
Abstract
Retinitis pigmentosa (RP) is a hereditary retinal degeneration disease with no effective therapeutic approaches. Inflammatory and immune disorders are thought to play an important role in the pathogenesis of RP. Human umbilical cord mesenchymal stem cells (UCMSCs), with multiple biological functions such as anti-inflammation and immunoregulation, have been applied in different systemic diseases. We conducted a phase I/II clinical trial aiming to evaluate the safety and efficacy of intravenous administration of UCMSCs in advanced RP patients. All 32 subjects were intravenously infused with one dose of 108 UCMSCs and were followed up for 12 months. No serious local or systemic adverse effects occurred in the whole follow-up. Most patients improved their best corrected visual acuity (BCVA) in the first 3 months. The proportions of patients with improved or maintained BCVA were 96.9%, 95.3%, 93.8%, 95.4%, 90.6%, and 90.6% at the 1st, 2nd, 3rd, 6th, 9th, and 12th month follow-up, respectively. Most of the patients (81.3%) maintained or improved their visual acuities for 12 months. The average NEI VFQ-25 questionnaire scores were significantly improved at the third month (P < 0.05). The average visual field sensitivity and flash visual evoked potential showed no significant difference (P = 0.185, P = 0.711). Our results indicated that the intravenous infusion of UCMSCs was safe for advanced RP patients. Most of the patients improved or maintained their visual functions in a long term. The life qualities were improved significantly in the first 3 months, suggesting that the intravenous infusion of UCMSCs may be a promising therapeutic approach for advanced RP patients.
Introduction
Retinitis pigmentosa (RP) is a progressive, hereditary dystrophic eye disease that is mainly characterized by night blindness and progressive vision loss, with an estimated worldwide prevalence of 1/3,000–1/7,000 [1]. The typical characteristics of RP are degeneration and loss of the photoreceptors and retinal pigment epithelium (RPE), atrophy of the optic nerve, and impairment of the inner retina [2,3]. Currently, there are no effective therapeutic approaches for RP. In the past decades, various therapeutic strategies, such as gene therapy [4 –6], usage of neurotrophic factors, and visual prosthesis devices [7,8], have been explored for RP. But few therapeutic effects have been reported with the implementation of these approaches. In recent years, the adenoviral vector-based RPE65 gene therapy has demonstrated well tolerability and beneficial effects in Leber congenital amaurosis patients and has been in commercial use, which is an encouraging advancement in the treatment of RP [9 –12]. The pathological mechanisms of RP are thought to be the progressive apoptosis of photoreceptors mainly due to the primary genetic defects of photoreceptors or secondary to genetic defects of retinal pigmental epitheliums [13,14]. However, some recent studies reported that inflammatory and immune processes play an important role in the progression of RP [15 –17], which are new areas to explore for treatments for RP.
As a major kind of mesenchymal stem cells (MSCs), umbilical cord mesenchymal stem cells (UCMSCs) have many beneficial properties, such as anti-inflammation, immune regulation, proliferation, differentiation, low immunogenicity, and neurotrophy [18 –21]. The intravenous infusion of UCMSCs has been applied in the treatment of different systemic diseases, and different levels of improvement have been achieved [22 –24]. Intraocular transplantation of MSCs by an invasive approach has been attempted in animal models of RP and RP patients [25 –27], but the effectiveness was limited and complications still occurred. Recently, a local administration of UCMSCs by sub-Tenon's capsule injection has shown significant advantages in improving the visual function of RP patients, which confirms the visual restoring potential of UCMSCs [28]. The intravenous infusion of MSCs, a noninvasive method of administration, has been proven to be effective in some animal models of retinal disease [29 –32], but it has not been applied in RP patients.
In our previous study, intravenous infusion of UCMSCs was found to improve the retinal impairments of patients with diabetic retinopathy, suggesting that the anti-inflammatory effect of UCMSCs may affect this process [33]. Given the natural course of exponential decline in visual field, electroretinogram (ERG), and visual acuity in RP patients [3,34 –37], we conducted this single-arm clinical trial to determine whether the intravenous administration of UCMSCs can help improve or maintain the visual function of RP patients, and here we report the results.
Materials and Methods
Study design
This is a prospective, open label, single arm, phase I/II clinical trial that was conducted from April 2014 to December 2017. This study was approved by the Medical Ethics Committee of Southwest Hospital at the Army Medical University. All subjects received a single intravenous infusion of 1 × 108 UCMSCs and were followed up for 12 months. Systemic and ophthalmological examinations were performed to assess the safety and efficacy (Fig. 1). The study adhered to the principles of the Declaration of Helsinki and the International Ethical Guidelines for Biomedical Research Involving Human Subjects and was registered in the Chinese Clinical Trial Registry (Primary Registry of the International Clinical Trials Registry Platform of the World Health Organization) (ChiCTR-ONC-16008839). Every patient recruited for the study signed a written informed consent form.
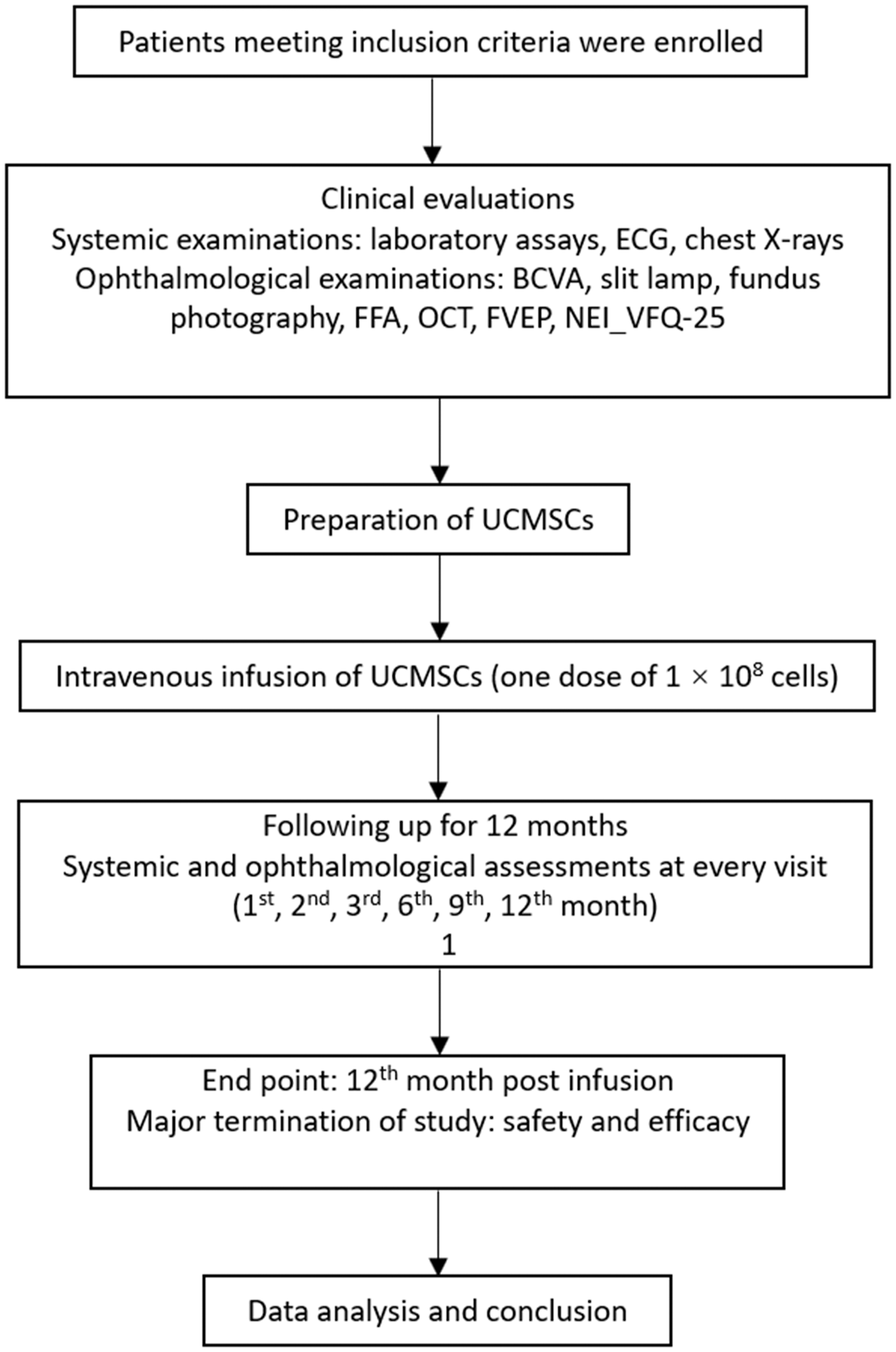
Study flow chart of UCMSC intravenous infusion. UCMSC, umbilical cord mesenchymal stem cell.
UCMSC preparation
Umbilical cord-derived MSCs for this study were derived from neonatal umbilical cord tissue according to the standard protocol and met the criteria approved by the International Society for Cellular Therapy [38 –41]. UCMSCs were isolated from umbilical cord tissues donated by consented mothers after full-term healthy births. All six donors were screened for inherited and infectious diseases beforehand. Cell preparation was performed by the Biotherapy Centre of the Army Medical University. Briefly, the Wharton's Jelly tissue was aseptically cut into a homogenate of 2–3 mm3 tissue blocks, which were seeded into T75 flasks in Mesenchymal Stem Cell Basal Medium (DAKEWE, Beijing, China) supplemented with 5% UltraGRO™ (HPCFDCRL50, Helios). The tissue blocks were cultured at 37°C, 5% CO2 for about 10 days for UCMSCs to reach confluence. Then cells were digested with 0.125% Trypsin and passaged at 1:3 ratio. Each enzymatic digestion step was considered to be a passage. Cells at P3-P5 were used for infusion. All infused UCMSCs were prepared based on the criteria approved by the International Society for Cellular Therapy. The final products met all of the following criteria: the number of cells in each batch was no fewer than 1 × 108; cell viability was no less than 95%; the cells were sterile; the cells did not have endotoxins, mycoplasma, hepatitis B, hepatitis C, or syphilis; and the cells had the appropriate surface marker expression (the positive rate of CD34 and CD45 was less than 0.5%, positive rate of CD29 was more than 90.5%, positive rate of CD90 was more than 92.3%, positive rate of CD105 was more than 95.1%, and positive rate of CD71 was more than 94.7%). The cell differentiation ability and nontumorigenesis were also tested to ensure that achieved UCMSCs meet the standard (Supplementary Figs. S1, S2, S3).
Patient screening
The inclusion criteria were as follows: Patients aged 18–65 (including 18 and 65) who had signed informed consent. Patients who voluntarily selected UCMSC transplantation for the treatment of advanced RP. Patients whose visual acuity of one or both eyes met the legal standard for blindness or low vision, that is, the best corrected visual acuity (BCVA) of the better eye was <0.3 (or the BCVA was <55 letters using the Early Treatment Diabetic Retinopathy Study [ETDRS] visual acuity checklist at a distance of 4 m) or the radius of the visual field was <10 degrees. Patients who had the ability to adhere to the study follow-up and protocol requirements.
The exclusion criteria were as follows:
Patients with any active intraocular inflammation, infection, or concomitant diseases in their eyes that may affect the interpretation of the results of the study or may lead to visual impairment, including severe cataracts, glaucoma, retinal vascular obstruction, retinal detachments, macular holes, vitreous macular traction, and choroidal neovascularization.
Patients with a history of intraocular surgery.
Patients with a stroke, coronary heart disease, renal insufficiency requiring dialysis or kidney transplantation, or other systemic chronic diseases.
Patients with anaphylactic reactions to sodium fluorescein.
Patients with hypertension (systolic pressure >140 mmHg or diastolic pressure >90 mmHg) or diabetes that cannot be controlled by drugs.
Females who planned to become pregnant within the next 6 months, were pregnant, or were lactating.
UCMSC intravenous infusion
The vital signs of all patients involved in this study, including their temperature, respiration rate, pulse, blood pressure, oxygen saturation, electrocardiogram signals, and pain severity, were continuously monitored before, during, and up to 2 h after infusion. The patients underwent treatment only when all their vital signs were normal. First, every patient received 5 mg of dexamethasone sodium phosphate in an injection and then received a sequential intravenous infusion of UCMSCs (1 × 108 cells, 250 mL per person) through the dorsal hand vein within 60 min. During transplantation, the infusion was stopped immediately and treated in a timely manner when immune rejection, anaphylaxis, and infusion reactions, such as headache, dizziness, nausea, and vomiting, occurred.
Clinical evaluation
Safety and efficacy parameters were evaluated at baseline and 1, 2, 3, 6, 9, and 12 months after the intravenous infusion of UCMSCs. The systemic examinations included a chest X-ray, an ECG evaluation, and a measurement of the relevant blood biochemical index. BCVA was used as the visual acuity evaluation standard and was determined by the ETDRS alphabet. Fundus photography, fundus fluorescein angiography (FFA), and visual field tests were performed at every follow-up. Optical computed tomography (OCT) scans were performed to evaluate the average thickness of the macula. Three concentric circles were made with the fovea as the center, with diameters of 1,000, 3,000, and 6,000 μm. Two perpendicular lines were used to divide the whole macula into nine regions, and the average thickness of the nine regions represented the central macular thickness. The flash visual evoked potential (FVEP) was tested according to the standardized procedures developed by the International Society for Clinical Electrophysiology of Vision (ISCEV). The latent time and amplitude of the P2 wave were analyzed. The NEI_VFQ-25 visual quality questionnaire was administered at baseline and at 3, 6, and 12 months after the administration of the UCMSCs.
Statistical analysis
SPSS18.0 software was used to describe and analyze the data. The measurement data that had a normal distribution were expressed as the mean ± standard deviation (
Results
Intravenous infusion of UCMSCs showed no significant adverse effects
In total, 32 patients (64 eyes), including 20 males and 12 females, aged between 19 and 61 with an average age of 36 ± 2.45 years, were enrolled in the study. All patients were diagnosed with advanced RP, and the follow-up period for the patients enrolled in this study was 12 months (Supplementary Table S1 in supplementary data). The vital signs of all patients were stable during and after the infusion of UCMSCs. No severe adverse effects, such as fever, infection, allergic reactions, immune rejections, and systemic or local inflammation, occurred during the follow-up period. The blood assay results, such as the complete blood count and liver and renal function test results, were normal throughout the whole follow-up period (Supplementary Table S2 in supplementary data), and the chest X-ray examination and electrocardiogram signals were normal 30 days after transplantation (Supplementary Table S3 in supplementary data). No immune rejection (Supplementary Table S4) or tumorigenesis was observed, and no significant abnormal fluorescence leakage was found, as shown in FFA throughout the whole follow-up period (Fig. 2, Supplementary Fig. S4).

Fundus photography and FFA before and after UCMSC infusion.
Analysis of the thickness of the macula
The thickness of the macula was measured using OCT. The average macular thickness was stable after the UCMSC infusion (Fig. 3A). Compared to the baseline level before treatment, the average thickness increased at the 9th month after transplantation and then returned to the baseline afterward (Fig. 3B, 3C). However, this change was not statistically significant (P = 0.543).
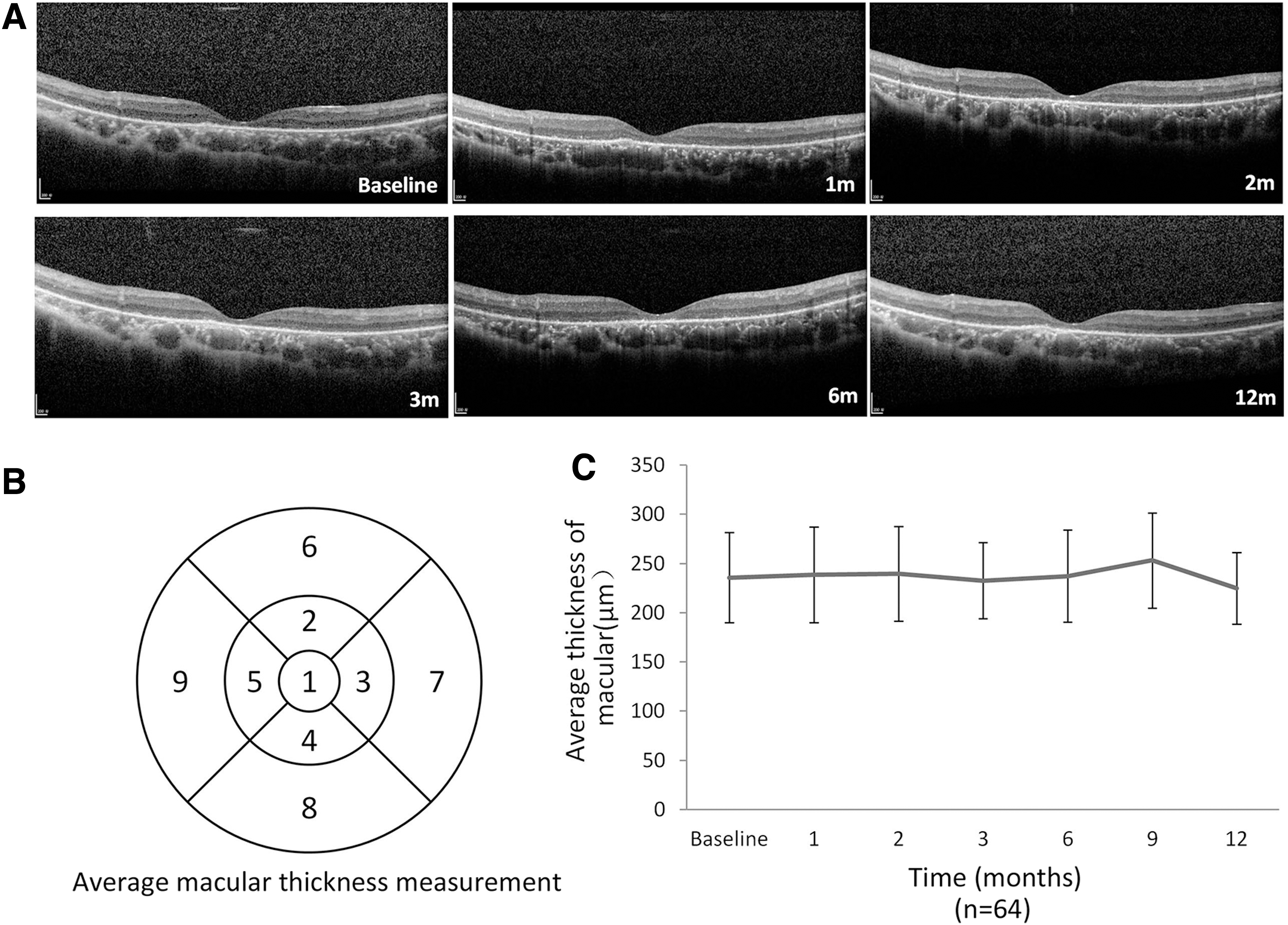
OCT examination before and after UCMSC infusion.
Visual function and life quality were maintained and partially improved
Visual acuity was tested with the Early Treatment Diabetic Retinopathy Study (ETDRS) chart and was determined to be improved (increased by 5 or more letters), maintained (changed by fewer than 5 letters), and lost (decrease by 5 or more letters). The proportions of patients with improved BCVA were 32.8%, 35.9%, 39.1%, 18.8%, 17.2%, and 17.2% at the 1st, 2nd, 3rd, 6th, 9th, and 12th month, respectively, after the UCMSC infusion. Correspondingly, the percentage of patients with maintained visual acuity was 64.1%, 59.4%, 54.7%, 76.6%, 73.4%, and 73.4%, respectively, and the percentage of patients with lost visual acuity was 3.1%, 4.7%, 6.3%, 4.76%, 9.4%, and 9.4%, respectively (Fig. 4A).

The efficacy of the UCMSC infusion in RP patients.
If the treatment is considered effective for patients with improved or maintained visual acuities, then the treatment was considered effective for 96.9%, 95.3%, 93.8%, 95.4%, 90.6%, and 90.6% of the patients at the 1st, 2nd, 3rd, 6th, 9th, and 12th month follow-up, respectively, and the treatment continued to be effective for 81.3% of the patients for 12 months after the infusion, for 3.1% of the patients for 9 months, for 6.3% of the patients for 6 months, for 3.1% of the patients for 3 months, and for 1.6% of the patients for 1 month. A total of 4.7% of the patients demonstrated a loss of visual acuity at the first visit after the infusion (Fig. 4B).
The average BCVA was also calculated to statistically analyze the change in visual acuity. There was a trend showing that the average BCVA increased gradually for 3 months after the infusion and then declined gradually but remained higher than the baseline value at the 12th month follow-up. The difference was not statistically significant (P = 0.236, Fig. 5A). Data of the average visual field sensitivity showed a fluctuating rising trend after treatment, but there was no statistical significance (P = 0.185, Fig. 5B). To assess the overall change in electrophysiological function, the FVEP was tested at each follow-up time point. The average amplitude/latency ratio (A/L) of the P2 wave showed no significant difference at each follow-up (P = 0.711, Fig. 5C) (Supplementary Fig. S5).
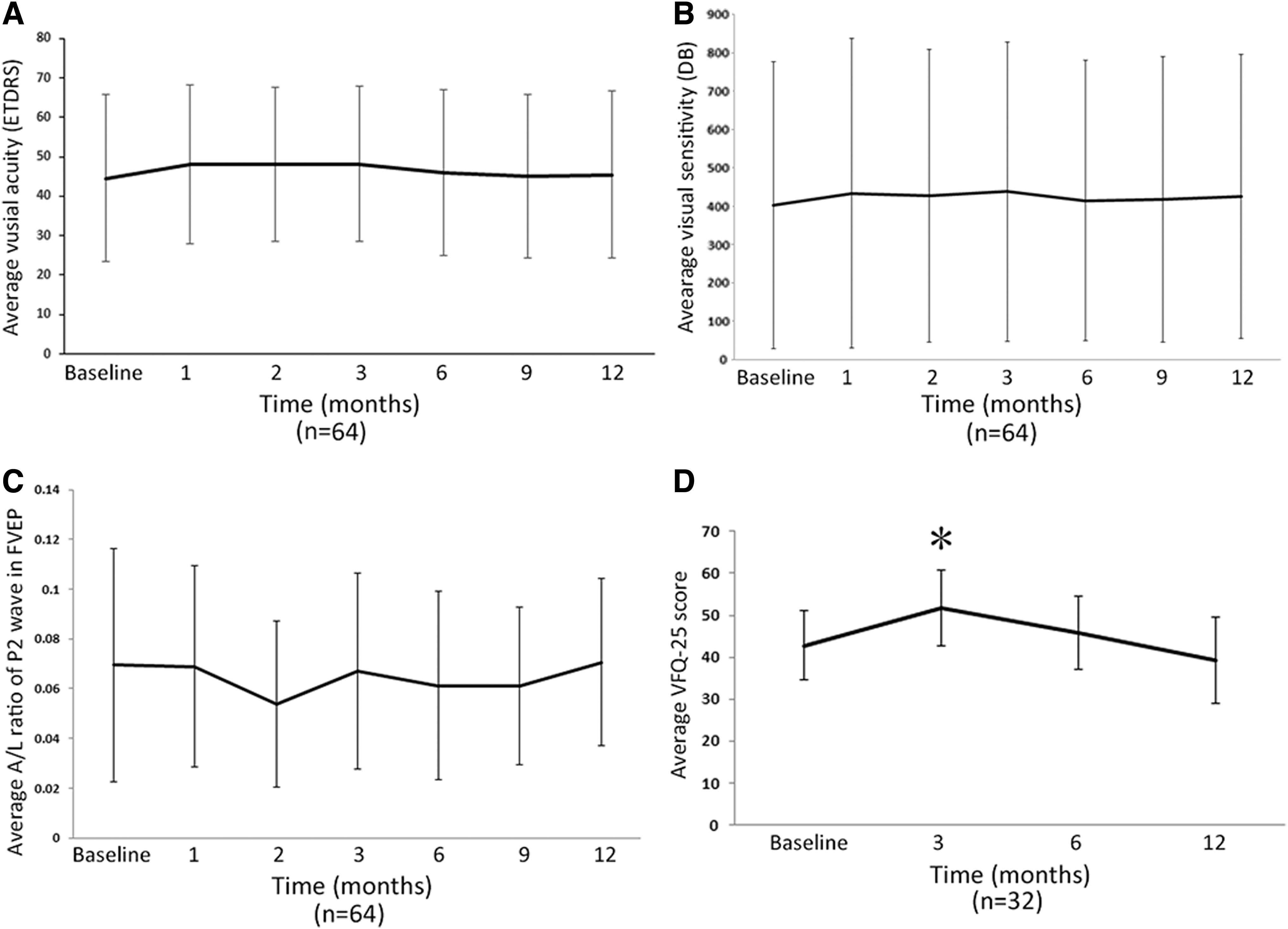
Changes in visual function and quality of life after the UCMSC infusion.
All patients completed the NEI-VFQ-25 questionnaire, which reflects the quality of life among visually impaired people. The average score of NEI_VFQ-25 improved significantly at the 3-month follow-up (P < 0.05, Fig. 5D) and then gradually returned to the baseline value, which indicated that an improvement in quality of life occurred at 3 months after the infusion.
Discussion
Patients with advanced RP have severely impaired central visual acuity or visual fields. Due to the inherited nature and irreversible damage of the RPE and photoreceptors, there are no effective treatments for RP. MSCs, with properties such as immune regulation, anti-inflammation, cell migration and differentiation, and paracrine and neurotropic effects, have been applied in a variety of systemic diseases [42]. Compared with other MSCs, UCMSCs have some additional advantages, such as low immunogenicity and strong migration ability; they are easy to collect, and they are associated with fewer ethical problems.
In some animal models of retinal degenerative diseases, the intravenous administration of UCMSCs has been proven to be effective in improving visual function [29 –32], but the underlying mechanism remains controversial since UCMSCs are considered incapable of penetrating the blood–retinal barrier (BRB). However, when retinal impairment occurs, such as inflammation, ischemia, and hypoxia, the retinal vascular endothelial cells are damaged, and the tight junctions of the cells are destroyed, which may increase the permeability of BRB [43,44]. RP is virtually an inflammatory disease, where chronic inflammation and immune reactions are involved and play an important role in the pathological mechanisms [15 –17]. So, anti-inflammation and immune regulation may be new therapeutic strategies for RP patients. In addition, the breakdown of BRB in the progression of RP makes it possible that infused UCMSCs can reach the impaired retinal tissue. Although some studies found that the majority of the infused cells accumulated in the lungs and liver and were rapidly eliminated [45], this noninvasive method of UCMSC transplantation is still potentially applicable given their wide range of biological functions.
Intravenous infusion of UCMSCs has been reported by some clinical trials to be effective for the treatment of neural, cardiac, pulmonary, and osteoarticular disorders [22 –24,46]. Recently, some clinical trials attempted to transplant MSCs into RP patients' eyes by intravitreal injection or subretinal injection [25,27,47]. The efficacy of these approaches remains controversial, and a variety of complications have been reported because of invasive treatment approaches. To the best of our knowledge, no clinical trials have been performed using UCMSCs to treat RP patients through an intravenous infusion.
In our study, the patients tolerated the UCMSC infusion well, and no severe adverse effects were observed during the follow-up period after transplantation, which is consistent with the results of previous reports. Moreover, neither tumorigenesis nor local/systemic immune rejections occurred. The average thickness of the macula did not change significantly, suggesting that no macular edema or inflammatory reaction occurred during the follow-up period.
In advanced RP patients, visual function is significantly impaired, resulting in seriously decreased visual acuity and visual field defects. Since the ERG waves are extinguished for most of the patients, the change of amplitude of ERG can't be accurately detected. Therefore, a sensitive index reflecting visual functional change is difficult to acquire. To evaluate the effect of the UCMSC infusion on RP patients, the variation in the number of ETDRS letters was analyzed. We found that there were more patients gaining ETDRS letters in the first 3 months after the infusion, indicating that the UCMSC infusion may improve visual function more effectively in this period, which provides evidence for the timing of a repeat treatment. If the treatment is considered effective for patients gaining or maintaining numbers of ETDRS letters, then the effectiveness of the UCMSC infusion can last for 12 months for most patients (81.3%), implying that the intravenous infusion of UCMSCs can improve or maintain the visual function of RP patients in the long term.
However, there were no significant differences found in the average number of ETDRS letters, in visual field sensitivity, or in FVEP change between all the follow-ups, which indicate that the effectiveness of UCMSC infusions is still limited. In contrast, as a progressive inherited disease, the natural course of RP has been revealed in early studies [34 –37]. It turns out the visual function (especially visual field and ERG) of RP patients declines in an exponential manner. So, the nonstatistical difference in this study also implies that the overall visual acuities and visual fields were maintained after treatment. What's more, the nonsignificant change of FVEP suggests that the visual function on a central nervous level may have been kept.
The National Eye Institute Visual Function Questionnaire-25 (NEI VFQ-25) is a widely employed test used to evaluate the general well-being of patients with diseases associated with vision loss [48]. It has been reported that the NEI VFQ-25 is useful in assessing the vision-related quality of life of patients with glaucoma, cataracts, age-related macular degeneration, and retinal pigmentosa as well [49 –52]. The assessment of vision-related quality of life of RP patients is thought to be particularly important in understanding the progression of retinal pathologies [53]. In our study, the average score of the NEI VFQ-25 was significantly increased (P < 0.05) at the third month after treatment, indicating a dramatic improvement in the quality of life at that time, which confirmed the trend of BCVA improvement after the infusion and further implied the time-dependent feature of the effect of the UCMSC infusion.
In this study, intravenous infusion of UCMSCs showed a relatively short duration of therapeutic effect, namely the first 3 months. We assume it is because infused UCMSCs gradually diminished their functional properties such as proliferation, differentiation, and immune and inflammatory modulation over time. How to maintain a long-term efficiency is still a concern of further study. Although repeated treatment is an option, modifying the biological features of UCMSCs or developing superior alternative cells are more promising approaches. As a kind of primary MSCs, UCMSCs together with bone marrow-derived MSCs and adipose-derived MSCs still have some limitations, including limited proliferative capacity, alterations in phenotype and differentiation potential after long-term culture, standardization difficulty, and decreased therapeutic efficacy during expansion [54,55]. MSCs induced from pluripotent stem cells (PSCs), such as embryonic stem cells and induced PSCs (iPSCs), have the advantages of infinite growth and differentiation and have been used as an alternative to primary MSCs in recent years [54,56]. Particularly, iPSCs can be obtained from almost any adult somatic tissues and have minimal ethical controversy. iPSC-derived MSCs (iMSCs) can exhibit all MSC properties and are more advantageous in terms of expansion, life span, differentiation, immune modulation, and so on [57,58]. At the same time, iMSCs can be rapidly scaled up without losing their functional properties, and even have been characterized as rejuvenated MSCs [59,60]. It may be promising applicating iMSCs in the treatment of RP in future.
Lack of placebo-controlled or double-blinded grouping makes our results still limited. However, an open label clinical trial study is advantageous for comparing changes between homogeneous groups before and after treatment. It is also suitable for long-term effectiveness study and extension study for participants especially when repeated treatment is needed. Nonetheless, to obtain more unbiased results, randomized controlled trials with independent adverse effect monitoring are still needed in future to further confirm our results.
In conclusion, the intravenous infusion of UCMSCs is a promising, low-risk, and relatively economical therapeutic method of treating advanced RP patients. Visual function was improved or remained consistent over a relatively long period of time for a large proportion of patients. Moreover, we assume that the most effective time period for the UCMSC infusion is the first 3 months after the intravenous infusion. Thus, a repeated infusion might be applied accordingly or even customized based on the patient's previous response.
Footnotes
Acknowledgment
The authors thank the Biotherapy Centre of the Army Medical University for the support of cell preparation.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
This work was supported by the National Basic Research Program of China (2013CB967002, to Prof. Zheng Qin Yin), Southwest Hospital Key Program (SWH2016ZDCX1001, to Prof. Zheng Qin Yin), the Military Key Program (BWS13C015), and the National Key Research Program (2016YFC1101103, to Dr. Yong Liu).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.