
Abstract
Craniofacial bone defects are challenging problems for maxillofacial surgeons over the years. With the development of cell and molecular biology, gene therapy is a breaking new technology with the aim of regenerating tissues by acting as a delivery system for therapeutic genes in the craniofacial region rather than treating genetic disorders. A systematic review was conducted summarizing the articles reporting gene therapy in maxillofacial surgery to answer the question: Was gene therapy successfully applied to regenerate bone in the maxillofacial region? Electronic searching of online databases was performed in addition to hand searching of the references of included articles. No language or time restrictions were enforced. Meta-analysis was done to assess significant bone formation after delivery of gene material in the surgically induced maxillofacial defects. The search identified 2081 articles, of which 57 were included with 1726 animals. Bone morphogenetic proteins were commonly used proteins for gene therapy. Viral vectors were the universally used vectors. Sprague-Dawley rats were the frequently used animal model in experimental studies. The quality of the articles ranged from excellent to average. Meta-analysis results performed on 21 articles showed that defects favored bone formation by gene therapy. Funnel plot showed symmetry with the absence of publication bias. Gene therapy is on the top list of innovative strategies that developed in the last 10 years with the hope of developing a simple chair-side protocol in the near future, combining improvement of gene delivery as well as knowledge of the molecular basis of oral and maxillofacial structures.
Introduction
C
As an alternative to traditional techniques, tissue engineering has developed as a new and promising multidisciplinary technique in the field of maxillofacial reconstruction and surgery [4].
With development of cell and molecular biology, DNA-based technology had appeared as a promising method to meet challenges of tissue engineering in different applications. The genetic principle is either applied individually or together with tissue engineering to be known as gene-enhanced tissue engineering that regenerates lost tissue by local delivery of cells that have been genetically modified to deliver signaling factors at the DNA level [5]. To date, gene therapy is the leading technology in medicine, providing hope for those individuals who are suffering genetic disorders.
Gene therapy is known to be transferring genetic material or functioning gene to replace a damaged one, inducing individual's own cells to produce a therapeutic agent to improve the clinical outcome. It has several advantages over traditional treatments as the expression in host cells lasts longer for weeks to years than pharmaceutical compounds or recombinant protein, which range from several hours to days. It reduces technical challenges associated with ex vivo protein expression and purification. Finally, the delivery of genetic sequences could mimic the natural biologic healing response [6,7].
There have been a couple of advances in gene therapy relevant to dentistry since 1995. When applying the gene therapy principles, the maxillofacial region has significant advantages compared with other locations in the body, including easy access and inspection. Gene-based tissue engineering in the oral and maxillofacial complex includes treatment of salivary gland diseases, autoimmune diseases, cancerous and precancerous lesions, pain, caries, dermatological disorders, delivery of growth factors for periodontal and pulp regeneration, treatment of malignant neoplasms of the head and neck, bone regeneration of large osseous defects in the craniofacial region, and articular cartilage repair [8,9].
Although gene therapy was originally accepted as a means of treating heritable genetic disorders, its application in the craniofacial region is more often directed at regenerating tissues by acting as a delivery system for therapeutic genes promoting healing directly to cells within the defect or by genetically engineering mesenchymal stem cell (MSC) progenitors to produce factors before implantation, resulting in higher and more constant levels of protein production [10 –12].
Thus, we have conducted a systematic review summarizing the articles reporting trials of gene therapy worldwide in the field of oral and maxillofacial surgery.
Materials and Methods
This study was registered in SYRCLE (SYstematic Review Centre for Laboratory animal Experimentation) systematic review protocol for animal intervention studies
Review questions
The following PICO question was mainly addressed: Was gene therapy successfully applied to regenerate bone or heal defects histologically or radiographically in animal studies in the field of oral and maxillofacial surgery?
Search strategy and selection criteria
A systematic review of the literature was performed to provide an overview of published articles describing gene therapy in the field of oral and maxillofacial surgery. Medical databases were searched to December 18, 2015. The data search included a combination of the following keywords: “Gene therapy” “AND” “Maxillofacial surgery” “OR” “Gene therapy” “AND” “Bone tissue engineering,” “Genetic Engineering” “AND” “Maxillofacial bone,” “Gene therapy” “AND” “Distraction Osteogenesis” “OR” “Gene therapy” “AND” “Alveolar bone” “OR” “Gene therapy” “AND” “Periodontal tissue” “OR” “Gene therapy” “AND” “Temporomandibular joint.” All the possible combinations of these words were explored. Medical subject headings (MeSH terms) without subheading restrictions were used and the heading sequence was “Gene therapy” “AND” “Dentistry.”
In addition, we performed hand search of the references of included articles, articles of interest, and related systematic or nonsystematic reviews. The International Journal of Oral and Maxillofacial Surgery, Journal of Craniomaxillofacial Surgery, Gene therapy, Molecular therapy, and Human gene therapy journals were also screened to identify possible references not reported elsewhere. No language or time restriction was enforced. Relevant full publications and meeting abstracts were identified by electronic searching of three online databases (PubMed, Cochrane library, and Web of Knowledge). After identification of articles in the databases, the articles were imported into Endnote X7 software (Thompson Reuters, Philadelphia, PA) to store, manage search results, and remove duplicates regardless of whether the studies are eventually included or excluded in the systematic review. Titles and abstracts identified were screened, resulting in a number of seemingly relevant studies for the systematic review. The abstracts of the articles were then reviewed and the full text was obtained for those articles with apparent relevance. The identified articles were selected based on the inclusion criteria and exclusion criteria. The study selection was assessed by two independent observers (R.F. and S.O.) and any differences resolved by discussion.
Inclusion criteria
(1) Studies using gene therapy for treatment of defects, (2) in vivo or animal studies, (3) surgically induced defects in the oral and maxillofacial region, and (4) any language were the inclusion criteria.
Exclusion criteria
(1) Review articles, (2) letters to the editor, editorials, poster or oral presentations, or articles with only abstract, (3) in vitro studies, (4) studies based on the use of only growth factors (protein-based) or cell-based therapies, (5) oral cancer or soft tissue lesions, (6) calvarial bone defects, and (7) gene therapy in bones other than maxillofacial were the exclusion criteria.
To improve the sensitivity of relevant studies, each publication identified in the electronic search was assessed independently by two independent reviewers (R.F. and S.O.) to make a decision on inclusion/exclusion criteria or data extraction and the quality of the articles with differences resolved by discussion.
Data extraction
All information was extracted using a standardized data form created in Excel. Data extracted included (1) Author, (2) Year, (3) Journal, (4) Country, (5) Language, (6) therapeutic gene, (7) Vector, (8) Control gene, (9) Virus titers (Concentration), (10) Cell lines for generation of virus, (11) Experiment design, (12) Defect model, (13) Site, (14) Animal model, (15) Sample size, (16) Defect size, (17) Carrier/Scaffold, (18) Gene delivery route, (19) Stem cell source, (20) Experimental groups, (21) Cell concentration to be used in the defect, and (22) Analysis methods with main endpoint results.
Data were extracted from either text or tables in the results section of the included studies by two independent observers (R.F. and S.O.). Data were extracted electronically from graphs using WebPlotDigitizer software, version 3.10 (WebPlotDigitizer, US;
Reporting the quality of submitted articles of animal studies (ARRIVE guidelines)
The reporting quality of all the included studies in this systematic review was performed based on ARRIVE (Animal Research: Reporting In Vivo Experiments) guidelines, which were designed to be used when submitting articles describing animal research [15], and evaluated based on a predefined grading system [16] applied to the following items: (1) Title, (2) Abstract/Summary, (3) Introduction/Background, (4) Introduction/Primary and secondary objectives, (5) Methods/Ethical statement, (6) Methods/Study design, (7) Methods/Experimental procedure, (8) Methods/Experimental animals, (9) Methods/Housing and husbandry, (10) Methods/Sample size, (11) Methods/Allocation animals to experimental groups, (12) Methods/Experimental outcomes, (13) Methods/Statistical methods, (14) Results/Baseline data, (15) Results/Numbers analyzed, (16) Results/Outcomes and estimation, (17) Results/Adverse events, (18) Discussion/Interpretation and scientific implications, (19) Discussion/Generalizability and translation, and (20) Discussion/Funding.
Risk of bias assessment
Collaborative Approach to Meta-Analysis and Review of Animal Data from Experimental Studies (CAMARADES) risk of bias tool was applied to assess the internal validity of included studies using RevMan software (version 5.3) [17,18]. A modified 7-point item checklist was used to assess the risk of bias, including (1) published in a peer-reviewed journal; (2) random allocation to treatment or control; (3) treatment allocation concealment; (4) blinded assessment of outcome; (5) reporting of a sample size calculation; (6) statement of compliance with animal welfare regulations; and (7) statement of potential conflicts of interest. Each trial was assessed by two independent observers (R.F. and S.O.) and any differences resolved by discussion.
Outcome measure
Bone formation was the only primary outcome measured. No secondary outcomes were measured. Bone formation was assessed as Effect size using histology (percentage of area and volume) or radiograph (bone volume fraction) between the experimental and control groups was assessed as effect size. Effect size quantifies the size of the difference between two groups and interprets the direction and magnitude of an effect of a treatment. The effect size in our review was a continuous outcome variable recorded as the mean difference (MD). The MD is the difference in the means of the treatment group and the control group. A meta-analysis is the use of statistical methods to summarize the results of the studies. According to Cochrane Handbook for Systematic Reviews of Interventions [19], meta-analysis is performed in a review to (1) increase the power of detecting a real effect as statistically significant if it exists; (2) improve precision: the estimation of an intervention effect can be improved when it is based on more information; (3) answer questions not posed by individual studies: primary studies often involve a specific type of patient and explicitly defined interventions (a selection of studies in which these characteristics differ can allow investigation of the consistency of the effect and, if relevant, allow reasons for differences in effect estimates to be investigated); and (4) settle controversies arising from apparently conflicting studies or to generate new hypotheses. Statistical analysis of findings allows the degree of conflict to be formally assessed and reasons for different results to be explored and quantified.
Grading the quality of evidence (GRADE approach)
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach [20,21] was used to assess the quality of evidence for each outcome variable included in the systematic review and the strength of recommendation regarding the use of gene therapy to regenerate bone or heal defects in animal studies in the field of oral and maxillofacial surgery. GRADEpro Guideline Development Tool was used to import data from RevMan to create the Summary of findings table. The methodological criteria by which evidence was assessed depended on five primary domains (risk of bias, inconsistency, indirectness, precision, and publication bias). The quality of evidence was judged as high, moderate, low, or very low. High quality was defined as further research is very unlikely to change our confidence in the estimate of effect; moderate quality was defined as further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate; low quality was defined as further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate; and very low quality was defined as we are very uncertain about the estimate. The quality of evidence was assessed by two independent observers (R.F. and S.O.).
Statistical analysis
A qualitative data analysis was performed with the aim of summarizing the results of the studies included. Meta-analysis as well as forest and funnel plots were conducted using RevMan software (Review Manager [RevMan] Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). Bone formation was assessed as continuous outcome variable by inverse variance method and recorded as the MD with 95% confidence interval (CI). The I2 indicating heterogeneity and Cochran's Q statistical test were calculated; a value of I2 0% to 40% might not be important, 30% to 60% may represent moderate heterogeneity; 50% to 90% may represent substantial heterogeneity, and 75% to 100% shows considerable heterogeneity [22]. A weighted random effect model was used to estimate the overall effect size. The data were aggregated using a random effect model due to the presence of heterogeneity. Results with a p < 0.0001 were considered indicative of statistical significance. RevMan provides a flexible framework for producing forest and funnel plots in the Data and analyses section of the Cochrane review. Potential publication bias was explored using funnel plots generated using RevMan.
Results
Search results
The search identified a total of 2081 references from different databases and hand search: PubMed (n = 2000), Web of science (n = 63), Cochrane library (n = 7), hand search (n = 11). After duplicate removal through Endnote duplicate function, 1509 articles were screened for titles/abstracts and resulted in only 148 studies for full-text evaluation. Further screening resulted in a total of 57 studies, which were considered eligible for the systematic review and fulfilled the final selection criteria. Figure 1 illustrates the search flow and identification of eligible studies. Supplementary Table S1 (Supplementary Data are available online at
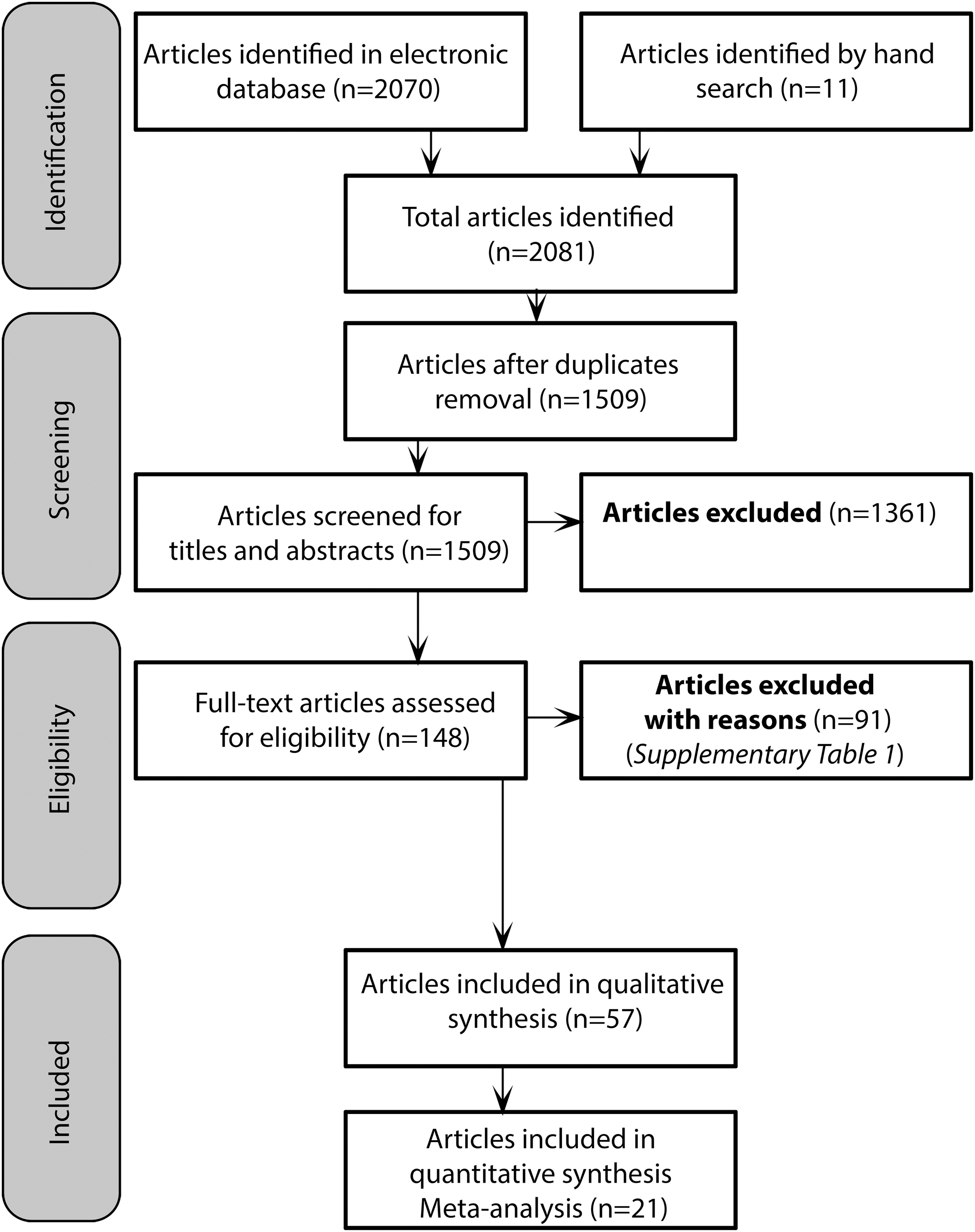
Flowchart of the process of literature search and studies included in the review.
Study characteristics
The articles analyzed were published between 1999 and 2015. Bone morphogenetic proteins (BMPs) were the most commonly used proteins for gene therapy (n = 28, 49.1%) [23 –50], followed by platelet-derived growth factors (PDGFs; n = 6, 10.5%) [47,48,51 –54], while the remaining 23 articles (40.4%) were using various proteins as follows: enhanced green fluorescent protein (EGFP) [55 –58], tumor necrosis factor alpha receptor (TNFR) [59], hepatocyte growth factor (HGF) [60], receptor activator of nuclear factor kappa-B ligand (RANKL) [61,62], basic fibroblast growth factor (b-FGF) [63,64], β-galactosidase (LacZ) [65], osterix (OSX) [66,67], LIM mineralization protein 3 (LMP-3) [68], vastatin [69], vascular endothelial growth factor (VEGF) [70], osteoprotegerin (OPG) [71 –74], runt-related transcription factor 2 (RUNX2) [75], nerve growth factor beta (NGFB) [76], tumor necrosis factor alpha-stimulated gene-6 (TSG-6) [77], mitogen-activated protein kinase (MAPK) phosphatase 1 (MKP-1) [78], and hypoxia-inducible factor-1 alpha (HIF-1A) [79].
In 30 articles (52.6%) [23 –25,27,28,31 –33,35,37,38,40,41,43,46 –54,60,63,65,68,75,78,80], adenovirus was the universally used vector. However, other vectors were used as follows: plasmid (n = 12, 21%) [26,29,30,42,44,45,55,64,66,73,74,81], adeno-associated virus (n = 4, 7%) [56,59,69,70], hemagglutinating virus of Japan (HJV; n = 3, 5.3%) [61,72,82], liposome (n = 2, 3.5%) [34,38], lentivirus (n = 5, 8.8%) [58,71,76,77,79], and retrovirus (n = 1, 1.8%) [57]. For the control genes, green fluorescent protein (GFP) was the most abundant control in 20 articles (35.1%) [25,29,30,32,33,35,43,46,48 –50,60,63,64,66,68 –70,75,76,79,81], followed by β-galactosidase (LacZ) in 9 articles (15.8%) [23 –25,27,31,37,38,40,78], and luciferase (Luc) in 6 articles (10.5%) [28,51 –55], respectively. However, in 22 articles (38.6%), the control gene was not reported. Table 1 presents the detailed characteristic of the included studies.
AAV, Adeno-associated virus; AV, Adenovirus; CRE8, Cre-expressing 293 cells; GFP, green fluorescent protein; HEK293, human embryonic kidney 293 cell line; HVJ, hemagglutinating virus of Japan; MOI, multiplicity of infection; PFU, plaque-forming unit; TU, transduction unit.
Alveolar bone defects with or without dental implant were the prevalent model used for gene therapy in 20 articles (35.1%) [23,25,26,28,30,31,35,38,40,41,44,45,48 –51,53,68,71,79], periodontal disease with or without alveolar bone involvement (n = 17, 29.8%) [27,33,36,39,42,47,52,54,55,58 –60,64,73,74,77,78], followed by distraction osteogenesis (n = 9, 15.8%) [24,29,34,37,63,66,67,75,76], temporomandibular joint (n = 4, 7%) [56,65,69,70], orthodontic tooth movement (n = 3, 5.2%) [61,72,82], sinus floor elevation (n = 2, 3.5%) [32,43], tooth restoration with bioroot regeneration (n = 1, 1.8%) [57], and central fissures (cleft) (n = 1, 1.8%) [46]. Most of the defects were in the mandible (n = 39, 68.4%) [23,24,29 –31,33 –46,48 –50,52,54,56,58,63 –71,73 –76,79], while in 16 articles (28%) [25 –28,32,43,47,51,53,55,59,61,72,77,78,82], the defects were created in the maxilla. One article reported defects in both jaws (1.8%) [60] and the location was missing in one article (1.8%) [57]. The posterior mandible (premolar–molar area) was the most frequent region. However, some studies did the experiments in the anterior region.
Sprague-Dawley rats were the frequently used animal model in the experimental studies (n = 17, 29.8%) [23,24,28,29,44,45,51
–54,56,58,59,69,70,77,78], followed by Wistar rats in six studies (10.5%) [38,55,61,68,72,82], Lewis Fisher in three studies (5.3%) [31,33,50], and guinea pigs or mice in one article each (n = 2, 3.5%) [40,65]. White New Zealand rabbits were also used as a small animal model for the studies (n = 14, 24.6%) [27,30,32,35,37,41,43,46,63,66,67,71,75,76]. For large animals models, dogs and pigs were commonly used in 11 (19.3%) [26,36,38,42,47
–49,64,73,74,79] and 4 (7%) studies, respectively [25,34,57,60]. Gene delivery route was ex vivo in 35 articles (61.4%) [25,27,29
–41,43
–46,50,56
–58,60,63,64,66
–68,71,73
–76,79], in vivo in 21 articles (36.8%) [23,24,26,28,42,47
–49,51
–55,59,61,65,69,70,72,78,82], and both in only 1 article (1.8%) [77]. The scaffolds used for seeding the cells were beta-tricalcium phosphate (β-TCP) [32,50,71], bioactive glass ceramic (BGC) [41], coral hydroxyapatite (CHA) [44,45], hydroxyapatite/collagen (HA/COL) [39,68], hydroxyapatite/beta-tricalcium phosphate (HA/TCP) [57], premineralized silk fibroin protein scaffolds (mSS) [31], natural nonorganic bone (NNB) [30], mesoporous bioglass/silk fibrin (MBG) [47], hydroxyapatite/polyamide (HA/PA) [35], pluronic F127 (PF127) [27], poly
The most commonly used analysis methods were PCR (n = 27, 47.3%) [32,33,35,38,40,42,47 –54,56,58,59,63 –65,68 –71,75,77,79], μCT (n = 20, 35%) [23,25,27,31,34,37,40,47,50,53,59, 60,63,64,68,72,75,78,79], [57], histology (n = 48, 84.2%) [23 –36,38 –44,46,47,49,50,52 –55,57,58,60,61,63 –68,71 –76,78,79,82], radiograph (n = 18, 31.5%) [24,26,29,31,35,37,38,44,46,50,57,59,63,66,67,73,75,79], histomorphometry (n = 22, 38.5%) [24,26,28 –33,35,36,41,43,44,46,47,49,50,54,57,71,76,79], and immunohistochemistry (n = 25, 43.8%) [25,29,31,33 –35,38,39,43 –45,54,57,58,61,63,67,69 –74,78,79]. Supplementary Table S3 summarizes the endpoint results of the main analytical methods used for the experiments either in vitro or in vivo.
Reporting the quality of submitted articles of animal studies (ARRIVE guidelines)
The items included in the assessment of the quality of the articles are summarized in Supplementary Table S4. The quality of finally selected studies was assessed by different categories [15,16]. A relationship was driven between the Quality Score/Maximum Score by dividing the maximum score by category to the total score (T = 36). Three possible quality coefficients were conducted: 0.8–1 Excellent, 0.5–0.8 Average, and <0.5 Poor, as reported elsewhere [15,16,83]. In the included articles, 21 articles were reported as excellent articles fulfilling nearly all the criteria of the ARRIVE guidelines with coefficients 0.8–1. Thirty-five articles were qualified as average articles with coefficients 0.5–0.8 and only 1 article was categorized as being of poor quality with coefficients <0.5. The detailed assessment of the quality of published articles included in the review according to the ARRIVE guidelines is presented in Supplementary Table S5. For more details of each category, refer Supplementary Data.
Risk of bias assessment of the included articles
Overall, all the studies were having low risk of bias in publishing in peer-reviewed journals. Random allocation of the treatment or control was reported in 29 articles [23,29 –33,37,43,50,54 –58,60,63,64,66 –73,76,77,79] and three studies [32,35,75] had a low risk of bias in random allocation concealment. Blinding of outcome assessment was performed in 13 studies [24,28,29,33,54,56,59,60,63,66,67,76,82] and only 2 studies [53,56] were reporting sample size calculation. The statement of compliance with animal welfare regulations was reported in 51 studies [24,26 –32,34 –37,39 –41,43 –50,52 –61,63 –79,82], while conflicts of interest were found in 11 studies [26,43,52,53,57,58,60,71,76,78]. More details about possible risk of bias are presented in Fig. 2.

Risk of bias graph for the studies included in this systematic review. Assessment of risk of bias using modified CAMARADES tool.
Meta-analysis
Fourteen studies were included in the histological meta-analysis of percentage of area of newly formed bone by gene therapy, whereas three studies were included in percentage of volume of newly formed bone. However, four studies were included in the radiographic meta-analysis of bone formation by calculating the bone volume fraction. Figure 3 summarizes the results of forest plot of gene therapy versus control treatment.
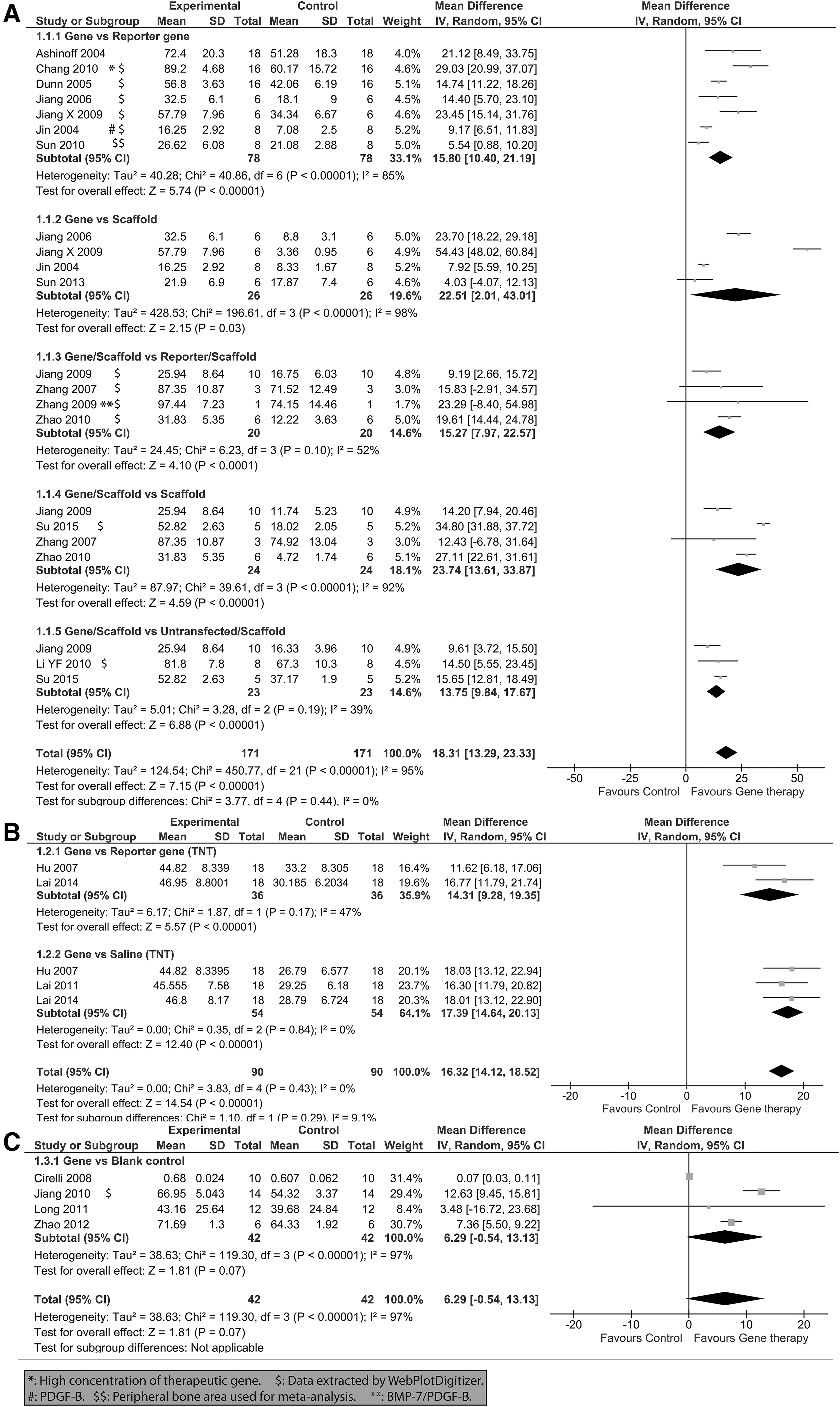
Forest plot of MD, with 95% CI in bone formation by histology and radiograph comparing different subgroups.
Percentage of area of bone formation by histology
Pooled data from gene versus reporter comprising intergroup comparisons generated from seven original studies involving 156 animals (78 treated and 78 control groups) were MD = 15.80, 95% CI = [10.40–21.19], heterogeneity: Tau2 = 40.28; Chi2 = 40.86, I2 = 85% (Fig. 3A), while data from gene versus scaffold comprising intergroup comparisons generated from four original studies involving 52 animals (26 treated and 26 control groups) were MD = 22.51, 95% CI = [2.01–43.01], heterogeneity: Tau2 = 428.53; Chi2 = 196.61, I2 = 98%.
Pooled data from gene/scaffold versus reporter/scaffold comprising intergroup comparisons generated from four original studies involving 40 animals (20 treated and 20 control groups) were MD = 15.27, 95% CI = [7.97–22.57], heterogeneity: Tau2 = 24.45; Chi2 = 6.23, I2 = 52%. However, data from gene/scaffold versus scaffold comprising intergroup comparisons generated from four original studies involving 48 animals (24 treated and 24 control groups) were MD = 23.74, 95% CI = [13.61–33.87], heterogeneity: Tau2 = 87.97; Chi2 = 39.61, I2 = 92%.
Finally, pooled data from gene/scaffold versus untransfected cells/scaffold comprising intergroup comparisons generated from three original studies involving 46 animals (23 treated and 23 control groups) were MD = 13.75, 95% CI = [9.84–17.67], heterogeneity: Tau2 = 5.01; Chi2 = 3.28, I2 = 39%.
Percentage of volume of bone formation by histology
Pooled data from gene versus reporter comprising intergroup comparisons generated from two original studies involving 52 animals (36 treated and 36 control groups) were MD = 14.31, 95% CI = [9.28–19.35], heterogeneity: Tau2 = 6.17; Chi2 = 1.87, I2 = 47% (Fig. 3B), while data from gene versus saline comprising intergroup comparisons generated from three original studies involving 108 animals (54 treated and 54 control groups) were MD = 17.39, 95% CI = [14.64–20.13], heterogeneity: Tau2 = 0.00; Chi2 = 0.35, I2 = 0%.
Bone volume fraction for bone formation by radiograph
Pooled data from gene versus reporter comprising intergroup comparisons generated from four original studies performed involving 84 animals (42 treated and 42 control groups) were MD = 6.29, 95% CI = [−0.54 to 13.13], heterogeneity: Tau2 = 38.63; Chi2 = 119.30, I2 = 97% (Fig. 3C).
Publication bias
Funnel plots of the study results are shown in Fig. 4. Symmetrical funnel plots were obtained in all the models. The funnel plot of the study standard error by effect size (MD) was symmetric. The funnel plot of standard error versus effect size (MD) was symmetrical, indicating the absence of potential publication bias among the meta-analyses of bone formation by histology (Fig. 4A, B) or radiograph (Fig. 4C).
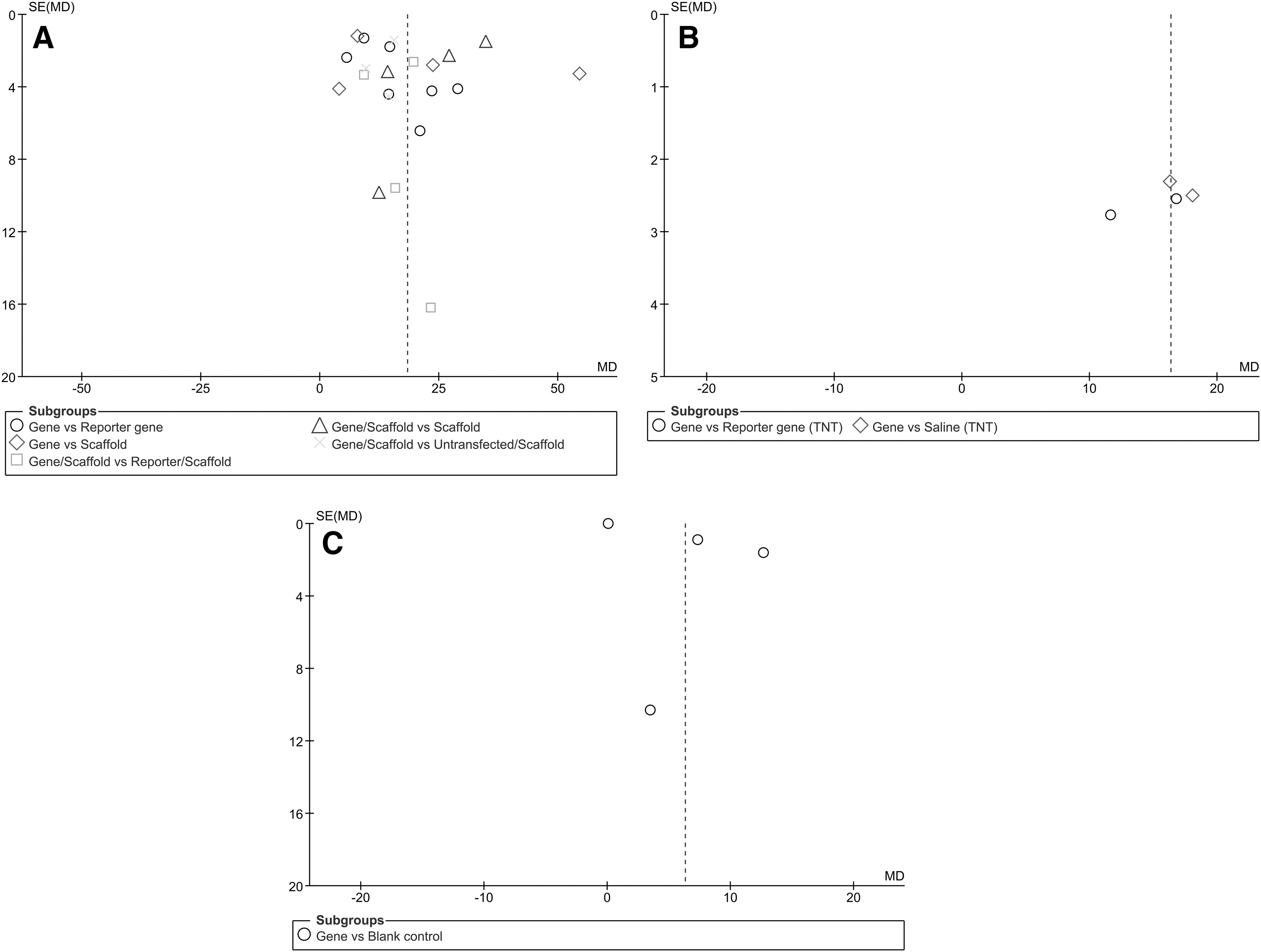
Funnel plot showing publication bias among the studies.
Quality of the evidence using GRADE approach
Using the GRADE criteria, the quality of evidence on the use of gene therapy to regenerate bone or heal defects in animal studies in the field of oral and maxillofacial surgery was very low to moderate for all assessed comparisons and outcomes (Fig. 5). These findings suggest that further research is likely to have an important impact on our confidence in the effect estimate and may change the estimate. The certainty of the evidence was downgraded because of a moderate risk of bias in studies. Additionally, inconsistency was a problem due to the large heterogeneity of the included studies as well as imprecision because of the wide CIs around the estimate of the effect and because the optimal information size was not reached.

Summary of findings table of studies comparing gene therapy versus control treatment generated by the GRADE tool. Footnotes provide detailed information about the rationale for downgrading. In short, evidence for all outcomes was rated as very low or moderate. Each outcome was downgraded on the base of risk of bias or inconsistency and imprecision in data, as shown by forest plots. GRADE, Grading of Recommendations Assessment, Development, and Evaluation.
Discussion
Several literature reviews have focused on gene therapy in bone tissue engineering, dentistry, or oral and maxillofacial surgery [9,12,84,85]. However, there has been no systematic review or meta-analysis with a specific focus on research covering gene therapy in the field of oral and maxillofacial surgery. Thus, we have conducted a systematic review of the studies addressing efforts made in the field of gene therapy for healing of maxillofacial defects, revealing the raised success rate during the recent years. Our meta-analysis results provided evidence that gene therapy was beneficial in treating maxillofacial defects in terms of improving bone formation based on histological and radiographic measures.
Although gene therapy was initially considered as a means of correcting hereditary disorders by changing the genes that cause the disease [86], more recent research is applying gene therapy to produce continuous amounts of biologically active molecules in the defects such as its potent ability for alveolar bone regeneration, periodontal healing, and dental implant osseointegration [47]. Clinical trials using gene therapy are now performed in salivary gland (
From our results, multiple genes were used as osteogenic factors for gene therapy in the maxillofacial region because of their potent induction of de novo bone formation in vivo with varying results as soluble growth factors (PDGF, FGFs), morphogens (BMPs), angiogenetic factors (VEGF), intracellular regulators (LIM mineralization protein-1: LMP-1), transcription factors (RUNX2) associated with bone, and cartilage-related gene expression [87,88]. However, BMPs were preferred candidates for local gene therapy for bone regeneration as they can initiate and sustain the entire bone formation cascade [89]. On the other hand, previous investigations had reported the effect of PDGF on osseous defect healing showing that PDGF signaling plays a role in chemotaxis and proliferation of osteoblasts and fibroblasts [90]. However, PDGF ability to induce osteogenic differentiation is less clear.
Another critical element of gene therapy is the vector, which is the vehicle that facilitates the transfer of genetic material into the target cell nucleus without causing degradation or toxicity. Two kinds of vectors have been employed: viral and nonviral vectors. Viral vectors have the advantage of being able to carry the gene efficiently and ensure long-term expression, but they can only trigger short-term gene expression and are highly immunogenic. They are also nonvirulent due to their modified genome, in which the essential viral genes are replaced by the therapeutic gene being unable to replicate in the absence of these critical gene products. Nonviral vectors could be also used due to their safety profile and minimal immunogenicity. However, the main disadvantage in their use is the insufficient transfection efficiencies [87,91 –95].
Reporter gene assays have emerged as a rapid and sensitive strategy for indirectly monitoring transgene expression by cloning the promoter region of the gene of interest correlated with the reporter gene and measuring reporter gene expression as a reflection of the expression of the gene of interest [96]. Commonly used reporter genes are GFP, which is a fluorescent protein (causing cells that express it to glow green under UV light), and luciferase (Luc) [97], which produces light by a catalytic reaction with luciferin. Another common reporter gene expressed in bacteria is the protein β-galactosidase (LacZ), causing bacteria expressing the gene to appear blue when grown on a medium that contains the substrate analog, X-gal. In our results, several reporter genes have been used, which give an add-on to the experiments, being internal controls for the expression of the gene of interest.
Various biological delivery systems have been applied for transferring the therapeutic gene to target cells. In the in vivo approach, cells can be genetically modified in situ or the vector is administered to the defect through systemic or local direct injection associated with a biomaterial. The combination of vector and biomaterial is called gene-activated matrix (GAM). GAMs are three-dimensional biomaterials acting as a scaffold for vectors introduced to a localized area and useful for avoiding unintended spread of transfection to local tissues. Regarding the ex vivo approach, cells are removed, genetically modified, and reimplanted in the defect by direct injection or using a biomaterial as carrier [98 –100].
Genetic modification of stem or progenitor cells serves as an important advancement in regenerative medicine to improve their in vivo performance. By combining gene with cell therapy, stem cell function may be enhanced by improving proliferation or differentiation of stem cells. The most common cell source is MSCs, which can be isolated from bone marrow, muscle tissue, peripheral blood, umbilical cord, adipose tissue, liver, multiple dental tissues, or induced pluripotent stem cells (iPSCs) [101,102]. The iPSCs are new source of stem cells generated from human somatic cells [103]. Various cells such as gingival or dermal fibroblasts, periosteal cells, primary articulated joint chondroblasts, bone marrow stromal cells/MSCs, muscle-derived stem cells, fat-derived stem cells, osteoblasts, and myoblasts have been successfully transfected or transduced by different vector systems [87].
Animal models are valuable tools in biomedical research in particular gene therapy to test the safety, efficacy, dosage, and localization of transgene expression in models that closely resemble human diseases. Animal craniofacial models for gene therapy exist not only for bone [104] but also for periodontal ligaments [54], temporomandibular joint [70], and cartilage [105], as well as salivary glands [106]. Such models have critical-size defects with the absence of spontaneous complete osseous regeneration of the created defects during the lifetime of the animals [107,108].
GRADE approach was a useful tool for interpreting the results of systematic reviews of animal studies indicating that when the quality of evidence is high or moderate, the more confidence we have for translating an animal study into a clinical trial. When the quality is low or very low, we suggest conducting more high-quality animal studies to assess the hypothesis regardless of whether the result is positive or negative.
Considering limitations of our systematic review, meta-analysis was conducted for only the few included studies due to the high level of heterogeneity in reporting the treatment outcomes. Statistical heterogeneity exists in our systematic review due to the fact that the true effects are being evaluated differently between studies with variation in sample size, characteristics of the samples, participants, interventions, exposures, design quality, or outcomes measured [109,110]. It is also important to consider that variability in research methodologies and characteristics of laboratory animals play a role in meta-analysis of animal studies. Moreover, the studies, which were included in our meta-analysis, generally used animal models for gene therapy. Therefore, randomized clinical studies in humans are needed to confirm our conclusions. However, meta-analysis was performed only for articles that had clearly reported bone formation (primary outcome) either by percentage of area or volume histologically as well as radiographically.
Conclusion
Challenging approaches had emerged for oral and maxillofacial reconstruction in the last decade due to the complex nature of craniofacial defects. Tissue engineering is attracting the spotlight as a new paradigm for bone regeneration, which requires the collaboration of multidisciplinary teams of surgeons, biologists, and biomedical engineers. Gene therapy is on the top list of innovative strategies in tissue engineering that developed in the last 10 years. While significant progress has been made toward preclinical studies of gene therapy in the maxillofacial region building the scientific basis of this technique, gene therapy is still in the clinical trials phase in salivary glands and craniofacial defects.
Footnotes
Acknowledgment
The authors would like to thank SYRCLE organization for their helpful comments and discussion.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.