
Abstract
Our previous studies demonstrated promising outcomes after haploidentical donor transplant combined with unrelated umbilical cord blood (haplo-cord- hematopoietic stem cell transplantation [HSCT]) for hematological disorders. However, clinical profiling regarding chronic graft-versus-host disease (cGVHD) has not yet been fully described under this protocol. This study analyzed the clinical characteristics of cGVHD among 300 patients with hematological malignancies who received haplo-cord-HSCT between January 2012 and July 2016 at our center. During the follow-up, the 5-year cumulative incidence of cGVHD based on the National Institutes of Health (NIH) consensus criteria was 32.2% (95% confidence interval [CI], 28.7–35.7); the 5-year cumulative incidence of moderate to severe cGVHD was 11.4% (95% CI, 9.4–13.4). After the multivariate analysis, the GVHD overall survival (GOS) was associated with relapse, thrombocytopenia, bronchiolitis obliterans syndrome, and steroid-refractory cGVHD. The infused CD34+ cells (≥3.46 × 106/kg) from haploidentical grafts were a protective factor affecting GOS. This study proposed a nomogram for predicting GOS using the aforementioned five variables. The concordance index was 0.877 (95% CI, 0.859–0.895) for the accuracy evaluation of the nomogram. Our results suggested that the 5-year cumulative incidence of NIH-defined cGVHD after haplo-cord-HSCT was 32.2%, and this nomogram may help clinicians select reasonable treatment strategies.
Introduction
Chronic graft-versus-host disease (cGVHD) remains a major cause of morbidity and nonrelapse mortality (NRM) after hematopoietic stem cell transplantation (HSCT) [1]. A large multicenter prospective study reports that cGVHD occurs in ∼50% of recipients defined by the National Institutes of Health (NIH) consensus criteria [2]. In recent years, the incidence of cGVHD is increasing despite advances in transplantation practices [3]. This has a significant impact on patients' quality of life stemming from active cGVHD itself and long-lasting immunosuppressive treatment [4]. Today, haploidentical donors have emerged as important alternative donor sources, especially in China [5,6]. Historically, the incidence of cGVHD in haploidentical HSCT (haplo-HSCT) is higher than that in human leukocyte antigen (HLA) matched HSCT [7,8]. Huang and colleagues [6] reported that the incidence of cGVHD 1 year after transplantation was 42% versus 15% for haploidentical donor versus HLA matched sibling donor transplant recipients, with the cumulative incidence rate of severe cGVHD after 1 year being 12% and 2%, respectively. Hence, strategies that can prevent this complication without compromising the beneficial graft versus tumor (GVT) effects are urgently needed.
Plenty of prospective studies aimed at reducing the incidence of cGVHD have been performed after haplo-HSCT. Early attempts to use T cell depletion and T cell replete of the grafts have been the milestone for haplo-HSCT to lower the risk of acute graft-versus-host disease (aGVHD) and cGVHD; however, those strategies were associated with graft failure, serious infections, and relapse [9,10]. Recently, the application of post-transplant cyclophosphamide (PT-Cy) by the Johns Hopkins group has improved the safety and efficacy of haplo-HSCT, and a report published by the Center for International Blood and Marrow Transplant Research (CIBMTR) showed that PT-Cy has emerged as an important alternative preventive strategy for cGVHD after haplo-HSCT [11]. Another study showed that the mesenchymal stem cells derived from the umbilical cord blood (UCB) could significantly reduce the 2-year cumulative incidence of cGVHD after haplo-HSCT (27.4% vs. 49.0%) [12].
Despite this, it is still necessary to explore more effective strategies to further decrease the incidence and severity of cGVHD among recipients who undergo haplo-HSCT. Previous studies demonstrated a low incidence of cGVHD following UCB transplantation compared with related and unrelated donor transplantation [13,14]. However, concerns still persist regarding graft failure, delayed engraftment, and delayed immune reconstitution [15]. We had attempted to combine the infusion of haploidentical stem sources supported by UCB from a third party (haplo-cord-HSCT) for transplantation as a novel approach to retain the GVT of the haploidentical donor and reduce the shortcomings of UCB, and our clinical practice had demonstrated encouraging outcomes, including reducing the incidence of cGVHD [16,17]. However, data fully describing the incidence, clinical manifestations, and outcomes of cGVHD following haplo-cord-HSCT are still lacking.
In this single-center prospective study, the clinical profiles of cGVHD according to the NIH criteria after haplo-cord-HSCT treatment protocol were characterized. In addition, for therapeutic trials or clinical use, a simple model and a nomogram of cGVHD prognosis were constructed. To our knowledge, this is the first report proposing a prognostic nomogram to predict the survival of patients with cGVHD.
Patients and Methods
Patient population
This open label, nonrandomized, single-arm prospective study included a serial group of 300 patients with hematological malignancies who underwent haplo-cord-HSCT between January 2012 and July 2016 at the Department of Hematology in the First Affiliated Hospital of Soochow University. Patients who were included into the study fulfilled all of the following criteria: the age of recipients ≤55 years; the first time HSCT; myeloablative conditioning regimen was adopted; haploidentical donor combined UCB transplantation was adopted due to no available HLA-matched siblings or HLA-matched unrelated donors; the Eastern Cooperative Oncology Group (ECOG) score of recipients was ≤2; and the expected survival after transplantation is more than 100 days. Exclusion criteria included the following: the age of recipient >55 years; reduced intensity conditioning regimen was adopted; recipients with nonmalignant hematologic disease; recipients who received HLA-matched siblings or HLA-matched unrelated donors HSCT; recipients who received anti-CD20 monoclonal antibody within 100 days after transplantation; the expected survival after transplantation is less than 100 days; an ECOG performance status >2; and the presence of uncontrolled infections and severe liver, renal, lung, and heart diseases. All patients were followed up, with a median follow-up of 26.4 months (range 0.2–61.8) from the initiation of transplantation. A cutoff date of July 31, 2017 was used for survival analysis. The follow-up clinical information was updated from the periodic outpatient records by referring physicians and generated using the clinical follow-up program in the department. The Ethics Committee of the First Affiliated Hospital of Soochow University approved this study (EUDRACT no.: 2015-117), and written informed consents were provided by the enrolled patients or their guardians (if patients were younger than 18 years old). The study was performed in accordance with the Declaration of Helsinki.
Transplantation procedures
The haploidentical donors were their parents, children, or siblings performed by HLA high-resolution techniques. All donors had received granulocyte colony-stimulating factor 5 mg/kg/day for five consecutive days before stem cell harvesting. If the counts of bone marrow CD34+ cells was <2 × 106/kg, peripheral blood stem cells were additionally collected. The UCB units came from the cord blood banks in China, and the criteria for UCB selection included the following: one unit, unit was HLA 4–5/6 matched with patient, at the same level of typing; the richest UCB units were chosen [18]. All recipients received modified busulfan/cyclophosphamide (BU/CY) as myeloablative conditioning regimen, which consisted of simustine 250 mg/m2 (Day −10), cytarabine (Ara-C) 4 g/m2/day (days −9 and −8), oral busulfan 4 mg/kg/day (days −7 to −5), and cyclophosphamide 1.8 g/m2/day (days −4 and −3). GVHD prophylaxis included rabbit antithymocyte globulin (ATG), cyclosporine A, short-course methotrexate (MTX), and mycophenolate mofetil (MMF).
Diagnosis, severity, and treatment of cGVHD
The clinical diagnosis and severity scoring of cGVHD syndromes were evaluated according to the NIH consensus conference [19,20] and the revised Seattle criteria [21]. The first-line treatment of cGVHD consisted of prednisone (1 mg/kg/day) given with or without a calcineurin inhibitor. The second-line treatment options included MMF, MTX, tacrolimus, sirolimus, imatinib, and rituximab [22]. The classification systems of a GVHD were graded according to the established consensus criteria [19,20].
Clinical definitions
Standard-risk diseases of hematological malignancies were defined as follows: acute leukemia in first (CR1) or second remission (CR2); chronic myeloid leukemia in the first chronic phase; myelodysplastic syndrome with <20% bone marrow blasts; and Hodgkin or non-Hodgkin lymphoma in first or second complete remission, partial remission, or stable disease. All others were defined as high-risk diseases [23]. Relapse was defined as the recurrence of malignancy after complete remission or any progression of malignant disease. NRM was defined as death in the absence of disease relapse or progression. Overall survival (OS) was defined as the time from the date of transplantation to death from any cause. Disease-free survival (DFS) was defined as the survival in a state of continuous complete remission after transplantation. GVHD-free, relapse-free survival (GRFS) includes grades III to IV aGVHD, cGVHD requiring systemic treatment, relapse, or death [24]. GVHD OS (GOS) was defined as the time from the day of aGVHD or cGVHD diagnosis to the day of the last follow-up or relapse or death. GVHD-specific survival (GSS) was defined as the time from the day of aGVHD or cGVHD diagnosis to the day of death due to GVHD-related complications, in the absence of relapse [25,26]. Steroid-refractory cGVHD (SR-cGVHD) was defined using the previous consensus [22].
Statistical analysis
Quantitative variables were expressed as median and range, qualitative variables were expressed as frequency and percentage, and differences between groups were compared using the chi-square test for categorical variables. Cumulative incidence estimates were used to summarize the probability of GVHD. The probability of developing cGVHD, grades II to IV aGVHD, relapse, and NRM was estimated to consider competing risks [27]. Competing events for aGVHD and cGVHD were death or relapse. NRM was estimated by considering relapse as a competing risk event and vice versa. The incidence of time-dependent outcomes was estimated using the Kaplan–Meier method and compared using a log-rank test. The tested variables included age, gender, primary disease, disease status before transplant, donor type, mononuclear cell dose, CD34+ cell dose, total body irradiation in conditioning regimen, numbers of cGVHD-involved organs, cGVHD response to initial therapy, global score by NIH criteria, bronchiolitis obliterans syndrome (BOS), cGVHD with liver involvement, platelet count at time of cGVHD onset, relapse, previous grades II to IV aGVHD, performance status at the cGVHD onset, Epstein–Barr virus, and cytomegalovirus status.
Logistic regression was used to identify factors associated with developing cGVHD. All tested variables met the assumptions for proportionality, and the final multivariate models were built using a forward stepwise model selection approach with 0.05 significance level. Cox proportional hazard regression was used to identify the risk factors associated with transplant outcomes. A nomogram was formulated based on the results of Cox analysis and using the package of rms26 in R version 3.4.1 (June 30, 2017) (
Results
Patient characteristics
Patients' median age was 25 years (range, 2–55); 187 (62.3%) were males and 113 (37.7%) females. The baseline features of patients, donor characteristics, and transplantation procedures are summarized in Table 1. During the process of engraftment, 254 patients had engraftment with haplograft, primary graft failure was found in 35 patients, and 11 cases showed stable engraftment of the cord blood unit or mixed engraftment. In this 300-patient group cohort, 23 patients died within 100 days after transplantation. In total, 190 patients survived, 93 patients died, and 17 patients were lost to follow-up before the cutoff date. The OS, DFS, GRFS, and NRM for all recipients are summarized in Supplementary Fig. S1 and Supplementary Table S1.
Patient and Transplantation Characteristics
aGVHD, acute graft-versus-host disease; ALL, acute lymphocytic leukemia; AML, acute myeloid leukemia; CML, chronic myeloid leukemia; CMV, cytomegalovirus; EBV, Epstein–Barr virus; HAL, hybrid acute leukemia; MDS, myelodysplastic syndrome; MNC, mononuclear cell; NHL, non-Hodgkin lymphoma; TBI, total body irradiation.
aGVHD incidence, severity, and survival
Furthermore, 113 (37.6%) of the recipients developed aGVHD; 90 (79.6%) recipients were classified with classic aGVHD and late-onset aGVHD, including persistent, recurrent, and de novo late aGVHD in 15 (65.2%), 2 (8.6%), and 6 (26%), respectively. The cumulative incidence of grades II to IV aGVHD on day 100 after transplantation was 36.7% (95% confidence interval [CI], 33.9–39.5) (Fig. 1A). The 2-year survival was 60.6% (95% CI, 55.2–66) in patients with classic aGVHD and was notably better in patients with persistent late aGVHD (37%; 95% CI, 24.1–49.9), de novo late aGVHD (33.3%; 95% CI, 14.1–52.5), and recurrent late aGVHD (0) (P = 0.05) (Fig. 1B).

cGVHD incidence, severity, and clinical characteristics
Overall, according to the NIH criteria, 73 (24.3%) patients developed cGVHD among the serial recipients before the cutoff day, and the median time of cGVHD onset was 6 months (range, 3–40) post-transplantation. The 1-, 3-, and 5-year cumulative incidence of cGVHD was 26.3% (95% CI, 23.5–29.1), 30.3% (95% CI, 27.3–33.3), and 32.2% (95% CI, 28.7–35.7), respectively (Fig. 1C). The 1- and 2-year cumulative incidence of moderate-to-severe cGVHD was 10.3% (95% CI, 8.4–12.2) and 11.4% (95% CI, 9.4–13.4) (Fig. 1C). In addition, 64 (87.7%) patients were classified as having classic cGVHD, and 9 (12.3%) patients were diagnosed with the overlap syndrome. Of the 73 patients with cGVHD, 17 patients with mild cGVHD were given topical glucocorticoids, 56 patients were treated with systemic immunosuppressive agents (first-line treatment), 35 (62.5%) patients with cGVHD had complete remission, while 21 (37.5%) patients received second-line treatments, including tacrolimus (n = 8), MMF (n = 6), imatinib (n = 2), ruxolitinib (n = 2), sirolimus (n = 1), MTX (n = 1), and rituximab (n = 1). Only 5 (23.8%) recipients discontinued immunosuppressive agents after 1 year at cGVHD diagnosis; however, 16 (76.2%) patients still received immunosuppressive therapy or died. Meanwhile, 89 patients were diagnosed with cGVHD using the Seattle criteria, with onset at a median of 5.7 months (range, 3.6–42) after haplo-cord-HSCT and reaching an estimated cumulative incidence of 35.1% (95% CI, 32–38.2) after 2 years (Fig. 1D). The cGVHD characteristics are shown in Table 2.
Characteristics of Chronic Graft-Versus-Host Disease Patients (n = 73)
cGVHD, chronic graft-versus-host disease; CNI, calcineurin inhibitor; NIH, National Institutes of Health.
Risk factors for developing cGVHD defined by the NIH criteria
The present study analyzed possible risk factors for the development of cGVHD after haplo-cord-HSCT, including patients, donor characteristics, and other clinical information regarding the transplant. The multivariate analysis revealed that standard-risk disease (odds ratio = 0.244; 95% CI, 0.072–0.83; P < 0.05) was the only significant risk factor for developing cGVHD in this study.
Clinical outcome of patients with cGVHD defined by the NIH criteria
For all 73 patients with cGVHD, the median survival time after cGVHD onset was 23.3 months (1–53.3); 53 patients survived, and 20 patients died during the follow-up period in the present study. The 1-, 2-, and 3-year GOS in the cGVHD group was 76.5% (95% CI, 71.6–81.5), 71.6% (95% CI, 66.2–77), and 67.6% (95% CI, 61.2–74), respectively. The GOS, GSS, and the cause of death in patients with cGVHD are shown in Fig. 2A and Supplementary Table S2. The 1- and 3-year GOS was shorter (66.7%; 95% CI, 51–82.4 and 35.6%; 95% CI, 17–54.2) in patients with overlap syndrome compared with those with classic cGVHD (78.2%; 95% CI, 73–83.4 and 74.4%; 95% CI, 68.8–80) (P = 0.055) (Fig. 2B).

Independent risk/protective factors and prognostic nomogram for GOS
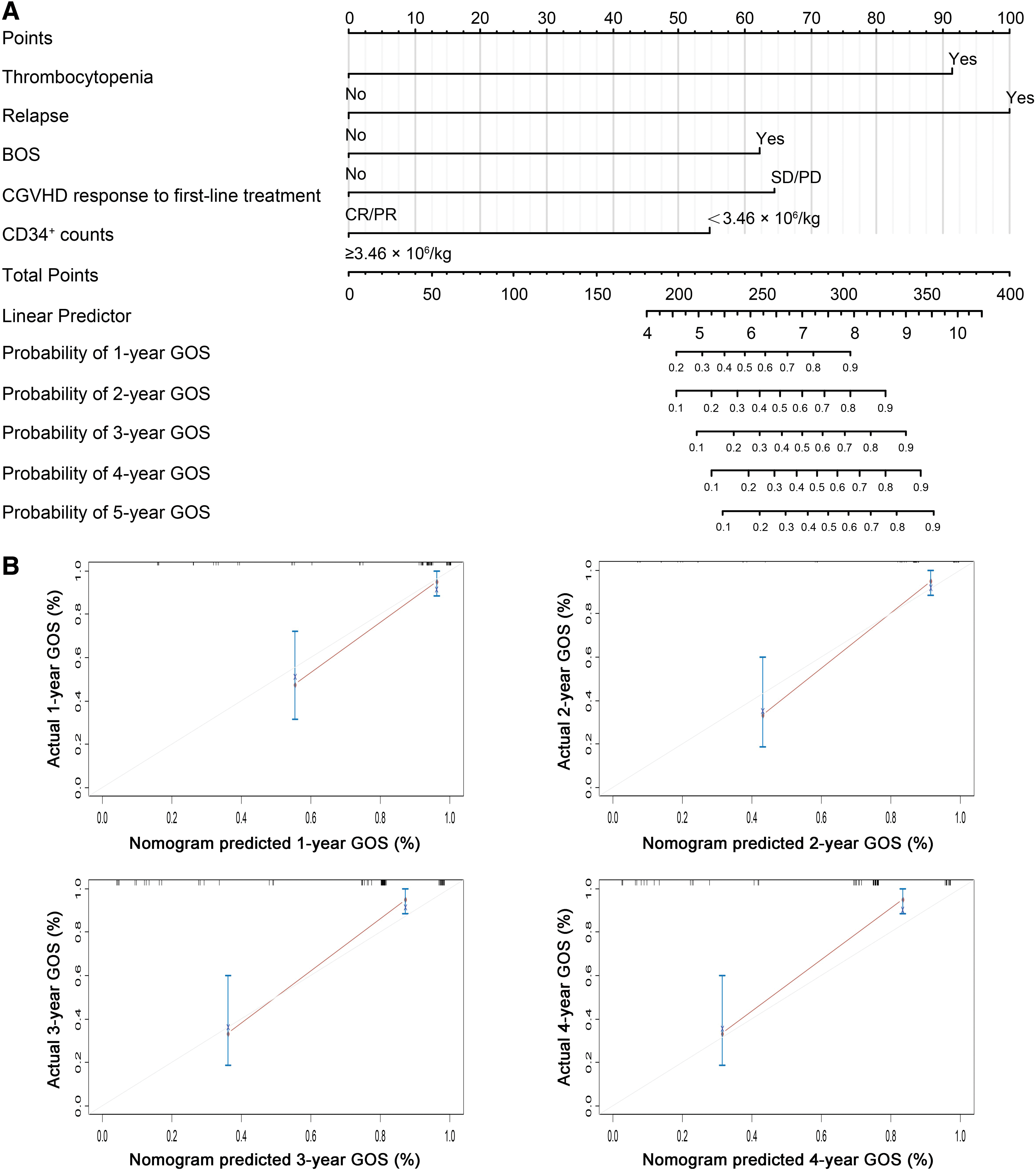
The results of univariate and multivariate analyses associated with survival after the development of cGVHD diagnosed by NIH criteria are shown in Table 3. The multivariate analysis demonstrated that the relapse of hematological malignancies (hazard ratio [HR] 17.89; 95% CI, 2.79–114.67; P < 0.05), BOS (HR 10.93; 95% CI, 2.43–49.16; P < 0.05), thrombocytopenia (HR 13.23; 95% CI, 2.99–58.55; P < 0.05), and failure of first-line treatment for cGVHD (HR 5.25; 95% CI, 1.48–18.71; P < 0.05) were mortality factors associated with GOS. In contrast, CD34+ count in graft source ≥3.46 × 106/kg was a protective factor for GOS (HR 0.178; 95% CI, 0.05–0.62; P < 0.05). A nomogram was developed to predict GOS using the five independent covariates identified in the final Cox model (Fig. 3A). The C-index for GOS prediction was 0.877 (95% CI, 0.859–0.895), and the calibration curve illustrated the predictions from the nomogram compared with actual outcomes for the 73 recipients with cGVHD (Fig. 3B).
Cox Multivariable Model of Factors Predicting Survival for Patients with Chronic Graft-Versus-Host Disease (n = 73)
BOS, bronchiolitis obliterans syndrome.
Discussion
Despite advances in donor selection, conditioning programs, and GVHD prophylaxis, cGVHD remains a major cause for treatment failure, often severely affecting long-term survivors after HSCT [30]. Unfortunately, the pathogenesis behind the syndrome remains elusive. Therefore, strategies for preventing cGVHD are urgently needed [31]. In our center, the haplo-cord-HSCT protocol that infusion of haploidentical graft primed by granulocyte colony-stimulating factor supported with UCB from unrelated donors under myeloablative conditioning regimens prepared with ATG is adopted. Our previous studies showed that the 1-year incidence of cGVHD following haplo-cord-HSCT was lower compared with not supported with UCB haplo-HSCT (19.3% vs. 48%) based on Seattle criteria [16,32]. Our another study also demonstrated that the cumulative incidence of cGVHD during the follow-up period was 22% and 34% for haplo-cord-HSCT and HLA matched sibling donor based on Seattle criteria, respectively, although the difference was not statistically significant [17].
In the present study, more patients were enrolled, and the NIH and Seattle criteria were both used prospectively to evaluate the cumulative incidence of cGVHD in a cohort of 300 patients with hematological malignancies who received haplo-cord-HSCT. On the one hand, this study showed that the 2-year cumulative incidence of cGVHD evaluated by Seattle criteria was lower compared with not supported with UCB haplo-HSCT (35.1% vs. 48%) [32]. In the present study, the 2-year cumulative incidence rates of cGVHD and extensive cGVHD diagnosed by Seattle criteria (35.1% and 21.4%) after haploidentical donor transplantation were lower than Peking protocol (53% and 23%) [33]. On the other hand, according to the NIH criteria, the 1-year cumulative incidence of cGVHD was lower compared with other centers of haploidentical transplant recipients (26.3% vs. 34%) [34]. In particular, the 1-year cumulative incidence of moderate to severe cGVHD (10.3%) was lower than those of other groups (15%–31%) [34 –36]. Besides, our analysis also revealed that the 2-year cumulative incidence of NIH-defined cGVHD (35.1%) was even lower than those of transplantation from HLA matched unrelated and sibling donors (53% and 47%) [2]. The understanding of the mechanisms underlying the involvement of the cord in cGVHD prophylaxis is quite limited, although several studies have demonstrated the unique tolerogenic properties of the fetal lymphoid system and the immunomodulatory effects of cellular components in the UCB [37,38]. Whether the cord has a functional role in preventing cGVHD is inconclusive. A well-designed randomized controlled trial should be conducted to determine whether the cord is beneficial in cGVHD prophylaxis and investigate its underlying mechanism.
Currently, cGVHD prognostic scoring systems should be investigated and focused on for future biomarker and clinical research. However, in most previous studies, cGVHD was not diagnosed or staged based on the NIH consensus criteria [39]. Furthermore, those cGVHD prognosis risk score systems should be used as a reference, but may not be very suitable for the population in China due to different transplantation procedures and ethnic diversity. In this prospective study, we analyzed survival after cGVHD based on local data to better guide cGVHD efforts in China. In the present study, the multivariate analysis identified five variables associated with cGVHD survival: relapse, platelet count, BOS, SR-cGVHD, and CD34+ cell dose. Over the past few decades, nomogram has been suggested as a clinically representative tool for calculating the probability of specific outcomes or other clinical events for individuals [40]. It facilitates discussion between physicians and patients using a graphic representation based on a statistical model, and hence, nomograms have emerged as a simpler, yet more advanced, method. To our knowledge, no nomogram with all the prognostic factors for cGVHD survival has been published so far. The present study proposed to develop a nomogram that could be used for risk assessment to predict the survival in patients with cGVHD using data from the Cox regression analysis. Each prognostic factor used to create the nomogram was given a score. By adding up these scores, a total score was obtained. Subsequently, a straight line down from the total point scale was used to estimate the 1–4-year survival for each transplant recipient. The discriminative ability and predictive accuracy of the nomogram were evaluated using the C-index and calibration curves. The C-index of the nomogram was 0.88 (95% CI, 0.80–0.96), and the calibration curve showed an optimal agreement between prediction and actual observation. Therefore, this novel nomogram could identify patients with cGVHD who were considered to have a worse prognosis based on the current standards. Prognosis stratification using this nomogram would be informative and helpful in clinical decision-making. However, the model and nomogram were established based on the data obtained from a single institution in China. Studies with other cohorts from different Chinese institutes and countries would help validate our model. At present, another cohort of patients with cGVHD is being enrolled to validate this model, and the results will be presented in future publications.
The present study had several limitations. First, the results were based on a single-center, nonrandomized noncontrolled study. Hence, randomized controlled studies are required to validate the findings. Second, all patients with cGVHD were diagnosed by experienced physicians, suggesting a diagnostic bias. In addition, several potentially important variables, such as HLA disparity, donor special antibody, and noninherited maternal antigen, could not be analyzed due to insufficient clinical information. Finally, several clinical outcomes such as immune reconstitution, quality of life, immunosuppression discontinuation, and assessment of Lee cGVHD symptom scale in cGVHD populations should be investigated in our future studies.
In summary, the results suggested that the 5-year cumulative incidence of NIH defined-cGVHD after haplo-cord-HSCT was 32.2% for hematological malignancies. Relapse, thrombocytopenia, BOS, and SR-cGVHD were independent risk factors for GOS, whereas CD34+ ≥3.46 × 106/kg was a protective factor affecting GOS in our study. In addition, a prognostic model and nomogram were proposed to predict the outcomes for recipients with cGVHD after haplo-cord-HSCT, which might be useful for clinicians and in future clinical research.
Footnotes
Acknowledgments
This work was supported by a grant from the National Natural Science Foundation of China (grant no. 81470296), Jiangsu Province Medical Youth Talent Program (grant no. QNRC2016719), and a C class sponsored project from Jiangsu provincial Six Talent Peaks (grant no. 2016-WSN-123). Gusu Key Medical Talent Program (grant no. GSWS2019007). Jiangsu Province “333” project (grant no. BRA2018391). The authors are grateful to Jing-jing Deng for the support given for the development of statistical analysis.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.