
Abstract
Multiple studies have been performed to evaluate the effects of mesenchymal stem cells (MSCs) in animal models of Parkinson's disease (PD). We performed a meta-analysis to estimate the treatment effect of unmodified MSCs on behavioral outcomes in preclinical studies of PD. We performed a systematic literature search to identify studies that used behavioral testing to evaluate the treatment effect of unmodified MSCs in PD models. Meta-analysis was used to determine pooled effect size for rotational behavior and limb function, and meta-regression was performed to explore sources of heterogeneity. Twenty-five studies, including three delivery routes, a wide range of doses, and multiple PD models, were examined. Significant improvement was seen in the pooled standardized mean difference (SMD) for both rotational behavior [SMD: 1.24, 95% confidence interval (95% CI): 0.84, 1.64] and limb function (SMD: 0.84, 95% CI: 0.01, 1.66). Using meta-regression, intravenous administration and higher dose had a larger effect on limb function. Treatment with MSCs improves behavioral outcomes in PD models. Our analyses suggest that MSCs could be considered for early-stage clinical trials in the treatment of PD.
Introduction
S
PD is the second most prevalent neurodegenerative disease behind Alzheimer's disease. PD is currently diagnosed clinically based on the presence of bradykinesia plus variable expressions of tremor, rigidity, and postural instability. The pathologic hallmark is dopamine depletion in the striatum and degeneration of the substantia nigra pars compacta [4,5] with the presence of intracytoplasmic eosinophilic alpha synuclein inclusions known as Lewy bodies. Current treatment strategies are primarily symptomatic and directed toward attenuating the motor and nonmotor features of the disease. However, long-term consequences of current medical therapies result in unwanted motor complications [6,7]. Therefore, progress must be made in improving treatment strategies directed toward slowing or halting disease progression.
To test both pathogenesis and treatment effect in PD, animal models have been developed with the most promising research demonstrated in cell therapy. Cell therapy has been explored in both animal models and clinical trials as a future treatment for various neurological disorders, including PD. Animals exposed to neurotoxins or pesticides to produce parkinsonian symptoms have been successfully treated with fetal midbrain grafts [8,9] as well as embryonic stem cells [10 –12], with some enriched to promote dopaminergic cell differentiation. Clinical trials involving transplantation of both embryonic and fetal-derived dopaminergic cells had inconclusive initial results [13]; however, follow-up 2–4 years later indicated a possible improvement in motor symptoms in some patients transplanted with embryonic tissue [14]. More recently, grafts have been shown to survive 14 years post-transplant [15] and symptomatic relief has been reported at 15 and 18 years post-transplant [16]. Limited tissue supply, graft-induced dyskinesia [17], and ethical concerns pose difficulties for the development of an embryonic or fetal-derived treatment.
Mesenchymal stem cells (MSCs) are another promising cell-based therapeutic strategy for neurological disorders for the following reasons: (1) MSCs are easy to obtain from multiple tissue sources [18 –20], (2) MSCs can migrate to sites of injury [21,22], (3) MSCs release a variety of secreted biological factors [23 –26], (4) MSCs may develop neuronal phenotypes under proper conditions [27], and (5) MSCs are not accompanied by the same ethical concerns as embryonic or fetal-derived cells. Clinical trials have demonstrated that autologous MSC administration is safe using intravenous (IV) administration in ischemic stroke [28] and multiple sclerosis [29] as well as spinal cord transplantation in amyotrophic lateral sclerosis [30] and intracerebral [31,32] and intra-arterial [33] transplantation in PD.
The efficacy of MSCs has been evaluated in 6-hydroxydopamine (6-OHDA) [34], rotenone [35], and 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) [36] animal models of parkinsonism. Although the mechanisms of action are unclear, positive results have been observed on immunohistochemical and behavioral testing. Behavioral testing allows insights into functional benefits of a treatment versus tissue analysis or metabolite measurement. For example, induced rotation has been shown to be related to the extent of nigrostriatal lesions [37] and dopamine content [38]. To consider the application of MSCs in a clinical trial involving patients with PD, we performed a meta-analysis to review the preclinical studies and estimate the treatment effect of MSCs on behavioral sensorimotor analysis in animal models of PD.
Materials and Methods
Systematic search
We performed a meta-analysis examining the pooled effect size of the administration of unmodified MSCs on behavioral outcomes in preclinical animal models of PD. Controls within each study were used for comparison, and heterogeneity was assessed by meta-regression analysis. Therefore, the participants were preclinical animal models of PD, the intervention was administration of unmodified MSCs, the studies were evaluated by comparing MSC to control-treated groups, and the outcomes were behavioral testing.
We undertook a comprehensive systematic search to identify all published studies of MSC therapy in animal models of PD using electronic databases (PubMed, Scopus, Embase, and Medline). We conducted the search based on the keywords of “animal, animal model, Parkinson, mesenchymal stem cell(s), and marrow stromal cell(s).” In addition, we identified articles by reviewing references from a recent review article on stem cells and PD [39]. The inclusion criteria for animal PD studies were as follows: (1) use of unmodified MSCs in at least one experimental group; (2) behavioral testing to measure response to treatment; (3) Parkinson's animal model or PD; (4) available in English; and (5) original data (not a review). We excluded studies only testing types of stem cells other than mesenchymal cells, studies that delivered MSC treatment before lesion induction, and studies with incomplete reporting of data or sample size. Studies published through the end of 2014 were included. Figure 1 shows our systematic search to identify all articles for the meta-analysis.
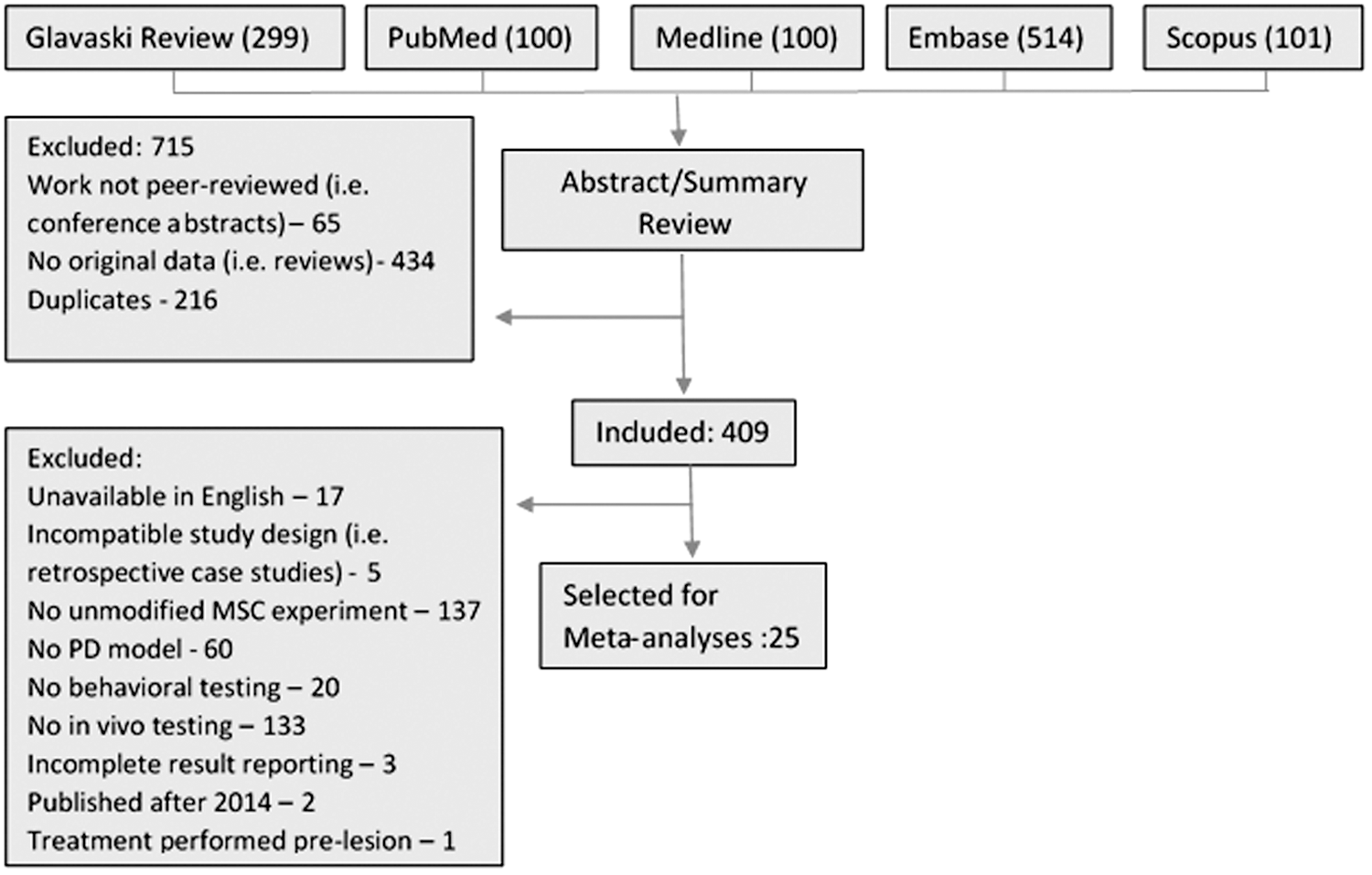
Summary of systematic literature search.
Data extraction
Data were extracted from text and graphs in each paper. When only graphical representation was available, values of mean and standard deviation (SD) or standard error (SE) were extracted from images by two abstractors. The mean difference between two abstractors was 2.6% for these data points. Average readings of two abstractors from graphs were used for data analysis. For each article, we collected article information, source of MSCs, route of administration, type of lesion model, dose of MSC, days between lesion and treatment, species of animals, number of animals per study arm, duration of follow-up period, as well as the outcome data from behavioral tests. SE was converted to SD for the studies if only SE was reported.
Quality assessment
We modified a previously published 11-item quality scale [40,41] to assess the methodological quality of included studies. Our scale consisted of the following seven items: (1) randomized assignment to treatment groups; (2) monitoring of any physiologic parameters during the surgical procedure (eg, temperature, blood pressure, etc.); (3) blinded outcome assessments; (4) assessment of ≥2 outcomes; (5) outcome assessment in the chronic phase (beyond 7 days); (6) pretreatment behavioral assessment; and (7) blinded administration of treatment or vehicle. Studies were then classified into three quality categories: category 1, 6–7 items; category 2, 3–5 items; and category 3, 0–2 items.
Statistical analysis
Outcomes of interest were results on the rotation behavior test or limb function tests. Limb function was defined as any test that analyzed forepaw use (cylinder, step, and adhesive removal tests). We calculated the effect size of MSC therapy, defined as the standardized mean difference (SMD) of these outcomes between MSC and sham groups, based on Hedges' method, which incorporates a bias correction factor for small studies. Fixed or random-effects model was performed according to the overall heterogeneity, which was examined with I 2 and Cochran's Q-statistic test [42]. A P value<0.1 was considered statistically significant for the Cochran's Q-statistic test [43]. If heterogeneity existed, the random-effects model based on DerSimonian and Laird method was applied to obtain the pooled effect size. We generated forest plots to depict the SMD along with its 95% confidence interval (95% CI) for each individual study as well as the pooled mean difference by combining all studies. The statistical significance of the pooled effect size of all studies was performed by z-test. A leave-one-out sensitivity analysis was performed by iteratively removing one study at a time to confirm whether our findings were driven by any single study. If needed, we multiplied by −1 for the consistency of larger values indicating superior outcome. Only the last time point measurements were examined for behavioral testing if outcomes were reported at multiple time points. For quality assessment score, the median and interquartile range of scores across studies were reported.
In addition, if a significance of heterogeneity was found, a meta-regression analysis was performed to assess whether heterogeneity among results of multiple studies was related to six specific characteristics of the studies: MSC dose, duration of follow-up period, species (Sprague Dawley vs. Wistar vs. Mouse), route (intravenous vs. intrastriatal), days between lesion and treatment, and quality assessment score. Potential publication bias was evaluated using funnel plots, and Egger test was performed to evaluate the symmetry of the funnel plots [44]. All analyses were performed with StataMP 11 (StataCorp LP, College Station, TX).
Results
Study characteristics
We identified a total of 25 studies (Table 1) involving all rats or mice. The delivery routes were intravenous, intranasal, or intrastriatal. Eighteen studies (72.0%) were post-treatment ranging anywhere from 5 to 30 days after lesion induction. Median duration of follow-up on neurological testing was 42 days. There were 18 (72.0%) studies using 6-OHDA, 3 studies using MPTP, 1 study using MG-132, and 3 studies using rotenone.
6-OHDA, 6-hydroxydopamine; IV, intravenous; Q1, first quartile; Q3, third quartile; MPTP, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine; MSC, mesenchymal stem cells.
For any study, if multiple outcomes or tests were reported and a separate control group was used, we considered these separate outcomes or tests as independent experiments within one study. There were 20 experiments conducted to evaluate rotational behavior and 8 experiments conducted to evaluate limb function. In addition, there were three studies using the rotarod test [36, 81, 83] and three studies using the open field test [80, 84, 89]. Because of insufficient numbers, these studies on rotarod and open field were not included in the meta-analysis.
Effect size on neurological testing
For rotation behavior, data from a total of 20 experiments were reported. The Cochran's Q-statistic test suggests there was significant heterogeneity (P value<0.0001) among these studies and the pooled effect size of MSC therapy was estimated based on the random-effects model. The estimated pooled SMD showed substantial and significant improvement with MSC treatment (SMD: 1.24, 95% CI: 0.84, 1.64) (Fig. 2) [23, 34, 35, 45, 52 –55, 57, 58, 77 –81, 85 –88]. Similarly, data from eight experiments (three step tests, two adhesive removal tests, and three cylinder tests) were reported for evaluating the effect of MSCs on limb function. Significant heterogeneity was observed across the studies (P value<0.0001) and using the random-effects model, the estimated pooled effect size of MSC therapy with 95% CI was 0.84 (0.01, 1.66) with P value<0.05 (Fig. 3) [23, 45, 63, 81, 82].

Forest plot of standardized mean difference (SMD) of rotation behavior between MSC therapy and sham groups along with 95% confidence interval (95% CI). The size of data markers represents the weight that each study contributes to the meta-analysis. The overall estimate and confidence interval are marked by a diamond. The P value of testing whether the overall SMD is different from 0 is <0.0001. The P value of Cochran's Q-statistic test for heterogeneity is <0.0001. MSC, mesenchymal stem cell.
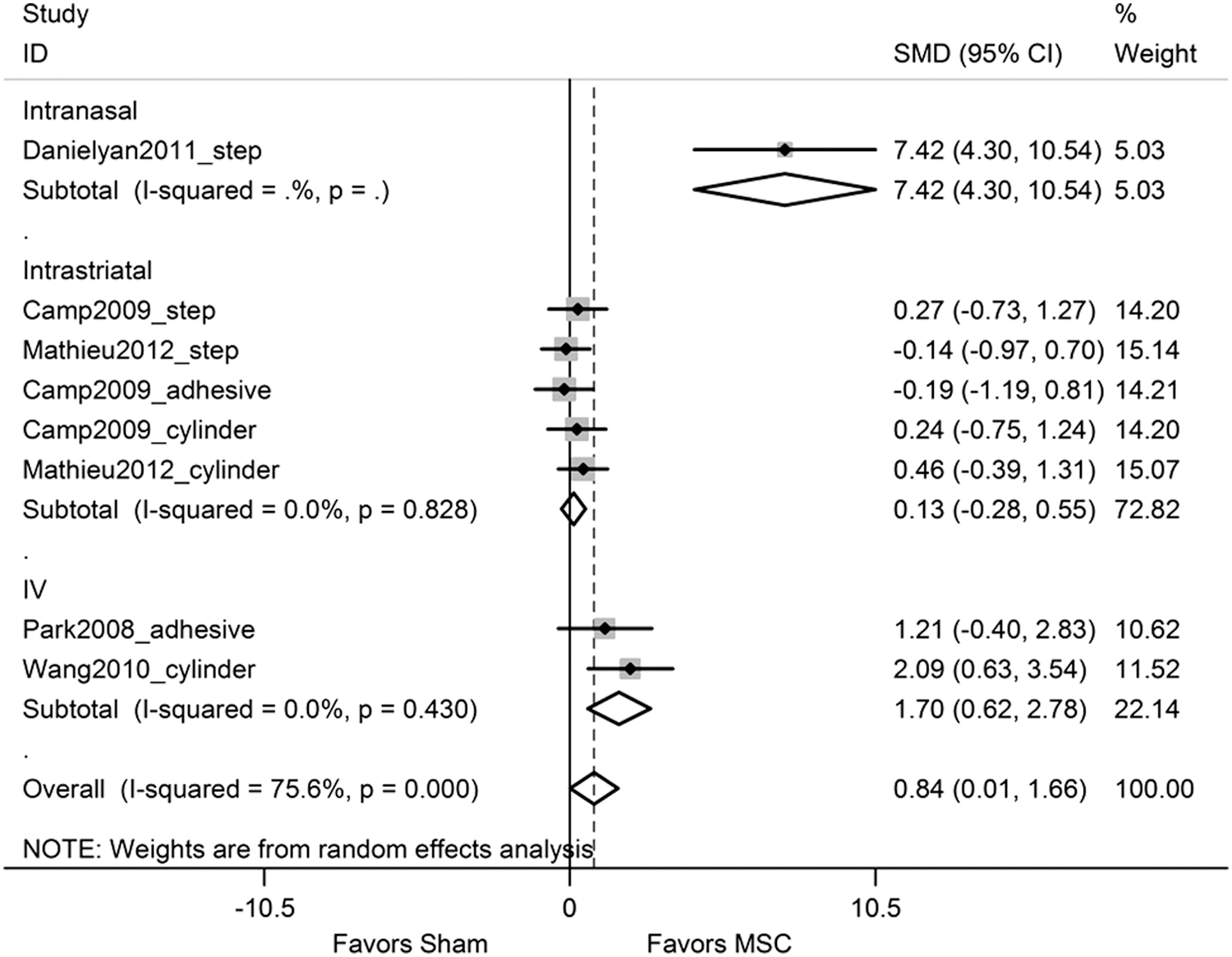
Forest plot of SMD of limb function between MSC therapy and sham groups along with 95% CI stratifying by different types of route. The size of data markers represents the weight that each study contributes to the meta-analysis. The overall estimate and confidence interval are marked by a diamond. The P value of testing whether the overall SMD is different from 0 is 0.047. The P value of Cochran's Q-statistic test for heterogeneity is <0.0001.
Meta-regression
For rotation behavior, there was no significant difference in effect size depending on delivery route, dose, duration of follow-up time, and treatment time after lesion induction. For limb function, we observed a significant difference in effect based on dose with higher dose (<1×106 vs. ≥1×106), indicating larger effect size (P value=0.042) and delivery route favoring IV compared with intrastriatal in univariate analysis (P value=0.045). The forest plot stratified by different delivery routes for limb function is shown in Fig. 3. The pooled effect size in studies using IV route with 95% CI for limb function was 1.70 (0.62, 2.78) with P value=0.002. However, the pooled effect size in studies using intrastriatal route was not significant.
Sensitivity analysis
To evaluate the robustness of the estimated pooled effect size for rotation behavior and limb function, we performed a leave-one-out sensitivity analysis by iteratively removing one study at a time and recalculating the pooled effect size of the remaining studies. For rotation behavior, the pooled effect was stable, indicating that the results were not driven by any single study. For limb function, if the only intranasal experiment [45] was removed from the study, the pooled effect size of MSC therapy based on other studies with 95% CI would be 0.39 (−0.10, 0.88), which is not significant and narrower than the original one.
Publication bias
Figures 4 and 5 show the funnel plots for the outcomes of rotation and limb function, respectively. The P values obtained from Egger's test for asymmetry of the funnel plot were 0.0001 for both outcomes. Those significant P values suggest asymmetric funnel plots that may indicate the possibility of either publication bias or a systematic difference between smaller and larger studies.
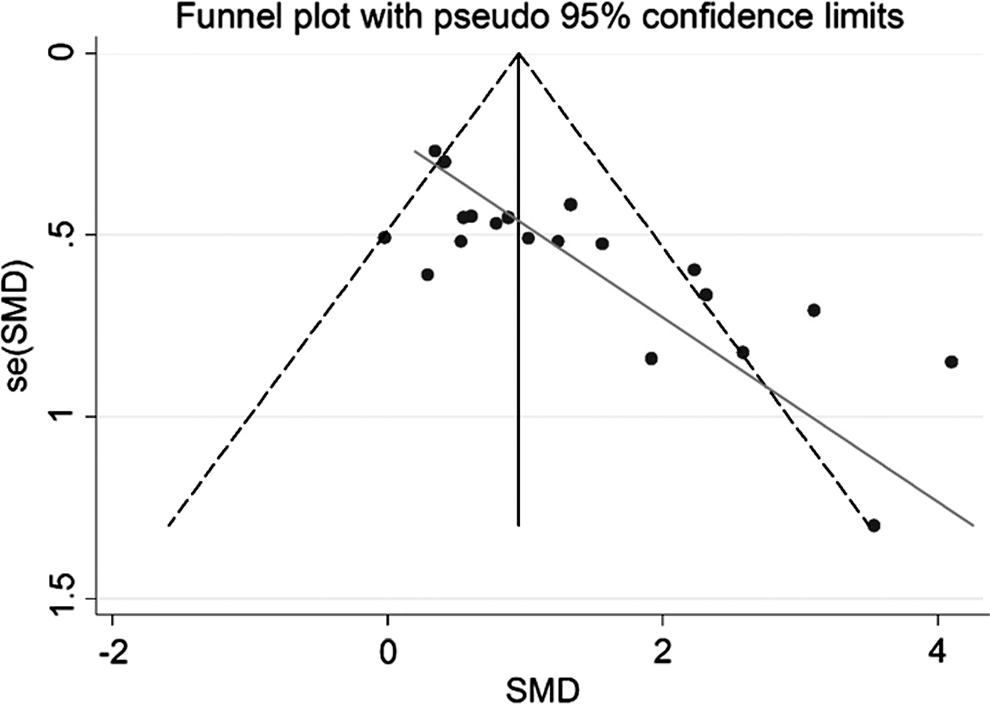
Funnel plot for effect size of MSC therapy for rotation behavior. Individual study results are represented by dots. The solid vertical line represents the pooled effect size. The dashed diagonal lines represent pseudo-95% confidence limits around the pooled effect size for each standard error (se) on the vertical axis. The diagonal solid line represents the fitted line between the treatment effect and its standard error for each study using Egger's test.
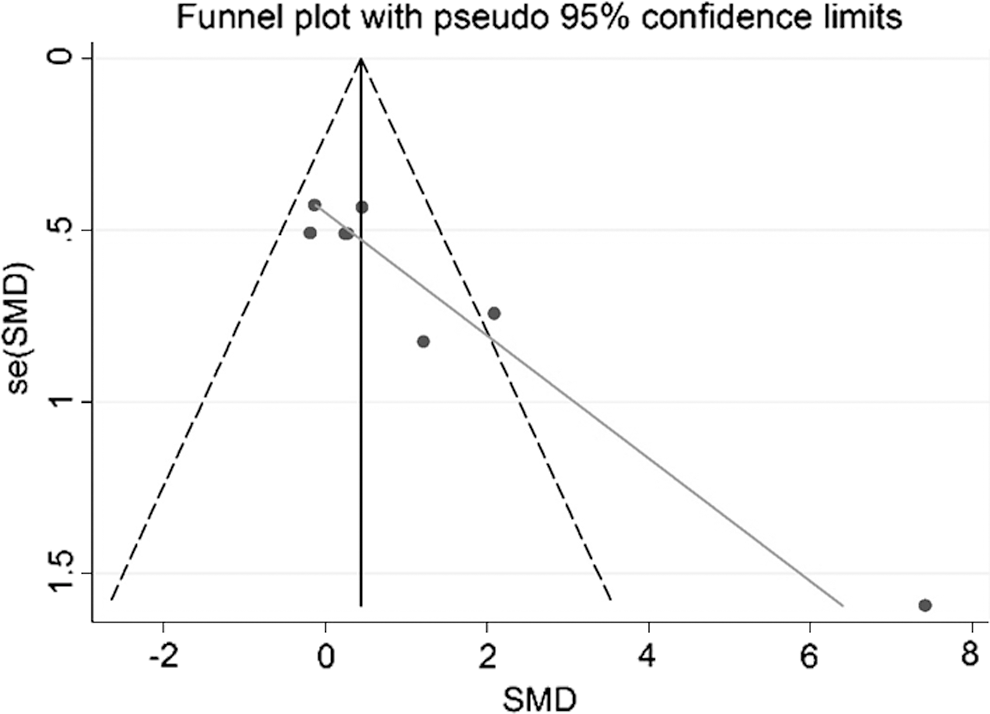
Funnel plot for effect size of MSC therapy for limb function. Individual study results are represented by dots. The solid vertical line represents the pooled effect size. The dashed diagonal lines represent pseudo-95% confidence limits around the pooled effect size for each standard error (se) on the vertical axis. The diagonal solid line represents the fitted line between the treatment effect and its standard error for each study using Egger's test.
Quality assessment
The median quality assessment score was 3.0 [interquartile range (IQR) 3–4]. The proportions of meeting each quality score criterion and proportions of studies in each score category are displayed in Table 2. The relationship between quality assessment score and the treatment effect was evaluated through meta-regression analysis within each type of outcome measure. We did not observe any significant impact of quality assessment score on treatment effect (P value=0.89 for rotation behavior and P value=0.09 for limb function).
Discussion
Based on our meta-analysis, treatment with MSCs significantly improves neurological outcomes in animal models of PD. We found a significant pooled treatment effect on rotation behavior and limb function. We analyzed behavioral outcomes, because we were the most interested in functional recovery, and behavioral testing is a parameter that is widely used to measure functional disability and recovery in animal models of neurological disorders [46 –48]. We examined rotational behavior, which is a long-standing measure of functional status in hemiparkinsonian rodent models that has been shown to correlate with nigrostriatal markers in 6-OHDA-treated rats [49,50]. More recent work has suggested that although rotational behavior is a good indicator of nigrostriatal dopamine depletion, additional testing of limb function also provides more clinically relevant data [48,51]. To date, this is the first meta-analysis of the effect size of unmodified MSCs on behavioral outcomes using rotational behavioral and limb function in preclinical studies of PD. Many studies have also examined various MSC modifications, including differentiation toward a neural lineage [52 –55], and expression of factors such as glial cell-line-derived neurotrophic factor [56], nerve growth factor [57], or persephin [58].
Clinical trials involving cell therapies for PD date back to the late 1980s when fetal dopaminergic grafting was performed [59]. Improvement was observed in some patients in multiple open label studies, although results were variable [60 –62]. More recently, two double-blinded trials showed that younger patients and those with milder disease were responsive to embryonic dopaminergic grafts [13,17]. However, the development of graft-induced dyskinesia [14,17] limited tissue availability, and ethical considerations have raised concerns through the years about fetal grafting. Many investigators have turned to alternative adult-derived cells such as MSCs, because they are easily obtainable and lack the ethical concerns that come with cells of fetal or embryonic origin.
Unlike previous clinical trials with fetal grafts, MSC treatment aims at altering the cellular environment of injured or vulnerable brain areas. Although some studies suggest differentiation of MSCs toward a neuronal phenotype or fusion with host neurons, the functional recovery that occurs with MSC treatment in animals is far more likely to result from secreted biological factors that MSCs produce [39]. MSCs are known to potently modulate the immune system and dampen the inflammatory response in various brain injury models [63 –65]. In PD models, MSCs reduce various pro-inflammatory cytokines and microglial activation, which are believed to contribute to ongoing neuronal degeneration and disease progression [45,66,67]. MSCs have also been shown to protect neurons by upregulating the expression of anti-apoptotic factors [35]. In addition, MSCs have been shown to lead to an increase in tyrosine hydroxylase-positive cells that also stain for cell proliferation markers, which may result from their known ability to stimulate endogenous neurogenesis [68 –72].
The results of this study indicate that MSCs may be a promising candidate to bring forward to clinical trials. Our analysis included multiple models that induce parkinsonian symptoms by a variety of mechanisms, including complex 1 inhibitors (MPTP and rotenone), an oxidative catecholaminergic toxin (6-OHDA), and a protease inhibitor (MG-132). We found no differences in treatment effects across a range of doses, delivery routes, and time to administration after injury on rotational behavior. However, it is interesting to note that the studies utilizing IV administration showed a greater positive effect on limb function than intrastriatal administration. Overall, these findings suggest that MSCs may exert similar effects by intravenous delivery and that more invasive, intracranial approaches may not be necessary for MSC delivery. We also observed a greater effect size of MSC therapy on limb function in studies treating animals with higher dose levels (≥1×106). Long-range studies showed positive effects till 1 year, indicating long-term and sustained treatment effects [35].
Although the effect size may be promising, we also assessed the quality of their methodology. The rigor of preclinical animal studies in neurological disorders has received increasing attention in the past few years [73]. Previous meta-analyses have suggested that animal studies that are less rigorously designed may over-estimate treatment effects [74 –76]. While the studies included in our analysis ranged in fulfilling various quality metrics, we found no correlation between the quality score of the studies and effect size. Another major limitation to a meta-analysis approach for measuring potential treatment effects is publication bias. Our methods indeed found significant publication bias supporting the concern that positive studies are far more likely to be published compared with neutral or negative studies while comparing a new therapy against controls. Furthermore, the motor tests in PD animal models do not fully capture all the components of neurological impairments of PD. Neurological outcome in PD models is also dependent on nonmotor deficits. Therefore, our results must be interpreted with caution.
In conclusion, there are extensive studies supporting a potential treatment effect of MSCs over a wide range of doses by multiple delivery routes in animal models of PD. The meta-analyses support considering early-stage clinical trials of MSCs in patients with PD.
Footnotes
Acknowledgment
None.
Author Disclosure Statement
No competing financial interests exist.