
Abstract
This study included data from 81 consecutively enrolled patients with hematological diseases who had been treated with unrelated umbilical cord blood transplantation (UCBT) between September 2014 and April 2019. All patients received intense conditioning regimens with combined fludarabine and high-dose cyclophosphamide (FC) before undergoing UCBT. Sixty-seven patients received a single UCBT, and 14 patients received a double UCBT. Fifty patients were pretreated with the fludarabine, busulfan, and cyclophosphamide (FBC) protocol, while 31 patients were treated with FC before transplantation. Graft-versus-host disease (GVHD) was prevented with cyclosporine A and mycophenolate mofetil administration. According to low-resolution, human leukocyte antigen (HLA) donor–recipient matching at six sites, 53 patients had 5–6 matches, while 28 patients had 4 matches. Seventy-eight patients (96.3%) achieved complete engraftment in this study. Thirty-six patients developed acute GVHD (aGVHD). The cumulative incidence of grade I–II aGVHD at day 100 posthematopoietic stem cell transplantation was 29.6%, and the cumulative incidence of grade III–IV aGVHD was 14.8%. At the end of the follow-up, 12 patients died due to treatment-related complications, and 4 died of disease relapse after transplantation. The transplant-related deaths were due to transplant-related infection (8 of 81), GVHD (2 of 81), and organ toxicity (2 of 81). The probability of overall survival (OS) was 80.2%. A higher dose of cyclophosphamide combined with fludarabine conditioning in UCBT was an effective curative method for treatment of hematologic disorders and could enhance the engraftment of umbilical cord blood stem cells, promote post-transplant immune reconstitution, and improve OS.
Introduction
Allogeneic hematopoietic stem cell transplantation (Allo-HSCT) has been successfully used to treat malignant hematopoietic diseases, hereditary immunodeficiency, and metabolic disorders [1]. Because of the single-birth policy in China, there are limited sibling donor resources, which is a significant problem. In the absence of such donors, transplantation of hematopoietic stem cells from an unrelated volunteer donor or unrelated umbilical cord blood (UCB) is a potential alternative. Transplantation of unrelated donor bone marrow can be complicated by human leukocyte antigen (HLA) matching requirements, severe acute and chronic graft-versus-host disease (GVHD), and opportunistic infection [2]. In recent years, the use of UCB as an alternative source of transplantable hemopoietic stem cells has steadily increased [3 –6]. However, compared with conventional bone marrow and peripheral blood cell grafts, UCB contains significantly fewer CD34+ cells and mature lymphocytes. In addition, a traditionally weak conditioning regimen is used in UCB transplantation (UCBT). These properties could be responsible for the increased risk of late hematopoietic recovery kinetics and for the increased risk of graft failure [7,8]. Thus, new strategies aim to improve engraftment and reduce transplantation related mortality (TRM). In this study, we adopted a new conditioning regimen that combines a high dose of cyclophosphamide with fludarabine (FC) to improve engraftment and increase overall survival (OS).
Materials and Methods
Patients
In accordance with the Declaration of Helsinki, all patients consented to the use of their medical information for this research before entering the study. The Southeast University Ethics Committees approved the study and required participants to sign a written, informed consent form. All authors and participants or, in the case of children, their parents or legal guardians consented to the publication of this article, and participants were required to sign a written, informed consent form. From September 2014 to April 2019, 81 consecutive hematology patients undergoing unrelated UCBT in our research center were approved by the institutional review board of the Hematological Institute of Southeast University and were required to sign a written informed consent to participate. Patients were eligible for unrelated UCBT if HLA-compatible peripheral blood and bone marrow stem cell donors were not available. Eighty-one recipients of unrelated donor UCBT were considered for potential matches. Patient diagnoses included acute myeloid leukemia (n = 25), acute lymphoblastic leukemia (n = 18), myelodysplastic syndrome (n = 7), severe aplastic anemia (n = 19), immunodeficiency disorders (n = 8), and inborn metabolic errors (n = 4). All of the blood malignancy patients included in this study had one or more of the following risk factors: (1) acute leukemia in CR1 with a high risk of relapse (with a genetic indicator of poor prognosis or complex chromosomal abnormalities), (2) acute leukemia in CR2 or CR3, or (3) acute leukemia in relapse and unable to achieve remission. Sixty-seven single UCBT and 14 double UCBT procedures were performed. Patients were followed until the end of the study evaluation period in May 2019. Characteristics of the patients and donors are displayed in Table 1.
Characteristics of Patients, According to Umbilical Cord Blood Transplantation
AA, aplastic anemia; ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; FBC, fludarabine, busulfan, cyclophosphamide; FC, combined fludarabine and high-dose cyclophosphamide; HLA, human leukocyte antigen.
Cord blood selection
UCB was selected according to the number of nucleated cells (NCs), the number of CD34+ cells, and the degree of HLA matching. A single dose of cord blood met the following requirements: HLA match of >4/6 loci between donors and recipients, NCs >3.5 × 107/kg of recipient body weight, and CD34+ cells ≥2.5 × 105/kg of recipient body weight; HLA match of >5/6 loci between donors and recipients, NCs >3.0 × 107/kg of recipient body weight, and CD34+ cells ≥1.7 × 105/kg of recipient body weight; and HLA match of 6/6 loci between donors and recipients, NCs >2.5 × 107/kg of recipient body weight, and CD34+ cells ≥1.2 × 105/kg of recipient body weight. If the number of cells was lower than that described above, two or more cord blood donors were selected from the cord blood bank. Allele-level typing for HLA-A, HLA-B, and HLA-DRB1 was available for the 81 cord blood recipients, among whom 21 were HLA matched and 60 were HLA mismatched with one (n = 32) or two (n = 28) antigens.
Conditioning regimens and GVHD prophylaxis
All malignant hematological patients received a non-TBI, high-dose conditioning regimen. The conditioning regimen consisted of daily intravenous administration of 2 g/m2 cytarabine for 2 days, followed by 30 mg/m2 fludarabine for 6 days, with 0.8 mg/kg busulfan administered intravenously every 6 h for a total of 12 doses. Cyclophosphamide (60 mg/kg/day) was administered intravenously for 3 days following the completion of busulfan treatment, followed by semustine (MeCCNU, 250 mg/m2) in a single oral dose. Nonmalignant hematological patients received 30 mg/m2 fludarabine for 6 days with cyclophosphamide (60 mg/kg/day) administered intravenously for 3 days. Patients received 4 mg/kg antithymocyte globulin (ATG Fresenius AG, Oberurse, Germany) intravenously every day for two consecutive days (Fig. 1). All patients received 5 μg/kg granulocyte colony-stimulating factor daily from day 7 after transplantation until neutrophil engraftment. GVHD prophylaxis for UCBT consisted of cyclosporine A (CSA) continuously for 24 h and an intravenous infusion from 1 day before transplantation to day 28 post-transplantation. Thereafter, the patient was switched to oral CSA (5 mg/kg, twice per day) to maintain blood CSA concentrations between 200 and 400 ng/mL. A 0.5-g dose of mycophenolate mofetil (MMF) was given every 12 h orally from 1 day before transplantation to day 30 post-transplantation.

Different conditioning regimens between malignant hematological patients and nonmalignant hematological patients in UCBT.
Supportive care and infection prophylaxis
All patients were hospitalized in rooms with high-efficiency air filters and received oral trimethoprim–sulfamethoxazole to prevent Pneumocystis carinii. Ganciclovir (two doses of 5 mg/kg per day, intravenously) was administered for prevention of cytomegalovirus infection from day 7 before transplantation to day 2 before transplantation [9,10]. Additionally, 10 mg/kg/day acyclovir was given from one day before transplantation until day 30 after transplantation to prevent herpes virus infection. Itraconazole was administered intravenously to patients with mycotic infections [11]. Prostaglandin E1 (0.2 μg/kg/day, twice daily) was administered intravenously for prophylaxis against hepatic veno-occlusive disease. Patients received transfusions when platelet levels were below 20,000/μL or hemoglobin levels decreased to 60 g/L during hospitalization; all blood products were irradiated and leukocyte depleted.
Evaluation of engraftment
Engraftment was defined as achievement of an absolute neutrophil count >0.5 × 109/L for three consecutive days, while platelet recovery was defined as an absolute platelet count >20 × 109/L without the support of transfusions for seven continuous days. Bone marrow morphological examination was performed in the first, second, and third months after transplantation. DNA fingerprinting (short tandem repeat polymorphisms), sex chromosome analysis, and ABO blood typing were also performed to confirm donor engraftment.
Lymphocyte immune reconstitution studies
We collected patient bone marrow samples into 2–3 mL of EDTA-K2 anticoagulant and analyzed CD3+ lymphocytes, CD4+ lymphocytes, CD8+ lymphocytes, CD19+ lymphocytes, and CD16+/CD56+ natural killer (NK) cellular expression levels using flow cytometry (fluorescence-activated cell-sorting Vantage cytometers; BD Biosciences). The analysis of lymphocyte recovery was performed at the following five time points: pretransplant and 3, 6, 9, and 12 months after transplantation.
Statistical analysis
The major study endpoints were neutrophil and platelet engraftment, acute GVHD (aGVHD; grades I–IV), chronic GVHD (cGVHD), TRM, relapse, and survival. The cumulative incidence of acute and cGVHD was also calculated by treating deaths from other causes as competing risks. Patient and donor characteristics and transplantation-related variables were analyzed using the chi-square test. Continuous variables were described as the mean ± SD, with the median range in parentheses. The probability of leukemia-free survival was calculated by the Kaplan–Meier method [12], with statistical comparisons completed using the log-rank test and Cox regression for multiple regression analysis [13]. Independent variables with P > 0.1 were sequentially excluded from the model, and P < 0.05 was considered statistically significant. All values were two-tailed. For the analysis of leukemia-free survival, relapse and death were regarded as events, and data of living patients and patients in continuous remission were censored at the last follow-up. Statistical analysis was performed with SPSS (version 11.5).
Results
Patient characteristics
UCB patient demographics matched for age, diagnosis, disease risk, and transplant conditioning regimens are shown in Table 1. There were no significant differences in recipient age, weight, or malignant hematologic disease versus nonmalignant disease characteristics. All malignant hematologic disease recipients received a myeloablative conditioning regimen. In patients receiving cord blood grafts, the total NC dose standard was based on HLA disparity; the cell dose was no less than 3 × 107/kg in single-antigen-mismatched grafts and no less than 3.5 × 107/kg in two-antigen-mismatched grafts.
Hematopoietic recovery and engraftment
Among the 81 patients, 78 (96.3%) were successfully engrafted (two aplastic anemia patients and one leukemia patient failed engraftment), and no patient experienced a second graft failure. The median time to reach a neutrophil engraftment count of 0.5 × 109/L was 17 days (ranging from 13 to 30 days), and the median time to reach a platelet engraftment count of 20 × 109/L was 28 days (ranging from 14 to 90 days).
aGVHD and cGVHD
Twenty-four patients developed aGVHD. The cumulative incidence of grade I–II aGVHD at day 100 post-HSCT was 29.6%, while that of grade III–IV was 14.8% (grades I–II in 24 patients, and grades III–IV in 12 patients). Two patients died from severe aGVHD, and nine patients developed cGVHD (one in nine patients had extensive cGVHD involving more than two organs/systems). The cumulative incidence of cGVHD was 11.1%. There was a trend toward fewer cases of cGVHD than aGVHD in UCB recipients (Fig. 2).
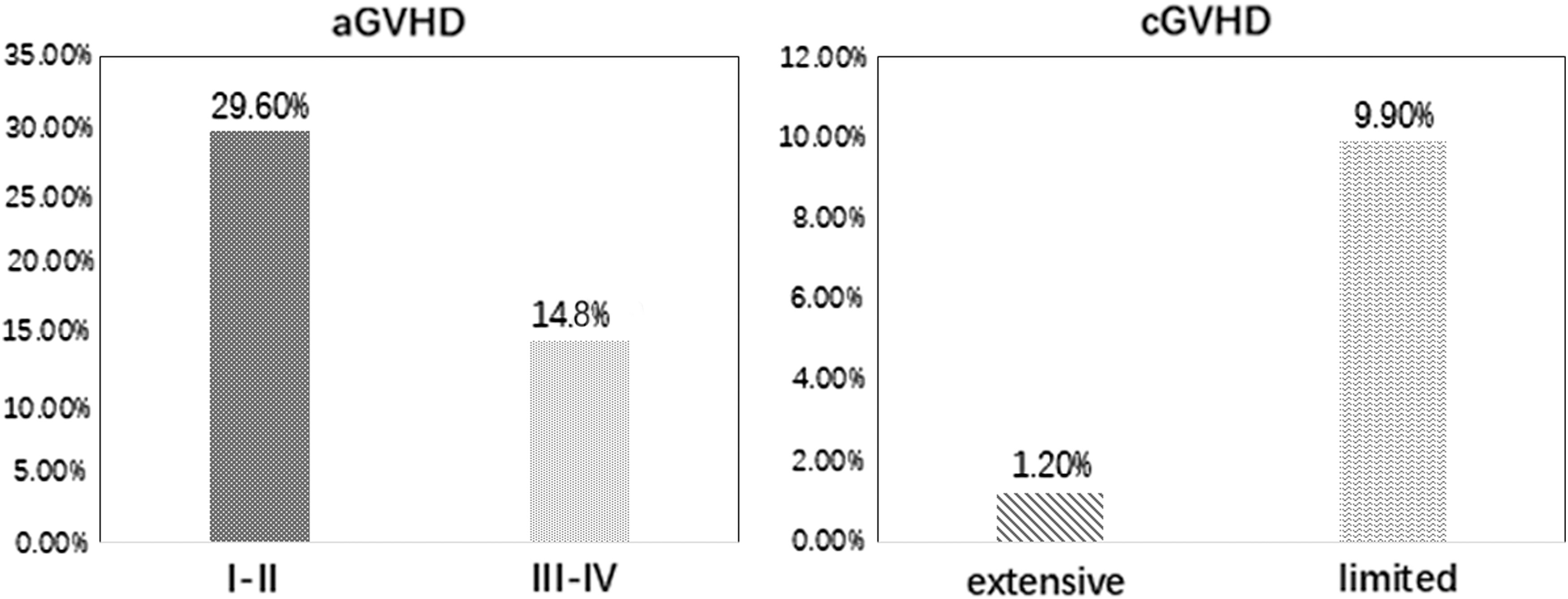
Cumulative incidence of aGVHD and cGVHD after UCBT. aGVHD, acute GVHD; cGVHD, chronic GVHD; GVHD, graft-versus-host disease.
Opportunistic infections
There were 23 cases of opportunistic infections in the patients during the follow-up period. There were 10 cases of bacterial pneumonia, 5 cases of invasive aspergillosis, 1 case affecting the central nervous system, 2 cases affecting the oral mucosa, 3 cases of catheter-related infections, and 2 cases of fever and unclear foci.
Analysis of prognostic factors
There were some differences between the two groups in terms of their pretreatment characteristics, so we analyzed the association of those characteristics with survival (Table 2). Those factors included age, gender, disease type, disease status at transplantation, disease duration, CD34+ cells, HLA disparity (0–1 vs. 2), donor–recipient sex matching, and conditioning regimens. The univariate analysis indicated that age, disease type, disease status, conditioning regimen, CD34+ cells, and disease duration influenced OS. Gender, HLA disparity (0–1 vs. 2), and donor–recipient sex were not identified as risk factors for OS. A multivariable analysis indicated that the most independent predictors of OS were age, active disease, disease type, and CD34+ cells, with hazard ratios of 2.97, 3.63, 2.31, and 3.15, respectively (Table 2).
Analysis of Factors Predicting Overall Survival After Umbilical Cord Blood Transplantation
Multivariable analysis, factors with at least borderline statistical significance in the univariant analysis (P < 0.1) were included in a Cox proportional hazard model; multivariate analysis (P < 0.05) reaching statistical significance.
HR, hazard ratio with 95% confidence intervals; n, number; OS, overall survival rate at 4 years.
Lymphocyte reconstitution in all patients
A decline in CD4+ and CDl9+ lymphocytes was obvious after initiation of treatment. CD4+ lymphocytes decreased from 1 month post-transplant to the lowest level in 2 months. CD19+ lymphocyte transplantation decreased to the lowest level in 2 months post-transplant. CD19+ lymphocyte transplantation decreased to the lowest level in 3 months after transplantation. In all patients, CD4+ lymphocytes recovered to near normal levels within a mean of 11 months after transplantation; these lymphocytes returned to normal levels within a mean of 10 to 12 months post-transplant. After transplantation, CDl9+ cells required a mean of 12 to 14 months before the counts reached normal levels. In contrast, CD8+ cell counts reached normal levels within 5 to 7 months after transplantation. We analyzed five lymphocyte subsets, namely CD3+, CD4+, CD8+, and CD19+ lymphocytes and CD16+/CD56+ (NK) cells; there was no statistically significant difference in the recovery of baseline levels or the time to lymphocyte reconstitution between the UCBT and PBSCT groups (in our previous study) [14] (Fig. 3).

The outcome of reconstitution of six lymphocyte subsets in the recovery of baseline levels of time.
Relapse and survival
By April 2019, with a median follow-up of 24 months (ranging from 3 to 55 months), 65 patients survived and 16 died. Twelve patients died from treatment-related complications, and 4 died from disease relapse after transplantation; 8 of 81 transplant-related deaths were due to transplant-related infection, 2 of 81 were due to GVHD, and 2 of 81 were due to organ toxicity. The Kaplan–Meier curve was used to estimate OS and disease-free survival in patients according to the disease subsets. The differences among the two groups were significant (P < 0.05) (Fig. 4).

Kaplan–Meier curve estimate of OS and DFS in patients according to the disease subset.
Discussion
For many years, Allo-HSCT has been limited by 3 major complications: engraftment failure, severe GVHD, and delayed immune reconstitution [15 –17]. UCB contains a limited number of NCs and the immunogenicity of UCB was weak; UCB also carries a higher risk of graft failure, and hematopoietic and immune reconstruction can be delayed. Retrospective UCBT data indicate that the overall frequency of graft failure was independently associated with the number of HLA mismatches and the number of NCs [18 –20]. The cord blood stem cell number, defects in the host BM microenvironment, and recipient immune response are considered major factors for engraftment failure. Graft failure can also be caused by nonmyeloablative conditioning regimens, T cell depletion from the graft, and so on. In this study, among the 81 patients, there were 3 cases of graft failure, leading to a graft failure rate of 3.7%. The reason for our low graft failure rate may be related to the intense patient conditioning regimens. We had increased the total cyclophosphamide dose to 180 mg/kg, although patients did not show increased renal toxicity or transplant-related mortality. Many factors affect immune reconstitution after transplantation, including recipient age, the source of stem cells, disease type, disease status and HLA disparity, the occurrence of GVHD, the conditioning regimen, and post-transplant immune suppression programs [21,22]. In our study, we developed a new conditioning regimen that combined fludarabine and a high dose of cyclophosphamide and could significantly improve engraftment and immune reconstitution compared with previous regimens [23].
The incidence of pre-engraftment syndrome (PES) after UCBT is higher than that after sibling or unrelated donor transplantation. PES is considered corticosteroid responsive. Factors implicated in development of PES include various conditioning types, GVHD prophylaxis, and the number of stem cells. Common features include noninfectious fever, vascular leak more than 1 week before engraftment, rash, and diarrhea. A 1-mg/kg/day starting dose of methylprednisolone is usually sufficient to counteract these features. In this study, we found that the 100-day cumulative incidence of grade I–II or grade III–IV aGVHD was significantly lower in cord blood transplantation than in sibling or unrelated donor transplantation (in our previous study) [24]. We were able to decrease the incidence of aGVHD through the combination of CSA and methylprednisolone, as well as with the addition of MMF as prophylaxis against GVHD.
However, we found that the cumulative incidence of relapse is one important cause of death after Allo-HSCT. In our study, six patients relapsed after UCBT, of whom two had not achieved complete remission before transplantation; one patient had a bone marrow relapse 64 days after transplantation. After the withdrawal of all immunosuppressive agents, fever, rash, and diarrhea were observed. After 2 weeks, the proportion of the recipient's chimeric X and Y chromosomes was consistent with the donor type. In another case (in a child), 38% of cells were leukemia cells before transplantation and that patient achieved complete remission after transplantation. A second relapse occurred 86 days after transplantation, after the patient had stopped taking all immunosuppressive agents. At that point, the patient was given interferon-α treatment. After 1 week, the patient showed severe aGVHD and large exfoliative dermatitis; after interferon-α withdrawal, the patient still survived. This group of patients confirmed that UCB stem cells have potent graft-versus-leukemia effects and that the relapse rate is low after transplantation.
In conclusion, our results show that a high-dose, FC conditioning regimen can be used to effectively treat malignant and nonmalignant hematologic diseases. This new conditioning regimen could significantly improve engraftment, prevent infection and GVHD, and promote OS. For nonmalignant hematological diseases and bone marrow failure, the UCB graft rate is relatively low. We used a new conditioning regimen to not only improve the total antileukemic effect but also to affect the hematopoietic microenvironment in the marrow. We chose fully HLA-matched cord blood and showed that higher CD34+ and UCB stem cell numbers can improve the likelihood of engraftment and OS. We acknowledge that our study involved a limited number of patients with different diseases treated at a single transplantation institution, so some potential bias may have existed in the selection of patients. Therefore, a larger, multicenter prospective trial is required to confirm our findings and to assess the long-term benefits of our intensive, FC conditioning approach.
Footnotes
Acknowledgments
The authors thank the three transplantation institution staff members, nurse practitioners, and nurses at the Hematopoietic Cell Transplantation Department for their dedication and excellent patient care.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The design and performance of this study were supported by the Key Department of Jiangsu Medicine (2016-12).