A) and remained significantly higher at 120 days. The prolonged retention of hcMSCs in joint tissues was further examined by monitoring fluorescent PKH67-stained hcMSCs. At 14 days, PKH67-stained hcMSC fluorescence intensity above background levels was detected only in joint tissue (Fig. 6B). Compared with values obtained 30 min after intra-articular injection, photon counts in joint tissue were 4.2-fold lower on day 14 and 32.9-fold lower on day 21 (Fig. 6C).
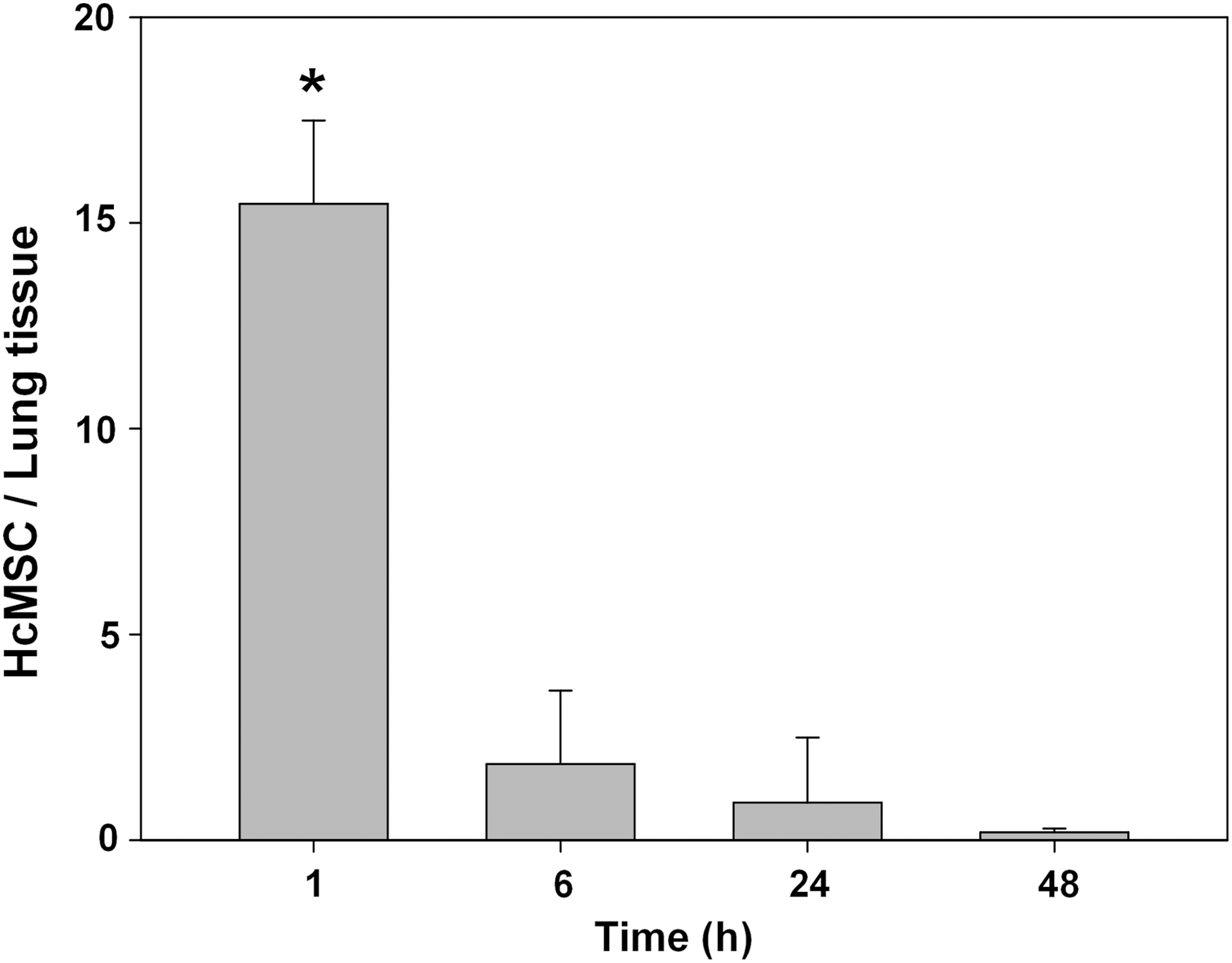
Retention of intravenously administered hcMSCs in the lung. Mice were intravenously injected with hcMSCs (5×105 cells). Lung tissues were collected at various time points after a single injection, and the number of hcMSCs was quantified by qPCR of hAlu in 100 ng of extracted gDNA. Results are expressed as mean±SD (*P<0.05 compared with other groups, ANOVA, and Student–Newman–Keuls test; n=5).

Retention of intra-articularly transplanted hcMSCs in joint tissues. Mice were intra-articularly injected with hcMSCs (5×105 cells).
Discussion
In this study, we present a quantitative analysis of the pharmacokinetics and in vivo trafficking of intra-articularly transplanted hcMSCs in comparison with those of intravenously administered hcMSCs. A pharmacokinetic analysis of blood concentration profiles of hcMSCs demonstrated that mean residence time values for intra-articularly transplanted hcMSCs were longer than those for intravenously administered hcMSCs. With respect to biodistribution, intra-articularly transplanted hcMSCs were retained in injected joint tissues and detectable for 120 days. This contrasts with intravenously administered hcMSCs, which were mainly distributed to the lung and were rapidly cleared within 2 days.
In the current study, hcMSC lines were established by the subfractionation culturing method, a new isolation procedure [17]. MSCs can be isolated from adult tissues and expanded in culture for several generations [2]. With existing gradient centrifugation methods, it is often difficult to identify diverse stem or progenitor cells in isolated cell populations, and a variety of clinical trials have proceeded using mixed cell populations. Nonhomogeneous MSCs from different separation methods exhibited different results in clinical trials [20]. It has been reported that the existence of clones with different characteristics or subpopulations resulted in heterogeneity of obtained MSC pools [21]. Indeed, we observed that the cells of different clones showed unidentical differentiation potentials (Fig. 1 and Supplementary Fig. S1). Unlike the conventional gradient centrifugation method, the subfractionation culture method is known to allow the more homogenous clonal expansion of MSCs [17]. The therapeutic benefit of using hcMSCs over MSCs isolated using the gradient centrifugation method has been reported for graft-versus-host disease [18] and hair regeneration [22]. In addition, the isolation method of hcMSCs requires only a small amount of bone marrow aspirate and thus reduces extraction time, cost, and donor pain. Several studies have reported the anti-inflammatory [23], immunosuppressive [24], and wound-healing effects [25] of hcMSCs. Such a diverse pharmacological profile may make it possible to apply hcMSCs for arthritis treatment.
For quantitative pharmacokinetic analyses and biodistribution studies of hcMSCs in mice, we selected hAlu as a human cell-specific endogenous biomarker. The Alu family is a highly repetitive and abundant element in the human genome [26]. Previously, radiolabeling or reporter gene-transduction methods have been used to track the in vivo fates of stem cells. Radiolabeling of the surface of human fetal liver stem/progenitor cells [27] and human MSCs [28] with technetium-99 has been used in biodistribution studies. Murine MSCs transduced with a luciferase reporter gene using a simian immunodeficiency lentiviral vector [29] or retroviral vectors [11] have been employed for assessing in vivo trafficking of injected cells. The fates of bone marrow-derived stem cells, transduced with a thymidine kinase reporter gene using an adenoviral vector, have been traced following injection by measuring reporter gene levels [30]. Human neural stem cells transduced with the adenoviral E1A transcriptional regulatory region have been used for pharmacokinetic analyses [31]. However, radiolabeling or viral transduction of stem cells may alter the natural properties of the cells, which may affect their in vivo fates. Emission of radiation may also impair stem cell proliferation and survival [2]. Moreover, viral vector-mediated transduction of stem cells can raise concerns about associated immunogenicity and insertional mutagenesis [32]. By using an endogenous hsMSC-specific biomarker, it is possible to eliminate the extra processing of stem cells and the consequent concerns about potential alterations of stem cell properties.
We observed that intravenously administered hcMSCs were mainly distributed to the lung and did not relocate to other organs (Fig. 4A). This pulmonary first effect of intravenously administered rodent stem cells has been reported by other groups [33,34], who showed that intravenously injected murine MSCs were distributed to the lung at 5 min postdose in mice [33], and intravenous bolus administration of rat mesenchymal stromal cells resulted in a lung-oriented distribution immediately after injection into Sprague-Dawley rats [34]. One explanation for this distribution pattern is the larger size of these cells (∼15–19 μm), as evidenced by the fact that smaller murine bone marrow-derived mononuclear cells (7 μm) distribute to the lung to a lesser extent than MSCs. In addition to cell size, over-expression of vascular cell adhesion molecule 1 on the surface of MSCs is known to lead to pulmonary accumulation [34].
After the initial distribution to the lung, intravenously administered hcMSCs were rapidly cleared, almost completely disappearing from the lung at 48 h postdose (Fig. 5). Consistent with this, a recent study reported rapid clearance of human MSCs from the lung in rats [28]. Using whole-body nuclear imaging, these authors found that the levels of human MSCs in the lung at 18–20 h postdose were more than an order of magnitude lower than those at 0–2 h postdose. They further reported that MSCs showed no significant redistribution from the lung to other tissues at 20 h postdose.
Unlike intravenously administered hcMSCs, intra-articularly administered hcMSCs survived in the injected joint tissues for a more prolonged period, remaining at detectable levels over 120 days postdose. Following intra-articular injection in dogs, canine adipose tissue-derived MSCs were shown to reside near the injection sites for at least 2 weeks [15]. After intra-articular administration in rabbits, rabbit adipose tissue-derived stromal cells were detected in knee joint injection sites on days 3 and 20 [16]. While we were conducting the current study, distribution of human adipose tissue-derived stem cells was reported after intra-articular administration [35]. However, in this latter study, the quantitative pharmacokinetic comparative analysis and the short-term trafficking of intra-articularly transplanted MSCs relative to the intravenously administered stem cells were not investigated. Moreover, we used a homogenous population of hcMSCs rather than conventionally isolated human adipose tissue-derived stem cells.
Although the mechanisms by which intra-articularly injected hcMSCs persist in joint tissue will require further study, several possibilities suggest themselves. One is that joint tissues may provide a favorable microenvironment for the survival and proliferation of hcMSCs. In this context, a recent study reported that the mouse knee joint synovium could serve as a niche for MSCs and facilitates their proliferation and differentiation following injury [36]. Another possibility is the immune-privileged status of joint tissues. It has been suggested that synovial joints are immune privileged owing to their poor vascularization, dense extracellular matrix, and separation from other tissues by a physical capsule [37]. Moreover, as shown by our characterization of hcMSCs (Fig. 1E) and that by others [3,4], the immunosuppressive property of MSCs per se may contribute to their prolonged survival in joint tissues.
A direct comparison of PKH67-stained cell imaging and hAlu-specific qRT-PCR-based retention studies of hcMSCs in joint tissue (Fig. 6) supports the higher sensitivity of the qPCR method compared with the fluorescent molecular imaging approach. The photon counts of PKH67-stained hcMSCs decreased to background levels at day 21 after injection, whereas hcMSCs were detectable up to 120 days after injection by qPCR. This observation implies that qPCR is more suitable for studying the long-term in vivo distribution of stem cells.
In conclusion, the pharmacokinetics and in vivo trafficking of intra-articularly transplanted hcMSCs were substantially different from those of intravenously administered hcMSCs in mice. Intra-articularly transplanted hcMSCs exhibited a peak blood concentration at 8 h postdose and a mean residence time almost two orders of magnitude longer than intravenously administered hcMSCs. Unlike intravenously administered hcMSCs, which were mainly distributed to the lung and rapidly cleared within 2 days, intra-articularly administered hcMSCs were retained in injected joint tissues and persisted for up to 4 months. Moreover, there were no significant differences in biodistribution patterns among normal and MIA-treated osteoarthritis mice models. These observations may provide a framework for the transplantation study of stem cells for arthritis treatment.
Footnotes
Acknowledgments
This work was supported by research grants from the Ministry of Science, ICT and Future Planning (NRF-2012R1A2A1A01007005) and the Korean Health Technology R&D Project (A092010), Ministry for Health and Welfare.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.