
Abstract
Diabetic foot ulcer (DFU) is a multifactorial complication of diabetes, mainly manifested as infection, ulcer, or destruction of deep tissue, and there is currently no effective treatment. Several preclinical and clinical studies have proved that the transplantation of mesenchymal stem cells (MSCs) improved wound healing. In this study, we evaluated the therapeutic efficacy of human umbilical cord (hUC-MSCs) in DFU rat model. One dose of hUC-MSCs (1 × 106 cells) was subcutaneously injected around wounds in male Sprague-Dawley rats. Wound healing was evaluated macroscopically (wound closure) every 3 days. In addition, we measured growth factors and specific proteins [matrix metalloproteinases (MMPs)-9 and MMP-8] on Day 14 post hUC-MSC transplantation. Results showed significant differences in the wound healing kinetics of lesions that received hUC-MSCs compared to lesions that received vehicle (phosphate buffered saline; P < 0.05). Enzyme-linked immunosorbent assay analyses indicated that MMP-9 protein contents were significantly upregulated in DFU animals, while MMP-8 was downregulated compared to the diabetic rats (P < 0.05). After MSC treatment, the level of MMP-9 and MMP-8 decreased and increased compared to the vehicle group, respectively. These findings suggest that hUC-MSC transplantation can ameliorate the healing process of DFU rats and a potential mechanism through which MSCs enhance DFU wound healing by decreasing MMP-9 expression and increasing MMP-8 expression. This study represents a promising opportunity to gain insight into how MSCs mediate wound healing.
Introduction
Diabetic foot (DF) is a common chronic complication of diabetes. Diabetic foot ulcers (DFUs) have become the main cause of chronic intractable wounds [1], and it is easy to cause noninjury lower limb amputation, which is very harmful [2]. DFUs are in a state of long-term chronic low-grade inflammation, and the special pathophysiological abnormalities in the high glycemic environment, including vascular problems and inhibition of epithelial regeneration, lead to the failure of treatment with a single approach to DFUs [3]. Therefore, there is an urgent need to develop the latest comprehensive treatment strategies to improve the healing of DFUs.
In recent years, the cell-based treatment of DFUs has developed rapidly and become a research hotspot [4]. Stem cell therapy, as a strategy for the treatment of DFUs, has shown safe and effective effects in both preclinical and clinical trials [5]. Studies have confirmed that the soluble mediators and paracrine factors released by mesenchymal stem cells (MSCs) can regulate immune response, promote angiogenesis and stimulate cell differentiation, and play a key role in wound healing [6,7]. Nevertheless, the underlying specific mechanisms of the therapeutic effects of MSCs remain unclear.
Matrix metalloproteinases (MMPs) play an important role in both the pathology and repair of DFUs. In particular, MMP-9 is overexpressed in chronic diabetic ulcers [8]. Recent studies have shown that MMP-9 is not conducive to wound healing, while MMP-8 plays a beneficial role in healing wounds [9]. However, whether the function of MSCs in the treatment of DFUs is related to the regulation of MMP-9 and MMP-8 levels and the exact molecular mechanism is still unclear.
Human umbilical cord mesenchymal stem cells (hUC-MSCs) have many advantages, such as abundant sources, no influence on the donor, convenient sampling, low immunogenicity, and no ethical obstacles [10,11]. In this study, we attempted to investigate the effect of hUC-MSC transplantation on DFU wound healing using a rat model and to explore the potential mechanism of the therapeutic effects of MSCs, aiming to provide more evidence for the repair of injures by MSCs.
Materials and Methods
Animal model establishment
Male Sprague-Dawley rats weighing 180–220 g were purchased from Beijing Vital River Laboratory Animal Technology Co., Ltd. The rats were housed in polycarbonate cages (three animals per cage) with corncob bedding and were given standard rodent food and water. All animal studies were conducted in accordance with the guidance of the Animal Care and Use Ethics Committee of Capital Medical University.
Intraperitoneal injection of streptozotocin (60 mg/kg; Sigma) was given to establish a diabetes model; the blood glucose higher than 16.7 mmol/L for at least 2 consecutive days was considered to be successful. We set diabetic rat model group as the control group (DM group). Foot wound surgery was performed on diabetic animals to establish DFU models. Anesthesia for ulcer surgery used isoflurane inhalation. Rinse the skin on the back of the right hind foot with 75% ethanol and make a 5 × 10 mm full-thickness excision wound with a scalpel. Take digital photos on the day of surgery (day 0) and every 2 or 3 days thereafter. On the 14th day after the wound was formed, the skin of the wound area was collected by rapid freezing with liquid nitrogen and fixed in 4% paraformaldehyde (PFA). They were embedded in paraffin for hematoxylin and eosin (HE) staining and immunohistochemical analysis and then frozen to −80°C for western blot and enzyme-linked immunosorbent assay (ELISA) analysis.
Isolation and expansion of hUC-MSCs
The schemes detailed below follow the regulations of the National Health Commission on stem cell research and have been ethically approved by the Ethics Committee of Beijing Luhe Hospital affiliated to Capital Medical University. The methods for isolation and subculture of hUC-MSCs follow the previously published protocols. First, the obtained umbilical cord was washed with phosphate buffered saline (PBS) at 4°C and cut into small pieces of 1–2 cm. Then, the umbilical artery and vein were removed (Fig. 1A), and Wharton's jelly was carefully separated. Finally, they were cut into small pieces with sharp scissors and a scalpel and inoculated into a 10 cm Petri dish. Alpha modified eagle medium (α-MEM) medium supplemented with 10% fetal bovine serum, penicillin (100 U/mL), and streptomycin (100 μg/mL) were used. Incubate the cells in a carbon dioxide incubator at 37°C until they reach confluence. Continue the same procedure from passage (P) 3–6 in both media.

Morphology and immunophenotyping of hUC-MSCs.
Flow cytometry tests the characterization of hUC-MSCs
The isolated hUC-MSCs were characterized by specific cell surface markers. Evaluation was performed by flow cytometry using a variety of antibodies such as CD45 (PE labeled), CD73 (APC labeled), CD90 (FITC labeled), and CD105 (PerCP-cy5.5 labeled) (BD Biosciences). An appropriate isotype control was selected to exclude nonspecific fluorescence. The cells at P3 were harvested and fixed with 4% PFA for 30 min at room temperature. They were then washed with PBS containing 0.5% bovine serum albumin and incubated with specific antibodies in PBS for 1 hour on ice. After incubation, the cells are washed and resuspended in 500 μL of PBS. Then we transferred them to the flow-type test tubes and tested on the BD FACSCanto II. Finally, we used FlowJo software to analyze the data.
hUC-MSC transplantation
Twenty SD rats with DFUs on the right hind foot were divided into two groups: DFU-Vehicle (treated with PBS) and DFU-MSCs group. On the day of surgery (day 0), 1 × 106 hUC-MSCs were injected with 200 μL of PBS solution at multiple points around the DFUs using an insulin syringe. In the same manner, an equal amount of PBS (200 μL) was transplanted to the ulcer site. Animals were sacrificed on the 14th day after cell transplantation, and specimens were obtained for relevant tests.
Enzyme-linked immunosorbent assay
Plasma levels of VEGF, NO, and NOS were detected by ELISA according to the manufacturer's instructions. We manually grind the skin samples of DFUs collected from experimental animals in liquid nitrogen to obtain tissue homogenates. The homogenate was centrifuged at 5000 × g for 5 min. Remove the supernatant and measure it immediately. The amount of MMP-9 and MMP-8 in cell supernatant or plasma was quantitatively determined using MMP-9 and MMP-8 ELISA Kit (SAB, College Park, MD, USA.). They were normalized to the total protein concentration as determined by bicinchoninic acid (BCA) assay. The measurement procedure followed the instructions recommended by the manufacturer. All samples were analyzed in duplicate and compared with the standard internal curve of each experiment.
Histological evaluation
The tissue fixed by 4% PFA was embedded in paraffin, sliced (5 μm), and dewaxed to water. HE staining was performed to observe the formation of granulation tissue on the wound surface of each group, and the rate of reepithelialization was evaluated by comparing the thickness of the tissue. Immunohistochemical staining was performed. Antibody working solution prepared according to the dilution ratio in the instructions was added to the ulcer tissue sections. Sections were incubated with the monoclonal antibody against VEGF GB14165 and anti-MMP-9 mAb GB12132 (Wuhan Servicebio Technology Co., Ltd., Wuhan, Hubei, China) at 1:100 dilution. After overnight incubation at 4°C, the secondary antibody (goat anti mouse antibody, G1214, Wuhan Servicebio Technology Co., Ltd.) was added for 1 h of incubation at 37°C, and tissues were washed with PBS buffer before DAB development (DAB Chromogenic Kit, G1212, Wuhan Servicebio Technology Co., Ltd.) observation of chromogenic degree under a microscope.
According to the histology scoring system for murine cutaneous wounds of Mari van de Vyver et al. [12], we used six indexes (reepithelialization, epithelial thickness index, keratinization, granulation tissue, scar elevation index, remodeling) to evaluate the two groups of DF-vehicle and DF-MSCs. The t-test was used to detect differences between the two groups. Animals were scored for the HE staining at 14 days after surgery.
Western blot analysis
The frozen rat foot skin tissues were ground into powder under liquid nitrogen, and then tissue lysis buffer phenylmethanesulfonylfluoride (PMSF) (1 mmol/L, Sigma Aldrich) was added. The total protein was extracted by centrifugation at 12,000 g at 4°C for 20 min. The protein concentration was determined by BCA method, and the protein concentration was adjusted to make each group consistent. The same amount of samples was loaded, sodium dodecyl sulfate-polyacrylamide gel electrophoresis was performed, and the protein was electrically transferred to polyvinylidene fluoride membrane. After blocking, primary antibody and secondary antibody were applied in turn, and enhanced chemiluminescence (ECL) reagent was added, and then exposed with Bio-Rad ECL imaging system. The expression of MMP9 and VEGF in skin tissue was detected.
Results
Characterization of hUC-MSCs
The hUC-MSCs were grown from the edge of tissue explants (Fig. 1B) and created a homogenous monolayer of adherent spindle-shaped cells at passage 2–3 ( × 40) (Fig. 1C). The immunophenotypes of hUC-MSCs were analyzed by flow cytometry. The results showed that hUC-MSCs were positive for CD73 (95.7%), CD90 (99.3%), and CD105 (99.5%) and were negative for hematopoietic marker CD45 (2.8%) (Fig. 1D).
DFU in diabetic rats was ameliorated with the hUC-MSC transplantation
Time elapsed to wound closure was defined as the time in which the wound bed became completely reepithelialized and filled with new tissue. The wounds of the hUC-MSC transplanted group were closed after 14 days. Wound healing and representative images of the wounds are shown in Fig. 2A.

Effects of hUC-MSCs on wound healing in rats DFU and wound closure analysis.
As shown in Fig. 2B, the percentage of wound healing in the DFU-MSCs group was higher than the DFU-Vehicle group at day 5, 7, 10, and 14, respectively (P < 0.05). Wound closure started to be noticed after 3 days for the hUC-MSC treated rats and became more evident after 10 days compared to the other group.
hUC-MSC transplantation altered MMP-9 and MMP-8 levels
The expression levels of VEGF, NO, and NOS were upregulated in the hUC-MSCs group in comparison to the DFU-Vehicle and DM control group. But there was no statistical difference (Supplementary Fig. S1). We found that hUC-MSCs decreased MMP-9 levels compared to DFU-Vehicle group and increased the total MMP-8 levels (Fig. 3). The level of MMP-9 in the DFU-Vehicle group was significantly higher than that in the diabetic group, while the DFU-MSCs group significantly dropped to the level of that in the diabetic group. The level of MMP-8 in the DFU-Vehicle group was significantly lower than that in the diabetic group, while the DFU-MSCs group significantly rose above the level of that in the diabetic group (P < 0.05).

ELISA measurement of the expression of MMP-9 and MMP-8 from the wound tissue. MMP-9 and MMP-8 protein expression levels were altered with MSCs treatment. Mean ± S.D., n = 6 mice per group, *P < 0.05 by one-way ANOVA. ELISA, enzyme-linked immunosorbent assay; MMP, matrix metalloproteinase; S.D., standard deviation.
Figure 4A–C shows the representative images of HE staining of animal wound tissues in each group. HE staining showed that the DFU-Vehicle group (Fig. 4B) had more cell infiltration than DM model group (Fig. 4A) and DFU-MSCs group (Fig. 4C). The evaluation of epithelial thickness index and granulation tissue thickness showed that the granulation tissue in the DFU-Vehicle group was thinner, while the granulation tissue repair in the DF-MSCs group was nearly complete, the new epidermis was thicker, and the hair follicles and glandular canals were still missing under the skin. Consistent with the results obtained for reepithelialization, epithelial thickness index, granulation tissue thickness, remodeling, and scar elevation index were assessed in Fig. 4J. Figure 4D–H shows representative images of immunohistochemical staining of animal wound tissues in each group.
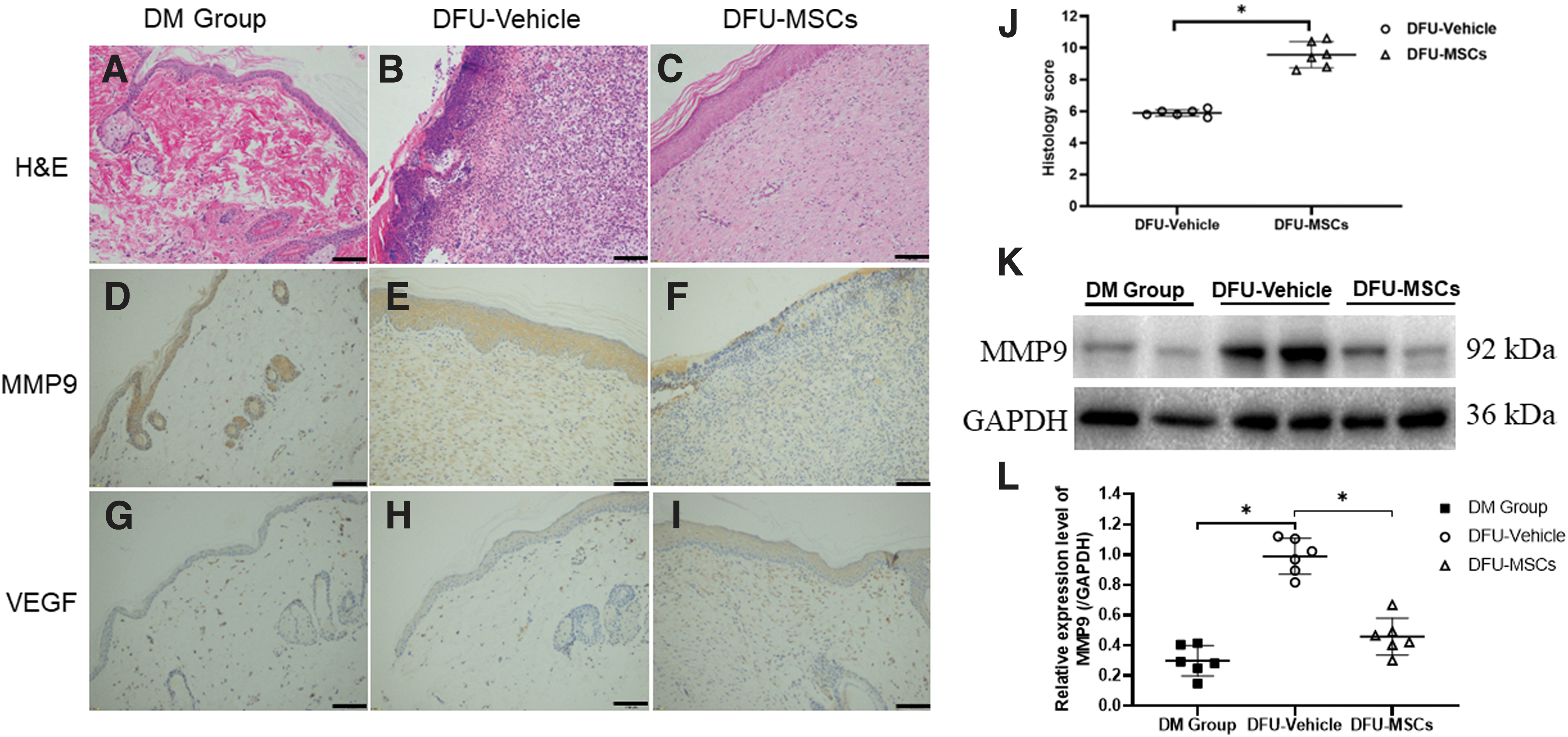
The results of HE staining
The staining of MMP9 in each group showed in DFU-Vehicle group (Fig. 4E) was more highly stained than that in DM model group (Fig. 4D) and DFU-MSCs (Fig. 4F), while there was no difference in antibody staining degree between DFU-MSCs group and DM model group. This was consistent with the quantitative detection of MMP9 expression in tissues by ELISA and western blot. Immunohistochemical staining results of VEGF in each group showed that DFU-MSCs group (Fig. 4I) had darker brown antibody staining than the DM model group (Fig. 4G) and DFU-Vehicle group (Fig. 4H).
According to the analysis results of the histology scoring system, there was a significant difference (P < 0.05) in the healing scores between the DF-vehicle and DF-MSCs groups at 14 days after operation (Fig. 4J).
MMP9 protein expression detection by western blot showed that the expression of MMP9 in DFU-vehicle was upregulated compared with the DM group and DFU-MSCs group (Fig. 4K,L). There was no significant difference between the DFU-MSCs group and the DM model group. This is consistent with the results of immunohistochemistry.
Discussion
DFUs are one of the major complications in DM patients, and high blood glucose levels can slow down the wound healing process [13]. In DFU wounds with lack of blood supply, coupled with infection and poor tissue self-healing ability, clinical treatment is difficult; amputation rate and disability rate are high. Due to the complexity of wound healing, there is currently no standard strategy for the treatment of diabetic wound healing and ulcer complications. Therefore, it is a challenging task to determine an effective treatment method for DFUs, which requires no delay. Stem cell therapy is a kind of biological therapy that has emerged in recent years [11]. hUC-MSCs are derived from zero-year-old stem cells with strong characteristics of proliferation and multidirectional differentiation, and may be a good choice for the treatment of chronic trauma such as DFUs [14]. They are currently commonly used for clinical allotransplantation.
In this study, the hUC-MSCs that we isolated, cultured, and used were mainly in the shape of a shuttle. The hUC-MSCs with high expression of surface markers CD73, CD90, and CD105 could be detected by flow cytometry, but the surface marker CD45 of hematopoietic stem cells was not expressed. The cellular characteristics were consistent with the common characteristics of MSCs [15]. In this study, we established a model of delayed healing in SD rats. This model showed the characteristics of DFUs.
And subsequently we treated them with hUC-MSC transplantation. The animals received the same amount of PBS as a medium control. In the present study, hUC-MSCs were successfully transplanted into the right hind foot of diabetic rats. Interestingly, the DFU wound area was significantly smaller in the DFU-MSCs group than in the DFU-Vehicle PBS injection group at all time points, suggesting that hUC-MSC transplantation plays a good role in accelerating the process of wound healing. By comparing cure rates, we found that hUC-MSC transplantation also accelerated the process of wound closure.
HE staining was used to detect local inflammatory cell infiltration and granulation tissue, as well as reepithelialization in different groups of experimental animals. With these tests, we further validated these findings. Previous studies have shown that after local and systemic treatment of hUC-MSCs, collagen levels (types Ⅰ–Ⅳ) in DFU wounds are increased, and high expression of various growth factors has been observed, including epidermal growth factor (EGF) and keratinocyte growth factor (KGF), transforming growth factor β (TGF-β), VEGF, insulin-like growth factor 1 (IGF-1), IL-8, platelet-derived growth factor (PDGF), and angiopoietin 1 (
MMP-8 and MMP-9 are both MMPs, which are calcium-dependent zinc-containing endopeptidase families with a wide range of substrates, mainly including various types of collagen and gelatin and so on. As the most basic structure in the extracellular matrix, collagen provides support and tension for cells and tissues [17,18]. MMP plays an important role in normal wound healing and the pathology of DFUs [19]. Studies have shown that low levels of MMP-9 can promote wound healing [20]. A series of studies have shown that MMP-8 is beneficial to the remodeling of extracellular matrix and can promote wound healing. MMP-9 can cut laminin and promote keratinocyte migration, which has a harmful effect on wound healing [21 –23]. Nguyen et al. verified the presence of MMP-9 in human DFUs and revealed the discovery of a novel selective potent inhibitor that has shown excellent efficacy in diabetic wound management and is associated with MMP-8 and MMP-9 levels [9]. In this study, we explored the effects of hUC-MSCs on the levels of MMP-8 and MMP-9 in the wound surface of rats.
On the 14th day after surgery, the wound healing rate of the DF-MSCs group was significantly higher compared with the DF-Vehicle group, suggesting that hUC-MSCs could promote the healing of DFU wounds, which might be related to the fact that MSCs could reduce the level of MMP9 on the DFU wound surface and reduce the degradation of wound collagen. The levels of MMP-8 and MMP-9 in the supernatant of foot skin tissue of experimental animals in each group were detected by ELISA, and it was found that the MMP-9 protein level in DF-MSCs group was significantly lower than that in DF-Vehicle group, which was consistent with the results of western blot detection. Therefore, we suggest that inhibiting the harmful protease MMP-9 without affecting the beneficial protease MMP-8 can promote wound healing.
However, this study has some limitations. Based on the treatment of DFUs with MSCs, although the degree of wound healing was analyzed by taking photos at multiple time points, only the wound tissue at a single time point on the 14th day after wound healing was evaluated, and the monitoring of the dynamic changes at the corresponding molecular level in the tissue was lacking, nor was it able to further clarify the mechanism. Therefore, for further research and exploration, we hope to use MMP-9 inhibitors and MMP-8 activators to further verify the functional mechanism of MSCs. At the same time, it is expected to establish the corresponding association between MMP-9 and MMP-8 and angiogenesis.
Conclusions
This study suggested that MSC treatment can promote wound healing and regulated the level of MMP-9 and MMP-8. Our findings did not prove that MSC transplantation improved the healing process through decreasing MMP-9 expression and increasing MMP-8 expression. This study represents promising results for more sophisticated investigations.
Footnotes
Acknowledgment
The authors particularly acknowledge Dr. Zhao Yang who kindly provided assistance in the implementation of the research. The authors thank the Peking Union Medical College for supporting this research.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The project was funded by the following grant: Capital Medical University Funding (PYZ19085), Discipline construction project of Peking Union Medical College, and Lu He Hospital Funding (LHYY2019-JC19). And no potential conflicts of interest relevant to this article were reported.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.