
Abstract
Although regenerative endodontic procedures have yielded an impressive body of favorable outcomes, the treatment of necrotic immature permanent teeth in particular remains to be a challenge. Recent advances in dental stem cell (DSC) research have gained increasing insight in their regenerative potential and prospective use in the formation of viable dental tissues. Numerous studies have already reported successful dental pulp regeneration following application of dental pulp stem cells, stem cells from the apical papilla, or dental follicle precursor cells in different in vivo models. Next to responsive cells, dental tissue engineering also requires the support of an appropriate scaffold material, ranging from naturally occurring polymers to treated dentin matrix components. However, the routine use and banking of DSCs still holds some major challenges, such as culture-associated differences, patient-related variability, and the effects of culture medium additives. Only in-depth evaluation of these problems and the implementation of standardized models and protocols will effectively lead to better alternatives for patients who no longer benefit from current treatment protocols.
Introduction
O
The isolation and extensive characterization of dental stem cells (DSCs) have raised the hope for a new era of dental pulp regeneration, namely an era of stem cell-based dental tissue engineering. This review not only aims to summarize the current clinical practice in regenerative endodontics but also offers an overview of the progress in DSC-based approaches for dental pulp tissue engineering and its challenges. Next to an elaborate description of the currently used scaffold materials, this article will also address the present caveats in regenerative dentistry, in particular the importance of standardization and information for clinicians as well as patients.
Regenerative Endodontic Procedures
As any factor, which interferes with normal pulp physiology, may conflict with the completion of root development, the endodontic treatment of immature teeth, in particular, holds some major challenges [3,4]. The viability of Hertwig's epithelial root sheath is a key factor as arrested root development following pulp necrosis may lead to weakening of the root structure, thereby increasing the tooth's susceptibility to fractures and consequently reducing its survival rate [4 –7]. In 2008, Huang already mentioned a paradigm shift in the endodontic treatment of necrotic immature permanent teeth; to allow continued root development, necrotic immature permanent teeth should be treated as minimally invasive as practically possible [4].
The concept of revascularization was first described by Nygaard Östby in 1961, indicating sustained root development following blood clot induction in the root canal of immature teeth suffering from pulp necrosis [8]. Following numerous adaptations, this REP was recently described by the American Association of Endodontists (Fig. 1) [9]. The treatment protocol encompasses the disinfection of the root canal by means of sodium hypochlorite and triple antibiotic paste (first appointment, Fig. 1A), followed by irrigation with ethylenediaminetetraacetic acid (EDTA) and triggering the apical tissue with a hand file. Finally, the resulting blood clot is sealed with a biocompatible material and the access cavity is restored (second appointment, Fig. 1B) [10].
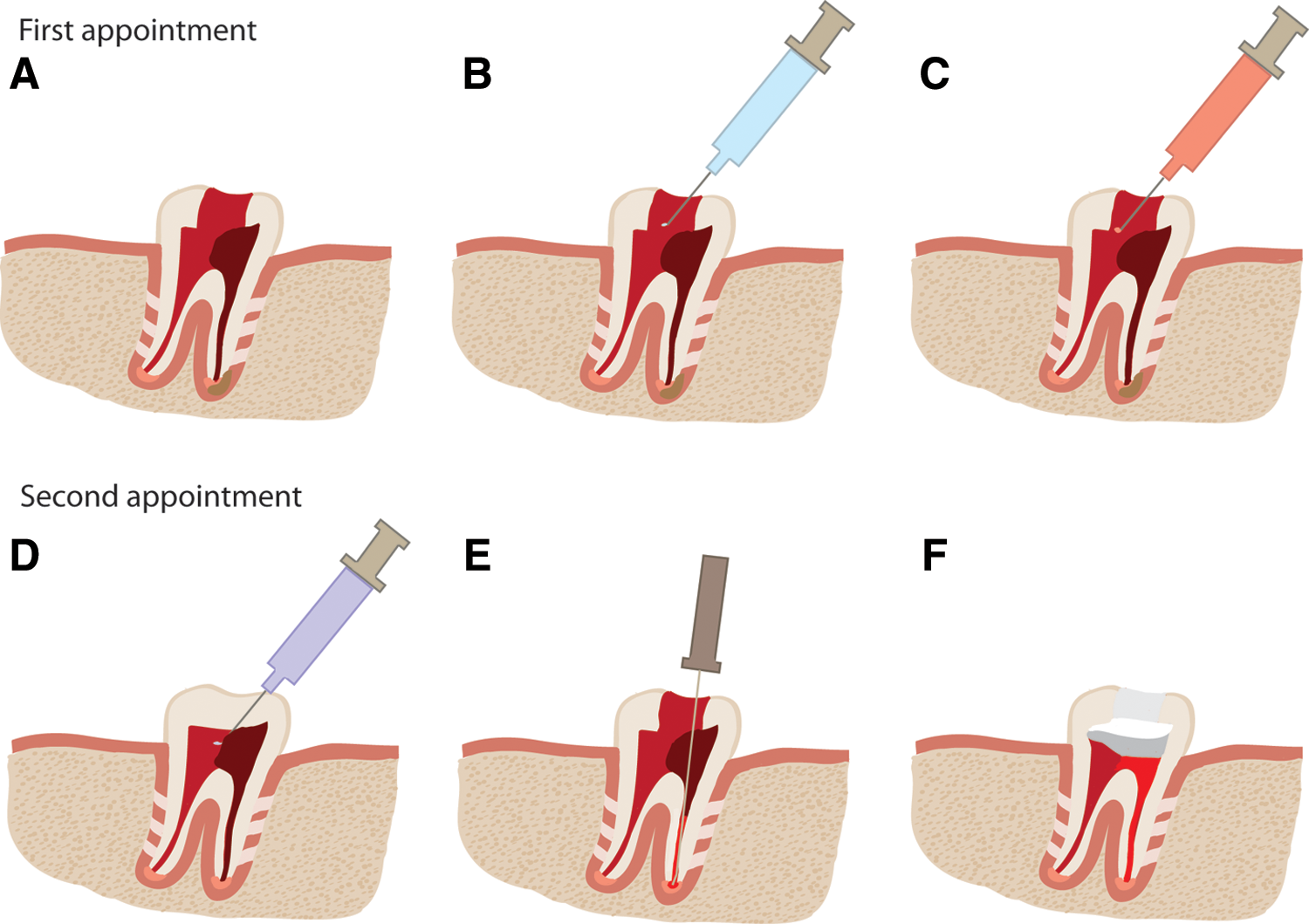
Regenerative endodontic procedure.
The induction of a blood clot not only causes the release of growth factors but presumably also serves as a scaffold for stem cells from the apical papilla (SCAPs), which survived the disinfection protocol [3,11,12]. Studies also mentioned the release of proangiogenic dentin matrix components following irrigation with EDTA, all together leading to an optimally conductive environment for dental pulp healing and regeneration [13 –15]. Another cell homing-based approach has also been recently described in several case studies, namely the application of platelet-rich plasma (PRP) or platelet-rich fibrin (PRF) as a scaffold to potentially attract residing stem cell populations and promote tissue restoration [16 –22]. However, as already mentioned by Diogenes and colleagues, definitive conclusions regarding the reported favorable outcomes and their predictability cannot be drawn at this point due to the different disease etiologies and the lack of standardized treatment protocols in numerous clinical case reports [3,7,10].
An additional drawback of the currently used cell homing-based techniques is the fact that the exact nature of the regenerated tissue in the pulp cavity is difficult to determine [23]. Due to its reliance on cell homing, regeneration by triggering the periapical tissue with a hand file and/or application of PRP can cause the invasion of different cell populations into the pulp cavity leading to ingrowth of periodontal tissue and deposition of cementum and bone [21 –26]. Next to a lack of information regarding the so-called critical size defect for dentin as well as pulp tissue, that is, a defect which is not able to regenerate naturally without any support, another often recurring concern in regenerative endodontics and revascularization/cell homing-based procedures in particular, is the size of the apex, which is required for adequate pulp revascularization, as vascular supply within the tooth is restricted by the apical foramen [23,27].
Several studies suggest a higher rate of dental pulp healing and revascularization with apical sizes ranging from 1.1 to 1.5 mm [23,28,29]. In terms of cell-based approaches, however, recent studies of Iohara et al. indicated regeneration of vascularized pulp tissue in mature dog teeth with an apical opening of 0.7 mm after transplantation of a subpopulation of dental pulp stem cells (DPSCs) [30,31]. Furthermore, this research group also reported a more pronounced volume of regenerated dental pulp tissue with a higher capillary density after transplantation of DPSCs in comparison with a cell homing-based approach with granulocyte colony-stimulating factor (G-CSF) and basic fibroblast growth factor [32]. These data are in accordance with recent work from our group, indicating a proangiogenic impact of DSCs in vitro and in vivo [33]. Taken together, these studies suggest the application of DSCs as a potential tool in regenerative endodontic approaches. The following sections offer a comprehensive overview of the current literature on the use of DSCs in dental tissue engineering.
Dental Stem Cells
Within the human tooth and its environment, several stem cell populations can be distinguished, such as DPSCs, SCAPs, dental follicle precursor cells (FSCs), and periodontal ligament stem cells (PDLSCs) (Fig. 2) [34 –37]. In general, DSCs can be characterized as mesenchymal stem cells (MSCs) according to the minimal criteria defined by the International Society for Cellular Therapy, that is, they are plastic adherent; they express markers, such as CD73, CD90, and CD105; they are negative for markers, such as CD14, CD34, and CD45; and they are capable of in vitro differentiation into adipogenic, osteogenic, and chondrogenic lineages [38 –42].
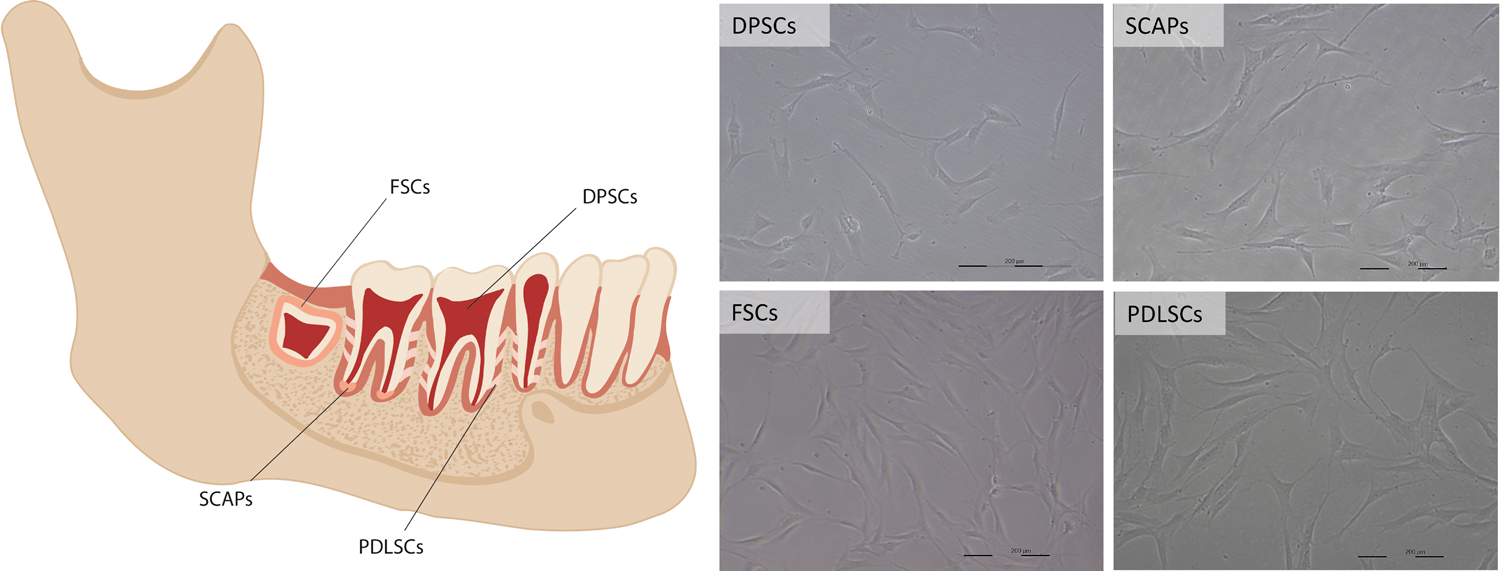
The location of dental stem cells in the oral environment. DPSCs, dental pulp stem cells; SCAPs, stem cells from the apical papilla; FSCs, dental follicle precursor cells; PDLSCs, periodontal ligament stem cells. Scale bar: 200 μm. Color images available online at
The origin of DSCs has recently been a subject of considerable debate. Up until now, it was assumed that given the reciprocal interactions between embryonic oral epithelium and neural crest-derived mesenchyme during tooth morphogenesis, DSCs are derived from the neural crest. However, a study of Kaukua et al. recently demonstrated the glial origin of a significant subpopulation of DPSCs, suggesting that depending on the tissue of origin, each DSC population is defined by its own ability to repair and/or regenerate diseased or damaged dental tissues [43]. With regard to dental pulp regeneration in particular, DPSCs, SCAPs, and FSCs have successfully been applied in a number of animal models.
Dental pulp stem cells
In 1996, Mooney et al. were the first to describe the in vitro formation of pulp-like tissue after culturing human pulp-derived fibroblasts onto a polyglycolic acid (PGA) matrix for 60 days [44]. When transplanting these cell–matrix constructs in immunocompromised mice, fibroblasts were able to survive and to produce extracellular matrix [45]. Around the same time, Gronthos and colleagues reported the isolation and characterization of a stem cell population within the dental pulp (Fig. 2). Transplantation of these stem cells in combination with hydroxyapatite/tricalcium phosphate (HA/TCP) particles in immunocompromised mice led to the formation of a fibrous pulp-resembling tissue containing blood vessels and human odontoblast-like cells, which lined a dentin matrix-like structure [34,46,47].
In spite of the numerous favorable results indicating the regenerative potential of DPSCs, clinical reality prompted the need for more standardized and representative experimental approaches, such as the tooth slice–scaffold model and the ectopic root transplantation model. Next to the investigation of dentinogenesis and the evaluation of pulp vascularization, a human tooth slice can also be adapted as a scaffold to support dental pulp regeneration [48 –50]. A couple of studies indicated the formation of vascularized pulp-like tissue after transplantation of tooth slices containing DPSCs or DPSCs from exfoliated deciduous teeth (SHEDs) in combination with a biodegradable scaffold in immunodeficient mice [51,52]. As the vascular supply within the tooth is restricted by the diameter of the apical foramen, a more exemplary model is the transplantation of emptied human root canals, that is, the ectopic root transplantation model.
In 2010, Huang et al. [53] were one of the first to show that DPSCs, seeded onto a poly(lactic-co-glycolic acid) (PLGA) scaffold, were able to form vascularized pulp/dentin-like tissue in an emptied human root canal, which had been subcutaneously transplanted into severe combined immunodeficient mice for 3 months. However, it should be noted that this study applied a rather large apical opening of 2.5 mm, which led the authors to question whether smaller canal openings would affect the efficacy of coronal tissue regeneration [53]. Vascularized pulp/dentin-like tissue was also formed in an ectopic root transplantation model of SHEDs in combination with a self-assembling peptide hydrogel. However, the authors did not seal one of the canal's ends, leading to the potential influx of nutrients and cells through both openings of the root canal [54]. When leaving an apical opening of 1 mm at one end of the human root canal, Dissanayaka et al. detected vascularized pulp-like tissue 4 weeks after transplantation of DPSCs or DPSC-human umbilical cord vein endothelial cells cocultures [55]. Similar results were reported by Yang et al. following 8 weeks of transplantation of (pretreated) DPSCs in a silk fibroin scaffold [56].
With regard to the regenerative potential of different subpopulations of DPSCs, a recent study indicated the regeneration of vascularized pulp tissue (with no mention of dentin deposition) in human root canals, sealed at one end with MTA, after a mere 21 days of subcutaneous transplantation. In particular, a G-CSF-mobilized subpopulation of DPSCs showed a significantly larger area of regenerated, vascularized pulp tissue in comparison with CD105+ DPSCs, unfractionated DPSCs, and induced pluripotent stem cells, suggesting that the regenerative potential of DPSCs as a whole is determined by the intrinsic properties of certain subsets of cells within the population [57].
Although the ectopic root transplantation model is a feasible proof-of-principle model for small animals, a more translational approach would require the in situ transplantation of DPSCs in (partly) pulpectomized teeth of larger animals. A decade ago, Iohara et al. already showed the formation of reparative dentin after autologous transplantation of bone morphogenetic protein (BMP)2-treated DPSC pellets onto the amputated pulp of dog teeth [58,59]. This group and others also indicated complete pulp regeneration after autologous transplantation of (certain subsets of) DPSCs in pulpectomized dog teeth [30,60 –62].
Recently, concrete steps toward a clinical application of DPSCs have been taken by Iohara et al. [31] through the autologous transplantation of clinical-grade G-CSF-mobilized DPSCs in permanent dog teeth with an apical opening of 0.6 mm. This study demonstrated the regeneration of vascularized and innervated pulp tissue together with the coronal formation of dentin after assuring the quality of the stem cells by karyotype analysis and ruling out potential tumor formation [2,31].
Stem cells from the apical papilla
At the apex of developing permanent teeth, a loosely attached soft connective tissue can be found, namely the apical papilla. In 2008, Sonoyama et al. [63,64] were the first to isolate and characterize the papilla's residing stem cell population, that is, SCAPs (Fig. 2). Comparative studies with DPSCs indicated a more pronounced population doubling capacity, a higher proliferation rate, and better migratory properties, indicating a more potent stem cell population. Given their origin from a developing tissue, the regenerative potential of SCAPs has gained increasing interest [63,64].
In 2006, Sonoyama et al. [63] already indicated the formation of a dentin/pulp-like complex in immunocompromised mice after transplantation of SCAPs in combination with HA/TCP particles. This study also mentioned the human origin of the dentin-producing cells, suggesting the differentiation of transplanted SCAPs into odontoblasts [63]. The in vivo odontogenic potential of SCAPs was also noted by Huang et al. after implantation of SCAPs in combination with a PLGA scaffold in an ectopic root transplantation model. Moreover, the formed dentin/pulp complex showed a more continuous and thicker dentin matrix in comparison with the model with a DPSC-PLGA construct [53]. More recently, the formation of a vascularized dentin/pulp-like complex with a continuous dentin layer has been observed following in vivo transplantation of SCAP-based cell sheet-derived pellets in dentin matrix fragments [65].
The vast body of evidence reporting continued root development after conservative treatment of immature teeth suffering from apical periodontitis and/or apical abscesses also suggests the survival of SCAPs after infection and their potential contribution to root formation by differentiating into odontoblasts [4,10,25,35,64,66 –71]. However, to date, there has only been one study showing the successful regeneration of a root/periodontal complex in an animal model after autologous transplantation of SCAPs and PDLSCs, indicating that more elaborate research is required to unravel the differentiation potential of SCAPs and their potential role in bioroot engineering [35,63].
Dental follicle precursor cells
Another developing dental tissue, which harbors stem cells, is the dental follicle (Fig. 2) [36]. The dental follicle is a loose connective tissue, which surrounds the developing tooth and later on in development gives rise to the periodontium. Given their immature nature and developmental origin, FSCs have been mainly investigated for their potential role in the regeneration of cementum and periodontal ligament [72 –79].
With regard to dental pulp regeneration, Guo et al. demonstrated the ability of rat FSCs to regenerate (pre)dentin and an odontoblast cell layer by transplanting treated dentin matrix (TDM)-FSC constructs in the omental pouch of adult rats [80]. The regenerative potential of rat FSCs was later on confirmed by the same group in a tooth root reconstruction model; transplantation of the aforementioned constructs in the alveolar fossa of adult rats not only led to the formation of a cementum-like layer and periodontal ligament but also a dentin/pulp complex [81]. Similar results were obtained after subcutaneous transplantation of human FSCs and (cryopreserved) TDM in immunocompromised mice [82,83].
These data suggest that dental follicles are an easily accessible favorable source of stem cells for the engineering of different dental tissues. However, the impact of different inductive microenvironments on the regenerative potential of FSCs as well as potential species-related differences definitely needs to be taken into account when contemplating translation into human patients. In addition, good manufacturing practice facilities and DSC banking are required to upscale the preparation and processing of DSCs in general.
DSC Banking
Dental tissues are an easily available source of mesenchymal-like stem cells as the extraction of third molars, premolars, and deciduous teeth is considered to be common orthodontic practice and the isolation of DSCs is a relatively easy and straightforward procedure.
Studies have indicated that DSCs retain their stem cell properties after (magnetic) cryopreservation of either cell cultures or whole dental tissues [84 –89]. In addition, their reported low immunogenicity and immunomodulatory properties, such as inhibition of T-cell proliferation, the inhibition of peripheral blood mononuclear cells, and the induction of T-cell apoptosis, led to an increasing interest in DSC-based regenerative therapies [90 –97]. However, the outcome of allogeneic DSC transplantation for pulp/dentin regeneration is currently not known, and the use of autologous DSCs at the time of therapeutic necessity has some drawbacks as it requires the extraction of a remaining tooth. The processing and conservation of clinical-grade DSCs in a DSC banking system would be a first step in the implementation of DSC-based regenerative therapy in a daily clinical setting [23,98].
DSC banking and serum-free cell culture
When considering the upscale production and banking of (dental) stem cells, one should definitely take into account the culture conditions that are common practice nowadays. In particular, the addition of fetal bovine or calf serum (FBS and FCS) culture media has raised a lot of controversy. Despite its critical role in the provision of nutrients and growth factors for cellular proliferation, FBS is still a potentially hazardous product of animal origin. Besides bearing the risk of transmitting zoonotic, prion, or viral infections, the xenogeneic compounds could also elicit a host immune response [99 –101]. Another important concern is the batch-to-batch variety in the quality and protein concentration of FBS and FCS [100]. Therefore, an increasing number of researchers are looking for alternative, serum-free culture conditions.
With regard to serum-free culturing of DSCs, Hirata et al. demonstrated the sustained proliferation and expression of selected stem cell markers after culturing mouse DPSCs in serum-free media supplemented with a variety of growth factors [102]. Similar findings were reported by Bonnamain et al. [103], indicating the successful expansion of human DPSCs, SHEDs, and PDLSCs in a chemically defined serum-free culture medium supplemented with growth factors [103 –105]. However, depending on the panel of added growth factors, the serum-free medium can also induce stem cell differentiation. Karbanova et al., for example, mentioned the increased expression of endothelial markers after the addition of vascular endothelial growth factor and insulin–transferrin–sodium selenite to a serum-free DPSC culture [106]. Xiao and Tsutsui also indicated the neurogenic differentiation of DPSCs, using a commercially available serum replacement in a spheroid culture model [107].
In terms of suitable alternatives, an extensive body of research has already been published on the use of (autologous) human serum or other blood derivatives in MSC cultures [108 –115]. However, as already stated by Hemeda et al. [117], the extensive amount of human alternatives required for stem cell expansion, donor-related properties, and their limited availability pose an important problem in the search for appropriate and optimal culture conditions for the upscale expansion of (dental) stem cells. The variation in the study setup also makes it difficult to compare the aforementioned reports [100,101,116,117]. Before an educated decision can be taken, more standardized research is required to inform scientists and regulatory agencies about the advantages and risks of different medium additives.
DSC banking and patient-related variability
When working with (autologous) stem cells, not only the quality of the preserved cells and tissues should be monitored but patient-related variability also has to be kept in mind.
The patient's general dental health, for example, could have an effect on the intrinsic biological behavior of residing stem cells. Alongi et al. [118] noticed a lower yield of DPSCs isolated from inflamed dental pulp. The presence of inflammation also seemed to alter the stem cell properties of these cells. Although the cells were capable of forming dentin/pulp complexes in vivo, DPSCs of inflamed dental pulp exhibited a decreased mineralization potential [118]. Similar results were found for PDLSCs, showing an effect of inflammation on the migratory capacity of PDLSCs and a significantly lower amount of cementum regeneration induced by PDLSCs from inflamed tissue [119]. Likewise, the proliferation rate and differentiation potential of DPSCs are significantly affected by the presence of deep caries [120,121].
Orthodontic treatment is another aspect, which needs to be taken into account when evaluating the properties of DSCs. Pressure and tension caused by orthodontic tooth movement not only mediate bone remodeling and potential root resorption but they can also induce differentiation of residing DSCs [122 –124].
Aside from dental health, general health-related factors as well can have an impact on pulp homeostasis and DSC behavior. For example, an increase in pulp cell number was observed in rats subjected to a dietary deficiency of essential fatty acids [125]. Smoking, that is, nicotine, on the other hand not only affects the mineralization potential of DPSCs but also activates apoptotic pathways in PDLSCs [126,127].
A final factor that certainly needs to be considered is the donor's age. Given the emergence of MSCs as a potential treatment in various disease settings and the increasing number of ongoing clinical trials, multiple studies have already reported on the age-related decline in number and function of MSCs present in adult organs. Not only do MSCs express an age-related gene signature but aging also significantly affects their angiogenic properties as well as their plasticity [128 –131]. With regard to DSCs in particular, age-related effects on proliferation and migration, as well as differentiation potential were found in DPSCs as well as PDLSCs [132 –134]. Iohara et al. also indicated a diminished regenerative potential of DPSCs isolated from aged dogs [132]. Atari et al., on the other hand, showed the expression of stem cell genes in DPSCs from donors ranging from 14 to 60 years old [135]. These results have recently been confirmed by Kellner et al., stating that age is not a crucial factor in the maximal division potential of DPSCs and that cells derived from donors ranging from 12 to 30 years old are all suitable for stem cell banking [136].
In conclusion, the implementation of a public DSC banking system not only requires careful evaluation and legislation at different levels but it also demands further characterization of confounding factors such as age and (oral) health before any clinical need can be met.
Scaffolds
Besides responsive (stem) cells and growth factors (which are potentially delivered by cellular vehicles), tissue engineering requires the use of scaffolds to support and maintain a complex tissue organization [137,138]. Within the field of regenerative dentistry, numerous potential tissue substitutes have already been tested, one being more successful than the other (Tables 1 –3). An ideal scaffold should strongly sustain the physiological needs of the cells it supports; that is, it should closely resemble the natural extracellular matrix. Besides being biocompatible and providing conductive and structural support, scaffolds also require a predictable and controlled biodegradation into nontoxic waste products [138,139].
BMP, bone morphogenetic protein; TGF, transforming growth factor; DPSC, dental pulp stem cell; SHED, dental pulp stem cell from exfoliated deciduous teeth; PEG, polyethylene glycol.
TCP, tricalcium phosphate.
FSC, dental follicle precursor cell; SCAP, stem cell from the apical papilla.
Collagen
Collagen, for example, is a naturally occurring macromolecule with excellent biocompatibility, which has been widely applied in the regeneration of dental tissues (Table 1). In 1994, Nakashima already reported the formation of dentin following transplantation of collagen matrix combined with human BMP in the pulp cavity of dogs [140]. To date, a number of studies have described the regeneration of (vascularized) dentin/pulp-like tissue after combining collagen scaffolds with DPSCs in different animal models [52,54,141,142]. However, when contemplating the use of collagen and DSCs, one must take into account the strong matrix contraction caused by DPSCs, potentially limiting cell proliferation and obstructing tissue regeneration [143,144]. Due to its isolation from allogeneic tissue sources, the usage of collagen can also hold the risk of potentially transmitting species-related pathologies or of eliciting an immune response [139,145].
Fibrin and hyaluronic acid
Other naturally occurring biomaterials that are frequently applied in dental tissue engineering are fibrin and hyaluronic acid (Table 1). Due to its low mechanical stiffness and rapid shrinkage, fibrin is often used as a composite scaffold to improve its mechanical properties [145]. Galler et al., for example, demonstrated the formation of vascularized tissue following transplantation of dentin disks containing polyethylene glycol-modified fibrin and DPSCs in immunocompromised mice [146]. Suspension of porcine tooth bud cells in a mix of fibrin glue and PRF also led to the successful regeneration of dental tissues, that is, a vascularized dentin/pulp complex, cementum, and periodontal ligament, in a minipig tooth socket [147]. Likewise, the use of fibrin gel on its own resulted in the ingrowth of pulp-like tissue in an ectopic root transplantation model [148]. Vascularized pulp tissue formation was also reported by others when using hyaluronic acid either as a composite scaffold or on its own [149,150].
Polylactic acid, PGA, and PLGA
Besides naturally occurring biomaterials, synthetic polymers are also frequently used in regenerative dentistry (Table 2).
The combination of poly-(
Besides PLLA and PGA, a copolymer of both materials has also been successfully applied in dental tissue engineering (Table 2). Young et al., for example, mentioned the formation of a recognizable dentin/pulp complex following 20–30 weeks of transplantation of tooth bud cells seeded on PLGA scaffolds in the omentum of rats [152]. Similar results were observed by others, indicating the promotion of dentin/pulp-like tissue formation when combining distinct variations of PLGA scaffolds with dental (stem) cells in different animal models [53,141,154,155].
HA, calcium phosphate, and dentin matrix fragments
Next to their application in the healing of large bone defects, HA and TCP are frequently used scaffold materials for dental pulp tissue engineering (Table 3). Following the discovery and characterization of DPSCs, Gronthos and colleagues elaborately described the regeneration of dentin/pulp-like tissue after subcutaneous implantation of DPSCs and HA/TCP particles [34,46,47]. HA is a naturally occurring mineral, which comprises an extensive part of the composition of dentin.
As dentin matrix contains numerous proteins with a substantial influence on biological processes, such as cell proliferation, angiogenesis, and even dental regeneration, (treated) dentin matrix fragments are often used as a scaffold material (Table 3) [13 –15,52,156]. In particular, the regenerative potential of FSCs in combination with (cryopreserved) TDM has been investigated extensively [80 –83]. Transplantation of SCAPs in combination with dentin matrix fragments also led to the formation of a vascularized dentin/pulp-like complex with a continuous layer of dentin [65].
Self-assembling peptide hydrogels
Self-assembling peptides are biocompatible peptide chains consisting of naturally occurring amino acids capable of generating fibrous networks, which can be easily modified to meet specific requirements such as biodegradability [139]. In 2010, Galler et al. addressed the use of a self-assembling peptide hydrogel for regenerative dentistry (Table 3) [157]. Subcutaneous implantation of dentin cylinders filled with growth factor-laden hydrogels led to the ingrowth of fatty tissue and fibrous connective tissue. When encapsulating DPSCs in the same hydrogels, the formation of vascularized pulp-like tissue was observed following a transplantation period of 5 weeks [158].
With regard to the application of commercially available self-assembling peptide hydrogels, recent work of Cavalcanti et al. indicated that DPSCs were not only able to survive and proliferate in Puramatrix™ but the hydrogel also allowed the cells to differentiate into odontoblasts when applied into a tooth slice model [159]. The same scaffold was used in combination with SHEDs or DPSCs in an emptied root canal, demonstrating the regeneration of a vascularized dentin/pulp complex following transplantation in immunodeficient mice [54,55].
In summary, this overview suggests a particular role for customized synthetic polymers and peptides in dental pulp tissue engineering. However, more elaborate research on the modification of material properties and the in vivo behavior of the scaffolds is required before a widespread clinical application is possible.
Conclusion
Although REPs have yielded an impressive body of favorable outcomes, the treatment of necrotic immature permanent teeth in particular remains to be a challenge. An objective thorough comparison of the myriad of case reports not only requires the meticulous application of a standardized treatment protocol but also prompts the need for the expansion of the pre-existing clinical databases. Next to improving the knowledge of clinicians and patients, the enhanced gathering of information will also pave the way for the first, randomized clinical trials.
With information and standardization being the keywords, the implementation of potential treatment alternatives such as dental tissue engineering not only requires a systematic comparison between the in vitro and in vivo behavior of DSCs but also involves the indepth evaluation of patient-related properties and the potential harmful effect of culture medium additives. Only in that way, the field of regenerative dentistry can strive for better alternatives for patients who no longer benefit from current treatment protocols.
Footnotes
Author Disclosure Statement
No competing financial interests exist.